Blackburn J.A., Dulmus C.N. (Editors). Handbook of gerontology: evidence-based approaches to theory, practice, and policy
Подождите немного. Документ загружается.


526 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
45
In re Saikewicz, 370 N.E. 2d 417, 430–432.
health care decision. Generally speaking, patients can be divided into four cat-
egories (at the time of the decision to refuse life-prolonging procedures): the
competent patient; the once-competent, currently incompetent patient; the
never-competent patient; and the minimally conscious patient.
The competent patient is conscious and capable of giving informed consent.
Therefore, for these patients, there is no need for a surrogate decision maker and
no need for court intervention. Absent some concern about the patient’s ability to
give informed consent or the legality of the patient’s direction, or, perhaps, the
health care provider’s concern about liability because of an unconventional wish
of the patient, the patient’s decision controls. If the patient chooses to exercise her
“right to die” by having life-prolonging procedures withheld or withdrawn, then
the patient’s choice should be honored.
The most common category of patient is the patient who was once-competent,
but at the time to make the health care decision is no longer competent. Most of
the patients in the right to die decisions fall in this category, including Karen
Ann Quinlan, Nancy Cruzan, and Estelle Browning. For this patient, there must
be some surrogate decision maker and the application of the appropriate surro-
gate decision-making standard (most states apply the substituted judgment doc-
trine). The problem so often with these patients is that so few have made their
wishes known or designated a surrogate. Most commonly, the patient may have
made some statements in the past, but not in conjunction with his or her specific
health condition. Therefore, the patient’s wishes must be discerned as best as
possible, and it may be necessary for a court to determine whether there is suffi-
cient evidence of the patient’s wishes before life-prolonging procedures can be
withdrawn.
The never-competent patient is the patient who, although legally an adult based
on age, in the eyes of the law has never had the ability to make legally binding de-
cisions or to give informed consent. These patients suffer from severe mental retar-
dation (note that some people can suffer from developmental disabilities or mild
mental retardation and still be able to make legally binding decisions and give in-
formed consent) and generally have the IQ of a very small child. For these patients,
it was never possible for them to make advance directives or to state their wishes
regarding life-prolonging procedures. For these patients, it is necessary to have
court involvement to some degree, whether to appoint a guardian for the patient
with the authority to make health care decisions, including end-of-life decisions, or
to order the removal of life-prolonging procedures. For these patients, the court
must look at factors such as health condition, treatment, ability to cooperate with
the treatment, and side effects. An example of the court’s analysis of factors to con-
sider in such cases is contained in the Saikewicz decision.
45
The whole area of jurisprudence in the right to die is driven by the advances in
medical technology. So too is the fourth category of patient, the patient who is
minimally conscious. These patients have some awareness and interaction with
their environment and may be able to engage in rudimentary communication,
such as answering yes or no questions with repeated prompting using assistive
communication devices, eye blinks, and so on (Giacino et al., 2002). The challenge
in these cases is the reliability of the communication. There is no real way to

Health Decisions and Directives about the End of Life 527
46
Conservatorship of Wendland, 26 Cal. 4th 519, 529–530 (2001).
47
Id. at 524–526.
48
See, for example, Florida Statutes, 744.3115.
know whether the patient understands the question and whether the answer is
truly a reflection of the patient’s conscious decision. One of the more graphic ex-
amples of the issues faced in cases of patients who are minimally conscious is the
case of Robert Wendland,
46
who was not comatose or terminally ill, nor was he in
a persistent vegetative state.
47
Think about how the category of patient affects the patient’s right to refuse
life-prolonging procedures. One tool that patients can use, but often don’t, is the
advance directive.
A
DVANCE
D
IRECTIVES
Decisions about various health care issues at the end of life should be ad-
dressed in advance to avoid ambiguity or legal challenges. We review next some
of the most common decision categories, generally referred to as “advance
directives.”
Advance directives are expressions by individuals, made while they are legally
competent, about how they want certain health and medical procedures to be
done for or about them in the event of disability or incompetence. Disability and
incompetence can come in two forms: physical and mental. For example, follow-
ing an accident, injury, or illness, a person may not be able to independently pro-
vide for many of his own daily living needs, such as preparing meals, driving,
bathing, or caring for his own health care needs. Or patients may lose the capac-
ity to speak and easily convey their wishes. In the event somebody becomes phys-
ically disabled or incapacitated, on a temporary or permanent basis, what
guidelines should be used to provide care and services for him? What scope of
care and services would that individual want?
The matter is more challenging when there is a mental disability or incapacity.
Persons born with these incapacities have provisions made for them in the law,
wherein guardians are appointed to make decisions on their behalf.
48
But what
happens if, as a consequence of an illness or injury, a person loses substantial
mental capacities and is no longer able to make decisions or convey information
about his intentions?
Once a person has become incompetent, he is no longer legally capable of mak-
ing certain decisions, and his intentions may not be carried out unless he has
stated them in advance, according to the guidelines of specific state laws. As we
noted earlier, living wills and health care surrogates took root during the 1970s.
Generally, these advance statements are written documents, which may have
to be witnessed and notarized, and in some states, a particular form may have to
be used or followed if the document is to conform to the law. But this is not uni-
versal. Some states accept as evidence verbal expressions of intention—but prov-
ing these up can be difficult and certainly costly if there is a challenge.
For example, assume that a wife claims that she had been told by her husband
that he did not want any form of life-prolonging care in the form of a respirator,
nutrition/hydration tube, heroic measures to resuscitate, or even antibiotic
528 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
49
Bouvia v. Superior Court, 195 Cal. App. 3d 1075 (1987).
50
Satz v. Perlmutter, 379 So.2d 359 (Fla. 1980).
51
Wendland, op. cit.; Guardianship of Schiavo, 916 So.2d 814 (Fla. 2d D.C.A. 2005).
52
42 U.S.C. SS 1395cc, 395mm, 1396a.
therapy. But their child disagrees with his mother’s statement of intent and be-
lieves instead that his father should be allowed to receive heroic, life-sustaining in-
terventions at all costs. Families face disagreements every day around these
issues. Most of these are worked out through the auspices of a social worker, hos-
pice counselor, or therapist. But guilt, bad family relations, honest differences of
opinion, and other factors can and do get in the way of a seamless end-of-life pro-
cess. The consequences can be devastating, not only for family members who may
literally feud, but for the incapacitated person who may be subject to prolonged
periods during which his or her wishes are not being fulfilled. And we are not re-
ferring here to the physician-assisted suicide cases involving Dr. Kevorkian but to
cases like Elizabeth Bouvia
49
or Satz v. Perlmutter,
50
where competent patients had
to get court orders to have their wishes honored; and cases like Quinlan and
Cruzan, the once-competent, currently incompetent patients, where the decision to
remove life-prolonging procedures was contested; and more recently, the cases of
Wendland and Schiavo, where the dispute was among the family members. (Mr.
Wendland was clearly minimally conscious. There was a dispute between the par-
ties about Mrs. Schiavo’s condition. Her husband/guardian took the position that
she was once-competent, currently incompetent, but her parents argued that she
was minimally conscious, or more accurately, severely disabled.)
51
By executing an advance directive, ambiguity can be reduced and conflicts be-
tween family members mitigated, although having an advance directive doesn’t
guarantee that there will be no dispute. Furthermore, physicians and hospitals
greatly prefer to have advance directives in place because it reduces for them the
challenges of having to negotiate with patients or family members about what the
expectations and intentions are. Because the law requires that hospitals offer pa-
tients information about advance directives at the time of admission, patients
cannot claim a lack of knowledge.
52
Advance directives also may specify a person’s wishes about participating in
experimental research regimens for his or her disease, or they may provide for
the donation of all or part of the person’s body for use by others, for scientific re-
search or for public display. For example, since 2000, a new technique called plas-
tization has made it possible for people to have their body preserved using a
polymer injection process and to be displayed for public or research uses.
Any advance directive can be easily modified or destroyed if a person changes
her mind. In fact, many attorneys recommend revisiting advance directive docu-
ments and preferences every couple of years, just as one might revisit one’s will or
trust documents. It is also recommended that these documents be shared openly
with family members, physicians, and one’s attorney so that everybody knows
where they are and what they say.
Advance directive are generally classified into the following categories of ac-
tion or documents:
• Health care surrogates or durable powers of attorney for health care
•Living wills

Health Decisions and Directives about the End of Life 529
• “Do not resuscitate” (DNR) orders
• Organ and tissue donations
The advance directive process can include express reference to how a person
wishes to have her body treated once she dies. This relates to intentions regarding
burial, cremation, and donation.
Health Care Surrogate or Durable Power of Attorney for Health Care Although living
wills may be the most familiar term associated with advance directives, they are
not necessarily the most important or even the most useful. Rather, the designa-
tion of another person who is legally authorized to make medical and health care
decisions can be far more valuable. These documents are called health care surro-
gates or durable powers of attorney for health care.
Each state has provisions that allow individuals to expressly name another
person to make decisions about their health care. The scope of the designation can
be very limited or very broad. It can refer to limited periods of incapacity, for ex-
ample, during surgery or anesthesia, when a person is not able to make decisions
for herself; or it can refer to periods following an accident or serious illness that
might occur in the future, during which a person is similarly incapacitated. It can
be a broad-based granting of authority in the event of general incapacity, either
physical or mental (i.e., dementia). It can refer to specific types of medical deci-
sions (such as surgery, administration of certain medications, experimental pro-
cedures), or it can reference authority to make decisions to withhold heroic
measures or technological means of maintaining life.
It is prudent for a person to make a primary and a secondary designation for
surrogacy. The primary designee will have the responsibility for making the spec-
ified decisions, but in the event that the primary is unable or unwilling to serve,
the secondary surrogate assumes the responsibility. Selecting the persons to
serve in these capacities is an important and serious decision. Some people feel
that they are obliged to name their eldest child or their spouse, even though they
will confide that they are not convinced that person would always make decisions
in their best interests.
Some people also wish to select more than one primary surrogate, forming a
team of decision makers. This has certain advantages when there may be a need
for caring loved ones to discuss the realistic options and come to a consensus for
the benefit of all. Multiple surrogates can also be valuable if more than one per-
son is named and either individual is empowered to make decisions. This has par-
ticular value when surrogates do not live near the patient, or when one is not
easily accessible during a time when a decision must be made.
But naming multiple surrogates can be an invitation to confusion and complex-
ity, especially if it is done for the purpose of avoiding bad feelings among family
members.
It is recommended that multiple, original, signed surrogacy documents be cre-
ated and that copies be provided to the patient’s primary care physician, attor-
ney, and those who will be named as surrogates. Often, documents are executed
and then placed in a safe deposit box or in an obscure drawer where nobody even
knows they exist. Once a person is incapacitated according to the terms of
the surrogacy and the state law, the document should be shared with physicians,

530 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
hospital personnel, and others so that there are no mistakes about the intentions
of the person. Many hospitals now encourage patients to formally file their surro-
gacy documents upon admission, even for simple procedures.
The surrogacy is considered by many to be the most important of the advance
directives because it formally, legally, and expressly places a person’s health de-
cisions under the responsibility of a specific person. It helps up front to elimi-
nate ambiguity and questions about who should make what kinds of decisions
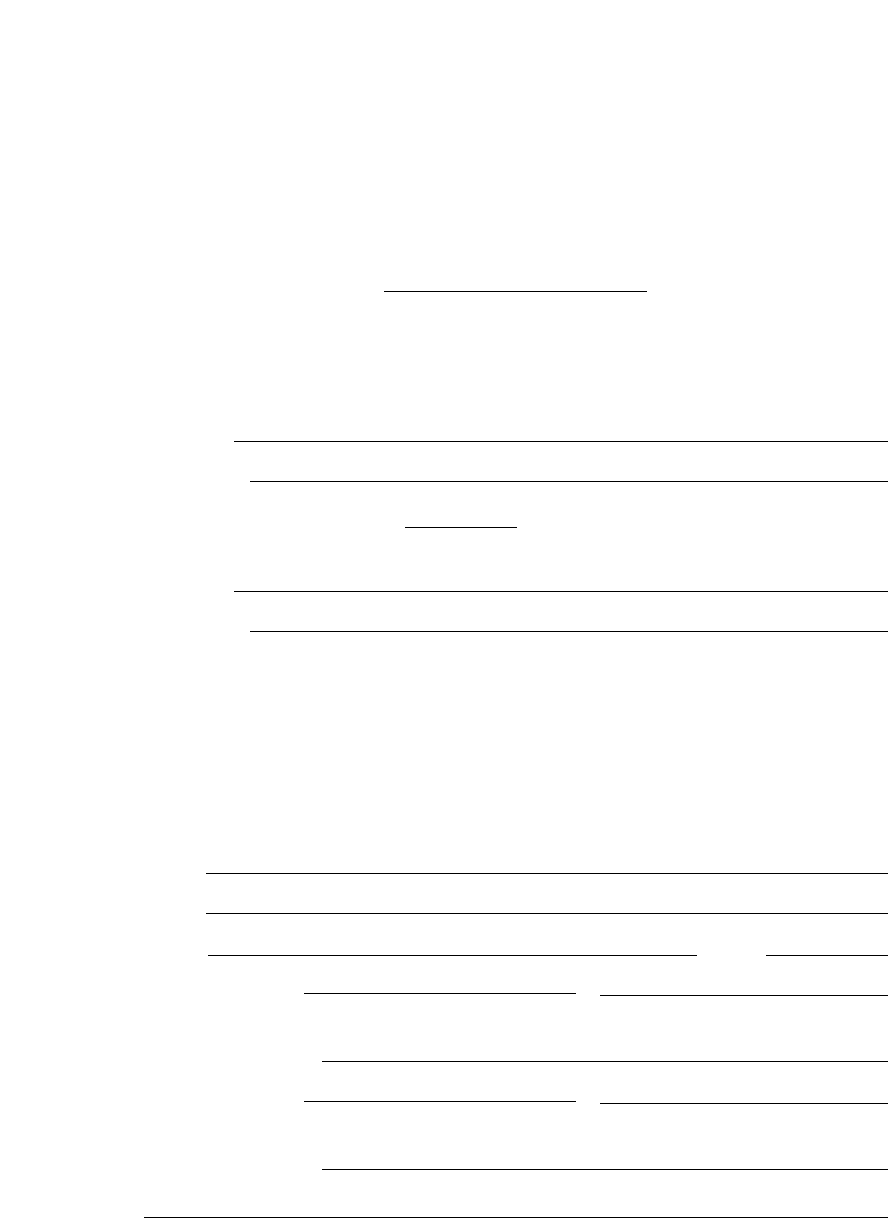
in the event of an incapacitating event. Figure 19.1 is an example of a surrogacy
document.
Living Wills Living Wills are probably the best-known form of advance direc-
tive, but they are not always the most useful or effective. Living wills are general
statements about how an individual wants to be treated in the event that a life-
threatening or terminal condition afflicts him. Living wills should generally be
used after a surrogacy document, and in the event that there arises a question
about what the person’s wishes really were about certain end-of-life issues.
Most states provide that individuals may choose to withhold or remove certain
medical care in the event of a terminal condition. “Terminal” refers to conditions
for which no reasonable medical recovery is likely, and include persistent vegeta-
tive state, dementia, and other conditions. Each state law should be consulted for
the specific conditions that apply. Often patients do not realize that their living will is
not effective unless those conditions are met.
Living wills allow individuals to state that they want to be kept alive at
all costs, regardless of their medical condition and regardless of the reasonable
likelihood of recovery. More commonly, however, the living will reflects a deci-
sion by an individual not to be kept alive in the event of certain conditions or
circumstances.
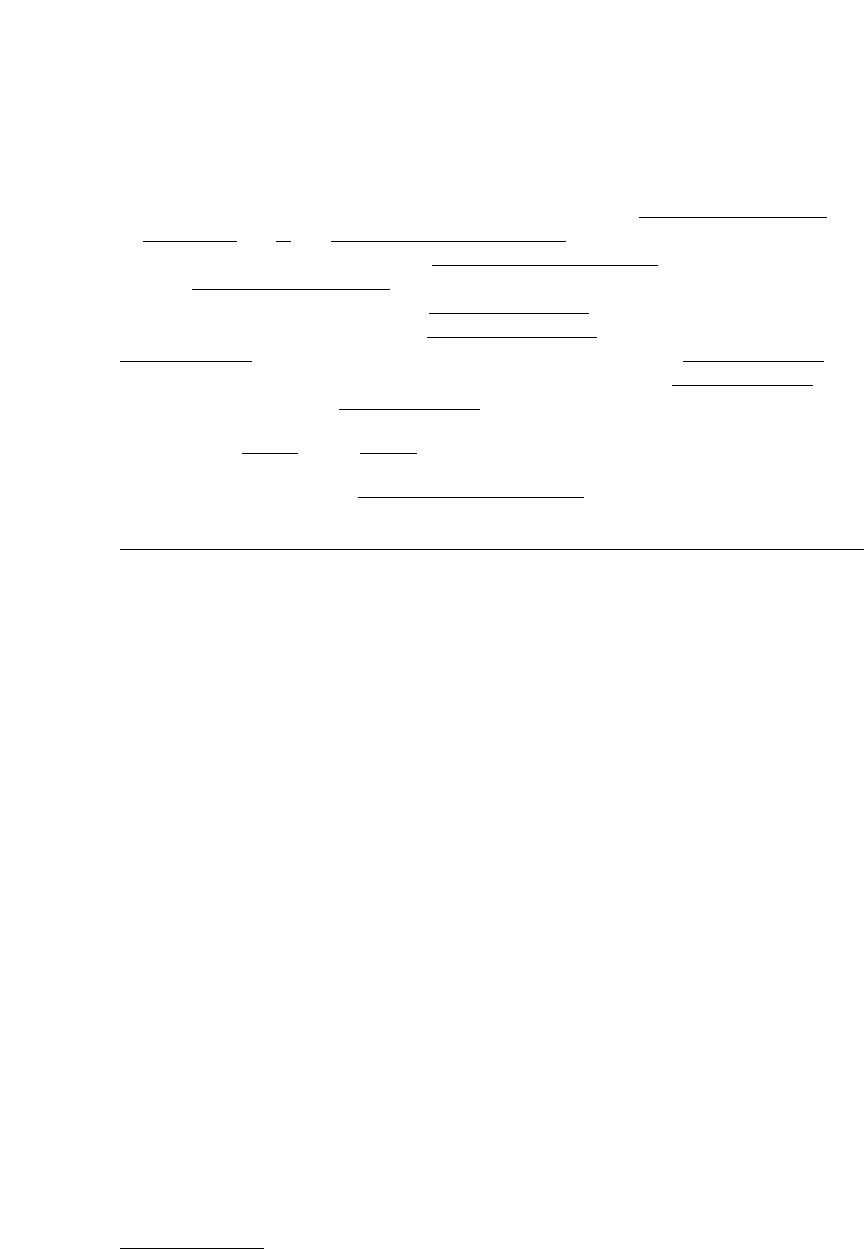
Figure 19.2 on page 533 is a sample living will document that provides a set of
options for the person executing the document. It is important to appreciate that
the living will should, to the extent possible, mirror the expected decisions that
the health care surrogate will be making on behalf of the incapacitated person.
Appointing a surrogate who will not uphold the intentions expressed in the liv-
ing will is an invitation for disaster and legal expense. The surrogate should be
fully familiar with the expectations in the living will and should be comfortable
carrying them out. If not, the wrong surrogate may have been chosen.
Physicians, nurses, and health care organizations are in the business of keep-
ing people alive and healthy as long as possible. Although physicians have not
tended to view themselves as agents participating in decisions to end life, tacit
understandings often existed between family members and physicians regarding
end-of-life decisions. They were just not announced or memorialized in writing.
When patients were very sick and in a terminal state, physicians would often let
them, if not help them, transition into a peaceful death.
Again, specificity is important to avoid ambiguity and controversy. The partic-
ular form of the living will document is also important. In most jurisdictions, it
must be signed, witnessed, and notarized. In some jurisdictions, it must follow a
particular format and reference state law. Not all jurisdictions will honor the liv-
ing will of another state. Persons who travel frequently or who have residences in
more than one state should determine how each state requires living will docu-
ments to be created.
531
STATE OF
FLORIDA
COUNTY OF HILLSBOROUGH
DESIGNATION OF HEALTH CARE SURROGATE
FOR
(Printed Name)
In the event that I have been determined to be incapacitated to provide informed
consent for medical treatment and diagnostic procedures, I wish to designate as my
surrogate for health care decisions, the following person, to act on my behalf:
Name:
Address:
In the event the above person,
, is unable or unwilling to serve as my
health care surrogate, I wish to designate the following person to act on my behalf:
Name:
Address:
I fully understand that this designation will permit my designee to make health care
decisions and to provide, withhold, or withdraw consent on my behalf; to apply for public
benefits to defray the cost of health care; and to authorize my admission to or transfer
from a health care facility.
I further affirm that this designation is not being made as a condition of treatment or
admission to a health care facility. I will notify and send a copy of this document to the
following persons other than my surrogate, so they may know who my surrogate is.
Name
Name
Signed Date
Witnesses: Name
Signature
Address
Name
Signature
Address
(continued)
Figure 19.1 Health Care Surrogate Template. Adapted from Florida Bar Templates,
http://www.floridabar.org/tfb/flabarwe.nsf/840090c16eedaf0085256b61000928dc
/b954f12053a410ec85256e28005bd4a0?OpenDocument.
532 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
STATE OF FLORIDA
COUNTY OF HILLSBOROUGH
The foregoing instrument was acknowledged before me this
day
of
200 , by who is personally known to me or
who has produced Florida State or
State Driver’s License,
Number
as identification and who did take an oath, and that the
affiant’s signature was witnessed by
who is personally known to me or
who has produced a Florida State or
State Driver’s License, Number
as identification and who did take an oath and by who
is personally known to me or who has produced a Florida State or
State
Driver’s License, Number as identification and who did take an oath.
Executed this
day of 200_.
Seal
My commission expires:
Figure 19.1
(Continued)
53
See for example, The Living Will Registry line at http://www.uslivingwillregistry.com.
54
www.agingwithdignity.org.
No legal document regarding a person’s life or health should be signed without
carefully considering the implications of that document and without consulting
family and loved ones. Executing a health care surrogate or a living will without
telling anybody about them is likely to create controversy and chaos. There are a
variety of commercial and not-for-profit options that are available for people to
use as repositories for their surrogate and living will documents. While a per-
sonal attorney, trust banker or friend/relative can serve as the holder of the docu-
ment, some may prefer another third party.
53
The Living Will Registry is a private company that seeks to provide national
virtual storage and access services for persons who wish to file their living will
documents in a central repository. But somebody still needs to know that you
have located your document with their service.
Some jurisdictions will accept video statements of intent regarding health care
surrogates and living wills. Some jurisdictions will accept verbal, unwritten evi-
dence of a person’s intent, usually subject to a hearing and the presentation of ev-
idence. But to avoid confusion and ambiguity, written, signed, witnessed, and
notarized documents are the only reasonable assurance that a person’s intentions
will be carried out.
The Robert Wood Johnson Foundation has funded the development and distri-
bution of a the Five Wishes program, which is administered by Aging with Dig-
nity, a Florida organization. Five Wishes is a document that offers a stepwise
approach to helping people and their families ask and answer questions about
end-of-life decisions.
54
The categories of issues addressed in the Five Wishes doc-
ument include who will make decisions, the kind of care and treatment to be pro-
vided, the level of comfort or relative pain a person agrees to experience, and
533
LIVING WILL DECLARATION
(Printed Name)
I,
voluntarily make this declaration on 200_ . I recognize that death
is natural and is but a phase of the cycle of life. I do not fear death as much as I fear the
indignity and futility of deterioration, dependence and hopeless pain. If there is no
reasonable medical expectation of my recovery from a physical or mental disability, I do
not wish to be kept alive by artificial means or heroic measures.
Therefore, if my attending or treating physician and another consulting physician
determine that there is no reasonable medical probability of my recovery from any of the
following conditions, I direct that life-prolonging procedures be withheld or withdrawn
when the application of those procedures would serve only to prolong artificially the
process of dying, and that I be permitted to die naturally with only the administration of
medication or the performance of any medical procedure deemed necessary to provide
me with comfort care or to alleviate pain, even if it hastens my death:
• I have a terminal condition caused by injury, disease or illness from which there is
no reasonable medical probability of recovery and which can be expected to cause
my death if not treated;
• I am in an irreversible end-stage condition that is caused by injury, disease or
illness that has resulted in severe and permanent deterioration, indicated by my
incapacity and complete physical dependency, for which treatment would be
medically ineffective to a reasonable degree of medical certainty;
• I am in a persistent or permanent vegetative state characterized by permanent and
irreversible unconsciousness and/or brain injury in which there is an absence of
voluntary action or cognitive behavior of any kind by me, with an inability to
communicate or interact purposefully with others in the environment around me.
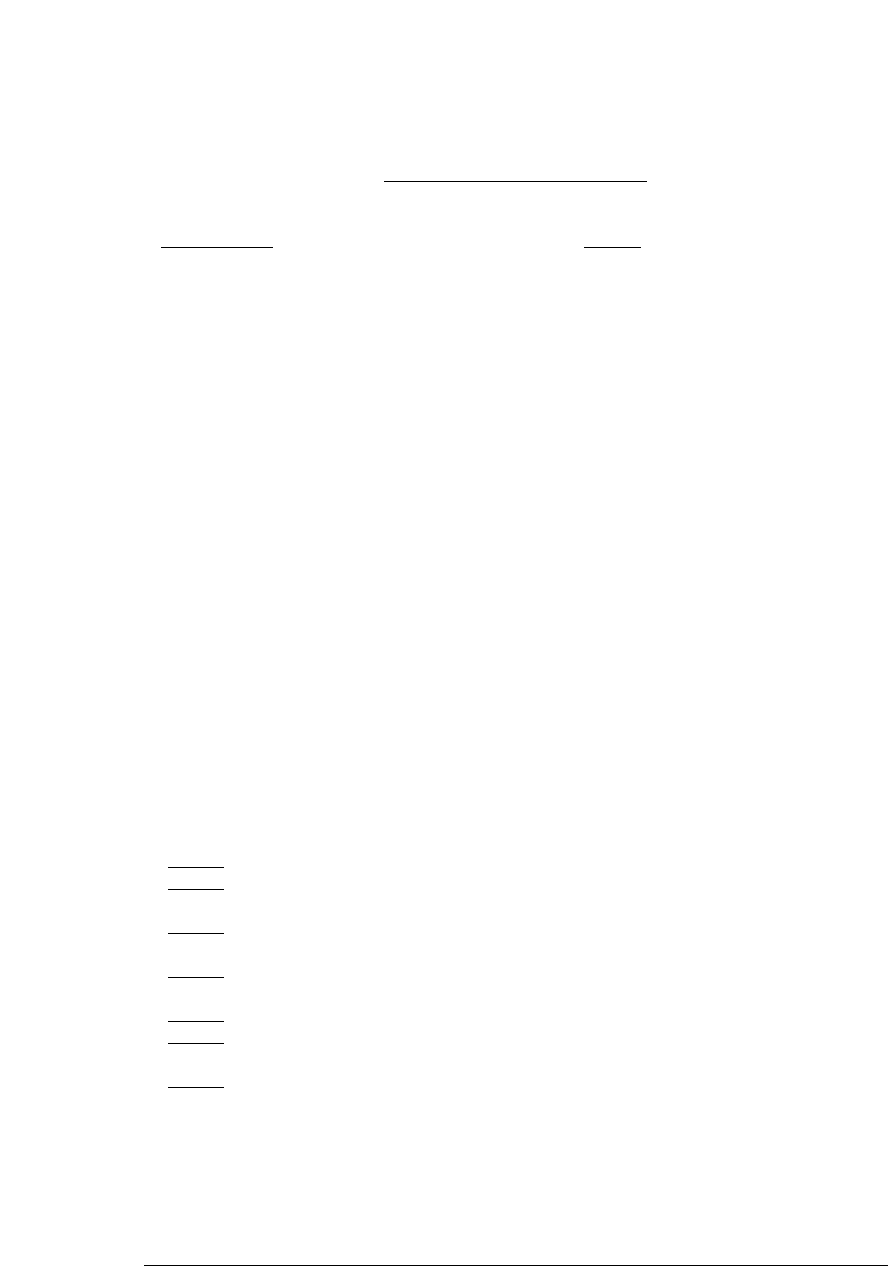
In any of the situations described above, I direct that the following medical interventions
that I have initialed be considered life prolonging procedures which I hereby direct not
be administered to me:
Placement on ventilator or other mechanical devices
Surgical procedures and blood transfusions, except as needed to prevent or
alleviate suffering
Placement in an intensive care unit except as an absolute necessity to
relieve suffering
Chemotherapy or radiation therapy, unless there is a substantial medical
probability my condition will materially improve
Resuscitation efforts in the event of arrest of my heart or breathing
Active treatment of a new reversible condition, such as a newly discovered
cancer, heart condition or pneumonia
Artificial nutrition and hydration (providing food and water through tubes)
I intend that this declaration be honored by my family and my physicians and health care
institutions as the final expression of my legal right to refuse medical or surgical
treatment or care and to accept the consequences for such refusal. I understand that my
wishes may place a heavy burden upon others, and so I make this declaration to
assume sole responsibility for my decision and to mitigate any feelings of guilt that my
wishes may cause.
(continued)
Figure 19.2 Living Will Template.
I am emotionally and mentally competent to make this declaration, and I understand its
importance.
200
This declaration is witnessed by us in the presence of the declarant:
Witness Witness
Address Address
Telephone Telephone
State of Florida /
/
County of Hillsborough /
/
The foregoing instrument was acknowledged before me this
day
of
200 by , who is personally known to me, and was witnessed
by
, who is personally known to me or produced a valid Florida Driver’s
License, and by
, who is personally known to me or produced a valid
Florida Driver’s License, after all of them did take an oath.
Notary Public
State of Florida
Figure 19.2 (
Continued)
what and when people should be told about them when they are going to die.
55
The 11-page document can be acquired through www.agingwithdignity.org.
E
THICS
C
ONSULTS
Both the Quinlan and Browning courts developed frameworks for deciding end-of-
life cases outside of court intervention. Many times, a hospital ethics committee
is involved in the review of the case and the proposed course of action. A hospital
ethics committee is usually an interdisciplinary committee that looks at the case
from a number of different perspectives, including, as the name implies, an ethi-
cal perspective.
56
This consultative body can provide guidance, make sure all the
right questions have been asked, and affirm the appropriateness of a particular
course of action. Ethics committees are generally composed of physicians, nurses,
nonclinical persons, and often a clergy member, and at least one member of the
534 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
55
Id.
56
See an example of an ethics committee handbook, the University of Kansas Medical Center, at
http://www.kumc.edu/hospital/ethics/ethics.htm.

57
See, for example, Florida Administrative Code 64E-2.031 and Florida Statutes, 401.45(3)(a).
58
See, for example, Will Doctors and Hospitals Recognize My Advanced Directive? http://www.abanet
.org/publiced/practical/directive_recognition.html.
Health Decisions and Directives about the End of Life 535
committee is trained in medical ethical decision-making issues and processes.
The purpose of the ethics committee is to place a variety of complicated clinical
decisions about care, treatment, death, and dying within a well-balanced, orderly
process. The entire palliative care movement to assure a comfortable, humane,
and desirable (by the patient) end of life has been one of the vital forces behind
the creation and operation of hospital ethics committees (Fins, 2005).
Do Not Resuscitate Orders Do not resuscitate (DNR) orders are formal medical or-
ders issued by a physician that carry instructions about resuscitating the patient.
There are two types of DNR orders: the in-hospital DNR order, which is entered
in the patient’s chart, and the out-of-hospital DNR order. Generally, the latter re-
lates to resuscitation in the event of an accident or a heart attack, stroke, or other
sudden threat to life that occurs outside of the hospital. Physicians will issue a
DNR order upon the request of a patient and after counseling if the patient suf-
fers from chronic, terminal, and life-threatening conditions and the patient does
not wish to prolong her life in a possible coma or vegetative state or in profound
disability. Such orders are agreed to between the physician and the patient and
signed by the physician.
57
The order is formally recorded in the patient’s medical
record. It should also be posted in an obvious place in the patient’s home, such as
on the refrigerator, and it can also be worn on a medical alert bracelet or necklace
to alert emergency medical personnel.
The DNR order is a serious and important document that, unlike other advance
directives, requires a physician’s formal prescription. Enforcing the DNR order can
sometimes be tricky, because the nature and severity of a potential life-threatening
event can be a subjective matter. During an emergency, for example, well-meaning
and well trained clinicians or others may automatically seek to provide CPR or
some other life-saving function because they are not aware of the DNR order, be-
cause they don’t believe that the event is sufficiently serious to cause potential
long-term adverse effects, or sometimes because they do not support the idea of a
DNR order. Some states have statutes or regulations that specifically address the
out-of-hospital DNR order. Some require that the order be on a specific color of
paper and have specific language and other requirements. In those states, a DNR
direction contained in a patient’s advance directive is not effective.
When an advance directive or the patient’s wishes are not honored because a
caregiver or health care provider refuses to honor the directive or disagrees
with the patient’s wishes, this can create a set of clinical, legal, and ethical
dilemmas. Directives may not be honored for a number of reasons: there may be
no knowledge of the directive’s existence; a traveling patient may have left the
directive at home; or the health care provider disagrees with the patient’s direc-
tions.
58
Advance directive statutes generally contain conscientious objector
clauses, which allow the health care provider to transfer the patient to another
health care provider if the original provider disagrees with the patient’s deci-
sion to refuse life-prolonging procedures on conscientious grounds (such as
religious or moral beliefs). Beyond those clauses, a caregiver or health care