Blackburn J.A., Dulmus C.N. (Editors). Handbook of gerontology: evidence-based approaches to theory, practice, and policy
Подождите немного. Документ загружается.


CHAPTER 15
Parenting Grandchildren
HWA-OK HANNAH PARK and JAN STEVEN GREENBERG
D
URING THE DECADES
of the 1970s and 1980s, researchers focused on the sig-
nificance and meaning of grandparenthood and on the grandparents’
level of satisfaction with this role (Cherlin & Furstenberg, 1986; Korn-
haber, 1985; Troll, 1983; Wood & Robertson, 1976). This interest in grandparent-
hood was explained, in part, by increases in the life expectancy of individuals
along with improvements in the health of older adults and a rapid growth in the
number of single-parent families due to divorce or nonmarital parenthood
(Pruchno & Johnson, 1996; Robertson, 1995). Longer life expectancy and im-
proved health and functioning of older adults has both extended the length of the
grandparenting role as well as the number of years in which older adults remain
actively involved in the life of their grandchildren. Whereas in 1900, most grand-
children never knew their grandparents, by 2000 over 96% of children under the
age of 20 had at least one living grandparent (Cherlin & Furstenberg, 1986; Uhlen-
berg & Kirby, 1998).
During the past decade, the focus has shifted away from the normative role of
grandparenthood to the role of grandparents as caregivers to their grandchildren
(Fuller-Thomson, Minkler, & Driver, 1997). According to the U.S. Census Bureau,
the number of children under 18 living in households headed by a grandparent
has grown from 2.2 million (or 3.2% of children in the United States) in 1970 to
approximately 4 million (or 5.5% of children) in 1997 (Lugaila, 1998). Although
the majority of grandparent-headed households also include at least one of the
grandchild’s parents, since 1990 the fastest growing type of grandparent-headed
household is one in which the grandparents and their grandchildren reside to-
gether without the grandchild’s parents. By 2000, it has been estimated that ap-
proximately 2.4 million grandparents were responsible for most of the basic
needs of their grandchildren (Bryson, 2001).
The role of grandparent caregiving has many challenges in common with
those faced by elders caring for a frail elderly family member. Both grandparent
caregivers and caregivers of elders are faced with multiple care-giving demands
that require an output of time and energy at a time in their lives when they may
397

398 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
be experiencing diminished capacity due to age-related changes. In addition,
the challenges of caregiving are likely to have rippling effects, producing addi-
tional strains in the areas of finances and family and social relationships. Fi-
nally, although the burdens of care are always present, both groups of
caregivers are likely to experience many aspects of the care-giving role as re-
warding and providing feelings of intimacy and a sense of meaning and pur-
pose in life (Jendrek, 1993; Kramer, 1997; Minkler & Roe, 1993; Schwartz &
Gidron, 2002).
Yet the differences between caring for a grandchild and caring for a frail el-
derly relative are greater than the similarities. First, the distinctive nature of
the grandparent-grandchild relationship gives rise to several unique stressors
faced by grandparent caregivers that are not commonly encountered by other
care-giving populations. Whereas most caregivers for the elderly are legally
empowered to make decisions for the elder, legal custody of a child is not auto-
matically bestowed on grandparent caregivers. Grandparents thus must seek
the parents’ permission to make decisions for the child. This can be quite stress-
ful if the grandparent and parent have differing views of what is in the best in-
terest of the child. In addition, although all caregivers face housing challenges,
grandparent caregivers living in public housing for seniors, which is not un-
common, may fear eviction if their skipped-generation family configuration vi-
olates the existing regulations for senior housing. Another challenge faced by
grandparent caregivers is dealing with school systems, which are oriented to-
ward younger families. These are but a few examples of the stressors encoun-
tered by many grandparent caregivers that are not typically faced by caregivers
of frail elders.
Second, whereas most caregivers of older adults will outlive the care recipient,
a major burden for grandparent caregivers is worrying about the future well-
being of their grandchild after the grandparents’ death. “What will happen when
I’m gone?” is a universal concern. Third, grandparent caregivers may be viewed
by others as not being able to care for their grandchildren. Older grandparents
may especially feel that they are being closely watched and quite vulnerable to
having their grandchild taken away (Janicki, McCallion, Grant-Griffin, &
Kolomer, 2000). This is rarely a concern among spousal or filial caregivers of older
adults or parents caring for children with disabilities.
Fourth, most caregivers are providing care for a frail elder because of the
elder’s chronic cognitive, mental, or physical disability, whereas grandparents
typically have assumed the care-giving role because of the parents’ incapacity.
Thus, it is not uncommon for grandparents to not only have care-giving responsi-
bilities for their grandchild but also be providing considerable support and assis-
tance to the grandchild’s parent. Finally, whereas the trajectory of an elder’s
disability is typically one of increasing disability of the care recipient and greater
dependence on the caregiver, grandchildren move toward greater independence
as they age. As the grandchild moves into adolescence, grandparents have dimin-
ishing influence over the grandchild’s behavior. Coping with adolescence is in
general a stressful time for parents, and may be amplified for grandparents be-
cause of the wider cultural gap between the generations. As we discuss in this
chapter, these unique challenges faced by grandparents must be considered in
developing community-based programs and services to target grandparents car-
ing for their grandchild.
Parenting Grandchildren 399
This chapter begins with an overview of the literature on the prevalence of the
grandparent care-giving phenomenon and provides a description of the charac-
teristics of this emerging and growing population. Next, we examine the context
of grandparent caregiving, reasons for providing primary care to grandchildren,
the impact of caregiving on grandparents, and factors associated with the well-
being of grandparent caregivers. Economic policy issues related to grandparent
caregivers are reviewed and evidence-based interventions for grandparent care-
givers and their families are considered. Finally, recommendations for practice,
policy, and future research are discussed.
A PROFILE OF GRANDPARENT CAREGIVERS
IN THE UNITED STATES
P
REVALENCE
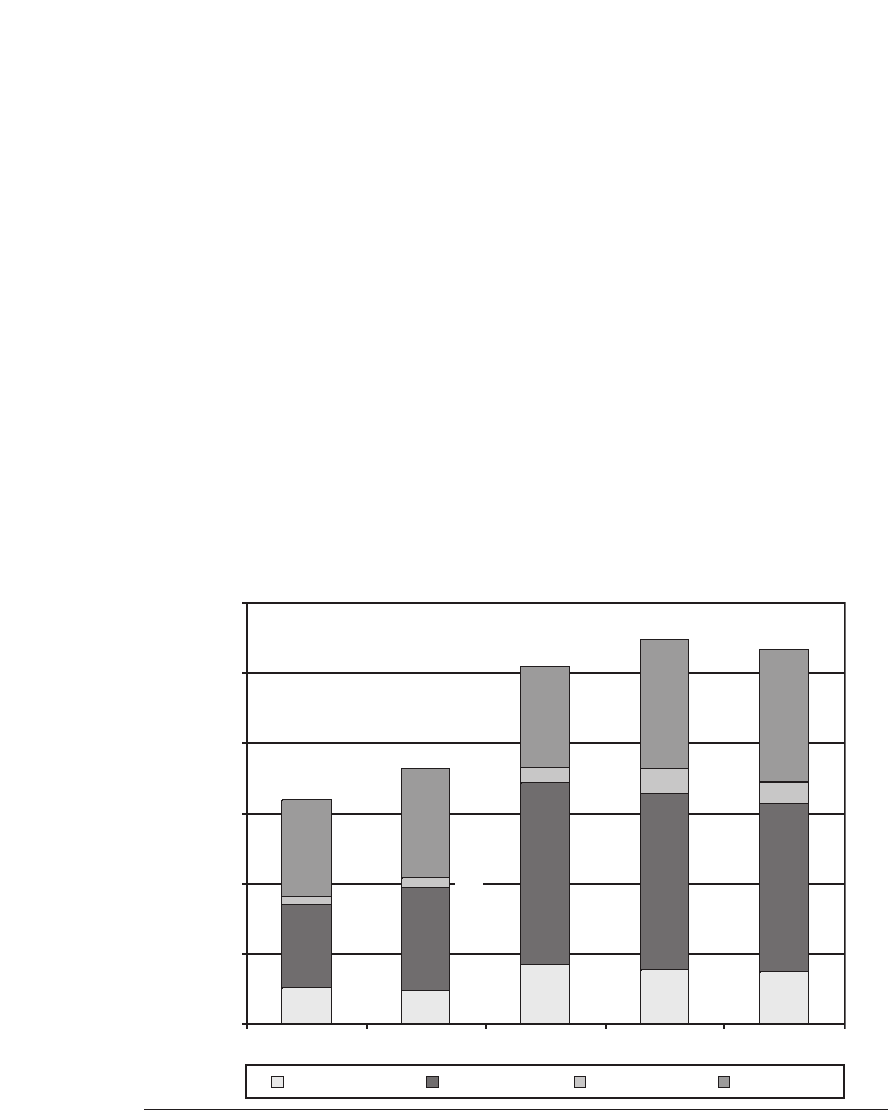
As shown in Figure 15.1, in 2000 5.3% (approximately 3.8 million) children
under the age of 18 lived in a household headed by grandparents, and of these,
1.4 million lived in a grandparent-headed household with neither parent being
Figure 15.1 Grandchildren in Grandparents’ Home, by Presence of Parents.
Sources:
Table CH-7: Grandchildren Living in the Home of Their Grandparents: 1970 to Present,
by
the U.S. Bureau of the Census, 2004, retrieved May 10, 2006, from www.census.gov
/population/socdemo/hh-fam/tabCH-7.pdf. Data from 1970 and 1980 censuses and 1991,
1997, and 2000, Current Population Surveys as reported in
America’s Families and Living
Arrangements: 2000
(U.S. Census Bureau, Current Population Reports, Series P20-537),
by J. Fields and L. Casper, 2001, Washington, DC: U.S. Government Printing Office, and
earlier reports.
1970 1980 1991 1997 2000
Percent of Children under 18
3.2%
3.6%
5.1%
5.5%
5.3%
0.5
0.5
0.9
0.8
0.7
2.5
2.4
1.2
1.5
2.6
0.1
0.1
0.2
0.3
0.3
1.8
1.9
1.4
1.6
1.4
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Both parents Mother only Father only No parent

400 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
Table 15.1
Percent of Children under 18 with Grandparent in Home by Number of
Parents in Home and Race: 1940−2001
Total Two Parents One Parent No Parent
Racial Racial Racial Racial
Diff. Diff. Diff. Diff.
Year White Black (W−B) White Black (W−B) White Black (W−B) White Black (W−B)
1940 10.3 16.0 −5.7 7.2 5.3 1.9 1.8 3.1 −1.3 1.3 7.6 −6.3
1950 10.6 18.5 −7.9 7.7 6.9 0.8 1.8 4.0 −2.2 1.1 7.6 −6.5
1960 6.8 15.8 −9.0 4.7 5.2 −0.5 1.4 4.4 −3.0 0.7 6.2 −5.5
1970 5.4 13.0 −7.6 3.0 3.5 −0.5 1.2 4.6 −3.4 0.9 4.9 −4.0
1980 4.8 12.2 −7.4 2.3 1.7 0.6 1.5 5.7 −4.2 1.0 4.8 −3.8
1991 5.3 14.9 −9.6 2.1 1.1 1.0 2.3 8.4 −6.1 0.9 5.4 −4.5
2001 6.8 14.8 −8.0 2.7 1.6 1.1 2.8 7.9 −5.1 1.2 5.1 −3.9
Sources: America’s Children: Resources from Family, Government, and the Economy,
by D. J. Hernandez and
D. E. Meyer, 1993, New York: Russell Sage Foundation; “Grandparenthood over Time: Historical and Demo-
graphic Trends” (pp. 23–39), by P. Uhlenberg and J. B. Kirby, in M. E. Szinovacz (Ed.),
Handbook on Grandpar-
enthood,
1998, Westport, CT: Greenwood Press;
The Diverse Living Arrangements of Children: Summer 1991
(Current Population Reports, Household Economic Studies, P70-38) by the U.S. Bureau of the Census, 1994,
Washington, DC: U.S. Government Printing Office, retrieved May 10, 2006, from http://www.census.gov
/population/socdemo/child/p70-38.pdf; and
Table C2: Household Relationship and Living Arrangements of Chil-
dren under 18 Years,
by the U.S. Bureau of the Census, 2001b, retrieved May 10, 2006, from http://www
.census.gov/population/www/socdemo/hh-fam/p20–537_00.html. Reprinted with permission.
present, a family structure we refer to as the “skipped generation.” Between
1970 and 1991, substantial increases occurred in the number of children living
with a single parent in a grandparent’s home. In 1970, approximately 817,000
or 1.2% of children lived with their mother in their grandparent’s home. By
1991, this increased to 1,674,000 or 2.6% of children. As shown in Figure 15.1,
there also was a considerable increase between 1991 and 1997 in the number of
grandchildren living with their grandparents only. In 1991, 1.4% of children
(937,000) lived with their grandparents only; by 1997 the number grew to 1.8%
(1,309,000). The number of these skipped-generation households (no parent
present) continued to increase in 2000, although other family structures involv-
ing grandparents remained stable or showed a slight decline.
As can be seen in Table 15.1, the likelihood of a child living with his or her
grandparents is strongly influenced by race. In 2001, African American children
were more than twice as likely as White children to be living with their grand-
parents. For both African American and White children, there has been a dra-
matic drop in the number of children living in a two-parent household along with
their grandparent. The number of White children who live with a single parent
and a grandparent increased by 55% between 1940 and 2001. In contrast, there
has been a 155% increase during the same period in the number of African Amer-
ican children living with a single parent and grandparent. The proportion of
White children living with a grandparent only (an indicator that the grandparent
is the sole caregiver of the grandchild) has been relatively stable since 1970. Al-
though the proportion of African American children living in this type of family
declined between 1960 and 1980, this trend has reversed itself in recent years and
grew approximately 6% between 1980 and 2001.

Parenting Grandchildren 401
D
EMOGRAPHIC
C
HARACTERISTICS OF
G
RANDPARENT
-H
EADED
F
AMILIES
Bryson and Casper (1999), using data from the 1997 Current Population Survey
(CPS), report that 51% of grandparent-headed families are maintained by both
grandparents, 43% by grandmothers with no spouse present, and only 6% by grand-
fathers alone, regardless of the presence of a parent. Among these families, substan-
tial differences emerge between grandmothers living in skipped-generation
families (no parent present) and other grandparent-headed family structures (i.e.,
grandmothers living with a grandchild and the grandchild’s parent; grandmothers
living with their spouse, a grandchild, and the grandchild’s parent; and grandfa-
ther-headed families). As shown in Table 15.2, single grandmother caregivers in
skipped-generation families were more likely than other grandparent heads of
household to be Black, poor, and in poor or fair health and less likely to have gradu-
ated from high school and be employed.
U.S. Census Bureau data do not allow one to determine how families headed by
grandparent caregivers differ from other families headed by grandparents who do
not live with grandchildren because the Census Bureau does not ask respondents
whether they are grandparents. Grandparent families are identifiable only if the
respondent has grandchildren in the household. To investigate how grandparents
caring for grandchildren differ from the general population of grandparents with-
out these care-giving responsibilities, Fuller-Thomson et al. (1997) investigated
the characteristics of grandparents who had assumed primary responsibilities for
their grandchildren for at least 6 months (“custodial grandparents,” as the authors
referred to them), using data from the 1992–1994 National Survey of Families and
Households (NSFH). They found that more than 1 in 10 grandparents (10.9% of
3,477 grandparents in the study) in the United States cared for a grandchild for at
least 6 months at some point in their lives. Among the final sample of 173 custodial
grandparents interviewed, 77% were women and the majority (62%) were non-
Hispanic White; 27% were Black, 54% were married, and 43% had less than a high
school education. The mean age of the custodial grandparents in 1993 was 59.4
years. They had mean incomes of $31,643 and 23% reported living in poverty.
When compared to grandparents with no primary responsibilities for a grandchil-
dren’s care, custodial grandparents were more likely to be younger, Black, women,
and living in poverty. These grandparent caregivers were less likely to have com-
pleted high school and less likely to be currently married.
In summary, a common profile of grandparent caregivers is emerging. First,
grandmothers are more likely to be caring for grandchildren than are grandfa-
thers. As has been noted, women are far more likely to provide the vast majority
of family care over their life course (Neal, Chapman, Ingersoll-Dayton, & Emlen,
1993) than men, who tend to assume a supportive and secondary role (Goldberg-
Glen & Sands, 2000). Thus, it is not surprising that the CPS data indicate that 62%
of grandparents who maintained families for their grandchildren in 1997 were
grandmothers (Bryson & Casper, 1999).
Second, many care-giving grandparents are younger than age 65, with many
still in their midlife (aged 45 to 55), which casts doubt on the “frail, dependent
grandparents” image. Many care-giving grandparents are still actively providing
care for their older parents and working part or full time (Jendrek, 2003).
Third, although the phenomenon of grandparent caregiving appears to have
become more common across racial groups, children living in grandparent-
headed households are disproportionately represented by minority groups. In
402
Table 15.2
Characteristics of Grandparents Who Coreside with Grandchildren
in Grandparent-Maintained Families: 1997
Grandparent-Maintained Families
Skipped- Three-Generational
Generational Household
Household (At Least
(No Parent) One Parent)
Grand- Both Grand- Both Grand-
mother Grand- mother Grand- father
Characteristics Total Only parents Only parents Only*
Grandmothers, total (number)
2,292 340 412 702 838 (X)
Percent distribution of grandmothers 100.0 100.0 100.0 100.0 100.0 (X)
Age
Under 45 19.4 6.9 14.8 24.2 22.9 (X)
45–54 36.0 34.1 35.2 30.1 42.0 (X)
55–64 29.5 36.9 36.4 25.4 26.5 (X)
65 and older 15.1 22.2 13.6 20.3 8.6 (X)
Race and Ethnicity
Caucasian 48.0 27.9 62.8 38.6 56.7 (X)
African American 31.0 53.5 18.8 45.4 16.0 (X)
Hispanic 16.4 15.8 15.3 12.5 20.5 (X)
Other 4.5 2.8 3.2 3.5 6.8 (X)
Education
< High school graduate 35.5 45.9 41.0 36.6 27.7 (X)
High school graduate 40.2 30.4 39.3 38.5 45.9 (X)
Some college 24.3 23.7 19.7 25.0 26.4 (X)
Marital Status
Married, spouse present 56.1 0.9 100.0 4.8 100.0 (X)
Divorced, separated 22.9 50.3 na 50.4 na (X)
Widowed 15.4 36.1 na 32.9 na (X)
Never married 5.5 12.7 na 11.9 na (X)
Work Experience in 1996
Did not work 43.6 61.8 46.3 38.2 39.3 (X)
Worked part-time 19.6 16.8 21.5 16.3 22.5 (X)
Worked full-time 36.9 21.4 32.2 45.6 38.3 (X)
Mean Income
Total household $43,783 $19,750 $41,709 $35,334 $61,632 (X)
Grandmother’s $14,063 $13,402 $11,028 $16,906 $13,440 (X)
Poverty Status
Poor 23.0 57.2 14.4 26.9 10.0 (X)
Not poor 77.0 42.8 85.6 73.1 90.0 (X)
General State of Health
Fair or poor 33.6 51.0 28.9 36.4 26.5 (X)
Good 31.2 27.9 32.4 26.4 36.0 (X)
Very good 21.9 12.0 27.2 22.9 22.6 (X)
Excellent 13.3 9.1 11.6 14.3 14.9 (X)
(continued)
403
Table 15.2
(Continued)
Grandparent-Maintained Families
Skipped- Three-Generational
Generational Household
Household (At Least
(No Parent) One Parent)
Grand- Both Grand- Both Grand-
mother Grand- mother Grand- father
Characteristics Total Only parents Only parents Only*
Grandfathers, total (number)
1,402 (X) 412 (X) 838 152
Percent distribution of grandfathers 100.0 (X) 100.0 (X) 100.0 100.0
Age
Under 45 14.9 (X) 11.0 (X) 16.9 13.8
45 to 54 32.0 (X) 23.7 (X) 38.4 19.3
55 to 64 32.6 (X) 38.8 (X) 29.9 31.0
65 and older 20.5 (X) 26.5 (X) 14.8 35.9
Race and Ethnicity
Caucasian 60.3 (X) 63.6 (X) 59.0 58.1
African American 18.3 (X) 19.5 (X) 16.2 26.0
Hispanic 17.3 (X) 14.6 (X) 19.2 14.1
Other 4.2 (X) 2.2 (X) 5.6 1.7
Education
< High school graduate 37.1 (X) 40.6 (X) 35.3 37.7
High school graduate 37.1 (X) 36.1 (X) 37.6 36.6
Some college 25.8 (X) 23.3 (X) 27.1 25.6
Marital Status
Married, spouse present 90.1 (X) 100.0 (X) 100.0 8.6
Divorced, separated 6.1 (X) (X) (X) (X) 56.0
Widowed 3.2 (X) (X) (X) (X) 29.0
Never married 0.7 (X) (X) (X) (X) 6.4
Work Experience in 1996
Did not work 27.9 (X) 30.6 (X) 22.7 49.3
Worked part-time 17.5 (X) 19.9 (X) 17.4 12.0
Worked full-time 54.5 (X) 49.5 (X) 59.9 38.7
Mean Income
Total household $53,811 (X) $41,709 (X) $61,632 $43,476
Grandmother’s $27,259 (X) $24,852 (X) $29,296 $22,561
Poverty Status
Poor 12.4 (X) 14.4 (X) 10.0 19.9
Not poor 87.6 (X) 85.6 (X) 90.0 80.1
General State of Health
Fair or poor 28.7 (X) 32.7 (X) 24.6 40.0
Good 33.9 (X) 31.1 (X) 35.6 31.9
Very good 22.0 (X) 21.5 (X) 24.4 10.1
Excellent 15.4 (X) 14.7 (X) 15.3 18.0
Note:
Numbers in thousands, Percent distribution of characteristics. (X) = Not applicable.
* Grandfather-maintained families may or may not include a parent of the children. The investigators combined
skipped- with three-generation families headed by grandfathers in their report due to the small sample size, as
compared to the size of other types of grandparent-headed families.
Adapted from
Coresident Grandparents and Grandchildren: U.S. Bureau of the Census, Current Population
Reports, P23–198.
by K. R. Bryson, and L. Casper, (1999), retrieved May 9, 2006, from http://www.census.gov

404 E
VIDENCE
-B
ASED
F
AMILY AND
C
OMMUNITY
P
RACTICE
2000, 12.1% of all African American children under 18 years of age were living
with grandparents, compared to 6.1% of Hispanic and 3.4% of Caucasian children
(U.S. Bureau of the Census, 2001b). With regard to the lifetime prevalence of
grandparent primary caregiving, a U.S. national study using the NSFH suggests
that about 30% of African American grandmothers and 14% of African American
grandfathers had assumed primary responsibility for a grandchild for at least 6
months (Szinovacz, 1998), compared with 11% of the total number of 3,477 grand-
parents in the study who did so (Fuller-Thomson et al., 1997).
Finally, one of the most striking findings is the disproportionately high level of
poverty among grandparent caregivers. In the 1997 CPS data, 57% of single grand-
mother caregivers in the skipped-generation families lived in poverty (Casper &
Bryson, 1998), and 58% of the 479 self-identified grandparent primary caregivers in
an American Association of Retired Persons’ study reported living on a fixed in-
come (Woodworth, 1996). Thus, the prototypical grandparent caring for a grand-
child is an African American single woman in midlife who is living in poverty.
CONTEXT OF GRANDPARENT CAREGIVING
R
EASONS FOR
P
ROVIDING
P
RIMARY
C
ARE TO
G
RANDCHILDREN
The available evidence suggests that grandparents do not seek out the role of co-
parent or caregiver to their grandchildren, but are thrust into the role because of
problems in the lives of their adult children (Goodman & Silverstein, 2002; Jen-
drek, 1993; Pruchno & McKenney, 2000). These problems include parental sub-
stance abuse (Burton, 1992; Goodman & Silverstein, 2002; Joslin & Brouard, 1995;
Kelley, 1993; Minkler & Roe, 1993; Pruchno & McKenney, 2000), child abuse, neg-
lect, or abandonment (Dubowitz & Feigelman, 1993; Jendrek, 1994), incarceration
(Dressel & Barnhill, 1994; Woodworth, 1996), divorce (Cherlin & Furstenberg,
1986), AIDS (Burnette, 1997; Joslin & Brouard, 1995), teenage parenthood (Good-
man & Silverstein, 2002; Pruchno & McKenney, 2000), and parental death (Jen-
drek, 1994). Other researchers note that the legal mandates and related changes
in child welfare reimbursement policies and practices, which have significantly
increased placement with relatives, help explain part of the increase in grandpar-
ent care (Bell & Garner, 1996; Harden, Clark, & Maguire, 1997).
However, the reasons grandparents assume primary care-giving responsibilities
for their grandchildren are very complex and interrelated. For example, a biological
parent’s dependency on alcohol or drugs may result in child abuse or neglect. Fi-
nancial difficulties resulting from parental unemployment were also found to be
common reasons for grandparents assuming primary care of grandchildren (Bur-
nette, 1997; Minkler, Berrick, & Needell, 1999; Woodworth, 1996). Thus, the reasons
for assuming a care-giving role for a grandchild are tied in fundamental ways to one
another. Although conceptually one can distinguish among the reasons, in the real
lives of these families they are so closely interrelated that efforts to distinguish the
primary from the secondary reasons for taking on the role are often quite arbitrary.
I
MPACT OF
C
AREGIVING ON
G
RANDPARENTS
Research examining the psychological well-being of grandparent primary care-
givers has documented the elevated psychological distress among this popula-
tion. Recent research has identified these older caregivers as “hidden patients”

Parenting Grandchildren 405
(Roe, Minkler, Saunders, & Thomson, 1996), particularly if they live in poor com-
munities or have insufficient economic resources (Joslin & Harrison, 1998).
Grandparent primary caretakers have generally been found to have elevated lev-
els of psychological distress, in particular depressive symptoms, compared to
grandparents who provide supplemental care to grandchildren (Bowers &
Myers, 1999; Musil, 2000), filial or spousal caregivers (Strawbridge, Wallhagen,
Shema, & Kaplan, 1997), age-matched peers who are not caregivers (Minkler,
Fuller-Thomson, Miller, & Driver, 1997), a normative sample of parents (Kelley,
1993), or members of the general population (Janicki et al., 2000; Kelley, Whitley,
Sipe, & Yorker, 2000).
In one of the more rigorously designed longitudinal studies of caregivers,
spanning 20 years, Strawbridge and his colleagues (1997) compared three groups
of caregivers (filial caregivers, spousal caregivers, and grandparent caregivers) to
noncaregivers. They found that, in 1974, filial and spousal caregivers did not dif-
fer from noncaregivers, but grandparent caregivers had poorer health than non-
caregivers and more stressful life events (e.g., serious illness, financial problems,
marital problems) than the other two groups. Analysis of the second wave of data
collected 20 years later revealed that the depressive symptoms of all three groups
were greater than that of noncaregivers. Also, grandparents reported poorer
mental and physical health and more activity limitations than the other two
groups. The authors concluded that filial and spousal caregiving constitute a new
burden in an otherwise “normal” life, whereas caring for grandchildren repre-
sents “yet another aspect of a difficult life course” (p. 505).
In addition, grandparent caregiving affects not only mental health but also
physical health. Grandmother caregivers experienced poorer physical health and
a greater number of physical limitations than grandmothers who were not care-
givers (Caputo, 2001) and biological mothers with low incomes (Bachman &
Chase-Landsdale, 2005). Single grandmother caregivers rated their health as
being poorer compared to married grandmother caregivers or married women
living with a spouse (Solomon & Marx, 1999). High rates of insomnia as well as
hypertension, back and stomach problems, and the frequent presence of multiple
chronic health problems have been reported in both national and smaller-scale
studies of grandparents raising grandchildren (Dowdell, 1995; Kelley, 1993; Roe
et al., 1996). When the caregivers were great-grandmothers or had several grand-
children, they experienced a greater decline in health over the previous year.
Great-grandparents or those caring for several grandchildren might lack the en-
ergy and vitality necessary to attend to the range of problems that resulted in
their rearing their grandchildren. However, these grandparents were likely to
minimize their health problems so that they might be up to the task of caring for
their grandchildren (Pinson-Millburn, Fabian, Schlossberg, & Pyle, 1996).
Although most research has focused on declines in physical and mental health
of grandparent caregivers, there is a growing attention to the effect of caregiving
on the grandparent’s social network. Increased social isolation has been widely
recognized as a consequence of caregiving generally, and more specifically
among grandparents caring for grandchildren. A study of urban African Ameri-
can grandparents by Burton and deVries (1992) found that the caregivers often
felt socially isolated. Those caring for grandchildren in skipped-generation
households as a result of parental AIDS or substance abuse experienced feelings
of alienation (Joslin & Harrison, 1998). Social alienation was also experienced by