Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 103 • Skin Graft—Split Thickness and Full Thickness 1155
STEP 4: POSTOPERATIVE CARE
◆ Wounds that result from decompression should be kept moist and wrapped with the burn.
Elevation should be routine to help decrease edema whenever possible.
STEP 5: PEARLS AND PITFALLS
◆ Keep in mind that all circumferential burns do not need to have decompression.
◆ In a moderate burn with an awake patient, you can follow closely with a clinical
examination.
SELECTED REFERENCES
1. Herndon DN: Total Burn Care. London, Saunders, 2002.
2. Barret JP, Herndon DN: Color Atlas of Burn Care. London, Saunders, 2001.
3. Sood R, Achauer BM: Achauer and Sood’s Burn Surgery: Reconstruction and Rehabilitation. Philadelphia,
Elsevier, 2006.
4. Green DP, Hotchkiss RN, Pederson WC, Wolfe S: Green’s Operative Hand Surgery, 5th ed. Amsterdam,
Elsevier, 2005.

1158
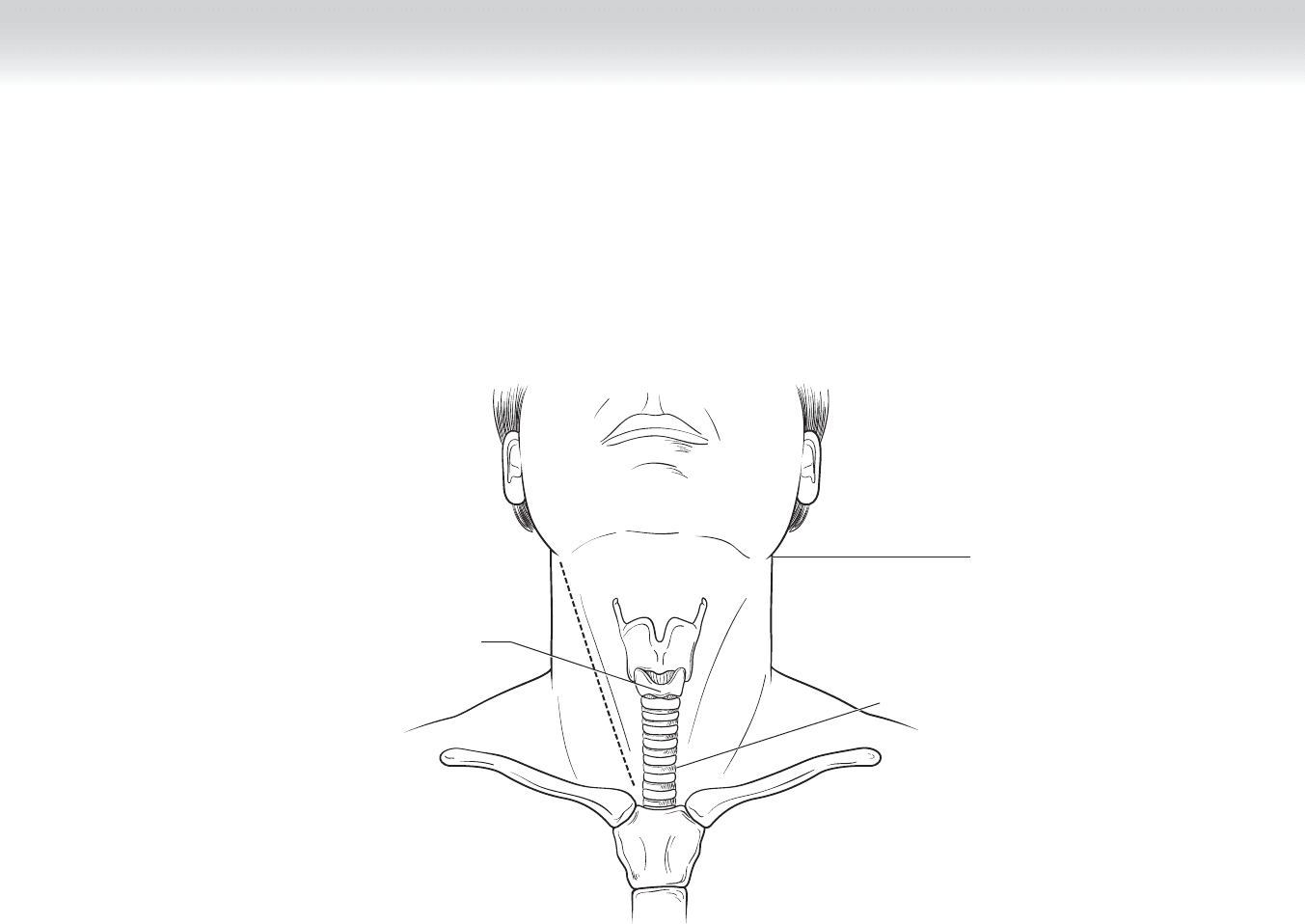
STEP 1: SURGICAL ANATOMY
The following anatomic features must be observed:
◆ Mastoid muscle
◆ Sternocleidomastoid muscle
◆ Thyroid cartilage
◆ Trachea
◆ Esophagus
◆ Carotid sheath
◆ Carotid artery (common, internal, external) (Figure 104-1)
◆ Jugular vein (facial vein)
◆ Vagus nerve and ansa cervicalis
◆ Angle of mandible (see Figure 104-1)
◆ Platysma muscle
◆ Hypoglossal nerve
◆ Digastric muscle (see Figure 104-1)
◆ Zone I: Inferior to cricothyroid cartilage
◆ Zone II: Cricothyroid to angle of mandible
◆ Zone III: Superior to angle of mandible
CHAPTER
104
Neck Exploration for Trauma
William J. Mileski
CHAPTER 104 • Neck Exploration for Trauma 1159
Cricoid
cartilage
Angle of
mandible
Zone III
Zone II
Zone I
FIGURE 104 –1
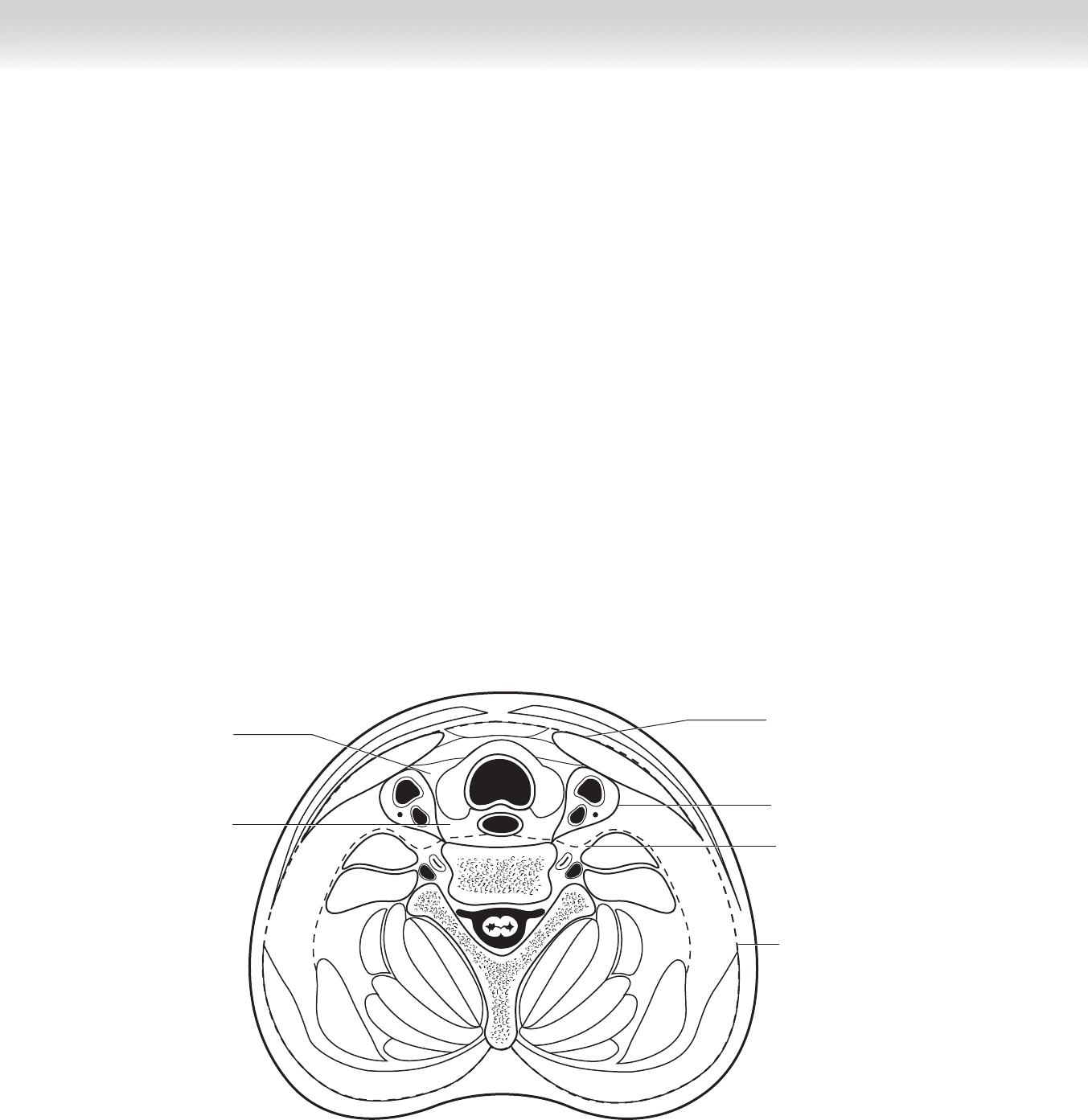
1160 Section XVI • Operations—Elective and Trauma
◆ Omohyoid muscle
◆ Inferior thyroid artery
◆ Middle thyroid vein
◆ Thyroid gland
◆ Parotid gland
◆ Cross-sectional view (Figure 104-2)
◆ Investing layer of deep cervical fascia
◆ Carotid sheath
◆ Prevertebral fascia
◆ Retropharyngeal space
Retropharyngeal
space
Pretracheal
space
Carotid sheath
Investing fascia
Prevertebral fascia
Investing layer of
deep fascia
FIGURE 104 –2

CHAPTER 104 • Neck Exploration for Trauma 1161
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The most common indication for neck exploration is penetrating trauma, although blunt
trauma may also present with vascular and aerodigestive tract injury requiring treatment,
identifi ed by hard signs on examination (active hemorrhage, expanding hematoma) or by
diagnostic study, computed tomography (CT), or ultrasound.
STEP 3: OPERATIVE STEPS
1. POSITIONING AND PREPARATION
◆ The patient is placed supine with a 3-inch towel roll beneath the shoulder, and the head is
rotated to the contralateral side.
◆ The fi eld is prepared from the base of the skull to include the entire chest, abdomen, and
both groins (for possible vein graft).
1162 Section XVI • Operations—Elective and Trauma
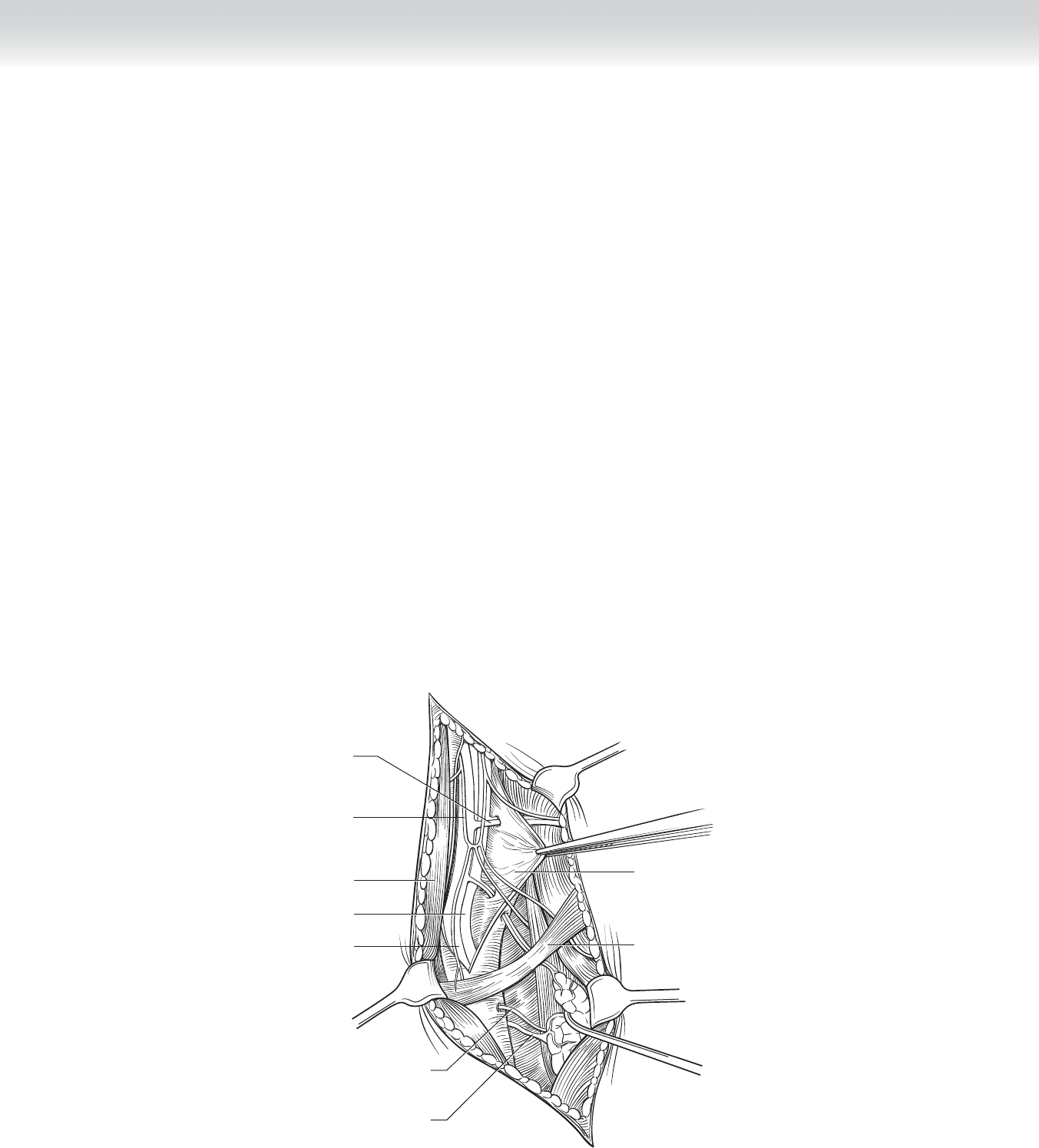
2. INCISION AND DISSECTION
◆ The skin incision is made along the anterior border of the sternocleidomastoid muscle from
the mastoid to the clavicle. The platysma muscle is incised (using electrocautery), the
sternocleidomastoid is retracted lateral, and the carotid sheath is opened from proximal to
distal. Transection of the omohyoid muscle proximally and digastric muscle distally may
improve exposure (Figure 104-3). Ligation of the facial vein, the inferior thyroid artery, and
the middle thyroid vein and transection of the ansa cervicalis allow exposure of the trachea
and esophagus by permitting easy lateral mobilization of the carotid sheath contents and
medial retraction of the thyroid gland (Figure 104-4, A).
◆ Tracheal injury may be primarily repaired with interrupted 3-0 polydioxanone (PDS)
sutures. Esophageal injuries are best repaired in two layers with an inner layer of 3-0 Vicryl
and an outer layer of 3-0 silk.
◆ When very distal exposure of the internal carotid is required, the mandible may be sub-
luxed anteriorly and medially using temporary wire fi xation (26 gauge) between the lower
bicuspids and anterior incisors (Figure 104-4, B). As the dissection on the anterior aspect
of the internal carotid is carried distally, transection of the digastric muscle will be neces-
sary, and care must be taken to avoid injury to the hypoglossal nerve.
Middle thyroid
vein
Inferior thyroid
artery
Internal jugular vein
Carotid artery
Sternocleidomastoid
muscle
Ansa cervicalis
Facial vein
Carotid sheath
opened
Omohyoid muscle
FIGURE 104 –3
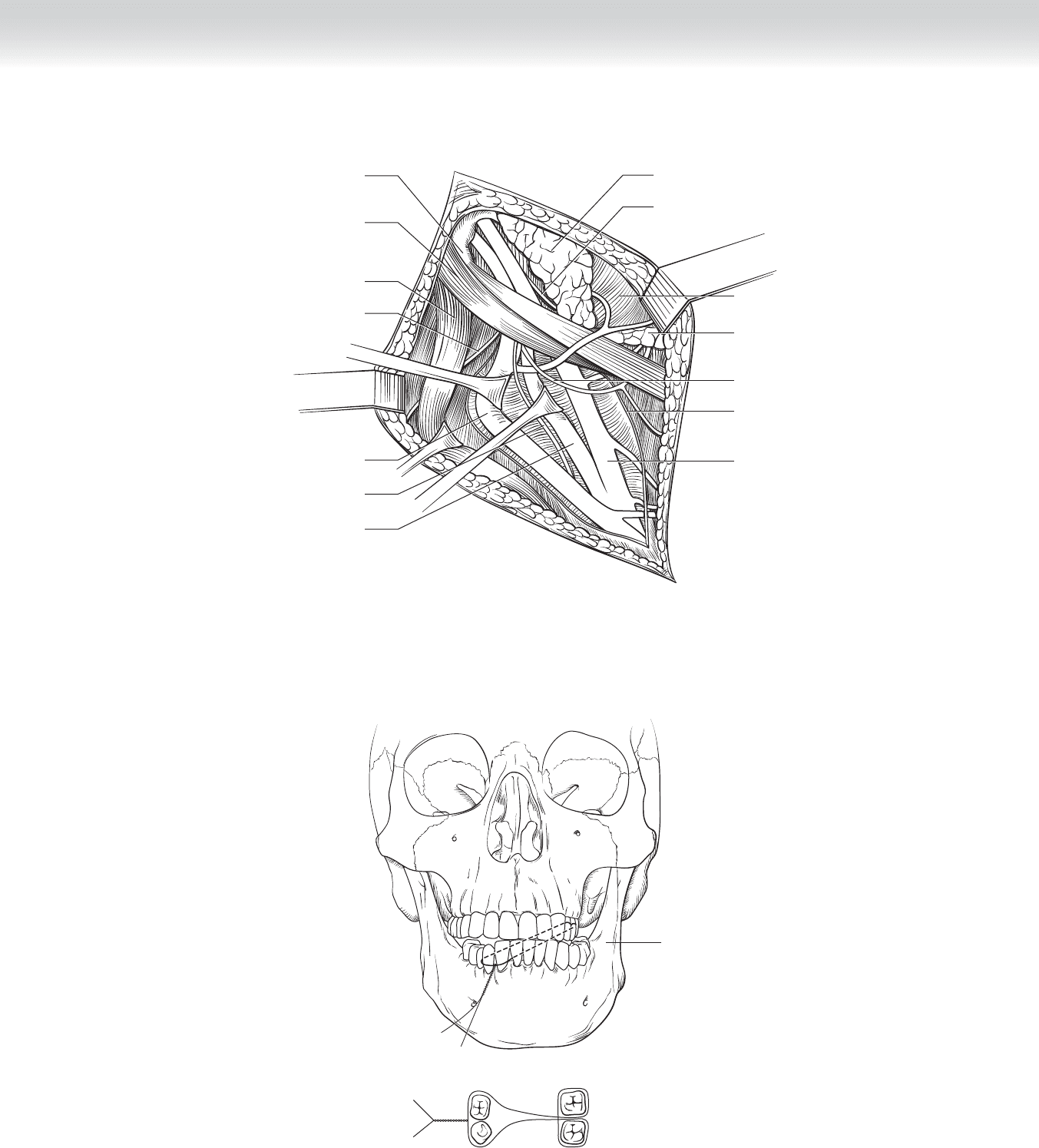
CHAPTER 104 • Neck Exploration for Trauma 1163
A
Posterior belly of
digastric muscle
Acessory nerve (XI)
Internal jugular vein
Vagus nerve
Internal carotid artery
External carotid artery
Cut edge of
carotid sheath
Submandibular
gland
Hypoglossal nerve
Masseter muscle
Glossopharyngeal nerve
Parotid gland
Sternocleidomastoid
muscle
Styloid process
B
Lower Upper
Anterior lateral
movement
FIGURE 104 –4
1164 Section XVI • Operations—Elective and Trauma
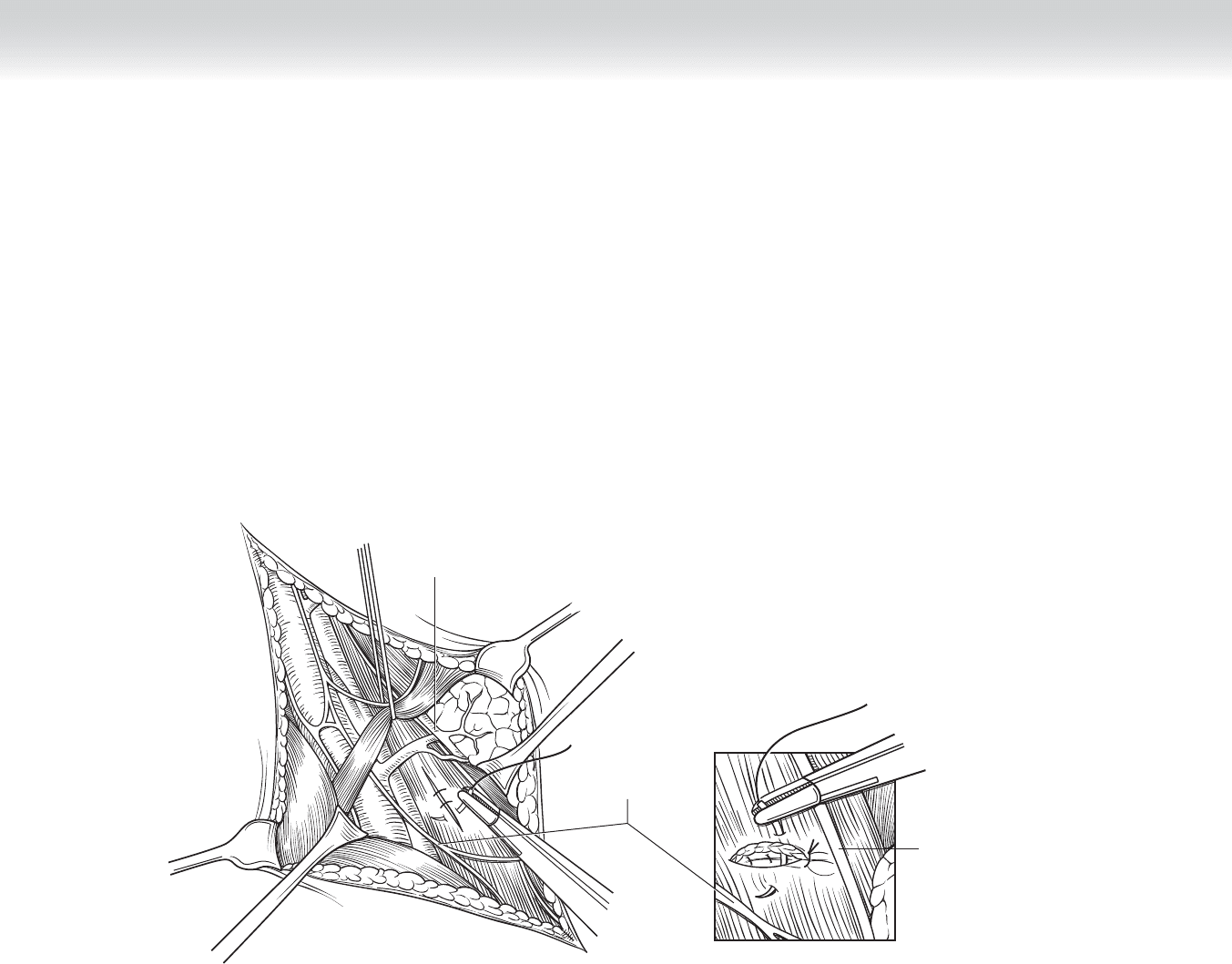
3. CLOSING
◆ A closed-suction drain is placed in the deep space between the investing fascia
(Figure 104-5) and closed with absorbable suture (3-0 Vicryl), and the skin is closed with
subcuticular 4-0 Monocryl.
Recurrent
laryngeal
nerve
Inferior thyroid
artery
Ansa cervicalis
(sternohyoid branch)
FIGURE 104 –5

CHAPTER 104 • Neck Exploration for Trauma 1165
STEP 4: POSTOPERATIVE CARE
◆ Elevate head, and maintain close observation for hematoma formation.
STEP 5: PEARLS AND PITFALLS
◆ Selective use of closed suction drainage may be indicated in aerodigestive injuries.
SELECTED REFERENCE
1. Thal ER, Weigelt JA, Carrico CJ: Operative Trauma Management: An Atlas, 2nd ed. New York,
McGraw Hill, 2002, pp 75-90.

1166
STEP 1: SURGICAL ANATOMY
The following structures must be observed (Figure 105-1):
◆ Clavicle
◆ Sternum
◆ Sternoclavicular junction
◆ Deltopectoral groove
◆ Right subclavian artery
◆ Right subclavian vein
◆ Innominate artery
◆ Innominate vein
◆ Aorta
◆ Left subclavian artery
◆ Left subclavian vein
◆ Thoracic duct (left)
CHAPTER
105
Subclavian Artery Stab
William J. Mileski