Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

Ministry of Agriculture, Fisheries and Food (1992) Report
on the Review of the use of Food Additives in Foods
specially prepared for Infants and Young Children
FdAC/REP/12. London: HMSO.
Morton RE, Nysenbaum A and Price K (1988) Iron status in
the first year of life. Journal of Pediatrics, Gastroenter-
ology and Nutrition 7: 707–712.
Mughal MZ, Salama H, Laing I and Mawer EB (1999)
Florid rickets associated with prolonged vitamin D
supplementation. British Medical Journal 318: 39–40.
Pugliese MT, Blumberg DL, Hludzinski J and Kay S (1998)
Nutritional rickets in suburbia. Journal of the American
College of Nutrition 17: 637–641.
Stordy BJ, Redfern A and Morgan JB (1995) Healthy eating
for infants – mothers’ actions. Acta Paediatrica 84:
733–741.
Thomas M and Avery V (1997) Infant Feeding in Asian
Families. London: Office of National Statistics.
Wharton B (1996) Weaning: pathophysiology, practice and
policy. In: Walker WA and Watkins JB (eds) Nutrition in
Paediatrics, pp. 423–435. Hamilton: BC Decker.
Wharton B (1997) Nutrition in Infancy. British Nutrition
Foundation Briefing Paper, BNF.
Wilson AC, Forsyth JS, Greene SA et al. (1998) Relation of
infant diet to childhood health: seven year follow up
of cohort of children in Dundee infant feeding study.
British Medical Journal 316: 21–25.
Zlotkin S (1999) Vitamin D concentrations in Asian chil-
dren living in England. Limited vitamin D intake and
use of sunscreens may lead to rickets. British Medical
Journal 318: 1417.
Feeding Problems
E M E Poskitt, Department of Public Health Nutrition,
London School of Hygiene and Tropical Medicine, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Nutrition is of great importance in infancy. Infants
are entirely dependent on others for their nutrition
and carers may have difficulty recognizing their
needs. This dependence and infants’ high nutritional
requirements for growth and development make mal-
nutrition a relatively common problem. Prolonged
malnutrition can impair both somatic growth and
brain development.
Failure to Thrive
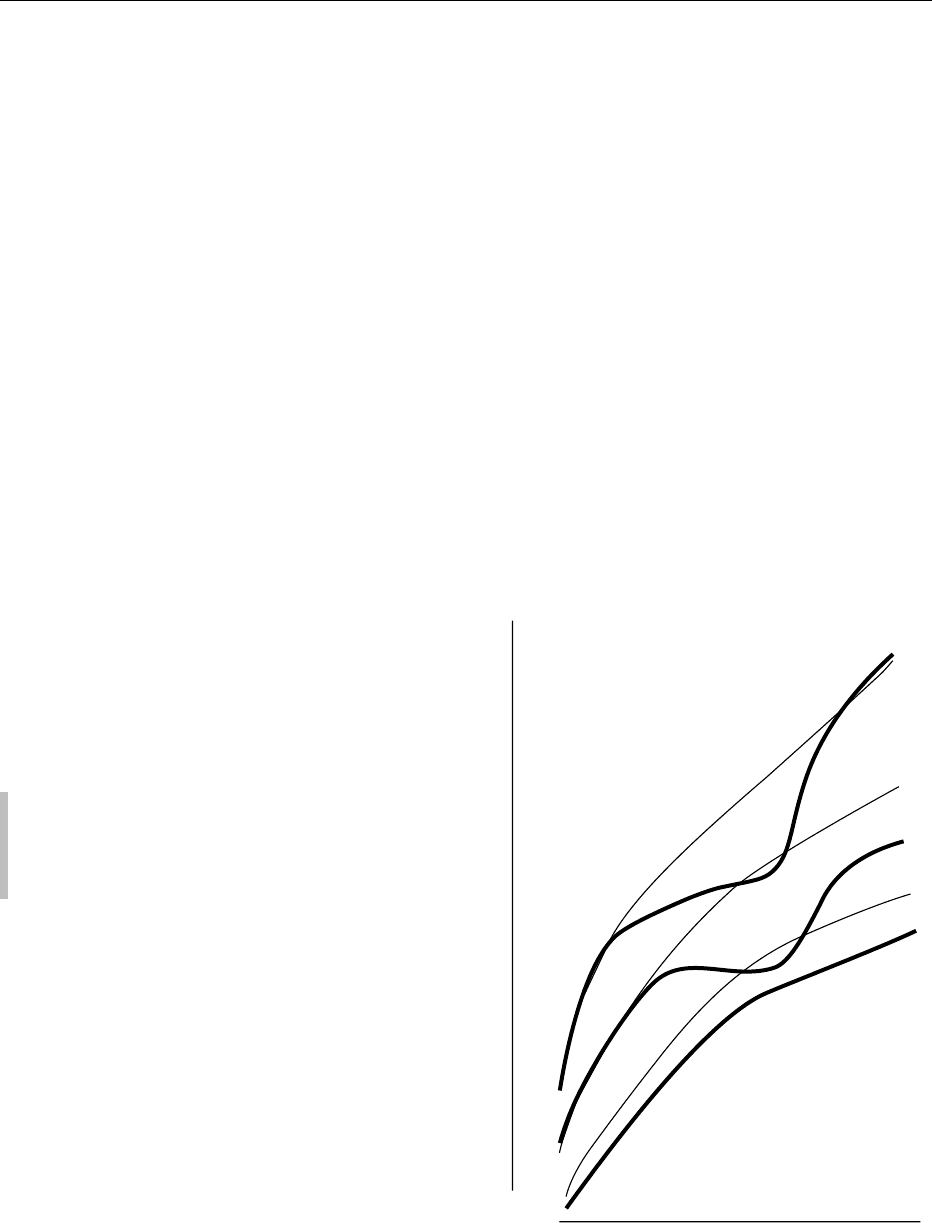
000 2 Failure to thrive (Figure 1) is failure to gain in height
and weight at the expected rates (determined from
recognized growth data). The causes are numerous
(Table 1) but if the precipitating causes can be
successfully treated, failure to thrive is followed by
accelerated or ‘catch-up’ growth (Figure 1a), pro-
vided extra food meets the nutritional needs of accel-
erated growth. Without extra nutrients, catch-up
growth is likely to be incomplete. Affected infants
may then resume normal growth rates, but along
lower growth centiles than previously (Figure 1b).
0003Some children with growth below the third centile
or 2sd weight-for-age or below (outside the rec-
ognized ‘normal’ range) may be labeled as failure-
to-thrive although growing at more or less normal
rates for age. They may have been low-weight for
gestational age at birth and always small (Figure 1c).
These constitutionally small children may show
delayed bone age, delayed adolescence, and some-
times late catch-up to more normal adult size.
0004Careful dietary histories should indicate which
infants are failing to thrive because of inadequate
intakes, inappropriately constituted feeds, or in-
appropriate weaning practices. Average milk or
formula intakes are 150 ml kg
1
day
1
(441 kJ kg
1
day
1
) for full-term normal infants. Around 6–8
weeks of age intakes often stabilize despite continuing
97
50
b
a
3
c
Weight
Age
fig0001Figure 1 Weight of children with (a) failure to thrive and com-
plete catch-up growth; (b) failure to thrive and failure of complete
catch-up growth; and (c) constitutional small size plotted against
the 3rd, 50th, and 97th weight-for-age centiles.
3300 INFANTS/Feeding Problems

increases in weight and intakes kg
1
day
1
thus
decrease.
0005 It may be difficult to assess the adequacy of milk
intake in breast-fed infants. Normal growth velocities
and general contentment after feeding suggest intakes
are adequate. If there is concern, weighing infants in
clean diapers prior to breast-feeding and then
weighing them again after feeding without diaper
change provides some indication of the weight, and
thus the volume, of milk consumed. This test
weighing must be for all feeds over 24 h since infants
may consume large feeds early in the morning and in
the evening, but relatively small amounts at other
times of day.
0006 When breast milk output seems insufficient for an
infant’s needs, improving maternal nutrition and in-
creasing the frequency of suckling may improve milk
secretion. Current recommendations are that infants
should be exclusively breast-fed until at least 4
months of age and preferably until 6 months of age.
Usually breast-feeding failure arises because of
inappropriate feeding practices (e.g., infrequent
suckling, especially in early lactation, or incorrect
positioning and failure by the infant to latch on).
Advice on feeding technique may resolve the
problems. However, mothers who are sick or very
malnourished may sometimes fail to produce suffi-
cient milk to support normal infant growth. The
decision whether to continue struggling to increase
breast milk production, to introduce infant formula
feeds, or to introduce weaning foods early is deter-
mined by individual circumstances such as the age of
the child and cause of breast-feeding failure. Failure
to thrive without evidence of nutritional inadequacy,
or secondary to persistent anorexia and vomiting,
requires urgent medical investigation.
0007Occasionally failure to thrive occurs without evi-
dence of clinical disease or nutritional inadequacy.
Children with such nonorganic failure to thrive may
eat well, sometimes excessively, but grow poorly.
Typically they are apathetic, showing little social
interaction, although some are restless and inatten-
tive. Developmental delay, particularly in social and
cognitive skills, is common. These children come
from home environments of social and/or emotional
deprivation. Environmental stress and lack of love
inhibit normal growth. Changing the home environ-
ment without necessarily changing the diet can induce
accelerated growth giving a dramatically improved
effect – confirming the diagnosis.
Vomiting
0008Most normal infants vomit occasionally and some
vomit frequently. Probably the most common cause
of persistent vomiting in infancy is laxity of the
gastroesophageal sphincter. The sphincter is the
spiral muscular area, 2–3 cm in length, at the lower
end of the esophagus. Sphincter competence is related
to the length of intraabdominal sphincter (which in-
creases with age) and to intragastric pressure. Com-
petence tends to be poor at birth but improves after
the first 2 weeks of life, regardless of gestational age.
The fluid diets of young infants and the high volumes
of liquid needed to meet nutritional requirements
produce gastric distension, high intraabdominal
tension, and easy regurgitation. Thickening feeds
to increase resistance to regurgitation, feeding
smaller feeds more frequently, and raising the head
end of the cot help reduce gastric distension and
regurgitation. As infants grow, consume more solid
food and adopt an upright posture, reflux ceases to be
a problem.
0009Feeding problems, including gastroesophageal
reflux, are common in children with neurological
handicap. Failure to thrive can be severe and may
improve with intragastric feeding through gastro-
stomy, but this exacerbates gastroesophageal reflux.
Surgical fundoplication is usually performed, prior to
gastrostomy, to control reflux.
0010Vomiting can be a symptom of serious gastrointest-
inal or parenteral disorder. When infants vomit and
fail to thrive, vomit bile or blood, or vomit to the
extent of causing dehydration, medical investigation
is required urgently.
tbl0001 Table 1 Classification of nutritional problems associated with
failure to thrive
Basic problem Examples
Inadequate intake Poverty; famine; ignorance of nutrient
needs
Vomiting: all causes
Feeding problems, including
neurological damage
Anorexia
Increased losses Protein-losing enteropathy
Glycosuria; proteinuria
Exfoliative skin conditions
Suppuration
Failure to absorb food Cystic fibrosis
Gluten-sensitive enteropathy
Giardiasis
Lactose intolerance
Failure to utilize food Inborn errors of metabolism
Endocrine problems
Micronutrient deficiencies, e.g., zinc
Chronic renal failure
Emotional deprivation
Increased requirements Small-for-dates and premature infants
Catch-up growth
Congenital heart disease: left-to-right
shunt
INFANTS/Feeding Problems 3301

Diarrhea
0011 Diarrhea is an increase in total stool output, usually
from increase in water content, volume, and frequency
of stools. The color, consistency, and frequency of
stools vary widely both between different infants
and in the same infant on different occasions. Exclu-
sively breast-fed infants tend to have frequent watery
yellow stools. Formula-fed infants have less frequent,
greenish, drier-looking stools.
0012 In infancy diarrhea is commonly part of either
a specific gastrointestinal or a generalized (usually
viral) infection. Infectious diarrhea has an acute
onset but is usually short-lived and associated with
other signs of infection: pyrexia, vomiting, anorexia,
and general malaise. Weight loss from anorexia and
dehydration are common. Weight recovery is gener-
ally rapid and complete. Acute diarrhea has little
effect on long-term weight-for-age and even less
impact on long-term height-for-age. However, chronic
diarrhea and significant growth faltering are common
with some gastrointestinal infections (especially rota-
virus, Giardia lamblia, and Entamoeba histolytica).
0013 Malnutrition causes profound changes to gastro-
intestinal mucosal structure and function. This pre-
disposes malnourished children to severe diarrheal
infection and high mortality from diarrheal illness.
0014 All diarrhea should be managed with extra fluids,
usually in the form of oral rehydration solution
(ORS). ORS suitable for most infant diarrhea has
lower sodium and chloride content than that intended
for rehydration in adults.
0015 Diarrhea which is persistent and associated with
failure to thrive, dehydration, bleeding or other
obvious illness, requires medical investigation.
Toddler diarrhea
0016 Some young children persistently pass watery stools
or have bouts of loose watery stools alternating with
episodes of constipation without evidence of infec-
tion, malnutrition, or other ill health. The diarrhea
stools are typically voluminous and watery with bits
of undigested food in them, indicating the visible bean
husks, tomato skins, and other vegetable matter pre-
sent, although less obviously so, in normally formed
stools. Children with toddler diarrhea are active and
thriving but their parents are usually very concerned.
0017 Toddler diarrhea has no recognized specific path-
ology and probably has many causes. Whole-gut
transit time is reduced but there is no evidence of
abnormal duodenal or jejunal secretion, nor of mal-
absorption. Minor infection may set off bouts of
diarrhea and in some children there is a family history
of response to stress with diarrhea. Poor hygiene and
low-grade infection associated with constant pacifier
(dummy) sucking and prolonged bottle-feeding may
contribute to the problem.
0018Many affected children have high intakes of
sweetened fruit juices and/or low intakes of dietary
fat. High fluid intakes with high simple carbohydrate
content encourage rapid intestinal transit which over-
whelms small intestinal function, so sugars reach the
large intestine unabsorbed. These and their fermenta-
tion products in the colon stimulate osmotic diarrhea.
Reducing fluid intakes, particularly of sweetened
juices and carbonated drinks, reduces the symptoms
in some toddlers. Changing to more adult diets with
higher concentrations of complex carbohydrates
and fats can also reduce diarrhea. Lipids in the
ileum slow duodenal and jejunal transit time (the
ileal brake) and may modulate mucosal contact time
and the absorption of intestinal luminal contents.
Graduating to cup-feeding usually results in less ex-
cessive fluid intakes and, particularly if pacifiers are
avoided, encourages more hygienic feeding practices.
0019Toddler diarrhea usually resolves as children move
on to more mature diets and develop continence. It is
unusual after the age of 6 years.
Micronutrient Deficiencies
0020Significant micronutrient deficiencies, other than for
iron, are rare in normal-weight, full-term healthy infants
in developed countries. Vitamin D deficiency rickets
can be a problem in low-birth-weight (LBW) infants
and noncaucasian infants. In developing countries low
levels of vitamin A are associated with high morbidity
and mortality from diarrheal diseases, respiratory infec-
tions, and measles. Iodine deficiency is also common.
Many countries now have supplementation programs to
prevent vitamin A and iodine deficiency.
Iron Deficiency
0021The human fetus has high hemoglobin levels to
accommodate low oxygen tension in utero. After
birth, in response to the high oxygen tension in the
extrauterine environment, the bone marrow becomes
relatively quiescent and hemoglobin levels decline.
Eventually (usually at 4–6 weeks of age) the bone
marrow becomes more active again but by then
infants have grown and their blood volumes have
expanded. Hemoglobin levels remain below adult
levels, at 11–12 g dl
1
, until late childhood.
0022Where infants are small and growing very rapidly
(e.g., premature and small-for-dates infants), with
initially low total blood volume and low total body
iron, the need for iron for new blood formation may
soon exceed the iron stored, so anemia results. Once
body weight has doubled, all infants are at risk of iron
deficiency since, without good external sources of
3302 INFANTS/Feeding Problems
iron, iron stores of the body will be distributed over
twice the blood volume, and hemoglobin levels will
have halved. However, iron supplementation should
probably be avoided in exclusively breast-fed infants
unless they show clinical evidence of deficiency, since
lactoferrin is a major immunological component of
breast milk. It binds iron in the small intestine,
speeding absorption and inhibiting multiplication of
iron-dependent bacterial pathogens. Iron fortification
of infant formulas reduces the prevalence of severe
iron deficiency in nonbreast-fed infants.
0023 Iron sufficiency is important. Table 2 lists some
factors predisposing to iron-deficiency anemia. The
frequency of iron-deficiency problems is an indication
of the small margin of safety between requirements
for iron and the quantity of iron young children are
likely to ingest and absorb from their diets. Low-
grade iron deficiency can impair growth rates, intel-
lectual function, and the immunological response to
infection. In countries where malaria is common,
anemia resulting from iron deficiency puts infants at
great risk of life-threatening severe malarial anemia.
Vitamin D Deficiency: Rickets
0024 Rickets used to be common in weanlings. The Clean
Air Act (1956) probably did as much to reduce rickets
in the UK as any medical intervention, since vitamin
D metabolites are predominantly derived from irradi-
ation of 7-dehydrocholesterol in the skin by sunlight
of wavelength around 300 nm.
0025 Rickets is still seen in the UK in newborn Asian
infants and mothers. The mothers have both inad-
equate absorption of dietary vitamin D and inadequate
skin synthesis of endogenous vitamin D because of
indoor habits and clothing cover when out of doors.
Low calcium absorption due to low dietary intake
and the high phytate content of traditional flours
exacerbates the need for vitamin D to optimize calcium
absorption from the small intestine. Skin pigmentation
increases the need for sunlight exposure when levels of
ultraviolet light of appropriate wavelength are low
(e.g., winter in northern latitudes).
0026Infants born to vitamin D-deficient mothers may
present with hypocalcemic tetany and convulsions
soon after birth or with rickets in the weaning period.
The incidence of rickets in Asian children is diminish-
ing in the UK as Asian women in this country adopt
lifestyles more suited to northern latitudes and their
need for vitamin D supplementation is better recog-
nized. However, signs of vitamin D deficiency in
mothers and children are widely reported from the
Middle East where there is plenty of sunshine of
vitamin D synthesizing wavelength, but little social
opportunity for women and children to expose their
bodies to the sunlight.
Vegetarian Diets in Infancy
0027Infants weaned on to vegetarian diets may become
deficient in a variety of nutrients. If diets include eggs
and milk, it is not difficult to achieve dietary require-
ments, particularly if breast milk or infant formula is
continued as a milk source beyond the first year of
life. Milk usually provides a substantial proportion of
riboflavin, calcium, and total energy intake in wean-
ling children. Infant formula can provide a fairly
absorbable dietary source of iron which may other-
wise be deficient.
0028Vegetarian diets tend to be of low energy density
because of high-fiber and low-fat content. Children
should be fed frequently (at least four times a day) to
enable them to consume the volumes of food neces-
sary to meet nutrient needs. No vegetable protein
contains the full range of essential amino acids so
diets should include a variety of protein sources
(e.g., beans, lentils, cereals, dark green leaves, soya
and homogenized nut products).
0029It is difficult to achieve adequate nutrition in very
young children with vegan, macrobiotic, and other
strict vegetarian diets. These diets are not recom-
mended for infants unless there is close pediatric
dietetic supervision.
Low-birth-weight Infants
0030The problems of both premature and LBW for gesta-
tional age (small-for-dates or SFD) infants are similar,
although the greater immaturity of the premature
infants’ gastrointestinal tracts and of other organs
makes the nutrition of the former more difficult
than that of the latter. In both groups there is a need
for more nutrients per unit of body weight to cope
tbl0002 Table 2 Classification of problems predisposing to iron
deficiency in childhood
Basic nutritional problem Example
Inadequate intake Early introduction to cows’ milk
Prolonged exclusive breast-feeding
Poor quality of weaning diet
Strict vegetarian diet
Increased losses Bleeding disorders
Reflux esophagitis
Failure to absorb Celiac disease
Pyrexia
Iron in ferric form
High-phytate diet
Failure to utilize Chronic infection
Hypothyroidism
Riboflavin deficiency
Increased requirements Rapid growth: low-birth-weight infants
Catch-up growth
INFANTS/Feeding Problems 3303
with the rapid growth to parallel intrauterine growth
in premature infants and catch-up growth in SFD
infants. The small stomach volumes of LBW infants
restrict the volumes which can be fed at any one time
without causing apnea, vomiting, or necrotizing
enterocolitis. Respiratory problems in premature
infants may also restrict the amount of enteral food
tolerated. Thus there is a conflict between increased
(proportionate to body weight) nutrient needs, espe-
cially for protein, calcium, phosphate, fluid, and
energy, and the amounts of food that can be adminis-
tered safely. Even when LBW infants are fed paren-
terally there are restrictions on the fluid volumes, and
thus the quantity of nutrients, that can be given safely.
The high demands for growth and development,
particularly for the brain, lead to deficiencies of
some nutrients which are usually synthesized by the
body. This critical nutrient status applies to the long-
chain polyunsaturated fatty acids, docosahexaenoic
and arachidonic acids, and possibly also carnitine,
nucleotides, and other nutrients. For this reason
breast milk, which has high levels of these nutrients,
may have advantages over infant formulas for the
nutrition of LBW infants, if supplemented with
energy to meet the high requirements of these infants.
However, manufacturers, aware of the physiological
needs of LBW infants, are gradually developing
formulas which aim to meet these special needs.
0031 Table 3 lists the problems of LBW infants which
are discussed elsewhere. LBW infants should be
supplemented at least with vitamins A, C, D, and
folate over the first year of life. Iron supplementation
in the neonatal period risks encouraging bacterial
infection and damage by free iron radicals, since
iron stores are replete following temporary bone
marrow inactivity associated with high hemoglobin
levels at birth. However, iron supplementation is ad-
visable in formula-fed infants after the first 4 weeks.
Iron supplements should probably not be given at all
to wholly breast-fed infants unless they show hema-
tological evidence of iron deficiency, since free iron in
the gastrointestinal tract can counteract the protect-
ive effects of lactoferrin.
Allergy
Cows’ Milk Protein Intolerance (CMPI)
0032Food allergies, particularly CMPI, are frequently diag-
nosed in infants. True CMPI affects between 1.5% and
5% of the population of western Europe. In families
with a strong atopic history the incidence may be much
higher. Cows’ milk protein intolerance most commonly
develops in children under 2 months of age, although
it may develop at a later age after gastrointestinal
surgery, malnutrition, or gastrointestinal infection.
0033Children with diarrhea and/or blood loss in associ-
ation with CMPI may show villous atrophy and
increased inflammatory cell infiltrations on jejunal
biopsy, or acute colitis on sigmoidoscopy. Those
with respiratory symptoms may present with pul-
monary hemosiderosis which resolves on removal of
all cows’ milk-containing products from the diet.
However, for most children, manifestations of CMPI
are varied and nonspecific.
0034Infants who vomit, have diarrhea, have a rash, or
cry a lot, are liable to be diagnosed as CMPI. They are
put on to commercial cows’ milk-free formulas and
may seem to improve. Improvements may have
been coincidental or as a result of mothers feeling
reassured that ‘something was being done.’
0035Commercial cows’ milk protein-free formulas are
also lactose-free. Excluding formula and cows’ milk
products from the diet does not distinguish between
CMPI and lactose intolerance. Children with lactose
intolerance commonly have a preceding history of
gastrointestinal infection, surgery, or malnutrition.
They have loose stools, weight loss, and abdominal
distension. Stools are acid and contain reducing sub-
stances. Thus, if infants’ stools show pH > 5.1 and
have no reducing substances in them and symptoms
resolve on cows’ milk protein-free diet but recur when
milk protein is reintroduced, CMPI is likely.
0036Where the child’s symptoms have been dramatic
(e.g., angioneurotic edema; profuse life-threatening
tbl0003 Table 3 Nutritional problems of low-birth-weight infants
Problem Precipitating factors
Immediate
hypoglycemia
Limited liver glycogen
Delay in mobilizing fat stores
Problems with supplying nutrition
Immediate
hypocalcemia
Loss of high calcium flux across
placenta
Immaturity of calcium homeostasis
Occasionally maternal vitamin D
deficiency
Later poor growth Low energy density of breast milk
Poor tolerance of other
energy/nutrient-dense feeds
Poor fat absorption by immature infants
Increased needs due to
bronchopulmonary dysplasia
Bone disease of
prematurity
Substrate deficiency, especially
phosphate
Renal calcium loss from acidosis
and/or diuretics
Vitamin D, protein, or copper
deficiency
Anemia Vitamin E deficiency increasing early
hemolysis
Folate deficiency
Iron deficiency
3304 INFANTS/Feeding Problems

diarrhea), challenging the diagnosis of CMPI by
reintroduction of milk and milk products can be
dangerous. Children should only be challenged with
milk under hospital supervision and even then with
great care.
0037 The particular elements of the cows’ milk protein
causing allergenic responses vary. At least 18 com-
ponents that can induce antibody formation have
been identified. When purified protein fractions are
used as challenges, b-lactoglobulin levels and casein
produce symptoms in over 60% of affected individ-
uals. Antibodies to cows’ milk protein are widespread
and neither their presence, nor their levels in the
blood, correlate well with reactions to cows’ milk.
0038 Breast-fed infants often show circulating cows’ milk
protein antibodies. Changing from breast-feeding to
cows’ milk formula feeding can, very rarely, precipi-
tate dramatic anaphylactic symptoms of angioneuro-
tic edema with acute and very dangerous swelling of
tissues around the neck and airway. Relevant proteins
from the cows’ milk consumed by the mother are
thought to be transferred to affected infants either
across the placenta or in breast milk, causing sensi-
tization. The infants are then desensitized by the
small amounts of antigen in maternal milk but are
overwhelmed when confronted with a large load of
antigen from formula feeding.
0039 The management of CMPI involves removal of all
cows’ milk protein-containing products from the diet.
Pediatric dietetic advice is advisable since milk and
milk products continue to contribute significant
amounts of energy and other nutrients to normal
children’s diets, even after the start of mixed feeding.
Difficulties in meeting nutritional needs on milk-free
weaning diets can lead to undernutrition. Soya-based
infant formulas can be helpful but infants with CMPI
may also develop soya protein intolerance. Hydro-
lyzed cows’ milk protein formulas are more suitable
for treatment of CMPI but are rather unpalatable (to
mothers anyway), not available in supermarkets in
the UK, and costly.
0040 Tolerance to cows’ milk protein usually develops as
children move into the second or third year of life.
Eczema
0041 The extent to which food intolerance is relevant to
the development of infantile eczema remains contro-
versial. Some infants with atopic eczema show signifi-
cant improvement in their skin problem when all milk
products are withdrawn from the diet. Others only
improve when put on very restricted lists of foods.
Studies of infants with familial high risk of atopic
eczema suggest that eczema may be prevented in
some infants by exclusive breast-feeding for the first
6 months of life. Moreover, exclusively breast-fed
infants who do develop eczema may have become
sensitized to foreign proteins transferred through the
breast milk.
Other Food Allergens
0042Other food allergies are quite common in infancy,
especially in those with an atopic family history.
Common precipitants are egg protein, citrus fruits,
nuts (not advised for young children anyway because
of the risks of inhalation), and the food colorants
tartrazine and quinoline yellow. Diarrhea, vomiting,
rashes, wheezing and – rarely – behavioral disturb-
ances may occur. (Most behavioral problems are dis-
ciplinary rather than allergic.) The pattern of
response in each child is usually repeated on subse-
quent contact with the allergen but there is great
variation in the pattern of individual responses.
Colic
0043Around 3 months of age healthy infants often develop
bouts of fractiousness and inconsolable crying, usu-
ally in the early evening. Their abdomens become
tight and distended, probably because of the air swal-
lowed whilst crying. Infants tend to flex their legs
when crying and this may be interpreted as abdom-
inal pain. ‘Three-month colic’ is an ill-defined prob-
lem with a wide range of symptomatology. In the long
term, colic resolves without specific treatment. It may
be a behavioral rather than a medical problem.
Nevertheless, it causes great distress to the child and
parents. Removal of cows’ milk formula and substi-
tution with nonallergenic formula or soya protein
formula has sometimes been associated with im-
provement. However it is difficult to know if this
has anything to do with resolution of symptoms in a
benign self-limiting condition.
Cot Death: Sudden Infant Death
Syndrome
0044Sudden unexpected infant death (SUID) affects about
1 in 500 infants in the UK. The condition is of mixed
etiology, since detailed history and autopsy reveal cause
of death or evidence of illness in many of the infants.
There remains a group of SUID infants for whom
detailed investigation shows no adequate explanation
for death. These are the cases of true ‘sudden infant
death syndrome’ (SIDS). In the past, anaphylactic
shock from acute CMPI was sometimes cited as pos-
sible etiology for SIDS since SUID is more common in
formula- than in breast-fed infants. Some infants have
postmortem evidence of milk/formula in the respira-
tory tract, perhaps as a terminal event. However, true
SIDS is probably not more common in formula-fed
INFANTS/Feeding Problems 3305

than breast-fed infants. It now seems likely that a major
component of death in SIDS relates to impaired cardi-
orespiratory arousal. Putting infants to sleep supine,
rather than prone or on their sides, has reduced SIDS
by about 35% in many countries.
0045 Another nutritional explanation proffered for
some forms of SUID is undiagnosed inborn errors of
metabolism involving inhibition of breakdown of
long-chain fatty acids. Children with inborn errors
of this kind are unable to metabolize fats to cope
with the stress of fasting and die of hypoglycemia.
Postmortem examination reveals acute fatty degener-
ation of the liver. In such very rare cases, SUID may be
familial since inborn errors of metabolism involving
fatty acid breakdwon are inherited, usually by auto-
somal recessive genes.
Teething Problems
0046 Teeth are erupting more or less continuously between
6 and 30 months. Teething children may show exces-
sive salivation, gingival swelling, and general irrit-
ability. These symptoms may exacerbate existing
illness but there is no evidence that teething causes
fever or diarrhea. Rubbing the gums with cool cloths
or giving infants firm objects to bite may reduce
teething discomfort.
0047 Most children develop their first teeth around 6
months of age but some do not develop teeth until
around 2 years. Late tooth erupters usually cope well
with chewing and should be encouraged to progress
in the weaning process in the normal way.
Nursing Bottle Syndrome: Rampant Caries in
Infancy
0048 Nursing bottle syndrome is the rampant carious de-
struction of the upper incisors in young children.
Although associated with offering bottles of juice/
milk or pacifiers sweetened with sugary solutions to
infants when they are ready to sleep, rampant caries
in this age group probably also reflects underlying
enamel hypoplasia in the primary teeth which is
secondary to prematurity or to maternal nutritional
deficiencies in pregnancy.
0049 Constant bathing of upper incisors with sugary
fluids, together with reduced salivary secretion and
reduced mouth movements at night, encourages the
development of plaque. Streptococcus mutans, which
survives well at low pH, collects under plaque and
adheres to tooth enamel. Enamel is eroded, allowing
opportunity for further tooth infection by other bac-
teria. Excessive vomiting, by creating an acid environ-
ment in the mouth, may contribute to the risk. Teeth
in the front of the upper jaw are reduced to carious
discolored stumps. Children may become faddy
eaters due to the discomfort of chewing meat and
biting vegetables and fruit.
0050Fluoridation of water supplies with one part per
million of fluoride protects against dental caries. If
water is not fluoridated, children can be supple-
mented with fluoride 1.25 mg day
1
in infancy and
1.5 mg day
1
between 1 and 3 years. Regular, at least
daily, tooth brushing should be taught from the first
appearance of teeth. Adults should supervise loading
children’s toothbrushes with small pea-sized lumps of
toothpaste since small children may eat toothpaste
rather than spit it out after cleaning their teeth. As
much as 1.66 mg of fluoride could be consumed by
small children brushing their teeth inexpertly twice
a day with fluoridated toothpaste.
0051All food, and particularly sweetened drinks, should
be discouraged after tooth brushing at night.
See also: Anemia (Anaemia): Iron-deficiency Anemia;
Cholecalciferol: Properties and Determination, Dental
Disease: Etiology of Dental Caries; Food Intolerance:
Types; Growth and Development; Inborn Errors of
Metabolism: Overview; Malnutrition: The Problem of
Malnutrition; Preterm Infants – Nutritional
Requirements and Management; Tocopherols:
Properties and Determination; Vegetarian Diets
Further Reading
Department of Health (1994) Weaning and the Weaning
Diet. Report on Health and Social Subjects, no. 45.
London: Her Majesty’s Stationery Office.
Hunt CE (2000) Sudden infant death syndrome. In:
Behrman RE, Kliegman RM and Jenson HB (eds)
Nelson’s Textbook of Pediatrics, 16th edn, pp.
2139–2143. Philadelphia: WB Saunders.
Filer LJ, Jr. (ed) (1989) Dietary Iron. Birth to Two Years.
New York: Raven Press.
Johnson D and Tinanoff N (2000) Dental caries. In: Behr-
man RE, Kliegman RM and Jenson HB (eds) Nelson’s
Textbook of Pediatrics, 16th edn, pp. 1114–1116.
Philadelphia: WB Saunders.
Simeon DT and Grantham-McGregor SM (1991) Nutri-
tional deficiencies and children’s behaviour and mental
development. Nutrition Reviews 3: 1–24.
Skuse D, Reilly S and Wolfe D (1994) Psychosocial adver-
sity and growth during infancy. European Journal of
Clinical Nutrition 48 (suppl. 1): S113–S130.
Standing Committee on Nutrition, British Paediatric Asso-
ciation (1988) Vegetarian weaning. Archives of Disease
in Childhood 63: 470–478.
Stevenson RD and Allaire JH (1991) The development of
normal feeding and swallowing. Pediatric Clinics of
North America 38: 1439–1453.
Walker-Smith J and Murch S (1999) Toddler diarrhoea. In:
Diseases of the Small Intestine in Childhood, 4th edn,
pp. 364–366. Oxford: Isis Medical Media.
Widdowson EM (1947) Mental contentment and physical
growth. Lancet i: 1316–1318.
3306 INFANTS/Feeding Problems

INFECTION, FEVER, AND NUTRITION
C J Field, University of Alberta, Edmonton, Alberta,
Canada
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Infection is a broad term that encompasses a number
of pathological situations initiated by invasion of in-
fectious organisms. An effort to reduce the number of
infectious incidences is a primary focus for those who
work in public health but also for those who work in
the clinical setting. Infections are responsible for
worsening the nutritional status of patients, doubling
the length of hospital stay, increasing the number of
medical and surgical procedures required, delaying
the provision of adjuvant therapies, and significantly
reducing patients’ quality of life. This article will
briefly review the immune response/role in infection
and fever, the importance of nutrition to the immune
system, and the role of nutrition and specific nutrients
on the response to fever and infection.
The Immune Response to Infection
0002 The immune system (cells and molecules responsible
for immunity) is defined as part of the host’s defense
against destructive forces from outside the body (i.e.,
bacteria, viruses, and parasites) and those from
within, such as malignant and autoreactive cells.
Appropriate interactions between the different cells
of the immune system are necessary to eliminate
infectious organisms (Table 1). The purpose is to
disadvantage and destroy invading organisms, while
protecting healthy tissue from the damaging
influences of the compounds produced during the
response. Cytokines and other compounds play a
central role orchestrating the immune response to
infectious organisms. However, the proinflammatory
cytokines and other molecules produced during
the inflammatory response also pose a danger to the
host. The host response (cytokines and acute phase
response) designed to fight infection is partially
responsible for a serious and life-threatening meta-
bolic condition called sepsis. Sepsis is characterized
by an unregulated host inflammatory response and
the presence of bacteria (though primary invasion or
secondary to other infections) or their products in the
bloodstream.
The Innate Immune System and Infection
0003The innate immune system comprises defenses that
are present early in life that function without
depending on previous exposure to a particular
pathogen, thereby providing the first line of defense
that protects the host during the 4–5 days it takes
for lymphocytes in the acquired immune system to
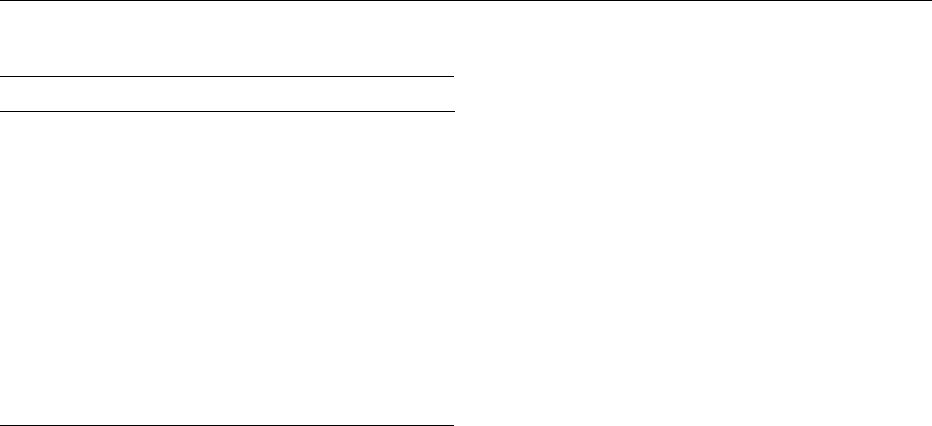
become activated. The major components of the
innate immunity are illustrated in Figure 1. The resist-
ance to bacterial invasions is thought to depend
primarily on nonT-cell branches of immunity such
as physical barriers (skin and mucous membranes),
tbl0001 Table 1 Immune responses to some common infectious agents
Infection type Examples Immuneresponse
Viruses HIV, influenza, rhinovirus
.
Humoral immune system blocks initial infection and recruits
other immune cells
.
Cell-mediated response is most effective at destroying cells
once infected with virus
Parasites Tr i c h in e ll a , Helminths
.
Low immune response, as there is no of the infectious agent
inside the host’s cells
.
May be some humoral and inflammatory response from B-cells
and macrophages/neutrophils near the invasion site
Protozoa Malaria
.
Bloodborne protozoa are destroyed by B-cell antibodies
.
Once cells are infected, cells are destroyed by cell-mediated
functions
Intracellular bacteria Listeria monocytogenes,
Mycobacterium tuberculosis
.
Cell-mediated, delayed-type hypersensitivity response
important in destroying intracellular bacteria
.
Stimulates a type-2 helper T-cell response (pattern of
cytokines)
Extracellular bacteria Streptococcus pneumoniae
.
Humoral immune system (located in lymphoid tissues
throughout the body) secretes antibodies
Sepsis (systemic inflammatory
response system)
Endotoxin, lipopolysaccharides
.
Caused by a dysregulated inflammatory response to an
infectious agent
INFECTION, FEVER, AND NUTRITION 3307
neutrophils, macrophages, complement, and acute
phase proteins. If infectious organisms penetrate this
barrier, the innate immune system responds immedi-
ately by activating the acquired immune system. If the
pathogens are bloodborne, the reticuloendothelial
system becomes involved.
The Acquired Immune System and Infection
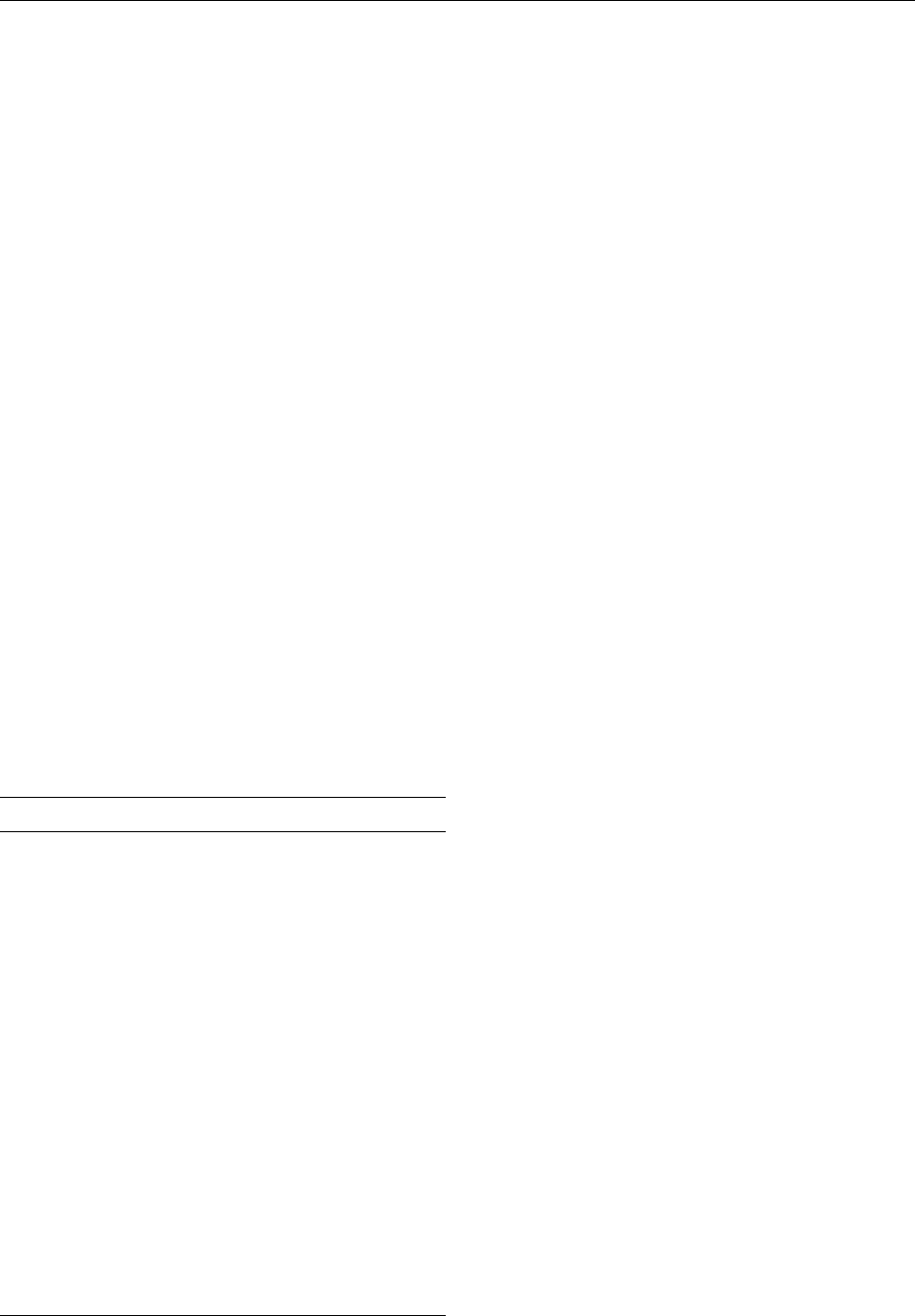
0004 The acquired (or adaptive) immune response de-
velops over one’s lifetime in response to environ-
mental challenges (pathogens/antigens). The cells
that comprise the acquired immune defense are illus-
trated in Figure 2. T- and B-lymphocytes (cells) are the
primary cells of this arm of immune system. The T-
cell population is divided into two basic subsets CD4
(helper/inducer) and CD8 (cytotoxic/suppressor)
cells. T-cells play multiple roles functions including
providing help to B-cells, stimulating the inflamma-
tory response, maintaining antigen-specific memory
and producing cytokines. Once activated, some
T-cells can directly destroy cells (via cytotoxic killing)
infected with intracellular pathogens. B-cells produce
and secrete antibodies for the elimination of extracel-
lular pathogens and parasites. B-cells can also serve as
antigen-presenting cells and activate T-cells.
The Mucosal Associated Lymphoid Tissue
0005 Mucosal tissues (contain components of both the
innate and acquired immune system) are strategically
located in areas where external pathogens enter the
body. Immune cells that reside in mucosal tissues
protect against the entry of infectious agents. The
immune responses arising in these regions must be
very selective so as to avoid mucosal damage that
would impair functions such as gas exchange (lungs).
The gastrointestinal system serves as a primary reser-
voir for bacteria that have the potential, if not prop-
erly controlled, to induce life-threatening infections.
A vast immune system exists in the gastrointestinal
tract with immune cells located in intraepithelial and
lamina propria regions of the gut and in specialized
lymph tissues, Peyer’s patches, lining the large and
small intestine. The main defense in the gut comes
from the large number of activated B-cells present in
the lamina propria region that secrete IgA.
Mediators of the Immune System
0006The response of immune cells to infectious agents is
mediated by a number of compounds. Cytokines are
glycoproteins that are secreted by immune and other
cell types and are a means of communication between
cells of the immune system and with other cells in the
body. The localized concentration of various cyto-
kines will determine what immune cells are activated.
T-helper cells type 1 cells (Th1 CD4þ cells) produce
interleukin (IL)-2 and interferon-g (IFN-g), which
generally promote a cell-mediated inflammatory re-
sponse. Th2-type CD4þ cells produce IL-4, IL-5, IL-
10, and IL-13, which support a humoral antibody
response. It has been hypothesized that the balance
of these cytokines offers a mechanism by which the
immune system can respond appropriately to a
specific type of infection.
0007Other important mediators of immune function
include epinephrine, glucagon, and cortisol, which
are released in response to stress and infection.
These hormones have been shown to have immuno-
suppressive effects on immune cells. Lipid-derived
factors such as eicosanoids, leukotrienes, and plate-
let-activating factor, made by a variety of cell types in
response to cytokines and other signals, also modu-
late immune function. When tissue is injured during
infection, the complement cascade is activated, and
fibronectin, vasoactive amines, and chemoattractants
are released. The complement cascade is important in
mediating inflammation and promoting phagocytosis
of microorganisms. Nitric oxide is a potent immuno-
biological compound produced by macrophages and
neutrophils to combat intracellular pathogens (i.e.,
parasitic fungi, protozoa, helminths, and mycobac-
teria) and viruses.
Fever
0008Fever is a host response that is characterized by an
elevation of core body temperature. The most
Cellular components
Phagocytes Natural killer
cells
Mucous
membranes
Skin
Physical barriers
Reticuloendothelial
system
NeutrophilsMacrophages
(activated
monocytes)
fig0001 Figure 1 Defenses of the innate immune system.
Cell-mediated
CD4
helper/inducer
T lymphocytes
CD8
cytotoxic/suppressor
T lymphocytes
Humoral
B-lymphocytes
(plasma cells)
Antibody production
(extracellular bacteria)
T helper type 1 T helper type 2
Delayed type hypersensitivity
response
(intracellular bacteria)
fig0002 Figure 2 Defenses of the acquired immune system.
3308 INFECTION, FEVER, AND NUTRITION

frequent cause of fever in acutely ill patients is infec-
tion (by bacteria, viruses, and/or their toxins). In most
cases, fever is initiated by the production of cytokines
(IL-1, IL-6, tumor necrosis factor (TNF)-a) from
macrophages and neutrophils. In general, it is be-
lieved that proinflammatory cytokines stimulate the
production of arachidonic acid metabolites (PGE
2
and thromboxane A
2
), which affect the temperature-
regulating areas in the brain (hypothalamus, me-
dulla). Subsequently, the brain signals mechanisms
that generate heat and reduce heat loss, thus increas-
ing core body temperature.
0009 It is widely accepted that fever has three distinct
phases. The first is known as the chill phase where the
individual experiences shivering and feeling cold. The
second phase is a plateau phase when the thermo-
static set point and body temperature are at the
same level. This is followed by a third phase known
as ‘defervescence’ when the fever ‘breaks,’ resulting in
flushing and sweating. This increase in body tempera-
ture is important as it increases the speed at which
neutrophils move and secrete antibacterial sub-
stances, increases B-cell and T-cell replication, and
results in a higher production of IFN-g (antiviral
and antibacterial properties). High fever, however, is
clearly maladaptive to the host resulting in loss of
appetite, increased sleepiness, muscle aches, and
hypermetabolism. Resting energy expenditure rises
by as much as 10–15% for each degree Celsius
increase in body temperature.
Interaction Between Nutrition, Infection
and the Immune System
0010 In children and adults with marginal or poor nutri-
tional status, episodes of infectious diseases are more
severe and result in more complications. Almost any
nutrient deficiency, if sufficiently severe, will impair
resistance to infection. The impact of infection on
nutritional status depends on the previous nutritional
health of the individual, the nature and duration of
the infection, and the diet consumed during the
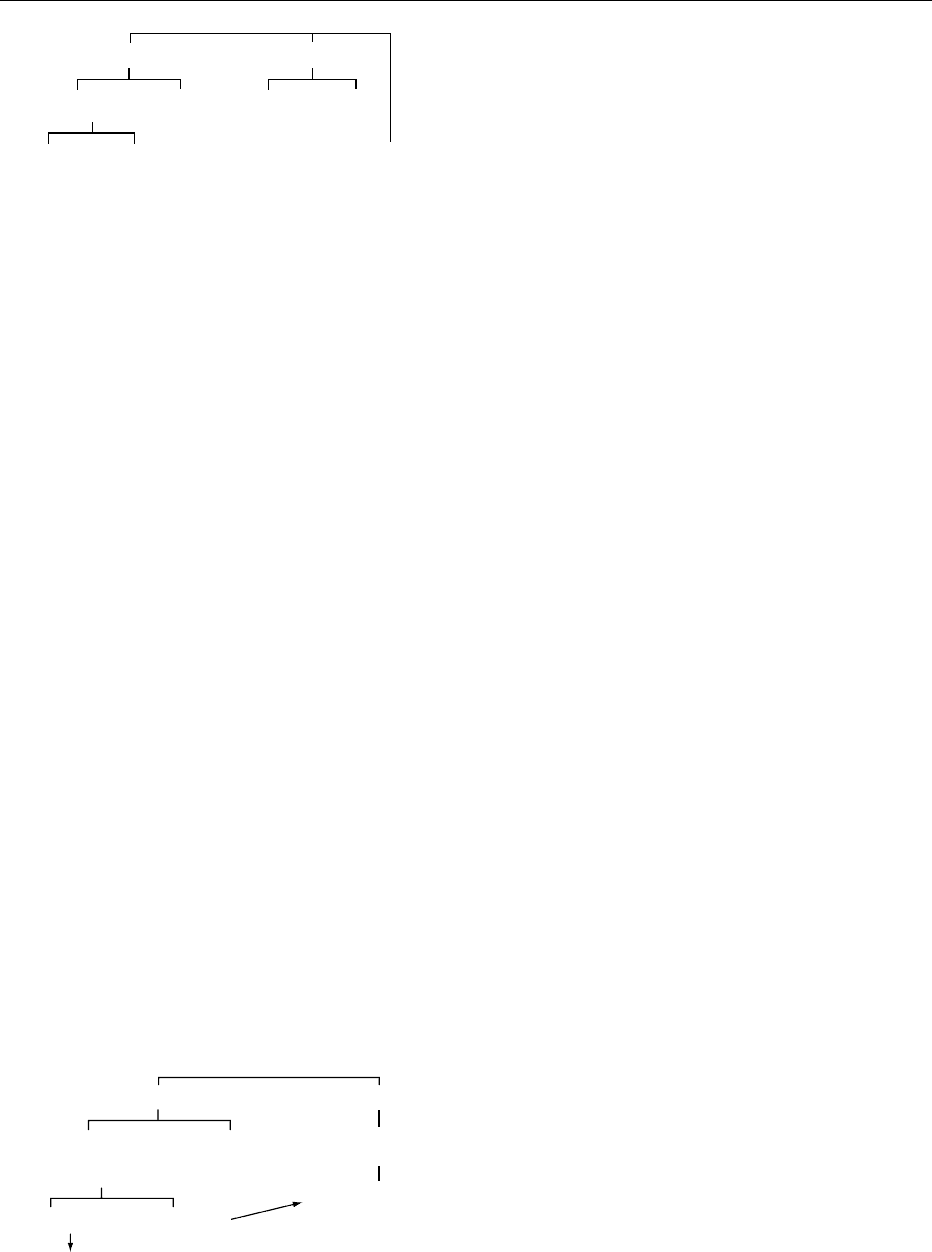
recovery period. Thus, infections themselves promote
malnutrition (appetite loss and anorexia, malabsorp-
tion, and elevated metabolism of energy, and other
nutrients), creating a complex cycle of immunosup-
pression and worsened nutritional status. Worsened
nutritional status will then further suppress immunity
and predispose the individual to opportunistic infec-
tions (Figure 3).
0011The interaction between nutrition and infection is
complex. The physiological mechanisms responsible
for metabolic changes during infection are not
completely understood, although cytokines are clearly
involved. Some degree of appetite loss (anorexia) is
present during most infections. In some cases, this
anorexia is due to nausea and vomiting; in others,
gastrointestinal lesions. Additionally, the presence of
a fever can result in appetite loss (anorexia) resulting
in a 10–40% decrease in dietary intake, not only of
protein and energy but also of most nutrients. Anor-
exia will precipitate clinical nutrient deficiencies of
any nutrient in which body stores are limited. The
extent of the depletion of nutrient status will subse-
quently increase the risk of damage to the host’s
tissues from the inflammatory response. To sustain a
hypermetabolic rate (i.e., in fever), there is an acute
mobilization of endogenous energy stores (glucose
and fat). However, during infections, there is also an
impaired ability to use these substrates. If body stores
are used to provide for the metabolic needs of infec-
tion and fever, weight loss occurs. In fact, this sort of
observation led to the introduction of the lay-term
‘consumption’ to describe tuberculosis, the classic
chronic wasting infectious disease. The high preva-
lence of infections among children living in poor areas
of developing countries results in impaired linear
growth. In addition, the acute phase response (e.g.,
proinflamatory cytokine release) to fever directly
affects bone remodeling that is required for long
bone growth.
Nutrition and the Immune System
0012The past 25 years have resulted in an explosion of
scientific literature defining the role of specific nutri-
ents on immunity. Most host defenses are breached
in protein-energy malnutrition, particularly cell-
mediated immunity. It is now generally accepted
that nutrition is an important determinant of the
immune response. It appears that almost every
known nutrient deficiency can affect disease resist-
ance if it is sufficiently severe, and this may also be
true for many nutrients consumed in excess. Nutri-
tional state and specific nutrients may impact on the
immune system directly (e.g., triggering immune cell
activation, or altering immune cell interactions) or
INFECTION
Immune
suppression
IMPAIRED IMMUNITY
MALNUTRITION
Barrier function
Cell mediated immunity
Fever
anorexia
metabolism
fig0003 Figure 3 Relationship between malnutrition, immunity, and
infection.
INFECTION, FEVER, AND NUTRITION 3309