Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 24 • Finney Pyloroplasty 269
Duodenum
Continuous
incision
(all layers)
Antrum
FIGURE 24 –2
Antrum
Pylorus
Duodenum
Running closure
of posterior
mucosal layer
FIGURE 24 –3
270 Section IV • The Abdomen
Duodenum
Running closure
of anterior
mucosal layer
Antrum
FIGURE 24 –4
Antrum
Duodenum
Interrupted
seromuscular stitches
FIGURE 24 –5

CHAPTER 24 • Finney Pyloroplasty 271
3. CLOSING
◆ The incision is closed in layers using 2-0 polyglactin in a running fashion. The subcutane-
ous tissue is reapproximated with a running 3-0 polyglactin suture. The skin can be stapled
together or closed with a running subcuticular suture of 4-0 undyed absorbable monofi la-
ment and adhesive strips.
STEP 4: POSTOPERATIVE CARE
◆ The patient should have already received a preoperative dose of a prophylactic antibiotic
such as cefazolin. Two additional doses should be given after the operation. Hydration will
be maintained with an intravenous infusion of a balanced dextrose and electrolyte solution.
Intravenous analgesics are used until the patient resumes enteral feeds. The decision to
decompress the stomach with a nasogastric tube is up to the individual surgeon, and the
current tendency is to use these tubes sparingly. Certainly, if the repair was deemed to be
tenuous, a nasogastric tube could prove to be very helpful. After 2 to 3 days (on average),
enteral feeds can be slowly and gradually resumed. The presence of bile in the gastric aspi-
rate does not necessarily represent a persistent postoperative paralytic ileus, because it could
be the result of the pyloroplasty itself, and it should not be a reason for undue delays in
resumption of enteral feeds. Pain, abdominal distention, tachycardia, and guarding should
prompt the surgeon to order a contrast study to investigate for leaks in the suture line.
STEP 5: PEARLS AND PITFALLS
◆ As mentioned previously, avoidance of tension on the suture line is essential. This is accom-
plished by a generous Kocher maneuver. Avoid approximating the antrum and duodenum
in such a manner that both structures have to be excessively rolled inward to approximate
the anterior layers. This can be achieved by placing the posterior seromuscular stitches as
posterior as possible (taking care not to involve the ampulla of Vater in the suture line),
giving ample room to perform the incisions in both the duodenum and antrum and
complete the anastomosis with minimal tension.
◆ As with any pyloroplasty, alkaline refl ux, alkaline gastritis, and dumping syndrome can be
problematic. Suture line leaks can result from undue tension or the approximation of
acutely infl amed or poorly perfused tissues.
SELECTED REFERENCES
1. Mercer DW: Stomach. In Townsend CM, Beauchamp RD, Evers MB, Mattox KL (eds): Sabiston Textbook
of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 1265-1317.
2. Warner BW: Pediatric surgery. In Townsend CM, Beauchamp RD, Evers MB, Mattox KL (eds): Sabiston
Textbook of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 2097-2132.

272
INTRODUCTION
This bypass operation is indicated in the presence of marked infl ammation or scarring of the
pylorus that precludes a Heineke-Mikulicz pyloroplasty. The procedure can be performed using
a standard handsewn technique or a stapler. The handsewn technique described in this chapter
is a two-layer anastomosis with a running inner layer of 3-0 absorbable sutures and a seromus-
cular outer layer of interrupted 3-0 silk sutures.
STEP 1: SURGICAL ANATOMY
◆ The pylorus sits at the distal end of the stomach and is marked by thickening of the circular
smooth muscle layer, thus forming the pyloric sphincter, which acts as a valve between the
stomach and the duodenum and regulates gastric emptying. The pylorus does not have
independent blood supply; rather, it gets its blood supply from the vessels that perfuse the
distal stomach and proximal duodenum. Innervation of the pylorus is through the terminal
branches of the right and left vagus nerves. Any injury to these nerves or denervation of the
pylorus will result in pylorospasm and delayed gastric emptying.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Confi rmation of the diagnosis of peptic ulcer disease or delay in gastric emptying should
be documented before the procedure with endoscopy, contrast studies, or technetium-99
sulfur colloid meals.
CHAPTER
25
Jaboulay Side-to-Side
Gastroduodenostomy
Carlos A. Angel

CHAPTER 25 • Jaboulay Side-to-Side Gastroduodenostomy 273
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The operation can be performed through a limited midline supraumbilical laparotomy. The
skin incision is made with the knife, and the rest of the layers are divided with electrocau-
tery, taking care to stay in the midline and paying close attention to hemostasis. Once the
peritoneum is opened, the surgeon’s fi ngers or a malleable retractor can be used to protect
the intestines from enterotomies.
2. DISSECTION
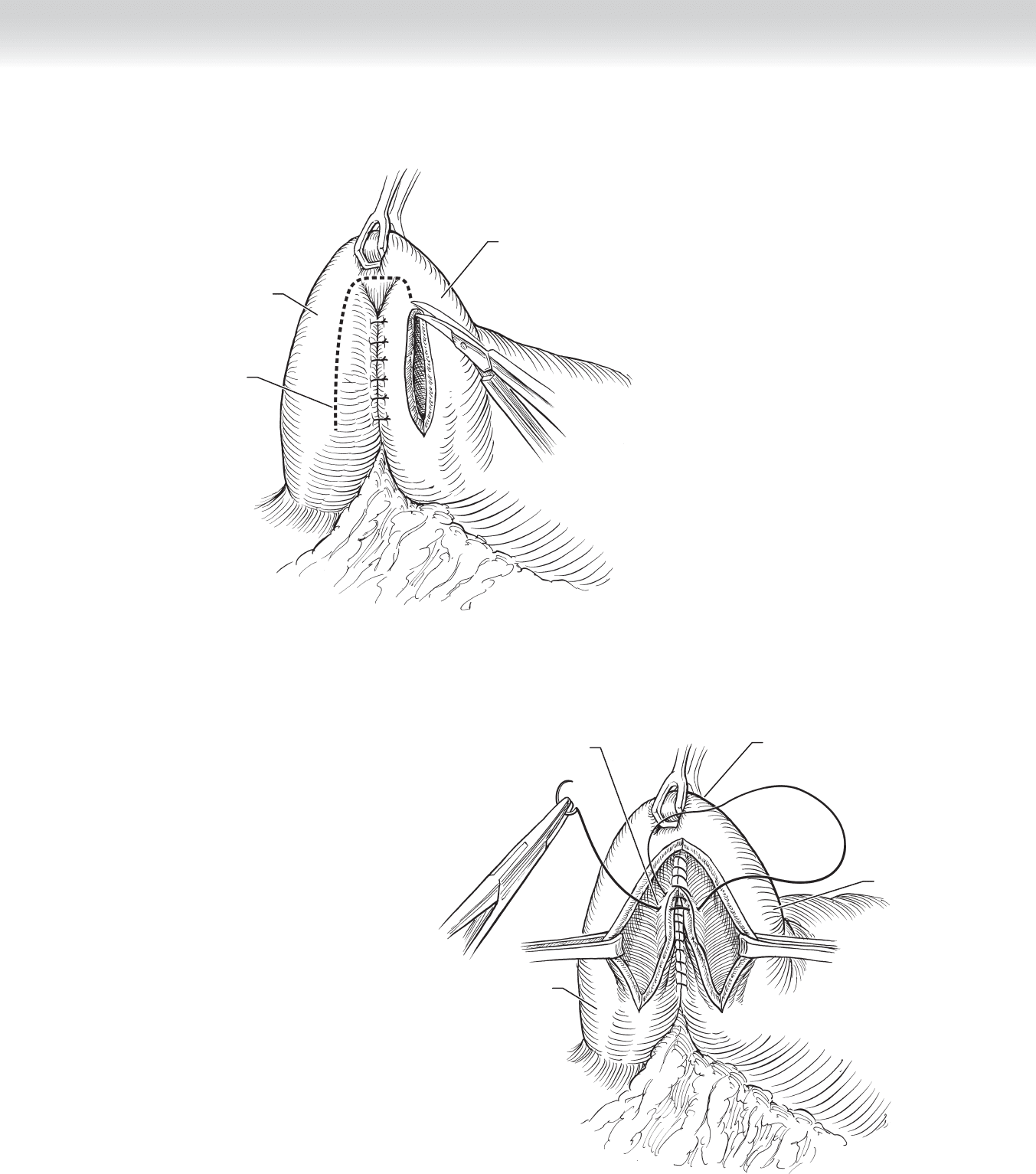
◆ After wide mobilization of the duodenum with a generous Kocher maneuver, the pylorus is
grasped with a Babcock forceps and a 3-0 silk stitch is placed approximately 7 cm distal from
this point to approximate the antrum and duodenum (Figures 25-1 and 25-2). Approximately
6 to 8 cm of duodenum and antrum are approximated with 3-0 silk, interrupted seromuscular
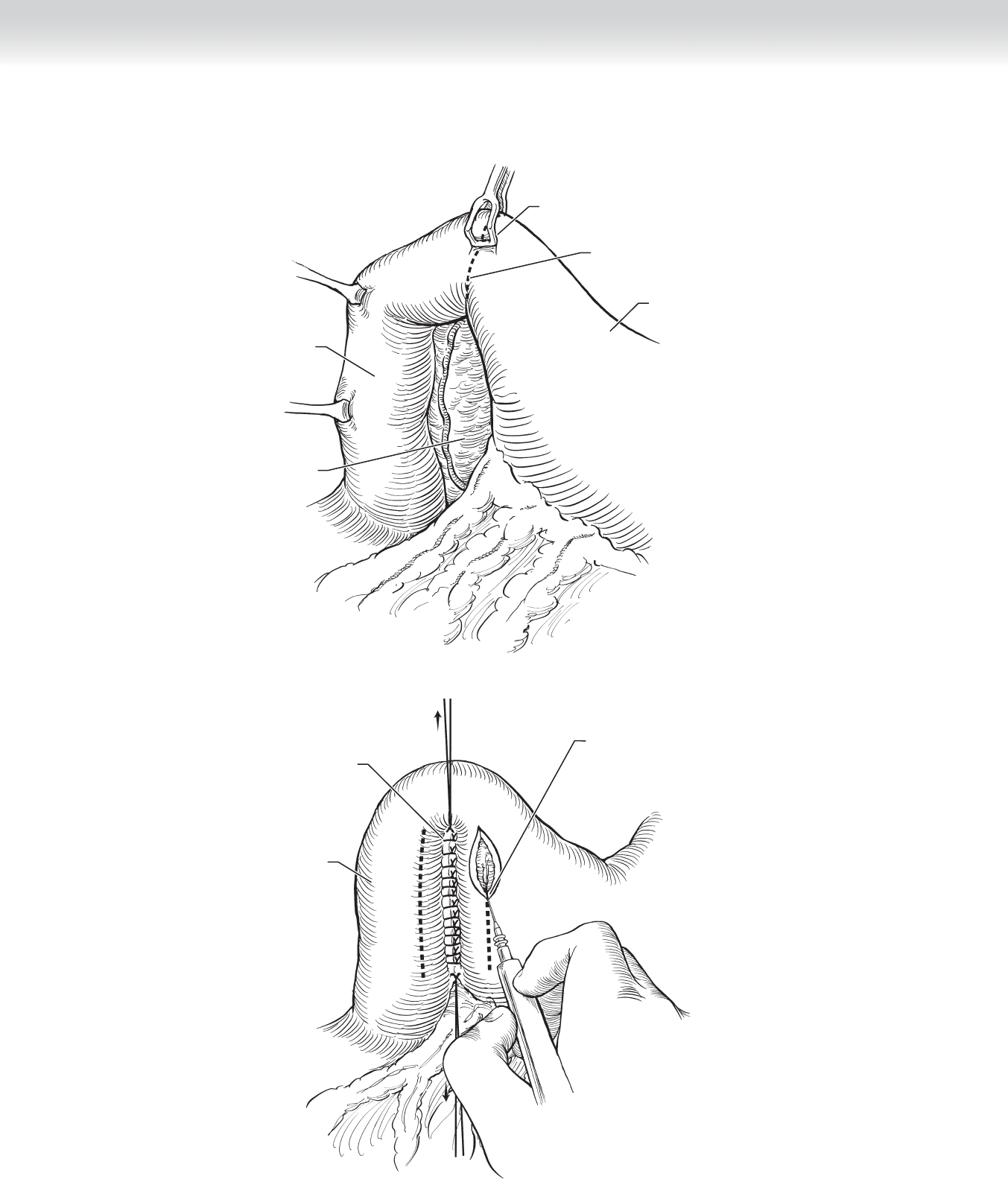
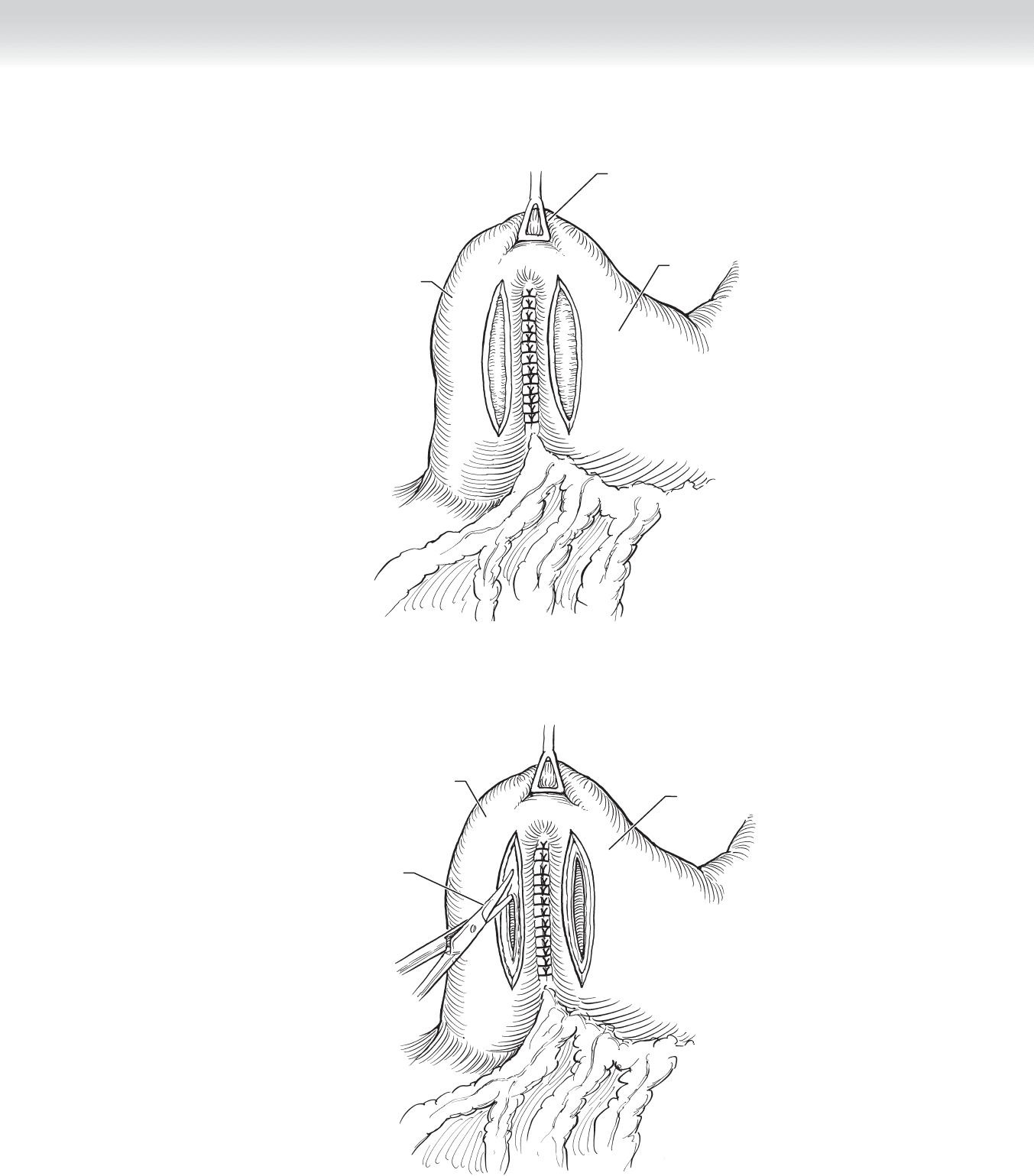
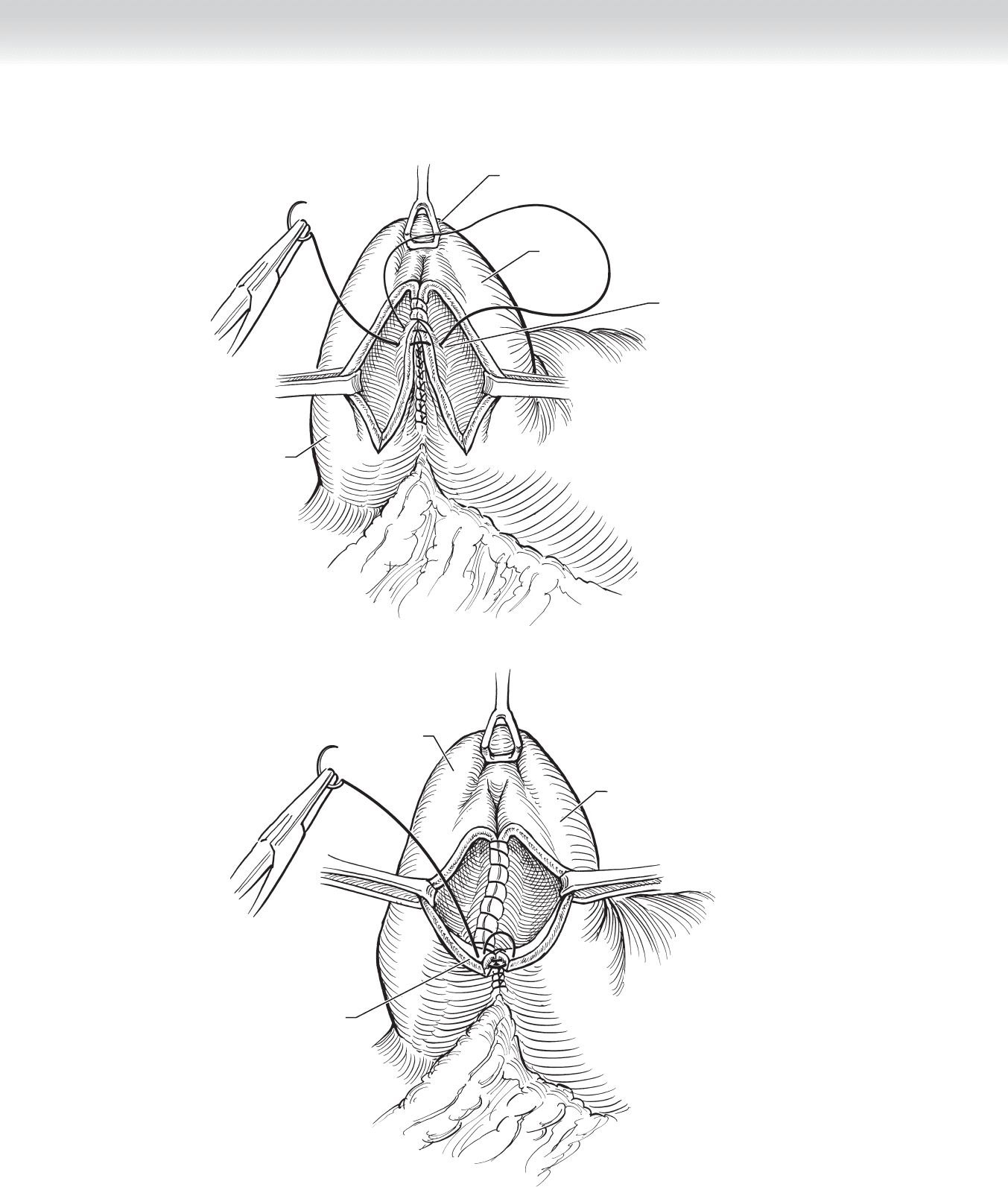
sutures (see Figure 25-2). The duodenum is incised down to the mucosa on both duodenal
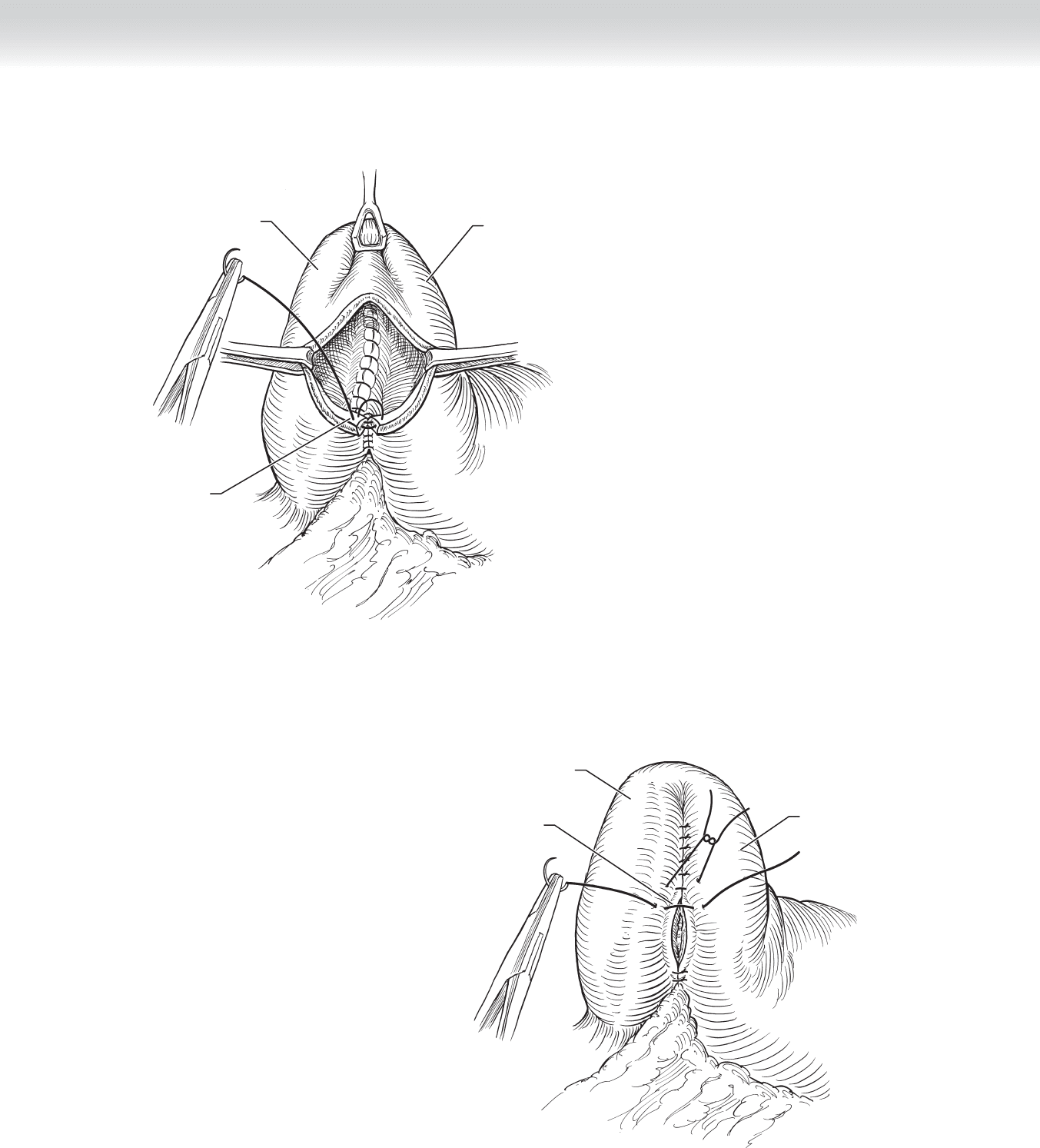
and antral sides. Bleeding points are cauterized (Figure 25-3). Antral and duodenal mucosas
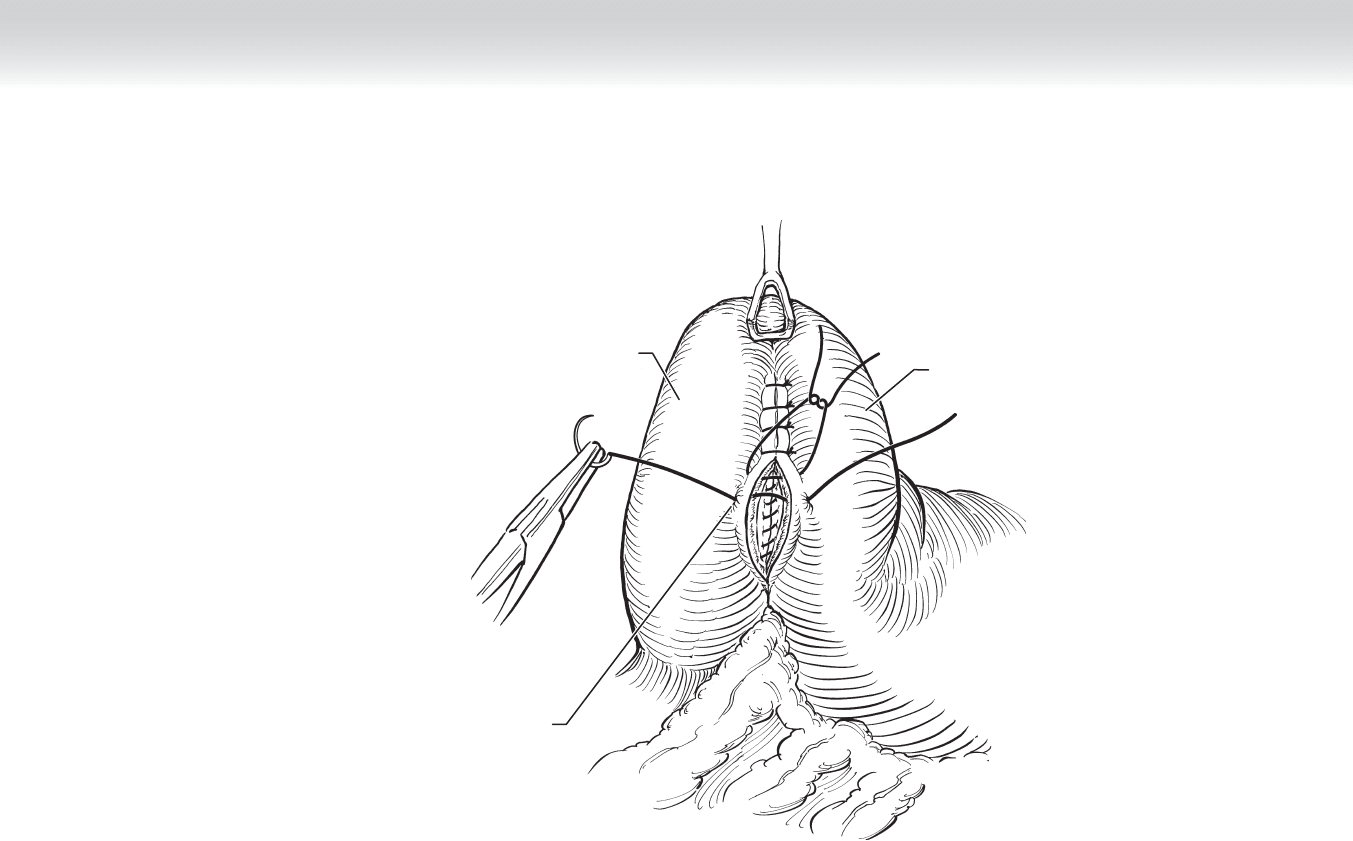
are sharply opened. Bleeding is controlled with cautery (Figure 25-4). The mucosa is approxi-
mated with a continuous, simple stitch of 3-0 absorbable suture, starting with the posterior
portion and fi nishing anteriorly (Figures 25-5 and 25-6). The anastomosis is completed with
interrupted 3-0 silk seromuscular stitches (Figure 25-7).
3. CLOSING
◆ The incision is closed in layers using 2-0 polyglactin in a running fashion. The subcutane-
ous tissue is reapproximated with a running 3-0 polyglactin suture. The skin can be stapled
together or closed with a running subcuticular suture of 4-0 undyed absorbable monofi la-
ment and adhesive strips.
STEP 4: POSTOPERATIVE CARE
◆ The patient should have already received a preoperative dose of a prophylactic antibiotic
such as cefazolin. Two additional doses are in order after the operation. Hydration will
be maintained with an intravenous infusion of a balanced dextrose and electrolyte solu-
tion. Intravenous analgesics are used until the patient resumes enteral feeds. The deci-
sion to decompress the stomach with a nasogastric tube is up to the individual surgeon,
and the current tendency is to use these tubes sparingly. Certainly, if the repair was
deemed to be tenuous, a nasogastric tube could prove to be very helpful. After 2 to
3 days (on average), enteral feeds can be slowly and gradually resumed. The presence
of bile in the gastric aspirate does not necessarily represent a persistent postoperative
paralytic ileus, because it could be the result of the pyloroplasty itself and it should not
be a reason for undue delays in resumption of enteral feeds. Pain, abdominal distention,
tachycardia, and guarding should prompt the surgeon to order a contrast study to
investigate for leaks in the suture line.
Text continued on p. 277
274 Section IV • The Abdomen
Antrum
Grasped with
Babcock forceps
Pylorus
Duodenum
Pancreas
MC
FIGURE 25 –1
Duodenum
First row of
interrupted sutures
Incision through
prepyloric area
FIGURE 25 –2
CHAPTER 25 • Jaboulay Side-to-Side Gastroduodenostomy 275
Antrum
Grasped with
Babcock forceps
Duodenum
FIGURE 25 –3
Duodenum
Opening of
mucosa on
both sides
Antrum
FIGURE 25 –4
276 Section IV • The Abdomen
Antrum
Grasped with
Babcock forceps
Closure of
posterior
mucosal layer
Duodenum
FIGURE 25 –5
Duodenum
Closure of
anterior
mucosal layer
Antrum
FIGURE 25 –6
CHAPTER 25 • Jaboulay Side-to-Side Gastroduodenostomy 277
Duodenum
Layer of interrupted
seromuscular
stitches
Antrum
STEP 5: PEARLS AND PITFALLS
◆ As mentioned, avoidance of tension on the suture line is essential. This is accomplished
by a generous Kocher maneuver. Avoid approximating the antrum and duodenum in
such a manner that both structures have to be excessively rolled inward to approximate
the anterior layers. This can be achieved by placing the posterior seromuscular stitches
as posterior as possible (taking care not to involve the ampulla of Vater in the suture
line), giving ample room to perform the incisions in both the duodenum and antrum
and complete the anastomosis with minimal tension.
COMPLICATIONS
◆ As with any pyloroplasty, alkaline refl ux, alkaline gastritis, and dumping syndrome can be
problematic. Suture line leaks can result from undue tension or the approximation of
acutely infl amed or poorly perfused tissues.
SELECTED REFERENCES
1. Mercer DW: Stomach. In Townsend CM, Beauchamp RD, Evers MB, Mattox KL (eds): Sabiston Textbook
of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 1265-1317.
2. Warner BW: Pediatric surgery. In Townsend CM, Beauchamp RD, Evers MB, Mattox KL (eds): Sabiston
Textbook of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 2097-2132.
FIGURE 25 –7

278
STEP 1: SURGICAL ANATOMY
◆ The blood supply to the stomach is abundant. The right gastric artery, a branch from the
hepatic artery, courses along the lesser curvature of the stomach to meet the left gastric
artery, which is a branch of the celiac axis. The right gastroepiploic artery, a branch of the
gastroduodenal artery, courses along the greater curvature of the stomach to meet the left
gastroepiploic artery, which is a branch of the splenic artery. In addition, the stomach
receives short gastric branches from the splenic artery. The venous drainage of the stomach
is into the portal venous system (Figure 26-1).
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The Billroth I procedure for gastroduodenostomy is the most physiologic type of gastric
resection, because it restores normal gastroduodenal continuity. It has been the preferred
treatment of gastric ulcer or antral cancer by a number of surgeons; however, its use for
duodenal ulcer has been less popular. The principal contraindications to a Billroth I oper-
ation include edema from acute or recurrent infl ammation and scarring and deformation
secondary to chronic disease.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ An upper midline incision or subcostal incision is an acceptable option for performing this
procedure. The line of division varies according to the extent of resection required. The
dashed line indicates an approximate 50% gastric transection with a line from the lesser
curvature slightly proximal to the incisura angularis (Figure 26-2).
CHAPTER
26
Gastric Resection: Billroth I
B. Mark Evers