Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 101 • Superfi cial Inguinal Node Dissection 1125
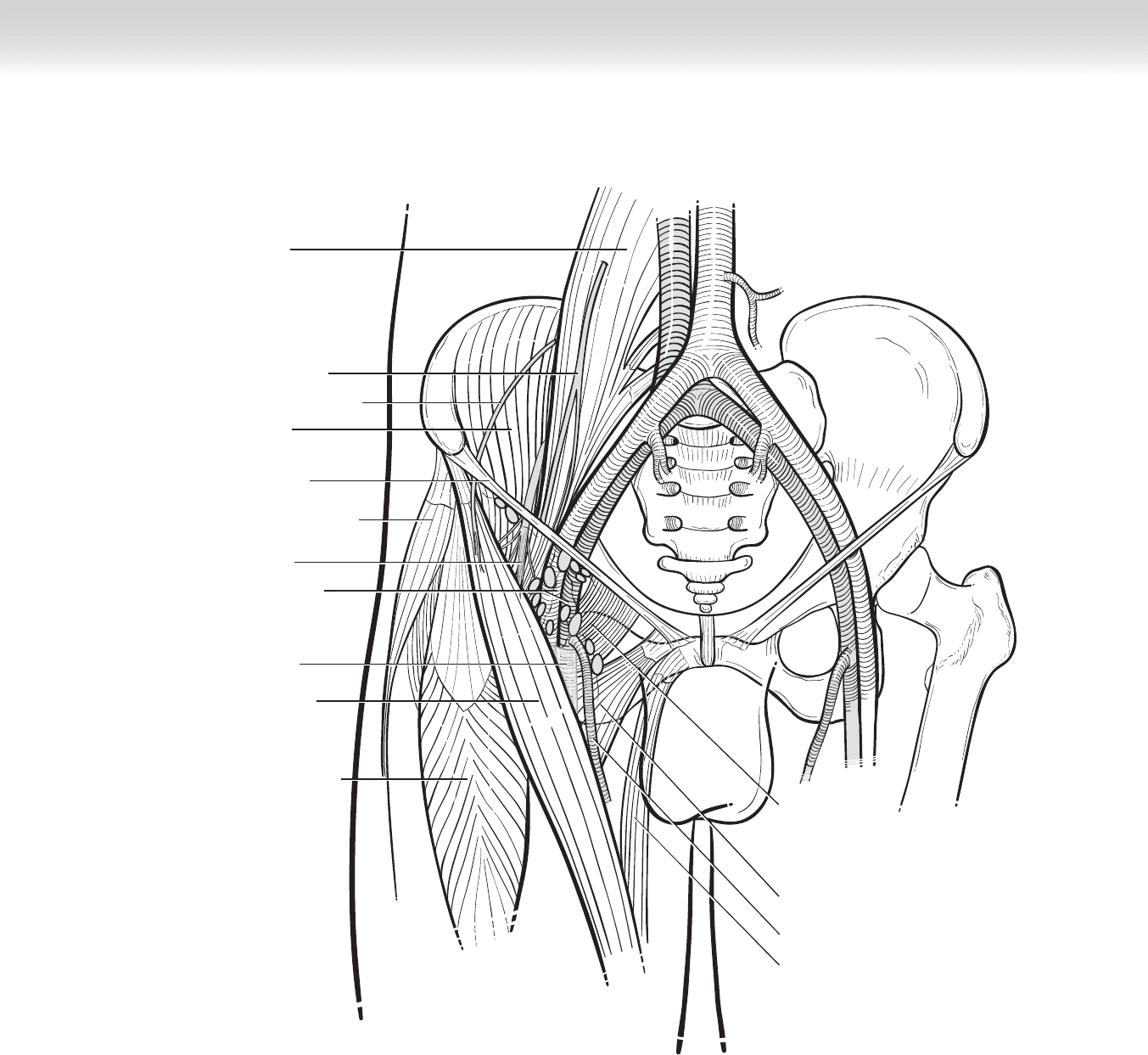
Rectus femoris muscle
Adductor longus muscle
Pectineus muscle
Inguinal ligament
Iliacus muscle
Genitofemoral nerve
Lateral femoral cutaneous
nerve
Psoas muscle
Tensor fasciae latae muscle
Femoral nerve
Femoral artery and vein
Sartorius muscle
Femoral sheath
Gracilis muscle
Great saphenous vein
FIGURE 101–3

1126 Section XV • Miscellaneous Procedures
2. DISSECTION
◆ Electrocautery is used to dissect down to subcutaneous tissue. Medial and lateral skin fl aps
are created. Superiorly, the skin fl aps should be thinner because nodal-bearing tissue may
be more superfi cial; as the dissection moves inferiorly toward the midthigh, the fl ap can
become thicker. The medial aspect of the dissection extends to the pubic tubercle and
extends laterally to include the entire length of the inguinal ligament. The boundaries of the
dissection include the medial border of the adductor magnus muscle and the lateral border
of the sartorius muscle.
◆ All fatty tissues, which include lymph node–bearing tissue (see Figure 101-1) both above
and below the inguinal ligament, down to the external oblique fascia and the inguinal liga-
ment are swept inferiorly. Medially, fatty nodal tissue is refl ected away from the spermatic
cord or round ligament, and all tissues overlying the femoral vessels, including the femoral
sheath, are carefully dissected en bloc into the specimen. Laterally, tissue anterior to the sar-
torius fascia are swept toward the specimen. Distally, as the saphenous vein dives behind
the sartorius muscle at the apex of the femoral triangle, the vein is divided (approximately
4 cm beyond the saphenofemoral junction). The tissue is swept superiorly until the fora-
men ovalis is encountered. Using a right-angled clamp, the surgeon ligates the saphenous
vein at the saphenofemoral junction and secures the vein with a 2-0 silk ligature. Posteri-
orly, the limits of dissection include tissue anterior to the fascia of the adductor muscles and
pectineus.
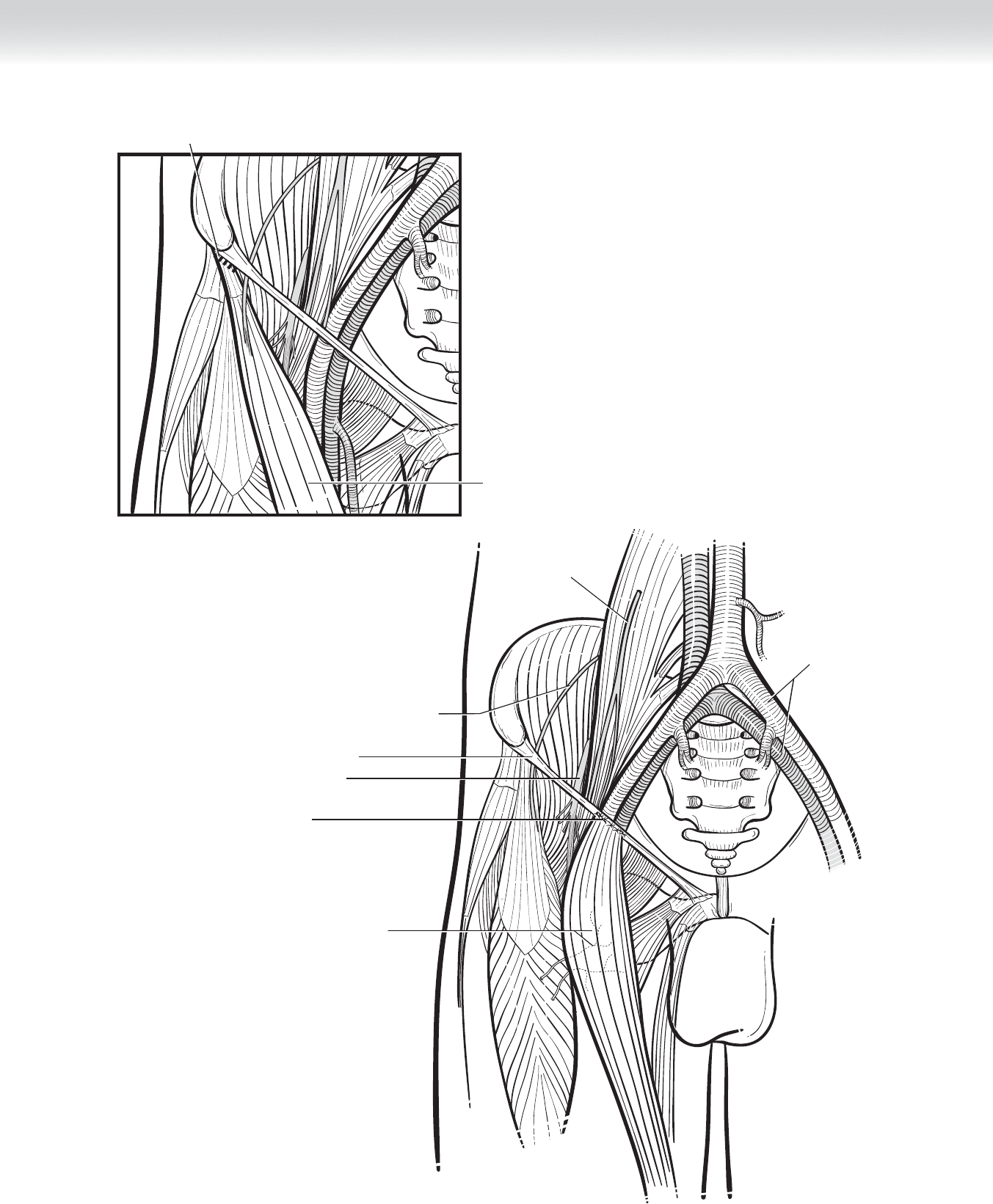
◆ The origin of the sartorius is identifi ed and divided off the anterior superior iliac spine.
The sartorius muscle is mobilized medially and transposed to cover the femoral vessels
(Figures 101-4 and 101-5). The lateral femoral cutaneous nerve arises underneath the lat-
eral aspect of the inguinal ligament and extends obliquely over the origin of the sartorius.
Care should be taken to identify and preserve this sensory nerve to the lateral thigh. Blood
vessels entering the sartorius muscle are preserved as the muscle is mobilized medially to
cover the exposed femoral vessels in a tension-free manner. The proximal aspect of the
muscle has to be rotated for the coverage to be tension free. The tendinous end of the mus-
cle is sutured to the inguinal ligament with 3-0 absorbable sutures using interrupted verti-
cal mattress stitches. The sartorius muscle will protect the femoral vessels from exposure
and subsequent bleeding, in case of skin edge necrosis, wound infection, and tissue break-
down, especially after adjuvant radiotherapy.
3. CLOSING
◆ The wound is irrigated and two closed-suction drains are placed, one exiting medially and
one exiting laterally. If the blood supply to the skin edges appears marginal, the edges
should be trimmed back to healthy tissue. The incision is closed in two layers. The deeper
fascial layer is reapproximated with 2-0 or 3-0 interrupted absorbable sutures, and the skin
can be closed using skin staples.
CHAPTER 101 • Superfi cial Inguinal Node Dissection 1127
Sartorius
muscle
Incision line
FIGURE 101–4
Inguinal ligament
Lateral femoral cutaneous nerve
Genitofemoral nerve
External iliac vessels
Sutures
Femoral nerve
Sartorius muscle and
blood supply
FIGURE 101–5

1128 Section XV • Miscellaneous Procedures
STEP 4: POSTOPERATIVE CARE
◆ Postoperatively, the patient may ambulate with elastic support on the leg, as tolerated. How-
ever, when the patient is at rest, the extremity should be elevated to decrease limb edema.
The drains can be removed when the drainage decreases to 30 mL or less per 24 hours.
◆ Lymphedema can occur in more than 50% of patients who have undergone superfi cial
lymph node dissection. Prophylactic measures, such as elevating the leg and wearing
elastic stockings, are important means to decrease the severity and incidence of this
potential complication.
STEP 5: PEARLS AND PITFALLS
◆ The most common acute postoperative complication is cellulitis and/or wound infection.
Although prophylactic preoperative antibiotics are recommended, the infection rates can
range up to 30%.
◆ The rate of lymphocele or seroma formation ranges from 3% to 23%. The use of closed-
suction drains for a longer period of time can decrease the incidence of fl uid formation
under the fl aps; however, prolonged use has to be balanced with the increased potential for
wound infection.
◆ The incidence of extremity lymphedema can be decreased with the use of elastic stockings,
limb elevation, and exercise.
◆ The incidence of thromboembolic events, such as deep vein thrombosis and pulmonary
embolus, was reported to be 13.6% in a study of patients who underwent inguinal node
dissection for melanoma. Prophylaxis with intermittent pneumatic compression devices and
low-dose anticoagulants may minimize this complication.
SELECTED REFERENCES
1. Karakousis CP, Heiser MA, Moore RH: Lymphedema after groin dissection. Am J Surg 1983;145:205-208.
2. Arbeit JM, Lowry SF, Line BR, et al: Deep venous thromboembolism in patients undergoing inguinal
lymph node dissection for melanoma. Ann Surg 1981;194:648-655.
3. Johnson TM, Sondak VK, Bichakjian CK, et al: The role of sentinel node biopsy for melanoma: evidence
assessment. J Am Acad Dermatol 2006;54:19-27.
4. Health Care Center for the Homeless. Available on the Internet: www.hcch.org
1129
STEP 1: SURGICAL ANATOMY
◆ The left kidney is most commonly procured for live donor kidney transplantation because of
its longer vein and greater ease of access. However, given the basic tenet of live kidney dona-
tion, “leaving the best kidney in the donor,” the donor surgeon should be familiar with right
and left donor nephrectomy. There are many donor nephrectomy surgical techniques available
and include pure laparoscopic; hand-assisted laparoscopic; robot-assisted pure laparoscopic;
robot-assisted and hand-assisted, using either a transabdominal or retroperitoneal approach;
and of course, open nephrectomy. The donor surgeon and operating room should be equipped
to convert from a laparoscopic to an open approach at short notice. Regardless of technique
used, understanding the three-dimensional relationships of both kidneys is essential.
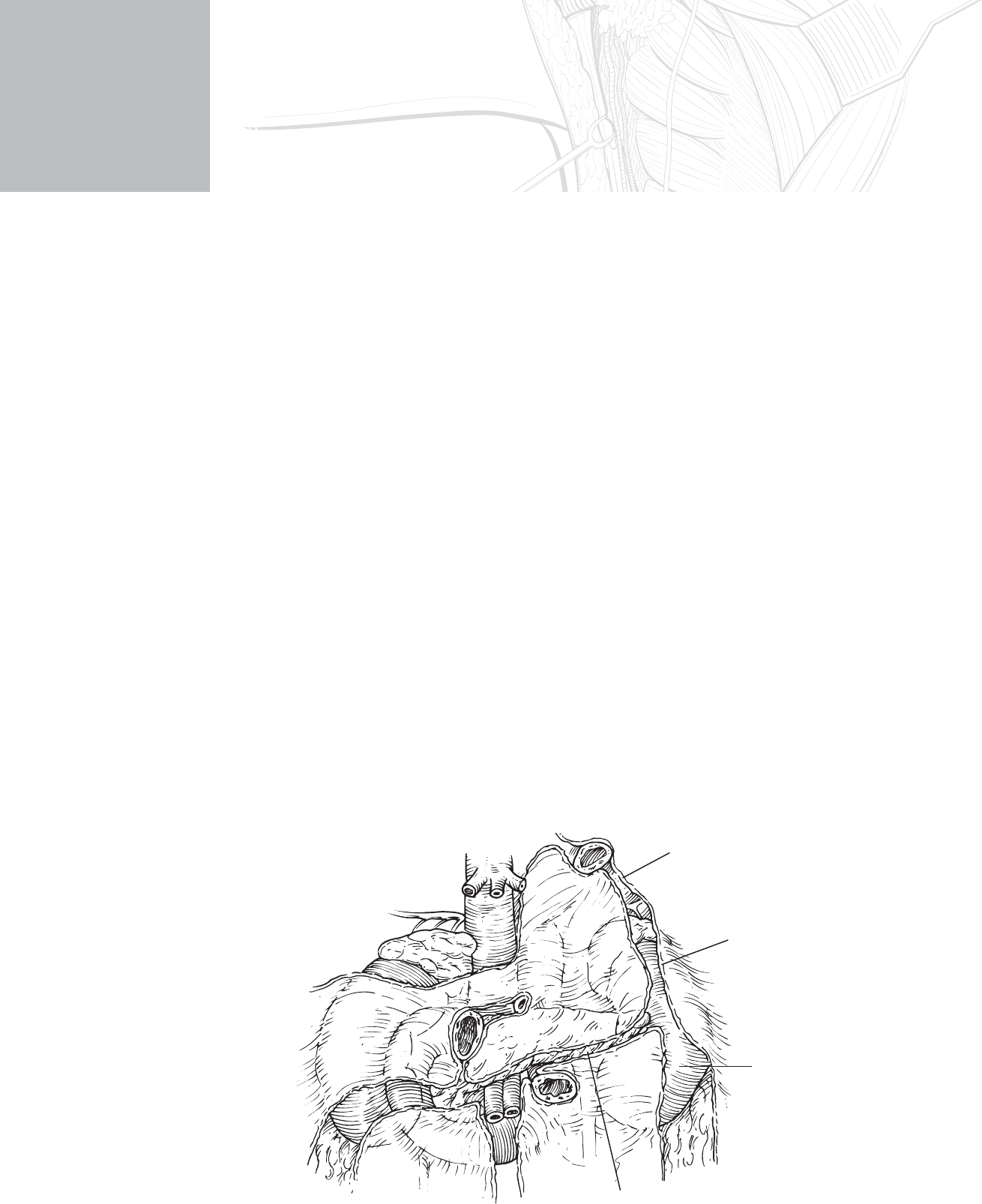
◆ Figure 102-1 illustrates some of the important anterior relationships of the right and left kid-
ney. Both kidneys are positioned high up in the retroperitoneum under cover of the costal mar-
gin. The body of the kidney is oriented obliquely on the diaphragm and quadratus lumborum
muscle in the long axis of the psoas. The hilum of the kidney and its contents are angled for-
ward. Although the position of the kidneys is altered with movement of the diaphragm, the
hilum of the right kidney (pushed down by the liver) lies just below the level of the transpylo-
ric plane, whereas that of the left kidney lies just above the level of the transpyloric plane,
approximately 5 cm from the midline. With such intimate association with the pancreas and
duodenum, it is easy to see how injuries can occur.
CHAPTER
102
Donor Nephrectomy
Jacqueline A. Lappin
Gastrosplenic
ligament
Lienorenal
ligament
Area for
splenic flexure
Transverse
mesocolon
FIGURE 102 –1

1130 Section XV • Miscellaneous Procedures
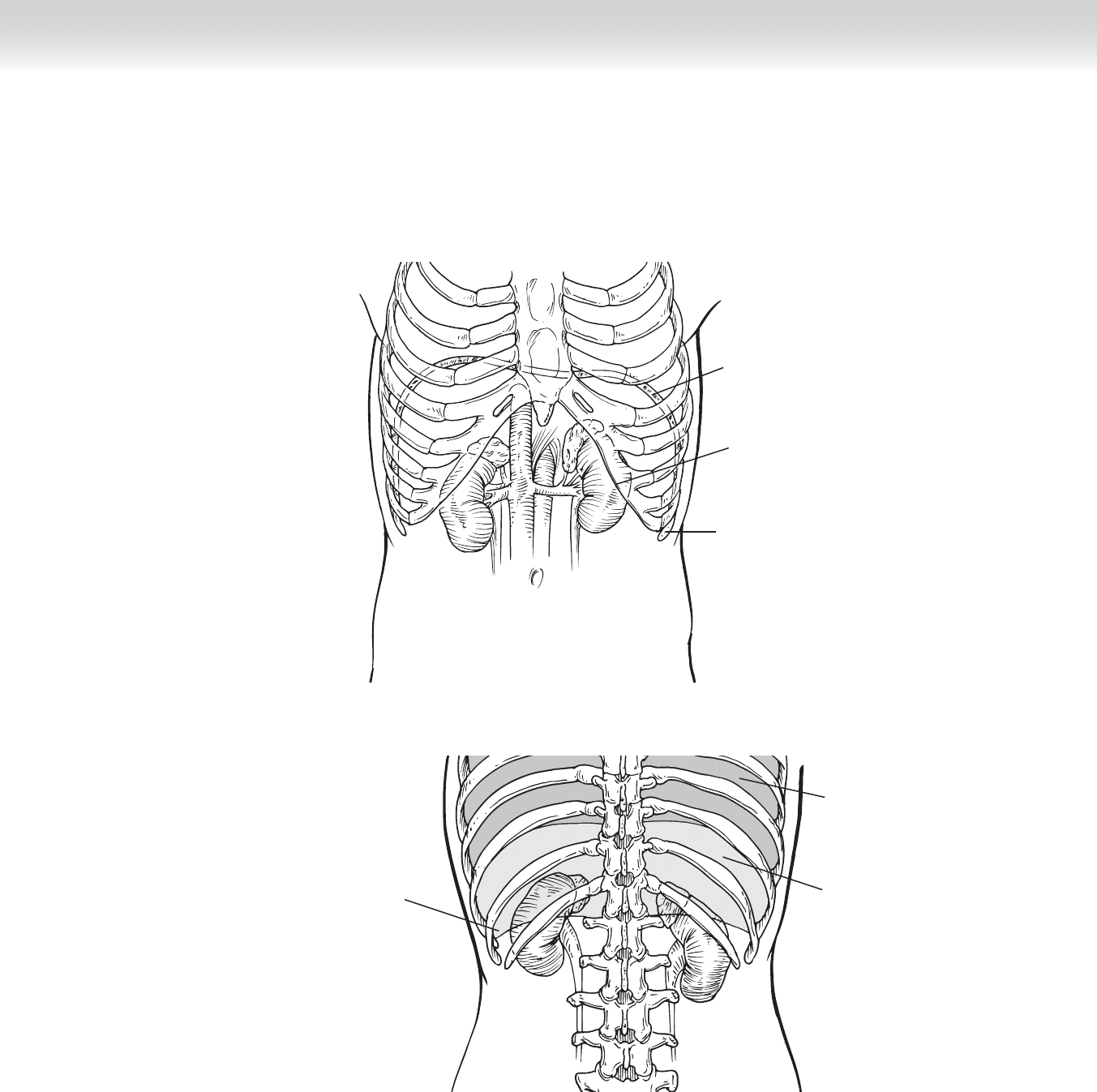
◆ Figure 102-2, A (anterior view) and Figure 102-2, B (posterior view) illustrate the rela-
tionship of each kidney to the pleura and rib cage. The parietal pleura reaches all the way
down to the spinous process of the 12th vertebra posteriorly and the 10th rib in the mid-
axillary line. This relationship becomes more important with a posterior approach to the
kidney.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Each kidney donor must undergo an extensive examination to determine physiologic,
psychological, immunologic, and anatomic suitability.
◆ The best kidney must be left in the donor.
◆ Surgical experience of the donor team will determine the surgical technique used in each
individual case.
◆ A preoperative bowel preparation, although not essential, can facilitate intraoperative and
postoperative management of the donor.
◆ Care should be taken to prevent dehydration of the donor as is apt to occur with preopera-
tive imaging, bowel preparation, and travel from out of town.
◆ Although donor evaluation is similar for both open and laparoscopic nephrectomy, it is
important to be familiar with the sensitivities and specifi cities of preoperative imaging
techniques used in your facility.
CHAPTER 102 • Donor Nephrectomy 1131
Diaphragm
Anterior View
Costal
margin
11th rib
A
FIGURE 102 –2
Lung
Pleura
Partial pleura
lower edge
B
Posterior View
1132 Section XV • Miscellaneous Procedures
STEP 3: OPERATIVE STEPS
LAPAROSCOPIC TRANSABDOMINAL LEFT DONOR NEPHRECTOMY
◆ What follows is a description of a laparoscopic transabdominal left donor nephrectomy.
Differences in technique for pure laparoscopic and hand-assisted approaches are described.
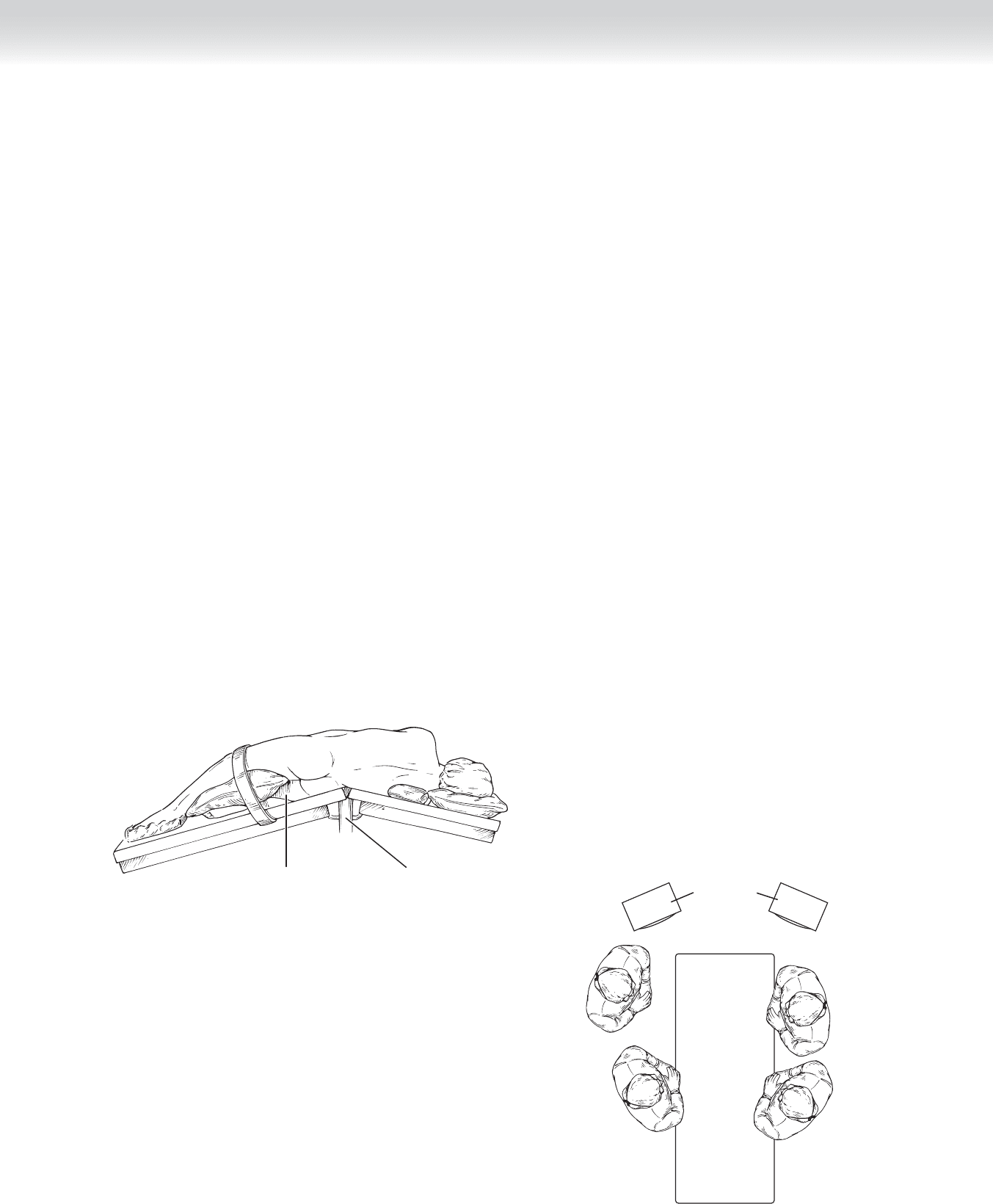
◆ Position of the patient is shown in Figure 102-3. An alternate position is supine with rota-
tion toward a right lateral decubitus position. Addition of Trendelenburg can also be helpful.
◆ After induction of general anesthesia, preoperative antibiotics are given; an orogastric tube
and Foley catheter are placed. Thromboembolic-deterrent (TED) stockings and sequential
compression devices are applied to the lower extremities. The patient is carefully positioned
in a modifi ed lateral decubitus position with the hips rotated posteriorly. An axillary roll is
placed and the arms are fl exed at the elbow and padded. A second roll is placed between
the patient’s knees with the lower limb fl exed at the knee. The kidney rest is elevated and
the patient is secured. Additional padded support may be applied to the patient’s right
shoulder, lower abdomen, and buttocks to facilitate intraoperative rotation of the table.
◆ The position of all the participants are illustrated (Figure 102-4). The surgeon stands on
the right side of the patient, and the camera operator, more caudad. The scrub nurse and
additional assistant stand on the patient’s left side. There are two video towers placed at the
top of the table on either side of the patient.
Lower limb flexed
The kidney rest
FIGURE 102 –3
Video tower
Head
Assistant
Scrub nurse
Feet
Camera
operator
Surgeon
Right Left
FIGURE 102 –4
CHAPTER 102 • Donor Nephrectomy 1133
1. INCISION
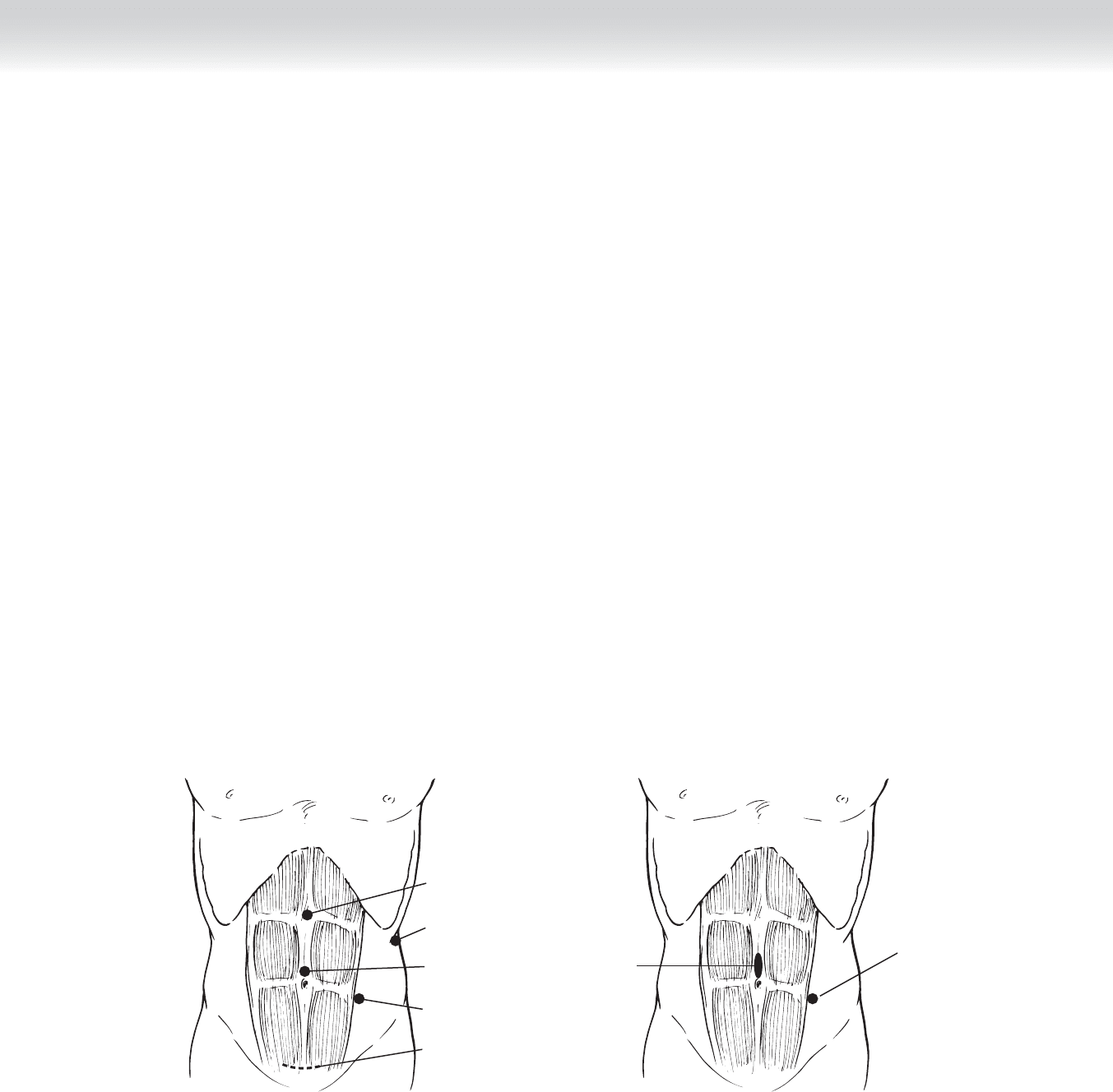
◆ Placement of trochars is shown in Figure 102-5. There are, however, many variations for
trochar and hand-port placement.
◆ Before placement of the pneumoperitoneum, the abdomen is marked for placement of tro-
chars and extraction incision. Each port site is infi ltrated with local anesthesic, which can
facilitate a reduction in narcotic use postoperatively. The ports are placed as illustrated. A
10- or 12-mm port that is primarily used for dissection is placed at the level of the umbili-
cus, a second 10- or 12-mm camera port is placed lateral to the rectus muscle, halfway
between the umbilicus and the anterior superior iliac spine. Transillumination of the abdo-
men can be used to prevent injury to the inferior epigastric artery with this latter trochar
placement. A third 5-mm port is placed in the midline, halfway between the umbilicus and
the xiphoid process, and a fourth 5-mm port can be placed in the fl ank for retraction. As
the operation progresses, the camera port and dissection ports can be interchanged to
obtain optimal exposure. Once the pneumoperitoneum is established, the zero-degree lens
camera is replaced with a 30-degree angled scope.
◆ For hand-assisted laparoscopic left nephrectomy, the umbilical port is lengthened in the
midline to facilitate placement of a pneumatic cuff or GelPort (Figure 102-6). At least two
laparotomy sponges can be introduced at this time.
5-mm port
(dissection port)
10-/12-mm port
(dissection port)
10-/12-mm port
(camera port)
Extraction
incision marked
Optional additional
flank port
FIGURE 102 –5
For hand
assist
10-/12-mm port
FIGURE 102 –6
1134 Section XV • Miscellaneous Procedures
2. DISSECTION
◆ The Harmonic scalpel or Bovie electrocautery, or both, can be used for the dissection. Be-
cause pneumoperitoneum affects renal blood fl ow, a pneumoperitoneum of 12 to 14 mm Hg
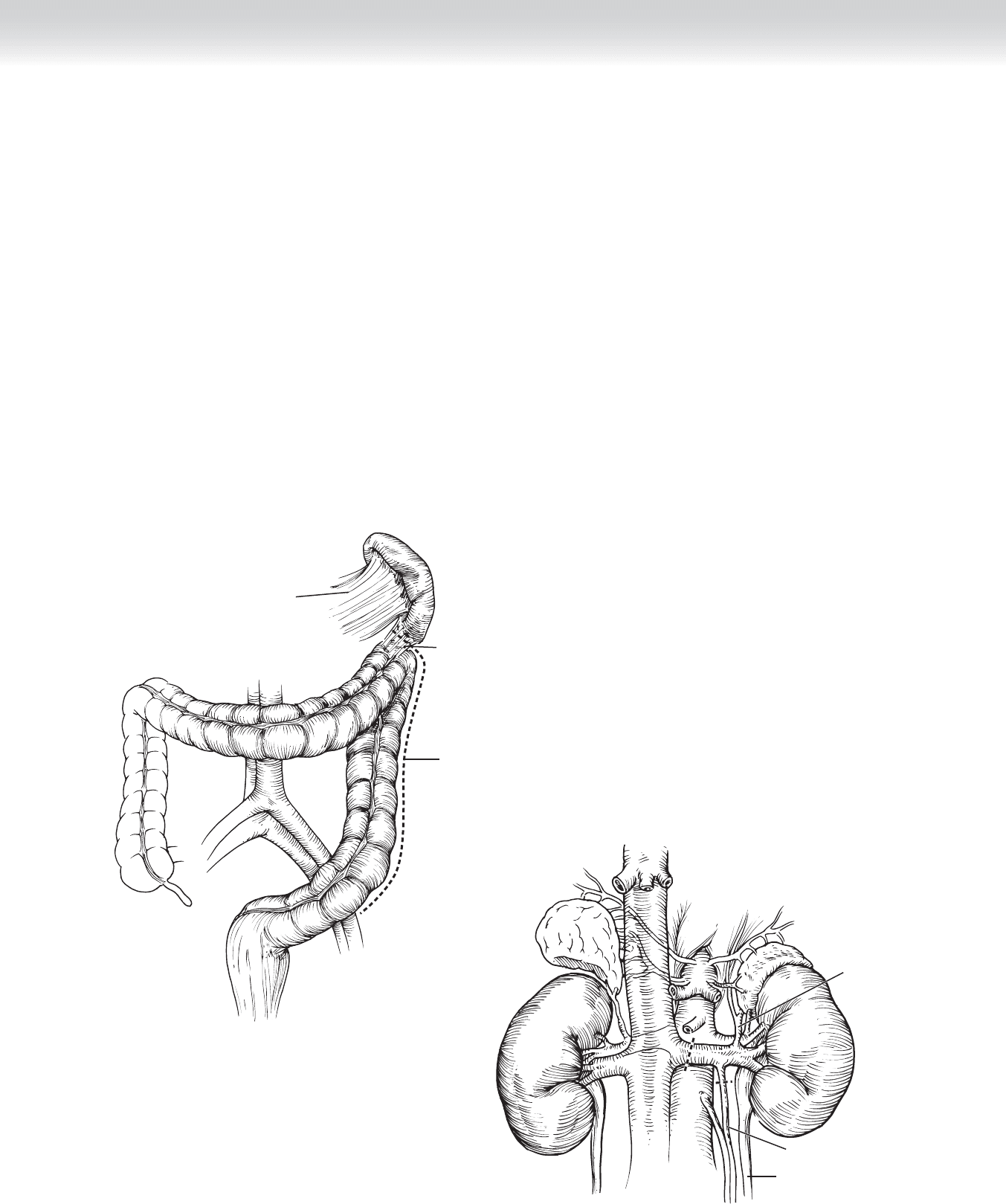
is maintained. The dissection proceeds with an incision placed along the white line of Toldt.
This is extended superiorly to include takedown of the splenocolic and lienorenal ligaments
and inferiorly to the sigmoid colon and iliac vessels (Figure 102-7). The superior and lateral
attachments of the kidney helps suspend and fi x the kidney to facilitate hilar dissection. The
analogy of taking the sheet off the bed has been used to describe this refl ection of the colon
medially to expose Gerota’s fascia and the kidney. As with open surgery, maintaining the cor-
rect plane is essential. There is a perceptible difference in the appearance of the mesenteric
and retroperitoneal fat (mesenteric fat is a brighter yellow).
◆ Next, the gonadal vein is identifi ed and traced superiorly to the renal vein, which is then
dissected out (Figure 102-8).
Lienorenal
ligament
Splenocolic
ligament
White line
of Toldt
FIGURE 102 –7
Adrenal
vein
Gonadal vein
Ureter
FIGURE 102 –8