Blackburn J.A., Dulmus C.N. (Editors). Handbook of gerontology: evidence-based approaches to theory, practice, and policy
Подождите немного. Документ загружается.

206 E
VIDENCE
-B
ASED
H
EALTH
P
RACTICE
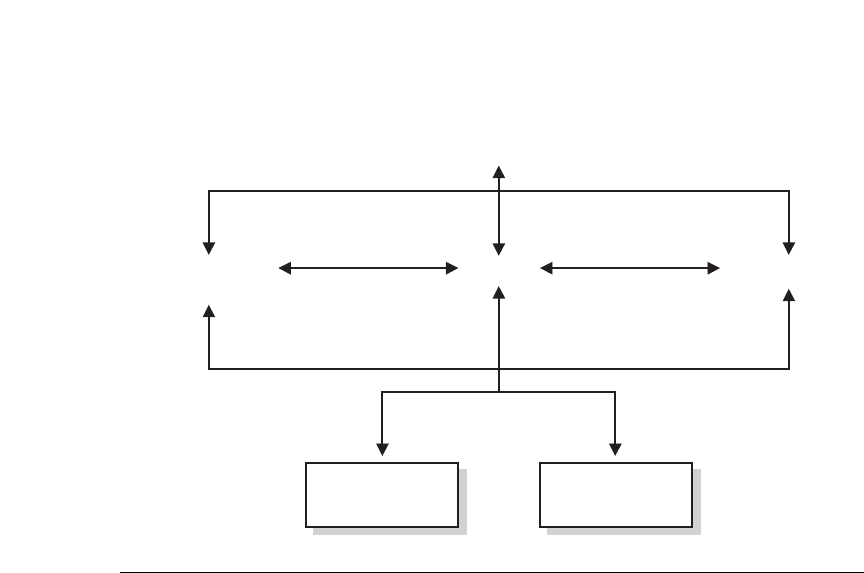
Figure 8.1 World Health Organization’s Biopsychosocial Model of Disability as the Basis
for WHO’s International Classification of Functioning, Disability, and Health.
Source:
Toward a Common Language for Functioning, Disability and Health: ICF,
by the World
Health Organization, 2002, Geneva, Switzerland: Author. Reprinted with permission.
(disorder or disease)
Activity
Contextual factors
Health condition
ParticipationBody Functions
and Structure
Environmental
Factors
Personal
Factors
and injuries, and contextual factors include environmental factors, such as social at-
titudes and structural barriers, and personal factors, such as age, gender, socioeco-
nomic status, geography, and coping skills. One of the purposes of this classification
based on health and functioning is to allow for parity among disabilities, despite
differing specific etiologies. The ICF outlines three levels of functioning: impair-
ment, activity limitation, and participation restriction. A particular health condition
can impact people in none, some, or all of these three areas, depending on both per-
sonal and contextual factors (see Table 8.1). The ICF is intended to help researchers
and practitioners operate from a standard understanding of disabilities; it remains
to be seen how the international community and those in the United States will ac-
tually use this model for developing an evidence base around disabilities.
In fact, there are literally hundreds of definitions of disability employed in the
United States alone. Adler and Hendershot (2000) counted 43 programmatic defi-
nitions of disability among federal programs alone, and states, local governments,
and other agencies can employ their own definitions. Disability has been vari-
ously defined based on individuals’ specific impairments, their functional limita-
tions, their receipt of disability benefits, their use of help for completing tasks, or
general perceptions of disability (Adler & Hendershot, 2000). Numerous mea-
surement problems result from these varied definitions, such as the lack of com-
parability between studies (Lightfoot & Lum, in press). In addition, the disability
rate is an elastic concept, with people reporting disability at differing levels de-
pending on a variety of factors, such as general economic conditions that influ-
ence their participation in the labor market or their receipt of disability benefits.
The two broadest definitions of disability among older adults is found in the
Americans with Disabilities Act (ADA; 1990). The ADA uses a functional defini-
Disability 207
Table 8.1
WHO Classification of Disability, Functioning, and Health
Health
Condition Impairment
Activity
Limitation
Participation
Restriction
Spinal cord
injury
Paralysis
Incapable of using
public transportation
Lack of accommodations in
public transportation leads to
unemployment
Epilepsy Seizures None, controlled by
medication
Does not go to school because of
stereotypes about disease
Vitiligo
Facial
disfigurement
None
Little participation in social activi-
ties because of discrimination
HIV None None Denied housing because of fear of
contagion
Adapted from World Health Organization. (2002).
Toward a common language for functioning, dis-
ability and health: ICF
. Geneva, Switzerland: Author.
tion of disability, which is broad enough to cover lifelong as well as newly acquired
disabilities. The Act defines an individual with a disability as someone who “has a
physical or mental impairment that substantially limits one or more of the major
life activities, has a record of such impairment, or is regarded as having such im-
pairment.” The ADA does not include a list of physical or mental impairments, but
rather focuses on the limitations that such impairment might have on activities of
daily living. This focus on activities of daily living is common for measuring and
comparing people with disabilities for both prevalence and severity.
The other federal definition of note is that of developmental disability, found
in the Developmental Disabilities and Bill of Rights Act (DD Act, 2000). A devel-
opmental disability refers to a host of conditions that begin at birth or in child-
hood and cause a lifelong functional limitation:
A severe, chronic disability of an individual that:
(i) is attributable to a mental or physical impairment or a combination of mental
and physical impairments;
(ii) is manifested before the individual attains age 22;
(iii) is likely to continue indefinitely;
(iv) results in a substantial functional limitation in 3 or more of the following
areas of major life activity:
a. self-care,
b. receptive and expressive language,
c. learning,
d. mobility,
e. self-direction,
f. capacity for independent living,
g. economic self-sufficiency; and
(v) reflects the individual’s need for a combination and sequence of special, in-
terdisciplinary or generic services, individualized supports, or other forms of
assistance that are of lifelong or extended duration and are individually
planned and coordinated.

208 E
VIDENCE
-B
ASED
H
EALTH
P
RACTICE
Many people with lifelong disabilities, such as intellectual disability, cerebral
palsy, Autism Spectrum Disorder, fetal alcohol syndrome, genetic and chromoso-
mal disorders such as Down syndrome and Fragile X, and some sensory disabili-
ties, fall under the category of developmental disability.
The etiologies of disability in older adults include everything from chromo-
somal abnormalities that cause impairments before birth that continue
through an individual’s life, to accidents or disease occurring in midlife, to
age-related disabilities, such as Alzheimer’s disease. Developmental disabili-
ties, by definition, occur either at birth or during one’s developmental years.
There are hundreds of causes of developmental disabilities, including injuries
and conditions in the brain before birth, during birth, or during childhood.
Some developmental disabilities have a clear etiology, such as Down syn-
drome, resulting from a chromosomal abnormality; others have unknown eti-
ologies or only inferred etiologies. For example, low birth weight is considered
a risk factor for intellectual disability (Leonard & Wen, 2002), yet it does not
meet the criteria for a cause of intellectual disability, as there is no clear
causal pathway. Although most developmental disabilities cannot be pre-
vented, there are some contextual characteristics that cause or influence de-
velopmental disabilities, such as poor nutrition, mother’s excessive intake of
alcohol or drugs before birth, injuries during birth, poor nutrition, and envi-
ronmental exposure such as lead poisoning in childhood. When possible,
knowledge of the etiology of an individual’s disability, especially those with
developmental disabilities, can be important for future screening for age-
related comorbid conditions that are specific to a particular health condition.
Key Health Issues for Older Adults with Intellectual Disabilities
• Dementia
• Visual impairment
• Hearing impairment
• Thyroid conditions
• Osteoarthritis
• Oral health
• Obesity
The health conditions that cause impairment or activity limitations that
people acquire over age 65 include visual loss, hearing loss, and arthritis,
whose rates all rise dramatically as people age (Ettinger et al., 1994; National
Center for Health Statistics, 1993). Other common age-related health condi-
tions that may or may not cause activity limitations are diabetes, heart
conditions, dementia, and hypertension (U.S. Census, 1996). Some disabili-
ties in older age are related to organic conditions; contextual factors, such
as smoking, poor diet, poor health care, and falls and accidents (Rubenstein,
Robbins, Josephson, Schulman, & Osterweil, 1990), also can influence
health conditions. Further, health conditions and activity limitations vary
based on race, ethnic background, and socioeconomic status (Verbrugge &
Jette, 1994).

Disability 209
EVIDENCE-BASED SUPPORTS FOR OLDER PEOPLE
WITH DEVELOPMENTAL DISABILITIES
Professionals caring for an older person with a disability should keep in mind
several key factors. First, in the area of disability, the concept of professional in-
tervention is more appropriately viewed as professional support for a person with
a disability. Second, all professional supports offered to a person with a disabil-
ity and his or her family should be based on the best evidence available, with an
eye to improving or maintaining an individual’s quality of life and inclusion into
the community. Up until very recently people with disabilities had very limited
civil rights, were regularly segregated or institutionalized, and were even used
for medical and social experiments without informed consent. Using the best ev-
idence available in designing and implementing professional supports for people
with disabilities can be one way to respect these individuals. Third, professionals
must recognize that the person with the disability and his or her family are al-
ways the experts on their individual situation and have the best assessment of
their needs and desires. When intervening in an individual’s life, the professional
must assume the role of subordinate to the individual, and allow and encourage
the person with the disability to make decisions based on evidence.
Professionals often collaborate with older people with disabilities to provide
needed supports in the following broad life areas: health, residential and commu-
nity living, life planning.
H
EALTH
One reason the number of older people with disabilities is rapidly expanding is
an overall improvement in health care, which has led to increased longevity for
people with and without lifelong disabilities. People with developmental disabil-
ities are also living longer because of greater access to health care and healthier
and more active lifestyles that accompany community-based living, especially in
comparison to living in an institution. People with developmental disabilities
never used to live into old age, but with their increased life span they are now ex-
periencing age-related health conditions. There is still extremely limited knowl-
edge about age-related health conditions for people with developmental
disabilities (Evenhuis, Henderson, Beange, Lennox, & Chicoine, 2000), though
there are more studies and medical trials in process (Seltzer, 2004). However, it is
clear that people with developmental disabilities have some age-related health
conditions similar to those of people without disabilities, but also have unique
health concerns. These can vary based on the specific etiology of the developmen-
tal disability; for instance, people with chromosomal syndromes, such as Down
syndrome, have different age-related impairments than people with a central
nervous condition, such as cerebral palsy.
The area with the most advanced research evidence is the health status of peo-
ple aging with Down syndrome. People with Down syndrome have a shorter life
expectancy than people with developmental disabilities. They also tend to expe-
rience age-related conditions earlier and have more significant age-related health
conditions. Common age-related conditions of people with Down syndrome are
adult-onset epilepsy, hearing loss, visual loss, hip disease, and thyroid disorder

210 E
VIDENCE
-B
ASED
H
EALTH
P
RACTICE
(Dinani & Carpenter, 1990; Janicki, Heller, Seltzer, & Hogg, 1996; Puri, Ho, &
Singh, 2001; Van Allen, Fung, & Jurenka, 1999). The most debilitating age-related
condition is early-onset dementia. People with Down syndrome have a very high
prevalence of early-onset dementia (Janicki & Dalton, 2000). Holland, Hon, Hup-
pert, and Stevens (2000) found that personality and behavioral changes are indi-
cators of early onset of dementia for people with Down syndrome; such
conditions may begin in their 30s, with Alzheimer’s disease following in their 40s
or 50s. It appears that people with other types of developmental disabilities have
no greater prevalence rate of dementia than people without disabilities (Zigman
et al., 2004).
Diagnosis of many age-related conditions, such as dementia, can be compli-
cated in people with developmental disabilities as it may be difficult to tease out
the cognitive impacts of the disability from that of the dementia (Shultz et al.,
2004). Further, there are few valid scales to measure common age-related condi-
tions in people with developmental disabilities (Shultz et al., 2004). There is a
new research focus on appropriate assessment of age-related health conditions in
people with disabilities, particularly for dementia since the advent of antidemen-
tia drugs (Strydom & Hassiotis, 2003). For example, there is growing evidence
that observer rater scales or instruments administered to informants have been
found to be much more accurate for diagnosing dementia for people with Down
syndrome than typical neuropsychological direct assessments (Deb & Braganza,
1999; Strydom & Hassiotis, 2003). Ball et al. (2004) found that an informant inter-
view, specifically the Cambridge Mental Disorders of the Elderly Examination
(CAMDEX) tool, is reliable and valid for assessing dementia. The most common
tool, the Dementia Questionnaire for Persons with Mental Retardation, has been
found to be both reliable and valid (Evenhuis, 1996), although there are still some
concerns about sensitivity (Strydom & Hassiotis, 2003). The development of spe-
cific assessments such as these, which are modified to take into account the
unique conditions of older people with developmental disabilities, are needed to
appropriately diagnosis this population and begin to provide them appropriate
treatment.
Another health-related concern for older people with developmental disabili-
ties is health care providers’ lack of general knowledge about their typical health
and functioning levels (Messinger-Rapport & Rapport, 1997). In addition, health
care providers may be unaware of the resistance some older people with disabili-
ties may have toward the medical profession, relating to previous poor service re-
ceived from untrained staff both in and outside of institutions (Seltzer &
Luchterhand, 1994). Few medical professionals have been trained to work with
older people with disabilities; there is a great need for combined training in the
areas of geriatric medicine and intellectual and developmental disabilities (Jan-
icki et al., 1999). A joint physician training program in aging and developmental
disabilities has been developed at the Strong Center for Developmental Disabili-
ties at the University of Rochester Medical Center (Program in Aging and Devel-
opmental Disabilities, 2006).
There are other accessibility barriers to receiving appropriate health care, in-
cluding a complex bureaucracy and physical and societal attitudinal barriers.
Many people with disabilities have complex cases and are receiving care from a
multitude of sources, resulting in a very complex management of care as well as

Disability 211
financial reimbursement problems. Case management by professionals with mul-
tidisciplinary training and expertise is necessary in these cases (Walsh, Kastner,
& Criscione, 1997). A variety of other barriers, such as physically inaccessible ser-
vices, must also be removed (Selzter & Luchterhand, 1994).
Along with improved health care, a healthier lifestyle associated with living in
the community has helped to improve life expectancy for individuals with devel-
opmental disabilities. However, this population is still more likely to have a
sedentary lifestyle and poor nutrition (Braunschweig et al., 2004; Heller et al.,
2002) compared to people without disabilities. Health promotion activities can
help them avoid conditions related to poor fitness and nutrition, such as Type 2
diabetes, osteoporosis, and coronary heart disease. Heller, Hsieh, and Rimmer
(2004) found that adults with Down syndrome involved in fitness and health ed-
ucation training programs have improved attitudes toward exercise, as well as im-
proved life satisfaction. Others have found that exercise and health training
programs for adults with intellectual disabilities result in dramatically increased
improvement in physical functioning and other fitness measures (Podgorski,
Kessler, Cacia, Peterson, & Henderson, 2004; Rimmer, Heller, Wang, & Valerio,
2004). Key barriers to such participation are caregivers who perceive that physical
fitness is not effective for adults with Down syndrome as well as access barriers
(Heller, Hsieh, & Rimmer, 2002).
The overall increased longevity of people with disabilities has led to a new area
of medical care that is just beginning to develop appropriate evidence for clinical,
programmatic, and policy recommendations. There is a need for more evidence-
based practice standards in the area of health care for older people with develop-
mental and other disabilities, as well as more well-trained medical professionals
who specialize in providing health care services to this population.
R
ESIDENTIAL AND
C
OMMUNITY
-B
ASED
L
IVING
Along with increased longevity, the other significant recent change for older peo-
ple with disabilities has been the large shift toward residing in community-based
settings. During the 1970s and 1980s, the philosophy of normalization (Wolfens-
berger, 1972) swept the field of disability services. Normalization meant that peo-
ple with disabilities should no longer live in segregated facilities and lead
segregated lives, but rather should lead “normal” lives in the community. This
emphasis on normalization, which is related to more modern concepts of commu-
nity integration and community inclusion, led to the closing of many large resi-
dential institutions and the deinstitutionalization movement in the United States
and abroad. The majority of large institutions have now been closed in the United
States, and most people with disabilities who are living outside their familial
home live in small or medium-size community-based settings with paid staff,
such as group homes or other shared living arrangements.
In the United States, federal policy has gradually shifted to support community-
based options for people with disabilities. In 1981, 10 years after Medicaid began,
Congress authorized states to use Medicaid to pay for home- and community-
based services for older people and people with disabilities who would otherwise
reside in or receive care from institutions (Omnibus Budget Reconciliation Act of
1981). The Home and Community-Based Services waiver is now the major source of

212 E
VIDENCE
-B
ASED
H
EALTH
P
RACTICE
funding for community living for older people with disabilities who receive fund-
ing for residential care. Currently, approximately 1.4 million people with disabili-
ties receive services through Medicaid that support them to live at home
(Harrington & Kitchener, 2003). Several years after the Medicaid waiver, the Nurs-
ing Home Reform Act was passed as part of the Omnibus Budget Reconciliation Act
of 1987 (PL 100-203). This law was intended to prevent the inappropriate institu-
tionalization of people with disabilities in nursing homes by requiring states to
conduct a Preadmission Screening and Annual Resident Review of individuals
with disabilities to ascertain if they actually needed skilled nursing care.
More recently, the Olmstead decision by the U.S. Supreme Court solidified the
notion that people with disabilities should not be unnecessarily institutional-
ized (Olmstead et al. v. L. C. et al., 1999). In this case, two women with intellectual
disabilities and mental illness voluntarily admitted themselves to a state psychi-
atric hospital in Georgia. When the two women and their service providers de-
termined that they were ready for discharge, the women were not discharged
from the hospital because there were no “slots” available for them. The Atlanta
Legal Aid Society filed a lawsuit on behalf of these two women, claiming dis-
crimination under Title II of the Americans with Disabilities Act of 1990. The
circuit court ruled in favor of the plaintiffs, and the U.S. Supreme Court upheld
the ruling on the basis that unjustified institutionalization of people with dis-
abilities is a form of discrimination under Title II of the Americans with Disabil-
ities Act. States are now instructed to have comprehensive, effective working
plans to ensure that individuals with disabilities receive services in the most in-
tegrated setting appropriate to their needs. The federal government signaled its
support of Olmstead with President Bush’s New Freedom Initiative of 2001. As
part of the New Freedom Initiative, President Bush released Executive Order
13127 (June 2001), which ordered states to offer people with disabilities of all
ages care in the least restrictive and most integrated setting possible and or-
dered federal agencies to work with states to ensure community-based alterna-
tives to institution-based care.
There is ample evidence that people with lifelong disabilities, people with age-
related disabilities, and their family members desire alternatives to nursing
homes and other congregate care facilities. For example, in a 1999 survey by the
AARP, 82% of people age 45 and older said that they would prefer to remain in
their own home even if they needed help caring for themselves (Bayer & Harper,
2000). Similarly, a 1997 International Communications Research (ICR) survey
asked people over age 50 where they would like to live if they had a disability that
needed care 24 hours a day, rather than just help with everyday activities; only
23% responded that they would rather live in a congregate care facility. Both peo-
ple aging with a disability and people with age-related disabilities demand such
community-based services, and there is a growing acceptance in the professional
fields of disability and aging services that community-based care is an appropri-
ate and desired practice.
As a result of the philosophical and policy shifts relating to residential care
and the ever-growing demand for community-based options, there has been a
rapid expansion of home- and community-based living arrangements for older
people with disabilities. Many residential providers, particularly in the field of
developmental disabilities, have made large-scale changes in their provision of
services, closing down large institutions and offering community-based residen-

Disability 213
tial options (Lightfoot, Hewitt, & Sauer, 2005). Unfortunately, the demand for
such community-based living arrangements currently far exceeds the supply,
with an estimated 75,000 people with intellectual and developmental disabilities
alone on state waiting lists for such services (Prouty & Lakin, 1998). As the rate of
older people with disabilities continues to grow rapidly, this supply problem may
last far into the future.
Although philosophy, policy, and some programs have clearly shifted toward
community-based living as the best arrangement for older people with disabili-
ties, the research base is more mixed for people aging with developmental dis-
abilities. For the most part, studies of middle-age and older individuals with
developmental disabilities who moved from institutional to community-based
care find that people living in the community fare better overall than those resid-
ing in institutions. Research has found that people with disabilities who have
transitioned from institutions to community-based residential settings experi-
ence an increase in health (Heller, Factor, & Hahn, 1999; Litzinger, Duvall, & Lit-
tle, 1993), activity levels (Barber, Cooper, & Owen, 1994), adaptive behavior
(Donnelly et al., 1994; Heller et al., 1999; Larson & Lakin, 1989; Young, Ashman,
Sigafoos, & Grevell, 2001), and level of community inclusion and integration (Bar-
ber et al., 1994; Heller et al., 1999).
However, several other studies have found that although certain aspects of the
lives of people experiencing deinstitutionalization improved, the level of adaptive
behavior either decreased (Barber et al., 1994) or showed no change (Young et al.,
2001). Findings regarding the actual impact of the relocation have also been
mixed, with some studies indicating that the relocation itself may cause some
problems (Heller, 1988) and others finding no impact from the relocation (Heller
et al., 1999).
There are a number of possible explanations for these mixed findings. It is
more likely that age-related or other conditions of individuals living in a commu-
nity setting will go undetected compared to those in an institutional setting.
This points to a lack of access to health care for older people with disabilities in
community settings, a lack of training and awareness on the part of health care
and social service professionals, and less supervision and fewer behavior inter-
ventions in community settings (Carlsen, Galliuzzi, Forman, & Cavalieri, 1994;
Rimmer, Braddock, & Marks, 1995). As mentioned earlier, there is a need for
those working with older people with developmental disabilities, both as medical
professionals and caregivers, to have training in the health needs of and provide
comprehensive geriatric assessments for those with disabilities, particularly
those residing in the community.
Although a large trend in the disability and aging field has been toward pro-
moting community-based formal options for older people with disabilities, the
most common living arrangement for adults with developmental disabilities re-
mains living with their family of origin. Fujiura (1998) estimates that about 60%
of adults with developmental disabilities live with their families rather than in
group homes or other formal arrangements. These families receive little federal
or state support in caring for their adult children with disabilities (Stancliffe &
Lakin, 2004), and there are very long waiting lists for any supportive services,
such as respite care, personal care assistance, and in-home health care, for these
families (Davis, 1997). As there is so little state support for family caregivers,
families end up spending large amounts of money caring for their adult children.

214 E
VIDENCE
-B
ASED
H
EALTH
P
RACTICE
Fujiura, Roccoforte, and Braddock (1994) found that families spend approxi-
mately one fifth of their pretax annual income on expenses related to caring for
their adult children. A survey of state units of aging regarding parent caregivers
of adults with developmental disabilities found that respite care was their great-
est unmet need (Factor, 2004).
Currently, over one fourth of the primary caregivers of adults with develop-
mental disabilities are over age 60 (Braddock, 1999; Fujiura, 1998). The number of
these “two-generation elderly families” (Davis & Berkobien, 1994) is expected to
rise over the next decade, with the aging of the baby boom generation and in-
creased life expectancies for all populations. These families often have not re-
ceived any formal supports (Smith, Fullmer, & Tobin, 1994). Some may have an
inherent distrust of the system and disability professionals if professionals ad-
vised these families to institutionalize their children at birth; some may not feel
the need for supportive services (Smith, 1997). People in some ethnic and cultural
groups may find natural supports, such as the extended family or community,
rather than a formal support system (Magana, 1999). Others report a need for
emotional and coping supports, such as support groups or counseling, but that
these services are unavailable (Smith, Majeski, & McClenny, 1996). Hayden and
Heller (1997) found that younger caregivers are more likely to seek supportive
services and have higher expectations of the social service system to provide sup-
portive services. As respite care use has been increasing by parents of older
adults with developmental disabilities, and more people are likely to use such
services in the near future both due to population growth and service-usage atti-
tude, there will be a need for greatly increased provisions of respite care and
other supportive services.
With increasing numbers of older adults with disabilities, including a new co-
hort of older adults with developmental disabilities, there is a dire need for new
residential options for older people with disabilities. This is especially true for
adults with lifelong disabilities who may need to transition at an older age to an
alternative living arrangement when their family is no longer able to care for
them because of family members’ own declining health or death.
Because most people want to remain in their own homes, whether in their fam-
ily home or in a long-term group home, there is a new focus on “aging in place”
for older people with disabilities. Part of this movement focuses on the use of en-
vironmental modifications and assistive technology to help people remain in
their own homes. This can include building ramps, modifying doorways, or using
devices such as walkers, amplifiers, or call buttons that help people maintain
their functioning level and independence (Hammel, Lai, & Heller, 2002). How-
ever, many older people with disabilities, especially those with cognitive func-
tioning issues, may require paid staff to remain at home. For people who had
been living with their parents, this could involve a move into the formal care sys-
tem, which may not allow them to age in place. For those already living in a for-
mal care arrangement, such as a group home, this may require changes to the
rules and standards of the group home, and could require additional funding
(Janicki, McCallion, & Dalton, 2002). Although aging in place is an attractive con-
cept, the funding streams for older people with developmental disabilities have
yet to make it a valid option for many.
There is also evidence that along with desiring community-based services,
many people with disabilities would prefer to manage these services themselves,

Disability 215
rather than having an agency do so. Several studies have shown that although
older people with disabilities are less likely to desire consumer-controlled ser-
vices than younger people with disabilities, there still are a significant percent-
age of people over age 65 who desire to control their own services. Mahoney
et al.’s (1998) study of personal assistance recipients in New York found that 55%
of people with disabilities under age 65 and 31% of those over age 65 desired a
cash option. Similar results were obtained in studies by Eustis and Fischer (1992),
who found that 33% of older clients showed evidence of participating in the con-
trol of their service, and Glickman, Brandt, and Caro (1994), who found that
roughly 33% of older clients indicated willingness to become involved in control-
ling their services.
Older people with disabilities who are unaccustomed to the consumer-control
model may be less likely to desire consumer-controlled services than younger
people with disabilities; however, as the baby boomer population ages, it is likely
that more people will desire consumer-controlled services (Batavia, 1998). Sur-
veys of the aging baby boomer population have confirmed this growing desire. In
the ICR (1997) survey of Americans over age 50, 76% of the respondents indicated
that they would prefer to manage their own home care services if and when they
acquired a disability. Furthermore, as evidence continues to grow that people
with disabilities have higher satisfaction under consumer-controlled models
(Beatty, Richmond, Tepper, & DeJong, 1998; Benjamin et al., 2000) with no harm-
ful health or safety impacts, it is likely that older people with disabilities will in-
creasingly desire to control their own services.
This move toward consumer-directed services has reached a degree of acceptance
in aging and disability services, and there are a number of pilot consumer-directed
services programs for people who are aging or have disabilities. For example, the
Cash and Counseling Demonstration and Evaluation is testing consumer-directed
services for people with disabilities of all ages on a large scale (Doty, 2000; Ma-
honey, Simone, & Simon-Rusinowitz, 2000).
L
ATER
-L
IFE
P
LANNING
Many parents do not plan for their adult child’s later lives, due to lack of informa-
tion, stress, worry, or denial (Heller & Factor, 1991; Kaufman, Adams, & Camp-
bell, 1991). When later life planning does occur, the people with developmental
disabilities themselves are often not included, consulted, or even informed of the
plans (Heller, Miller, Ksieh, & Sterns, 2000; Sutton, Sterns, & Schwartz-Park,
1993). Further, the plans often only include arrangements for where the adult
with disabilities will live in the future, without including other aspects of the in-
dividual’s life that can impact his or her quality of life, such as financial matters,
guardianship, retirement, and leisure activities (Reilly & Conliffe, 2002).
Residential planning is one of the key worries for people with lifelong disabili-
ties and their families. This is particularly true for those who have not been in-
volved in the formal service system and have been living at the family home. For
these families, on the death of the parents the adult child may experience many
significant transitions, coupled with grief at losing his or her parents, which can
cause depression and confusion (Ludlow, 1999). Even those involved in the sys-
tem usually experience some sort of transfer of care, either to a sibling or relative
or into a formal system.