Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

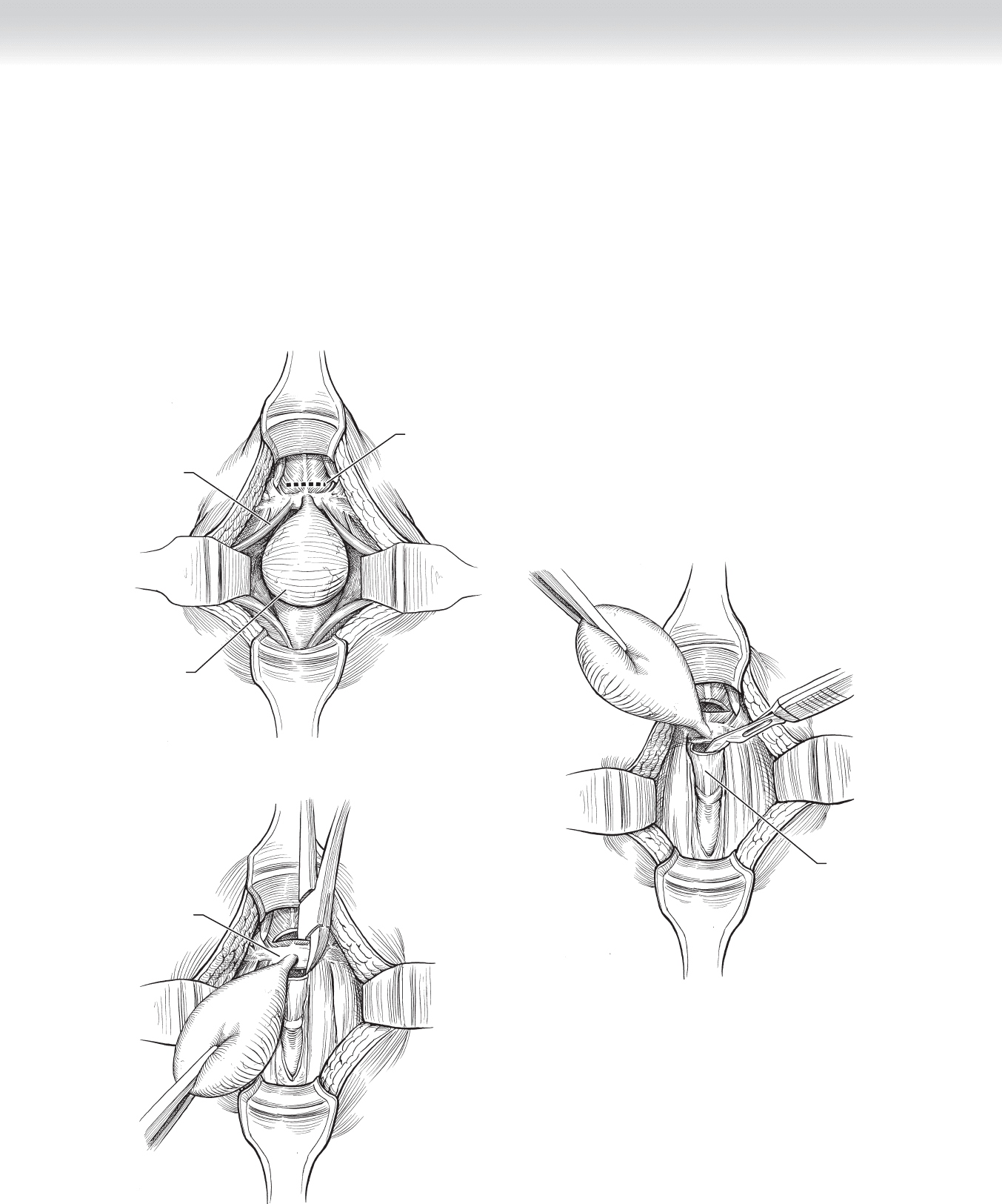
2. DISSECTION
◆ The cyst is dissected away from surrounding superfi cial attachments and followed between
the sternohyoid muscles to the hyoid bone (Figures 7-3 and 7-4). The central portion
of the hyoid bone is freed from strap muscle attachments (sternohyoid muscle inferiorly
and mylohyoid, geniohyoid muscles superiorly). After freeing up the posterior plane of the
hyoid bone from the thyrohyoid membrane, the surgeon resects the central portion (1 to
1.5 cm) of the hyoid bone along with the thyroglossal duct attachment (Figure 7-5).
Sternohyoid
muscle
Incision
Cyst
FIGURE 7 –3
FIGURE 7 –4
Thyrohyoid
membrane
Hyoid bone
FIGURE 7 –5
CHAPTER 7 • Thyroglossal Duct Cyst 85
86 Section I • Head and Neck and Endocrine Procedures
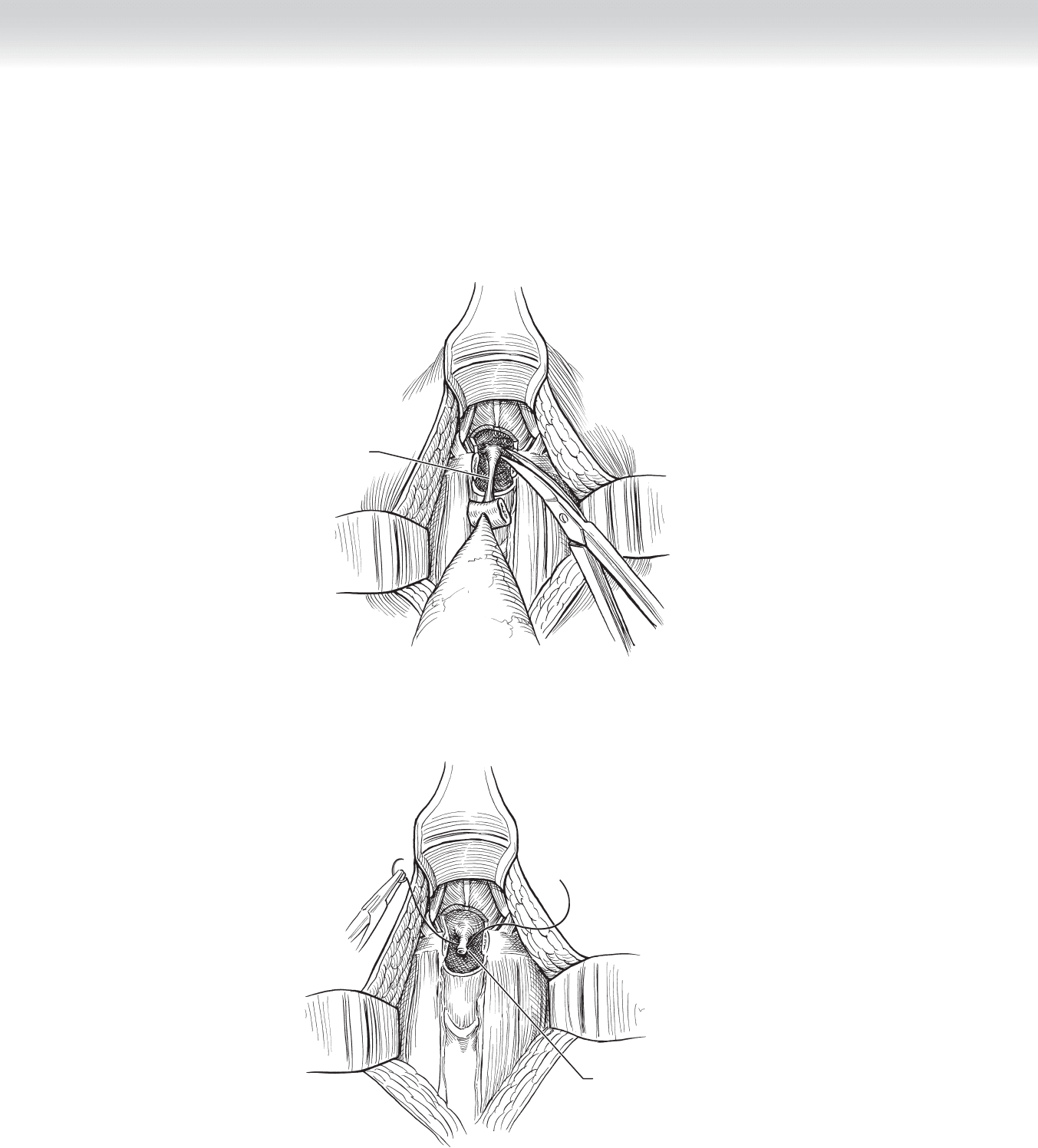
◆ The dissection is continued caudally toward the base of the tongue (Figure 7-6) and the
remaining duct is ligated with absorbable sutures (Figure 7-7).
Duct of cyst
FIGURE 7 –6
Suturing tract
FIGURE 7 –7

3. CLOSING
◆ After meticulous hemostasis, including at the cut ends of the hyoid bone, fascia is approxi-
mated in the midline using 3-0 polyglycolic acid sutures. After approximation of platysma
using 4-0 polyglycolic acid sutures, subcuticular skin closure is performed. No drain is
used.
STEP 4: POSTOPERATIVE CARE
◆ This procedure is routinely performed as an outpatient procedure.
STEP 5: PEARLS AND PITFALLS
◆ Resection of the central portion of hyoid bone with the thyroglossal duct specimen is
essential.
◆ Meticulous hemostasis must be achieved before wound closure to avoid postoperative
hematoma.
◆ Rule out presence of aberrant ectopic midline thyroid gland.
SELECTED REFERENCES
1. Foley DS, Fallat ME: Thyroglossal duct and other congenital midline cervical anomalies. Semin Pediatr
Surg 2006;15:70-75.
2. Bratu I, Laberge JM: Day surgery for thyroglossal duct cyst excision: A safe alternative. Pediatr Surg Int
2004;20:675-678.
3. Ostlie DJ, Burjonrappa SC, Snyder CL, et al: Thyroglossal duct infections and surgical outcomes. J Pediatr
Surg 2004;39:396-399.
4. Sistrunk WE: The surgical management of cysts of the thyroglossal tract. Ann Surg 1920;71:121-123.
CHAPTER 7 • Thyroglossal Duct Cyst 87

88
STEP 1: SURGICAL ANATOMY
◆ Successful adrenalectomy requires a precise knowledge of the anatomy of the retroperito-
neal space, the anatomic relationships of the adrenals to the surrounding structures, and the
differences in the blood supply to the two glands (Figure 8-1).
◆ The arterial supply to the adrenal glands enters the perimeter of the gland originating from
multiple sources including the inferior phrenic and renal arteries and directly from the
aorta. These are named the superior, inferior, and middle adrenal arteries, respectively.
◆ The right adrenal vein is very short and enters the vena cava on its posterior lateral aspect.
This vein does not necessarily get longer as an adrenal mass gets bigger. A large mass can
make identifi cation of the vein very diffi cult and potentially hazardous. Great care should
be used to get control of this structure early in the dissection to avoid catastrophic hemor-
rhage on the posterior aspect of the vena cava.
◆ The left adrenal vein is longer than the right. It is joined by the left inferior phrenic vein
before it drains into the left renal vein.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The indications for adrenalectomy include:
◆ Select adrenal cancers
◆ All biologically active adrenal masses
◆ Adrenal metastases
◆ Incidentally found masses more than 4 to 5 cm
◆ Primary adrenal hyperplasia
◆ The choice of surgical approach (open vs. laparoscopic, anterior vs. posterior) depends
on a number of factors including surgical training/experience, pathology, and presence of
contraindications to laparoscopic surgery.
CHAPTER
8
Adrenals—Anterior, Posterior
(Open and Laparoscopic)
Michael D. Trahan
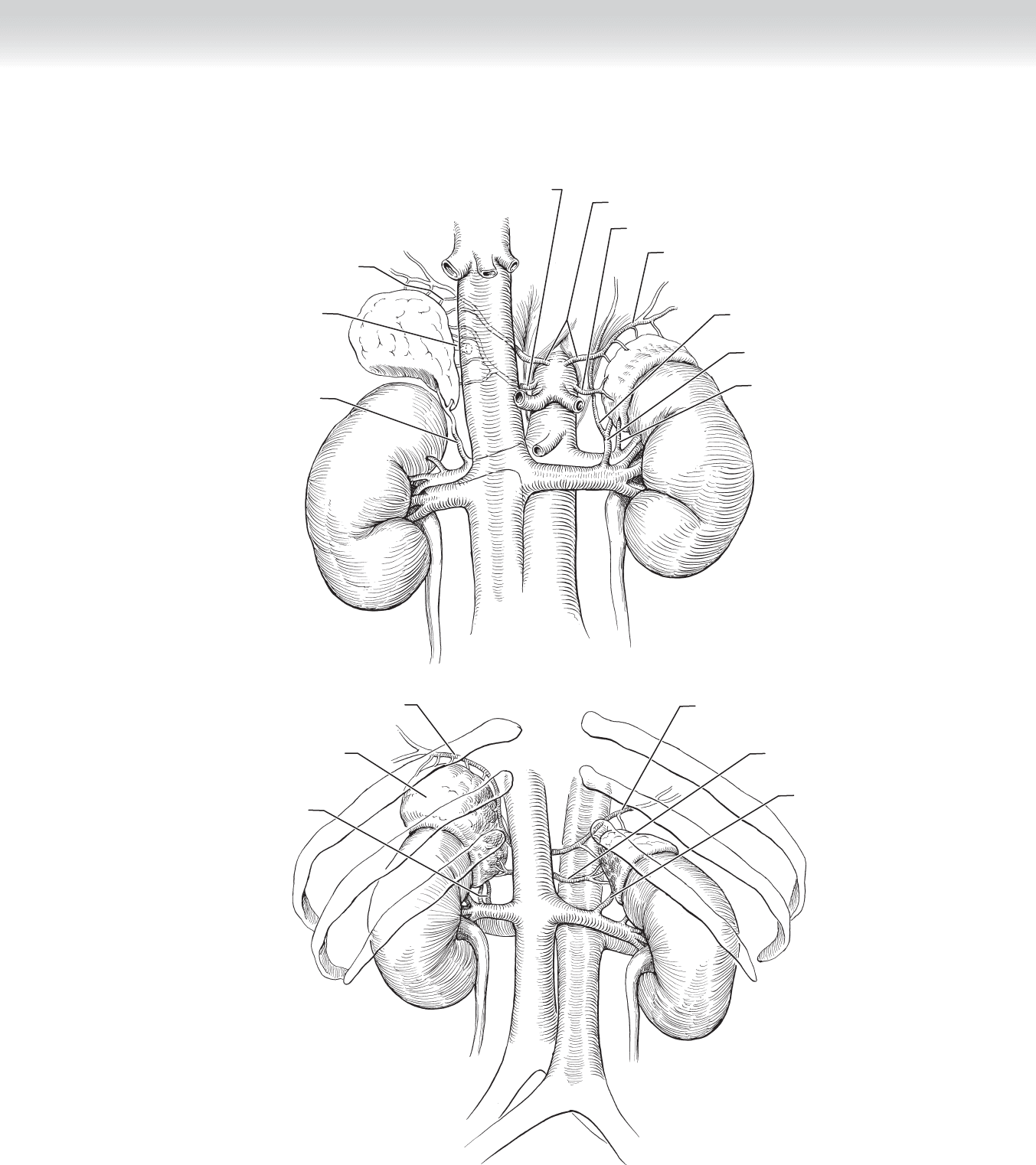
Right middle
adrenal artery
Right
adrenal vein
Left middle adrenal artery
Right and left inferior phrenic artery
Left superior
adrenal artery
Right inferior
adrenal artery
Right superior
adrenal artery
Left adrenal
vein
Left inferior
adrenal artery
Left inferior
phrenic vein
MC
A
Enlarged left
adrenal gland
Left inferior phrenic artery
Right inferior
phrenic artery
Right middle
adrenal artery
Left adrenal
artery and vein
Right inferior
adrenal artery
B
FIGURE 8 –1
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 89

90 Section I • Head and Neck and Endocrine Procedures
◆ Unilateral adrenalectomy is perfectly suited for the laparoscopic approach because of the
small size of most adrenal masses and the large incision necessary for open excision.
◆ Resection of an adrenal cancer should include en bloc resection of involved organs. Such an
extensive resection is best performed with an open approach.
◆ Patients with pheochromocytomas must be medicated preoperatively with phenoxybenza-
mine (alpha blocker) for 7 days or longer to control hypertension. If tachycardia is present
once the blood pressure is controlled, a beta blocker is added for another 5 days before
operation.
◆ A stress dose of glucocorticoids should be given preoperatively to all patients with hyper-
cortisolism.
◆ Routine prophylaxis against deep venous thrombosis and pulmonary thromboembolism is
standard of care.
◆ Preoperative intercostal nerve blocks or placement of an epidural catheter should be
considered for the open approaches to help with postoperative pain control.
STEP 3: OPERATIVE STEPS
1. INCISION
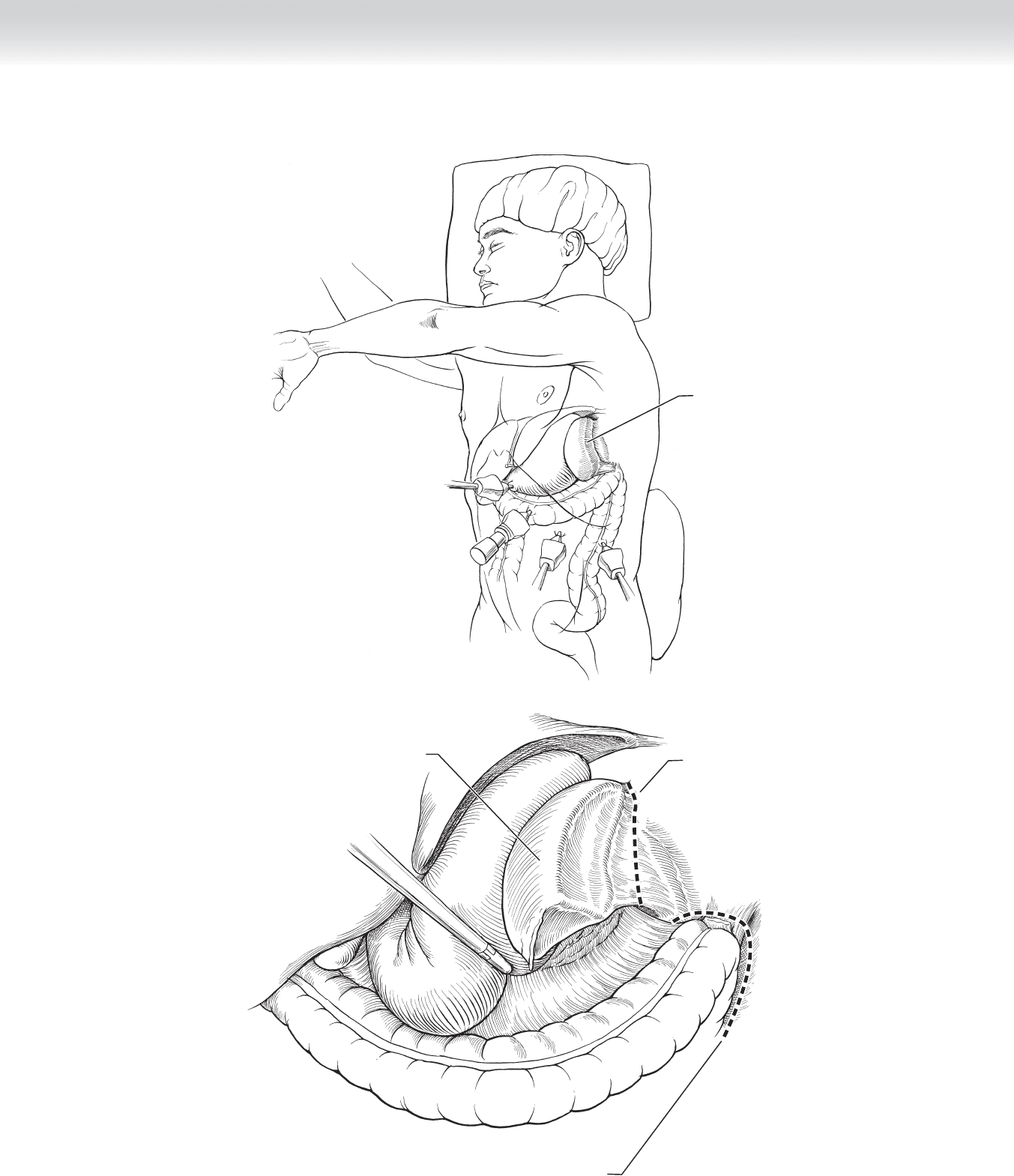
◆ Unilateral adrenalectomy is approached laparoscopically in most cases. The patient is
placed in the lateral decubitus position with the table fl exed. The open fl ank incision in the
lateral decubitus position or the posterior approach in the prone position is favored for
larger masses (⬎10 cm), which have a higher malignant potential.
◆ Bilateral adrenalectomy is often approached through a midline or bilateral subcostal
incision with the patient in the supine position. The laparoscopic approach can be used,
but the patient usually must be repositioned into the contralateral decubitus position
after the fi rst side is complete.
◆ Four ports are usually suffi cient for the laparoscopic approach. The size of the trocars will
depend on the size of the available instrumentation (scopes, clipping device, right-angle
dissector, liver retractor, retrieval bag) and the size of the lesion.
◆ The incision for the posterior approach is along the ipsilateral 12th rib with the patient
appropriately padded in the prone, jackknife position (Figure 8-2).
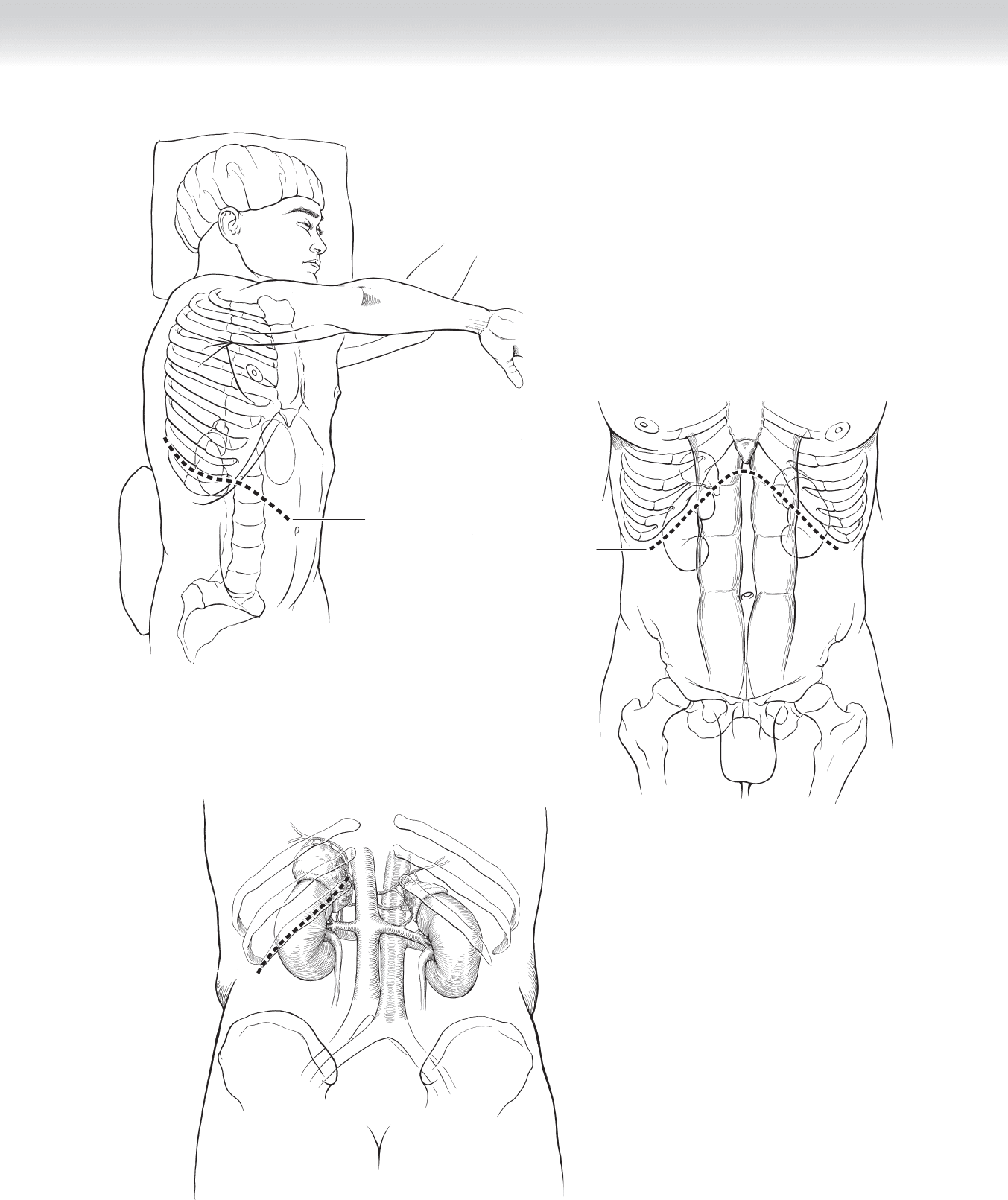
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 91
Thoracoabdominal
incision
A
Subcostal
incision
B
Incision over
12th rib
C
FIGURE 8 –2

92 Section I • Head and Neck and Endocrine Procedures
2. DISSECTION
Laparoscopic Adrenalectomy
◆ The fi rst port (12 mm) is placed using a trocar with internal visualization or by open
technique just below the ipsilateral costal margin in the anterior axillary line.
◆ A 12-mm port is placed higher along the costal margin at least a handbreadth from the fi rst.
Two 5-mm ports are placed lower along the costal margin down to the posterior axillary
line. The left colon will need to be mobilized before the most posterior port can be placed
for left-sided operations.
Left-Sided Laparoscopic Operation
◆ The splenic fl exure and some of the descending colon need to be mobilized using a combi-
nation of sharp and blunt dissection with care used to stay anterior to the kidney. The hook
cautery or ultrasonic dissector is used to accomplish this. The spleen and tail of the pan-
creas are then mobilized by dividing the splenorenal ligament. Gravity will help these
organs fall medially and out of the dissection fi eld (Figure 8-3).
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 93
Spleen hangs
toward midline
in left lateral
decubitus
position
A
Spleen hanging
toward midline
Incision to mobilize
splenic flexure
Incising through
splenorenal ligament
B
FIGURE 8 –3
94 Section I • Head and Neck and Endocrine Procedures
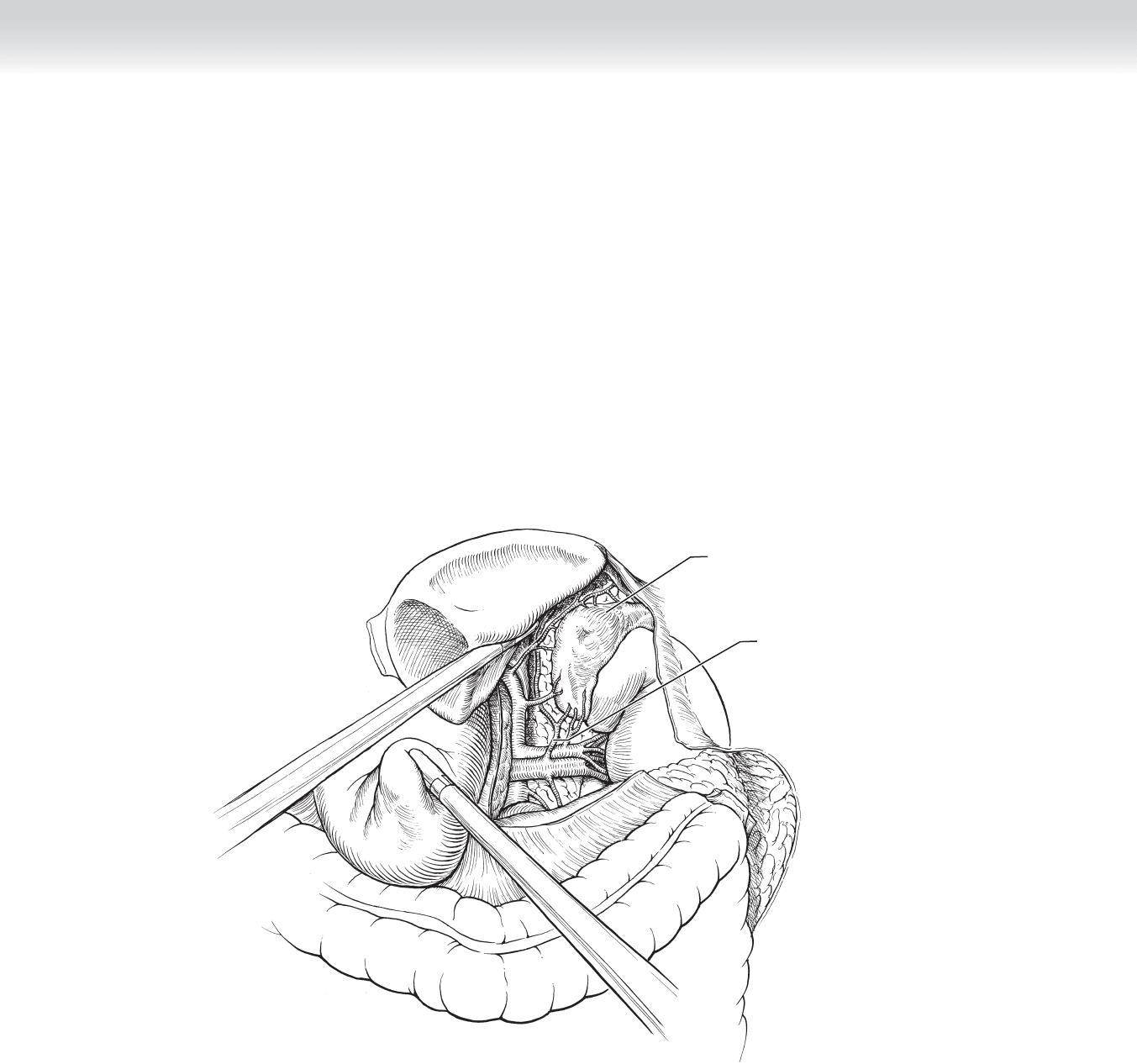
◆ Dissection medially between the adrenal gland and the superior pole of the kidney will
reveal the adrenal vein, which should be clipped and divided early in the operation
(Figure 8-4).
◆ The remainder of the gland’s blood supply and attachments can be effectively divided
with the ultrasonic dissector. Occasionally a larger blood vessel may be encountered that
warrants more secure ligation with clips. The inferior phrenic vein enters the left adrenal
vein medially and can be a source of troublesome bleeding if not identifi ed and con-
trolled.
◆ The entire gland is then placed in a retrieval bag and removed after slightly enlarging one of
the port sites.
Left adrenal
artery and vein
Tumor in
left adrenal
gland
FIGURE 8 –4