Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

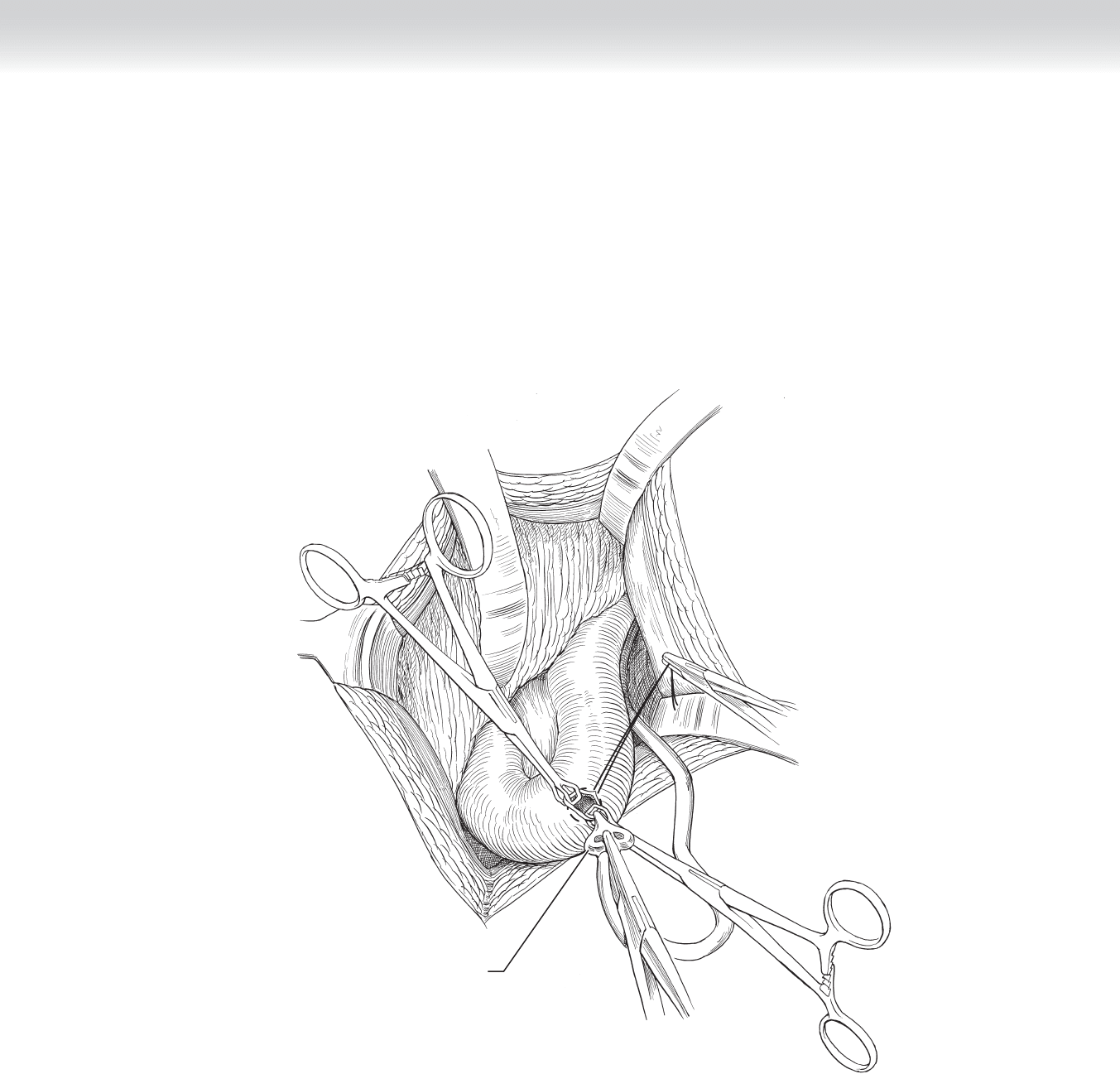
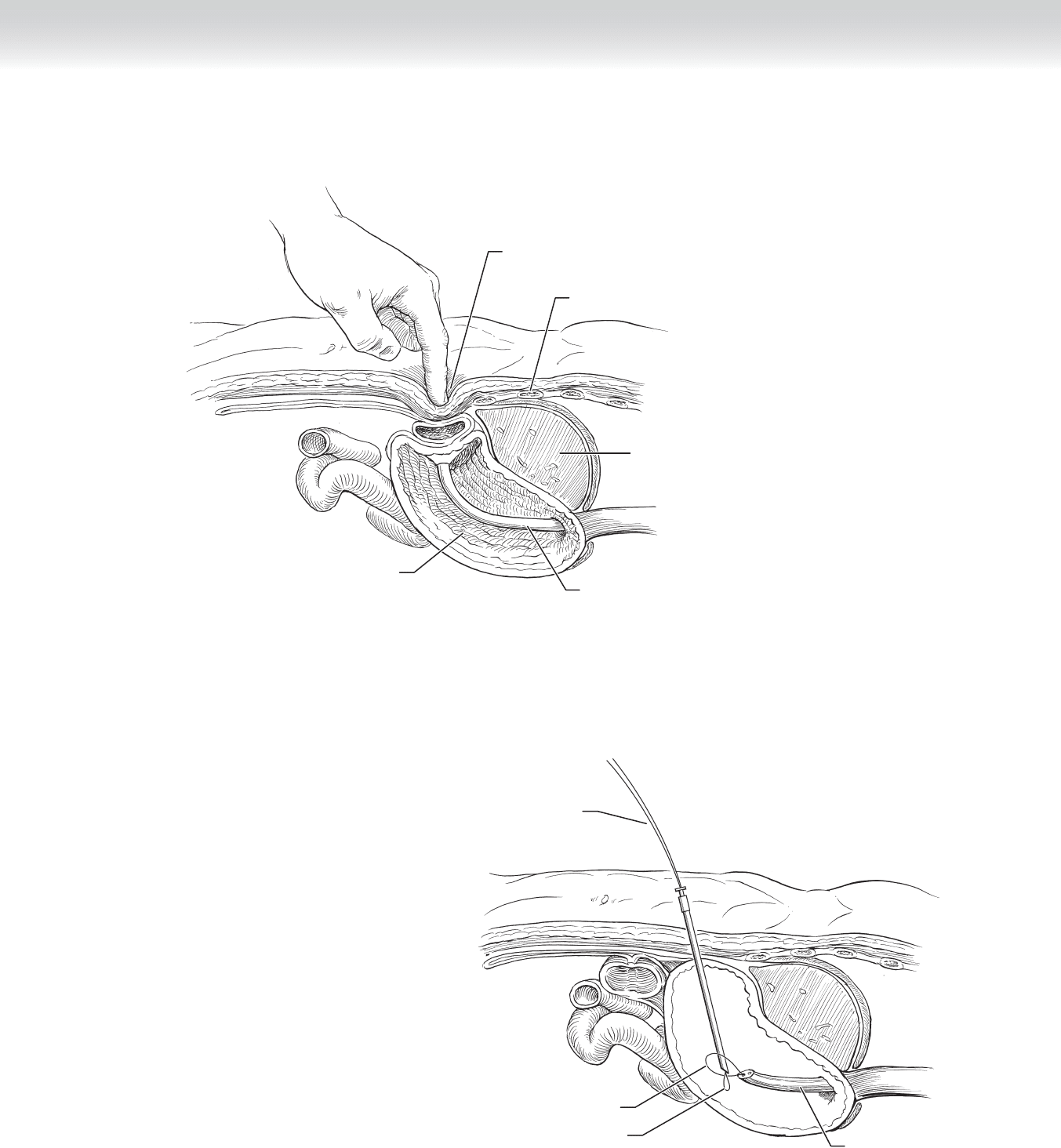
◆ Using two Babcock clamps for traction, use forceps to stent mushroom catheter tip and
place through enterotomy and advance tip 8 cm distally into intestine (Figure 21-4).
◆ Secure purse string around catheter.
Mushroom
catheter
FIGURE 2 1–4
CHAPTER 21 • Witzel Jejunostomy 249
250 Section IV • The Abdomen
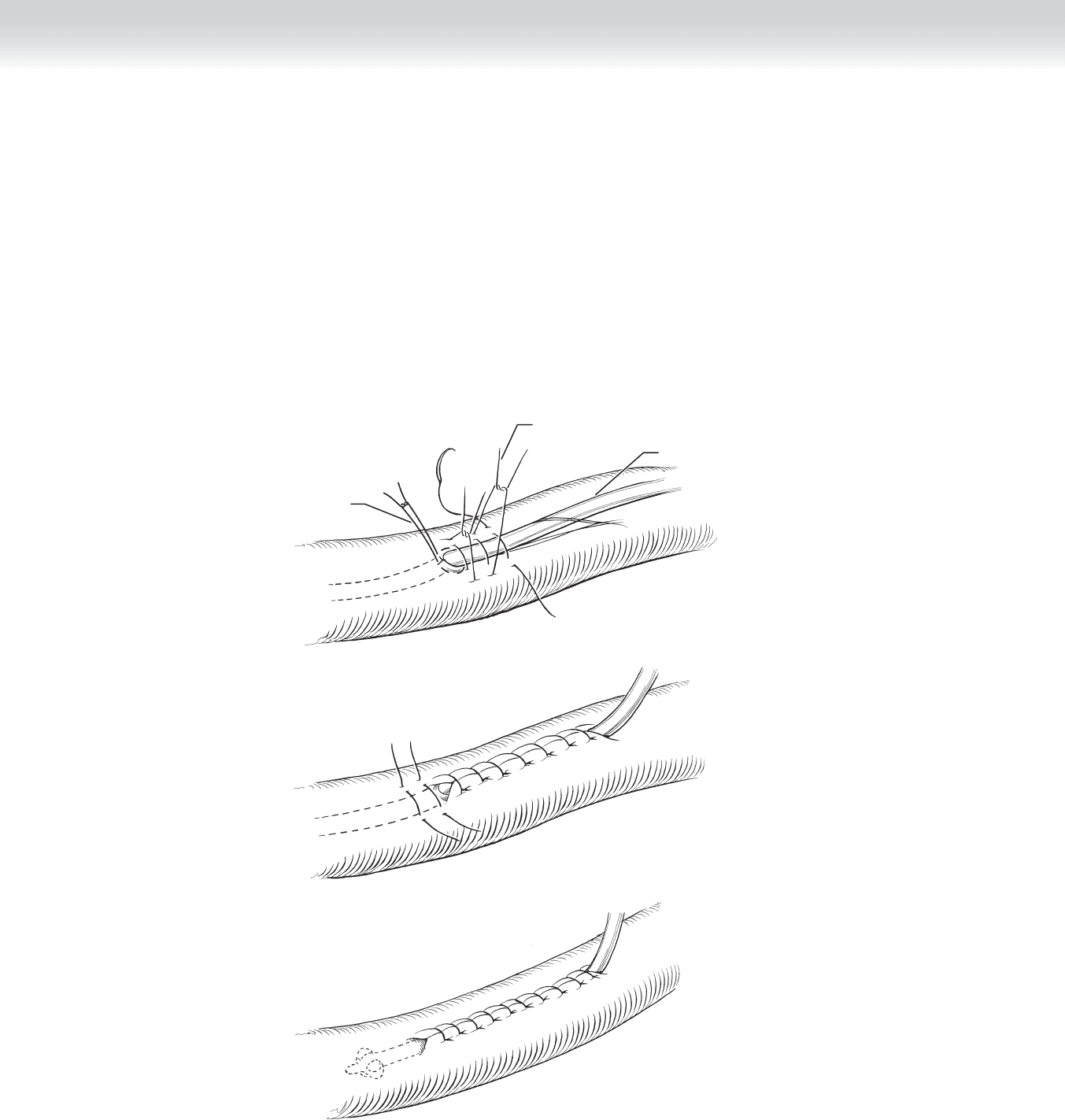
◆ Place multiple 3-0 silk interrupted sutures at 1-cm intervals for 6 to 8 cm proximal to
enterotomy and incorporate bowel wall on both sides of catheter (Figure 21-5).
◆ Tie sutures, thereby burying catheter within wall of intestine (see Figure 21-5, B).
◆ Place several additional 3-0 silk sutures at 1-cm intervals in a Lembert fashion, incorporating
enterotomy and continuing distally for 3 to 5 cm (see Figure 21-5, C).
Mushroom
catheter
Lembert sutures
Purse-string
suture
A
B
C
FIGURE 2 1–5
CHAPTER 21 • Witzel Jejunostomy 251
◆ Use several 3-0 silk sutures to anchor the antimesenteric wall of jejunum to peritoneum
(Figure 21-6).
◆ Retract mushroom catheter to approximate antimesenteric jejunal wall with enterotomy to
peritoneum, secure silk sutures.
Anchor sutures
Mushroom
catheter
Jejunum
Mesentery
Mesentery
Mesentery
FIGURE 2 1–6

252 Section IV • The Abdomen
3. CLOSING
◆ Close fascia with suture.
◆ Close skin.
STEP 4: POSTOPERATIVE CARE
◆ Routine: start feeds
STEP 5: PEARLS AND PITFALLS
◆ Use of two Babcock clamps grasping edges of enterotomy in conjunction with forceps
inserted into tip of mushroom catheter provides an excellent means for placing catheter
through enterotomy.
◆ Catheter should remain in place for at least 2 weeks to allow enterotomy tract and jejunum
to heal securely to peritoneum.
◆ Broad attachment of jejunal loop to peritoneum is advisable to minimize angulation of
small intestine.
◆ First place all the sutures from the antimesenteric edge of jejunum to peritoneum, and
then retract the catheter to approximate the jejunum to peritoneum and secure ligatures.
This sequence allows good visualization and space for placing sutures.
SELECTED REFERENCES
1. Zollinger RM Jr, Zollinger RM: Atlas of Surgical Operations. New York, Macmillan, 1983, p 92.
253
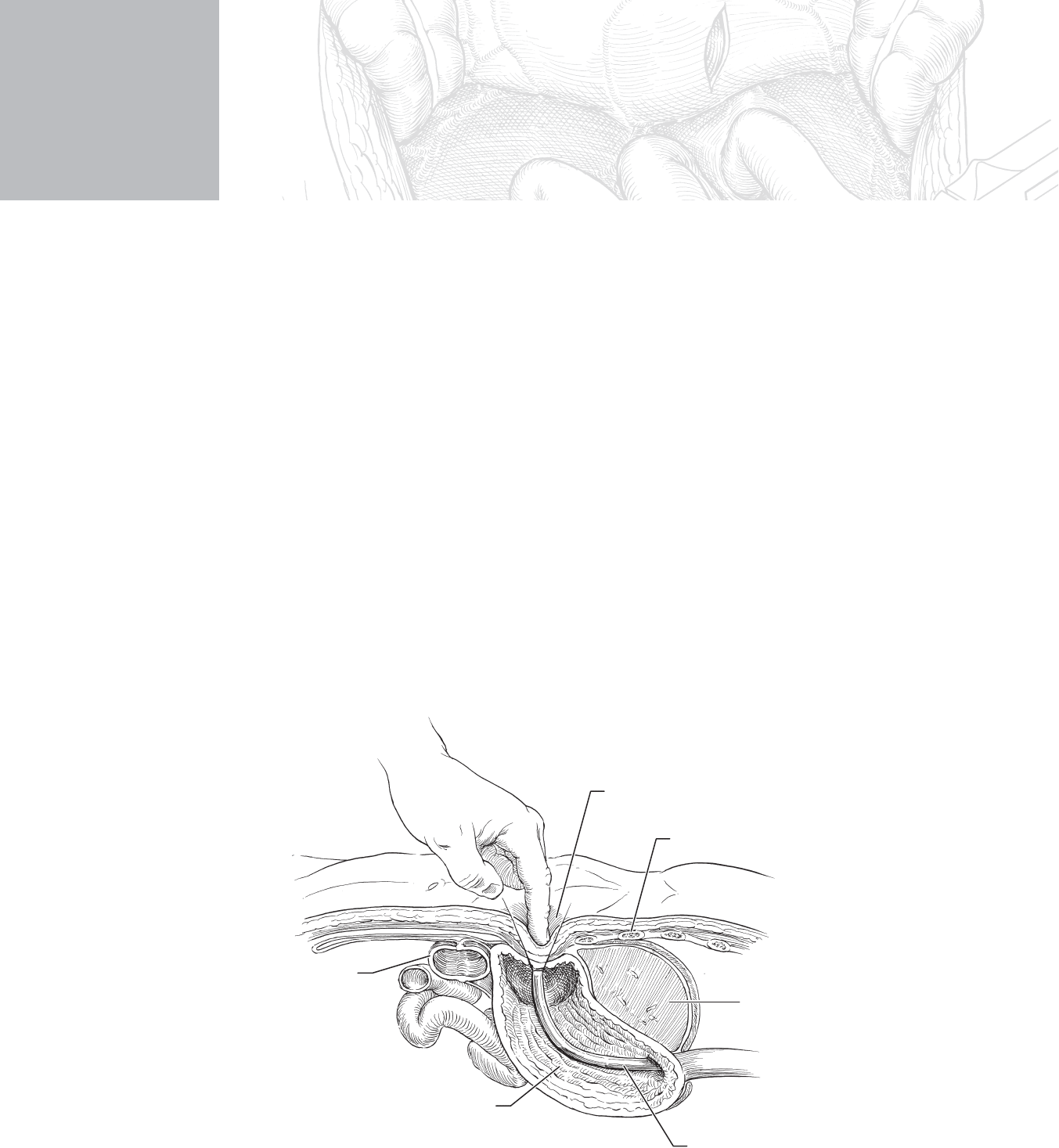
STEP 1: SURGICAL ANATOMY
◆ See Figure 22-1.
CHAPTER
22
Percutaneous Gastrostomy Feeding
Tube Placement (by surgeon
or gastroenterologist)
Dennis C. Gore
Colon
Stomach
Rib
Transillumination site
Liver
Scope
FIGURE 2 2–1

254 Section IV • The Abdomen
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Percutaneous endoscopic feeding tube placement is indicated for patients who have a functional
gastrointestinal tract but are unable or unwilling to meet nutritional demands by mouth, in gen-
eral for a period longer than 30 days (nasogastric or orogastric tubes are recommended for
shorter-term use). In addition, the patient’s potential survivability should be good if adequate
nutrition is achieved. Potential candidates include those with neurologic defi cits, psychomotor
defi cits, pseudodementia with starvation, facial trauma, facial tumors that will not immediately
threaten the patient’s life, and prolonged ventilation assistance, again with good survivability.
◆ Placement can be done at bedside, in the endoscopy suite, or in the operating room.
◆ Obtain informed consent. Often these patients cannot consent for themselves, so proper
planning with family members is important.
◆ Visualize the patient’s abdomen. Prior surgery may preclude proper placement. Adhesions
may prevent transillumination (at which point the procedure should be stopped to avoid
insertion into an overlying loop of bowel), or displacement of the stomach may cause
placement too close to ribs or belt line.
◆ If the patient has an oral or upper airway tumor, he or she may not be a candidate for
endoscopy or passage of the scope.
◆ Ensure there is no evidence of gastric outlet obstruction, in which case a jejunostomy
feeding tube may be required.
◆ Patients with excessive refl ux or nonfunctional esophageal sphincters may not be good
candidates for gastrostomy feeding tubes, which can increase risk of aspiration.
◆ Some surgeons advocate one dose of preoperative antibiotic, such as a fi rst-generation
cephalosporin, but this is not universal practice.
◆ Blood pressure, pulse oximetry, and electrocardiogram should be monitored in all patients
during the procedure.
◆ Place the video camera on the patient’s right to facilitate viewing during the procedure.

CHAPTER 22 • Percutaneous Gastrostomy Feeding Tube Placement 255
◆ Two operators are required—one for endoscopy and one for feeding tube insertion.
◆ Sedation/anesthesia considerations: Often these patients can be comatose or altered in
level of consciousness, so less sedation is required. Usually 1 to 2 mg of a benzodiazapine
and a small dose of narcotic can relax the patient to allow passage of the endoscope, which
may be eased if the patient can cooperate with swallowing. Topical spray to the oropharynx
will facilitate endoscopy. The abdominal insertion site should receive local anesthetic.
◆ Positioning/preparation: Patients are placed supine, often with the head of the bed raised at
30 degrees to prevent aspiration. A bite block is used in the mouth to prevent the patient from
biting the scope or the surgeon. Suction should be available for secretions and to prevent risk of
aspiration. The abdominal site is prepped widely with povidone-iodine (Betadine) or sterile
soap, and sterile drapes are applied. The endoscopist should be at the patient’s head on the left
and the assistant on the right by the patient’s abdomen.
STEP 3: OPERATIVE STEPS
In both methods currently used, at least two persons are needed to perform the procedure—one to
perform the endoscopic visualization and the other to perform insertion of the tube under sterile
technique. Both are performed using a prepackaged kit available from several manufacturers.

256 Section IV • The Abdomen
1. INCISION
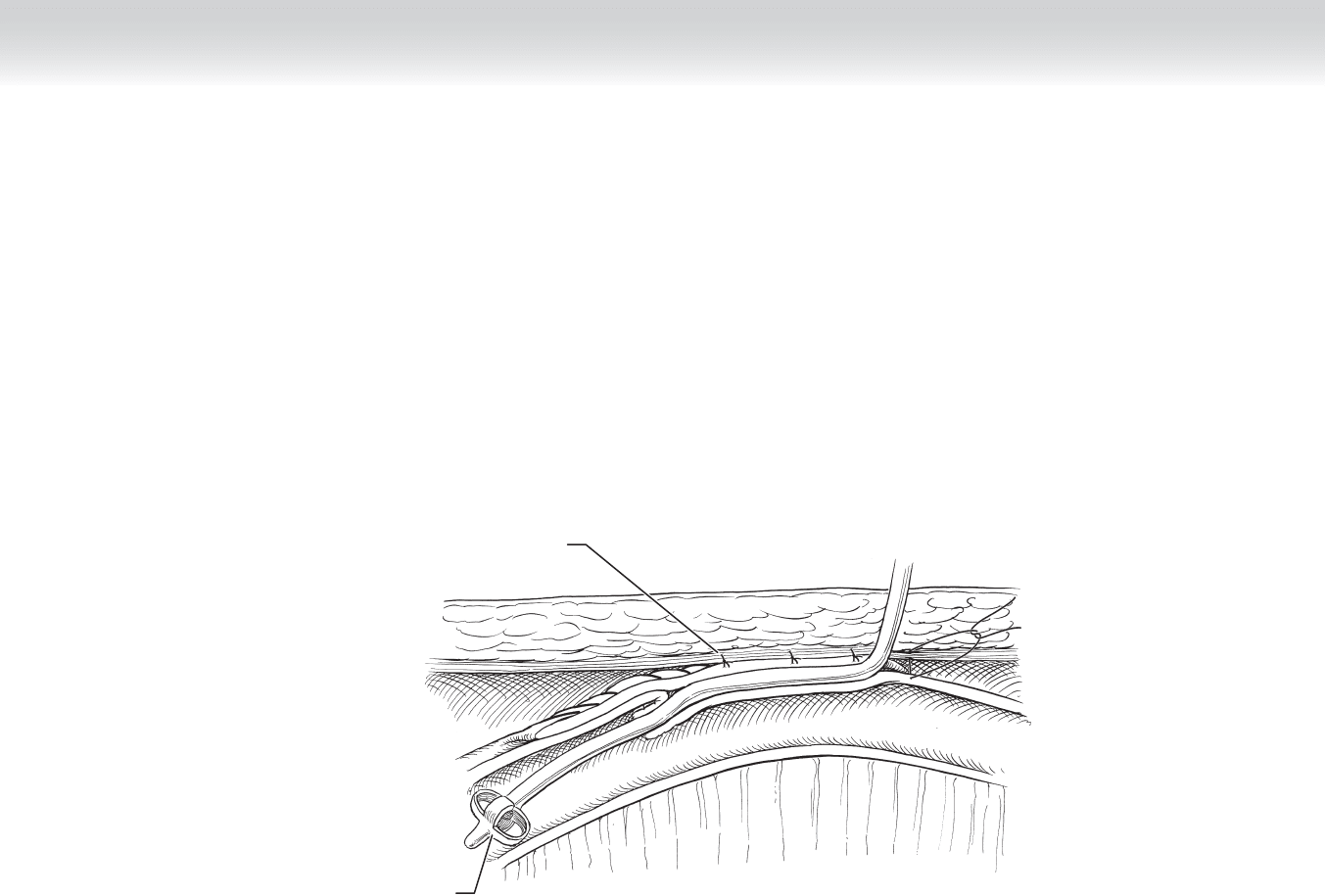
◆ Sheath method (Russell technique) (rarely used): After the patient is adequately sedated
and the abdomen is prepped in sterile technique, the endoscope is passed via the mouth
into the stomach. The stomach is insuffl ated and transilluminated (see Figure 22-1). The
lack of transillumination precludes safe placement (Figure 22-2). Once the light source is
visible through the skin, an area is marked for insertion (the site should be 2 cm away from
the costal margin) and lidocaine is injected. A no. 11 blade is used to make a small incision
(0.5 mm) in the skin. A 14- to 18-gauge needle is then passed through the incision with the
tip identifi ed on the video screen and endoscopy camera (Figure 22-3). The guidewire is
then passed through the needle and identifi ed inside the stomach and the needle is re-
moved. The dilator and then the sheath are passed in turn over the guidewire. Once the
sheath is confi rmed within the stomach, the feeding tube is passed through the sheath into
the stomach. Again after visualization of the tube, the balloon of the feeding tube is infl ated
inside the stomach.
CHAPTER 22 • Percutaneous Gastrostomy Feeding Tube Placement 257
Stomach
Rib
Liver
Scope
No transillumination
FIGURE 2 2–2
Distal end
of wire loop
Wire loop in endoscope
Wire loop through trocar
Scope
FIGURE 2 2–3

258 Section IV • The Abdomen
◆ Pull method (Ponsky): After the patient is adequately sedated and prepped using sterile
technique, the endoscope is passed via the mouth into the stomach. Visualization and
insuffl ation of the stomach is performed with transillumination (see Figure 22-1). After
identifi cation of an appropriate insertion site on the stomach (2 cm away from the costal
margin), the area is marked and lidocaine is injected. A small incision is made (1 cm) with
the no. 11 blade, and a 14- to 18-gauge needle is passed through the incision into the
stomach with visualization via the endoscope (see Figure 22-3). A braided suture is passed
through the needle and encircled by a snare passed through the endoscope. Once the
“rope” is securely entrapped, the needle is removed and the entire endoscope with snare
and attached rope is withdrawn through the mouth (Figure 22-4). The feeding tube is then
attached to the rope and lubricated well. The assistant then withdraws the rope from the
stomach wall, and the tube is carefully guided through the patient’s mouth into the stomach
and is pulled into position (Figure 22-5). Once the feeding tube has been drawn through
the skin to approximately 4 cm, the endoscope is reinserted into the stomach to ensure
proper seating of the feeding tube. A skin disc is placed to help hold the tube in position
against the abdomen (Figure 22-6).
◆ Push method (Sacks-Vine): After the patient is adequately sedated and prepped using ster-
ile technique, the endoscope is passed via the mouth into the stomach. Visualization and
insuffl ation of the stomach is performed with transillumination (see Figure 22-1). After
identifi cation of an appropriate insertion site on the stomach (2 cm away from the costal
margin), the area is marked and lidocaine is injected. A small incision is made (1 cm) with
the no. 11 blade, and a 14- to 18-gauge needle is passed through the incision into the
stomach with visualization via the endoscope (see Figure 22-3). A guidewire is passed
through the needle and encircled by a snare passed through the endoscope. Once the
guidewire is securely entrapped, the needle is removed and the entire endoscope with snare
and attached guidewire is withdrawn through the mouth (see Figure 22-4). Once enough
guidewire is visible through the mouth, the feeding tube is then fed over the guidewire and
lubricated well. The feeding tube is then fed through the mouth and pushed over the wire.
The assistant keeps tension on the guidewire and grabs the tapered end of the feeding tube
as it emerges on the skin. Once the feeding tube as been drawn through the skin to approx-
imately 4 cm, the guidewire is withdrawn and the endoscope is reinserted into the stomach
to ensure proper seating of the feeding tube. A skin disc is then guided over the feeding
tube to help secure its position against the skin (see Figure 22-6).
2. DISSECTION
◆ Not applicable
3. CLOSING
◆ Not applicable