Marshall L. Stoller, Maxwell V. Meng-Urinary Stone Disease
Подождите немного. Документ загружается.


10 Master, Meng, and Stoller
Several remedies for bladder calculi from folk medicine are described in the Talmud
(Gittin, folio 69b). One example illustrating the lack of understanding of pathophysiol-
ogy was to “take a louse from a man and a woman and hang it on the penis of a man and
the corresponding place in a woman; and when he urinates he should do so on dry thorns
near the socket of the door” (12). Surprisingly, this “remedy” remained in the medical
armamentarium through the Middle Ages. The extreme suffering generated by stone
disease and the importance of stone prevention is evidenced by finding recipes against
kidney stones in the Croatian prayerbook (13).
The use of surgical instrumentation in the treatment of urinary stone disease has a
checkered history, with admonitions against surgery from the start. The great Hippocrates
(460–370 BC), who was familiar with the pathology related to urinary tract stones,
included a passage regarding their treatment in the original Hippocratic Oath:
“I will not cut persons laboring under the stone, but will leave this work to be done by
men who are practitioners of this work.” (Adams translation) (14).
Of course, this statement can be interpreted two ways. Either the removal of stones
was considered too lowly a craft for physicians, or conversely lithotomists must have
possessed a fair degree of skill, or Hippocrates would not have recommended that only
practitioners of the craft perform the delicate surgery.
Lower Urinary Tract
URETHRAL
Possibly the earliest instrument for the treatment of stone disease could be thought of
as the urethral catheter. The purpose of the catheter was to bypass obstruction thus
permitting drainage. The word catheter is derived from the Greek cathienal, “to send
down,” although some ascribe it incorrectly to cathatos, which means perpendicular
(15). Initially, in an effort to bypass the obstruction resulting from the calculus in the
urethra or at the bladder neck, ancient Egyptians first used hollow reeds and curled-up
palm leaves, but later history records Egyptians using bronze and tin for making cath-
eters, knives, and sounds as early as 3000
BC. The ancient Hindus used tubes of gold, iron,
and wood for dilating the urethra at least before 1000
BC (16). The Chinese used a
lacquer-coated tubular leaf of the onion plant Allium fistulosum to make catheters as
early as 100
BC (17). Metal catheters and sounds made of bronze were found in the ruins
of Pompeii, which was buried in 79
AD (18). Although the catheters found at Pompeii
were doubly curved, all other ancient catheters and sounds had one common character-
istic: they were made straight and rigid without consideration for anatomic structure of
the posterior urethra. Surprisingly, the logical idea of making catheters curved was not
rediscovered until literally hundreds of years later. During the 10th century, Islamic
surgeons used rigid silver catheters and also catheters made of skins. Avicenna (980–
1030
AD) used sea animal skins stuck together with cheese glue and also recommended
lubricating the urethra with soft cheese before rigid catheterization. Many others tried
different materials that were both simultaneously stiff and malleable including silver,
copper, brass, ivory, pewter, and lead. Lack of the ability to create an indwelling catheter
was a continuing problem with all of these designs but nevertheless provided relief to
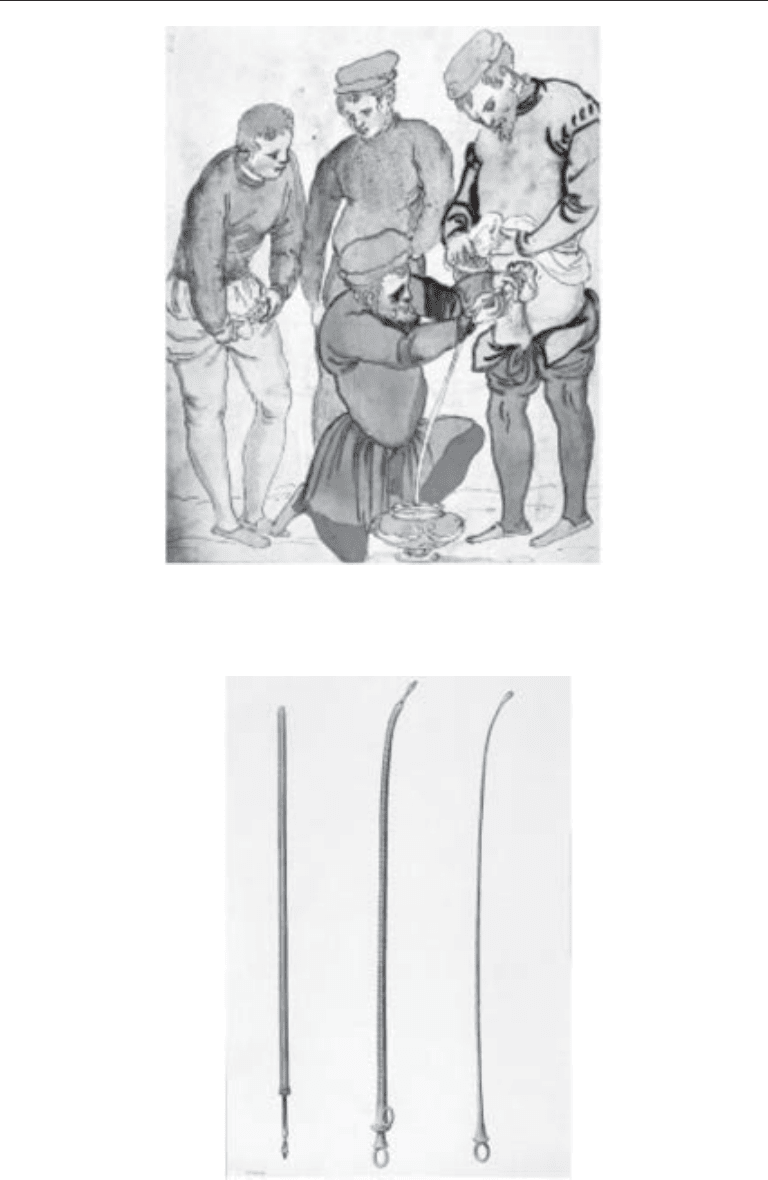
patients (Fig. 2). In the early part of the 18th century, a German anatomist, Lorenz
Heister (1683–1758), had catheters made of silver in the shape of the natural curve of the
prostatic urethra (Fig. 3). The true development of the modern catheter is felt to come
from Heister’s design and was perfected in the form of the “coude” (French, meaning
Chapter 1 / Stone Nomenclature and History 11
Fig. 3. Silver catheters showing evolution in design with the two on the right being bent to
simulate the natural curve of the prostatic urethra.
Fig. 2. Sixteenth century itinerant barber-surgeons catheterized grateful patients to relieve ob-
struction caused by bladder stones, as illustrated in a Italian medical picture book by Henricus
Kullmaurer and Albert Meher.

12 Master, Meng, and Stoller
elbow [noun], or bent [adjective]) catheter by the eminent French surgeon Louis Mercier
(1811–1882), although the literature still contains spurious assertions that a certain
Emile Coude was responsible (19).
The first flexible catheters were made of wax-impregnated cloth and molded on a
silver sound created by Frabricius, professor of surgery in Padua, in 1665. These cath-
eters were not very durable and softened rapidly, thus losing the ability to maintain a
patent lumen. Modern flexible catheters, basic prototypes of the ones used today, were
first made with the introduction of elastic gum, derived from the latex sap of the Hevea
tree species in 1735 (20). These were far more comfortable than the rigid catheters, but
still suffered from problems of extreme stickiness in hot weather and brittle stiffening
in cold weather. The ability to transform this elastic gum into a durable and versatile
substance that did not have temperature dependence was discovered by Charles
Goodyear in 1839, who termed this process vulcanization. After methods were devel-
oped for stabilizing the natural latex and preventing it from coagulating, rubber prod-
ucts could be made over a mold dipped into a vat of latex. This rubber catheter was
relatively durable, flexible, and therefore easily introduced and comfortably retained.
Its introduction marked the true beginning of the modern urinary catheter. This catheter
still required external appliances to hold it in place, such as taping it to the penile shaft
or suturing to the labia in women. In 1822, Ducamp used submucosal layers of ox
intestines, which were tied on to the catheters as inflatable balloons to hold a catheter
in place. In 1853 Reybard devised a catheter that incorporated a separate balloon chan-
nel. A growing surge of transurethral surgery led to the need to secure hemostasis and
finally resulted in F. E. B. Foley, an American urologist, devising the modern balloon
catheter in the 1930, which was distributed by Bard in 1933 (21). Modern 20th-century
developments in catheters have centered mostly on the use of different materials, like
silicone, to reduce urethral toxicity from latex.
A Parisian instrument maker, Joseph Frederick Benoit Charriere (1803–1876), devised
a sizing system for urologic instruments commonly called the French scale in the United
States, which is based on progressive diameter sizes differing from each other by one-
third of a millimeter, i.e., 1 mm = 3 French (Fr) or 0.039 inches (22).
It was known for millennia that merely pulling out stones lodged in the penile urethra
could result in irreversible urethral injury. In fact, Celsus himself, devotes a large section
of his book, De Medicina, to the removal of urethral calculi. He describes first using a
scoop, but failing that, urethrolithotomy was performed with a sharp knife. The urethra
and skin edges were left open to heal by secondary intention. An ingenious prevention
of fistula formation was to stretch the penile shaft skin distally and push the glans
proximally so that after the incision to remove the stone, the relaxed skin would result
in nonoverlapping urethral and skin openings (23).
B
LADDER
Perineal Lithotomy
The operation for bladder stone is one of the oldest recorded surgical techniques
apart from trepanning and circumcision (20). Patients were understandably reluctant to
undergo surgery, given the absence of anesthesia and the very high procedure-related
mortality, as described in the following paragraphs. Only severe, prolonged, insuffer-
able pain related to the stone made patients submit to the acute pain of the knife. The
literature is replete with descriptions of special instruments, knives, lancets, and gorgets
with unique blades for opening the bladder through the prostatic urethra. Medial litho-
Chapter 1 / Stone Nomenclature and History 13
tomy (cutting on the gripe) is the oldest variety of the perineal operation, but even
Celsus, in approx 50
AD, recognizing the great danger of rectal injury, deflected the
inferior end of the perineal incision toward the left ischial tuberosity before incising the
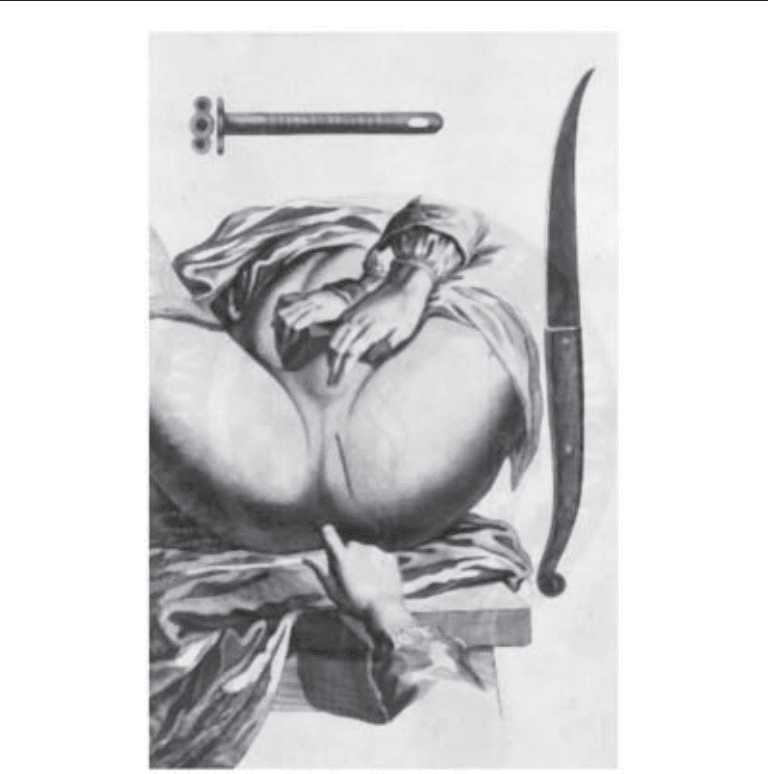
bladder. In perineal lithotomy of the “small apparatus” a staff or sound was passed
through the urethra into the bladder (Fig. 4). This sounding was the method employed
to confirm the presence and location of vesical stone. With the patient in a semisitting
posture, the tip of the sound was maneuvered to bring the stone down to the lowest point
in the bladder. When the perineal incision was made the surgeon felt for the groove on
the convex side of the staff as a guide for the incision into the membranous urethra and
prostate. When an assistant held the urethral staff, the surgeon could cut directly onto
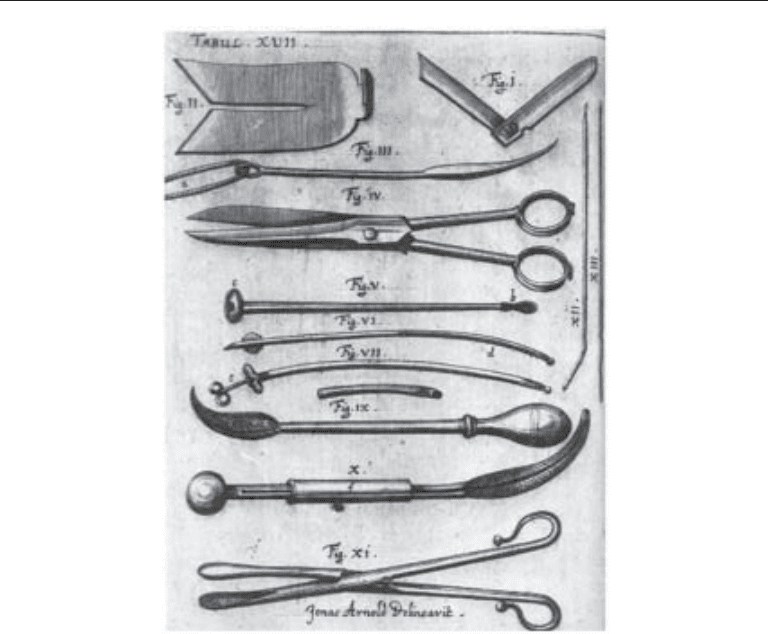
the stone. Perineal lithotomy using the “grand apparatus” of Mariano Santo came next
in 1535 (Fig. 5). Instruments, forceps, and scoops, rather than the finger, were inserted
Fig. 4. Lithotomy using instruments of the “lesser” apparatus. Note the lateral incision for
lithotomy. Note the sharp bistoury on the right and the cannula at top, which were designed by
M. Fourbert in the 18th century.
14 Master, Meng, and Stoller
through the perineal incision to engage and extricate the stone. In the main, it can be said
that the additional apparatus not only complicated the procedure but added to the
operative risk (24). The sole objective of lithotomy was to relieve the patient of stran-
gury by extracting the stone as quickly as possible through a perineal incision. Opera-
tions were frequently performed in the home. The patient was purged and often bled
before as well as after operation. Bleeding immediately beforehand had the advantage
of producing shock and considerable diminution in sensitivity to pain. As many as five
or more cases were often scheduled for one session. Pouteau, the great 18th-century
French surgeon, described the scenes as an “auto-da-fe affair” (act-of-faith affair). The
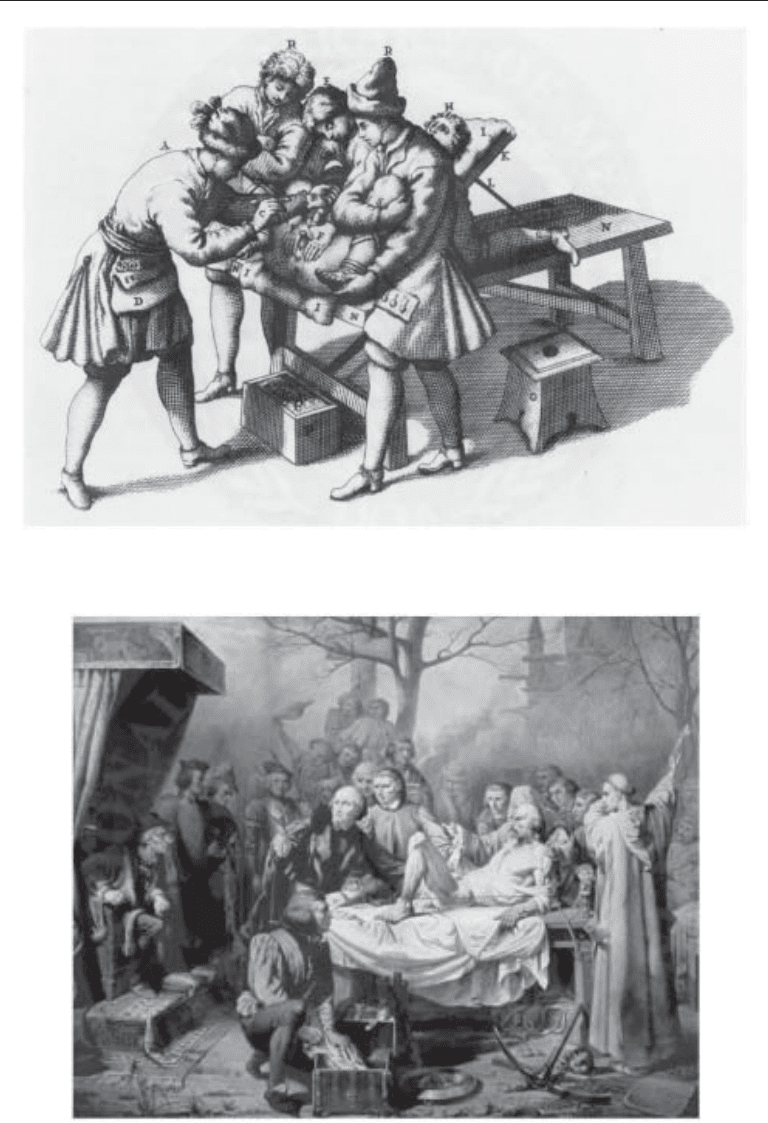
courage and agony of the patient on the lithotomy table, known as the scaffold or Bed
of Misery (Fig. 6), and the boldness and skill of the surgeon were the magnetic attrac-
tions that drew onlookers, both rich and poor (Fig. 7). After the terror and pain of the
operation, the patient usually had a sense of relief as urine escaped through the litho-
tomy wound without initiating attacks of vesical colic. Perineal lithotomy provided the
surgeon a fine opportunity to indulge in showmanship. Sir Astley Cooper often did the
operation in less than a minute and the average maximum time in a surgical editorial in
1828 was about 6 min (24).
Fig. 5. Elements of the “major” apparatus used for lithotomy in the 17th century. Note the
multiplicity of knives, spatulas, and hooks used for cystolithotomy in the later period compared
with that in Figure 4, which just used a knife and a cannula.
Chapter 1 / Stone Nomenclature and History 15
Fig. 7. Lithograph titled, “The earliest operation for the stone,” by Rivoulon. The patient is lying
on a platform and the physician is performing an operation before a large crowd, which includes
King Louis XI of France, seen seated on the left, intently watching the showmanship. This
fanciful lithograph has little relation to the pain the patient suffered during the stone removal.
Fig. 6. Lithotomist at work, ca. 1700. Two assistants are holding the legs in lithotomy position,
while a third pushes on the suprapubic region to keep the stone fixed in place at the bladder neck.

16 Master, Meng, and Stoller
From the mid-16th century well into the 18th, a brand of self-made stone cutters,
“specialists” who acquired art through apprenticeship, were the chief lithotomists.
Without formal training, they usually practiced poor operative technique and some were
charlatans (25). Mortality was high, approx 18 to 53%. Extravasation of infected urine
into the paravesical tissues was often the reason for death, rather than hemorrhage. Those
who cut too widely were known to lacerate the internal pudendal artery, often resulting
in exsanguination. Interestingly, there were a few outliers, most spectacularly, Pouteau,
a notable French surgeon of the 18th century, whose mortality rate was only 2.5%. This
was achieved a century before the development of antisepsis by his strict adherence to
the importance of keeping hands clean and the use of disposable paper dressings.
Strangely, published accounts of mortality even during the antiseptic era were almost as
high as the nonantiseptic era, in the range of 10% (24). One hypothesis is that the open
wound management after vesical incision essentially allowed for irrigation of the wound
by urine. It is interesting that the morbidity and mortality associated with this operation
was so high that some of the first informed-consent documents were associated with
lithotomy (26). The first suprapubic lithotomy for removal of a bladder stone was carried
out in 1561 by Franco, who performed removal of an egg-sized stone in a 2-yr-old boy,
but did not achieve acceptance as a safe modality at the time, likely because of the
frequent risk of peritoneal injury and septic death (27).
Celsus, Franco, and Cheselden stand out in their periods as the greatest contributors
to the development of lithotomy. The first truly sterile operation for stone was Joseph
Lister’s median lithotomy for vesical calculus on June 4, 1881. He swabbed the wound
with zinc chloride and left it open, but provided a drainage tube to facilitate the escape
of urine. The patient recovered quickly.
Urinary incontinence, occasionally reported after perineal lithotomy in the male, was
so frequent following urethrovesical lithotomy in the female that the procedure came to
be abandoned. Urethral dilatation was substituted because of the distensibility and short-
ness of the female urethra.
Lithotrity/Lithoprisy
The dangers and difficulties of lithotomy were an important spur that drove the devel-
opment of alternative minimally invasive methods of bladder stone extraction.
Ammonius, in 247
BC, is credited with fragmentation of bladder stones by impaling them
with an ice pick-like device passed through a catheter (11). After engaging the stone, a
hammer was used on the pick to fragment the stone. This idea was apparently unpopular
and there is no mention of stone fragmentation for several centuries. Some lithotomists,
such as Elderton in 1819, unsuccessfully tried to fix stones in place by loops of wire
passed through a straight catheter. When the stone was engaged a drill bow was used to
break up the stone (11). Interestingly, some famous self-performed operations for uri-
nary stones did involve lithotrity-type maneuvers, such as that of Colonel Martin of
Lucknow, a layman who in 1782 ingeniously devised instrumentation to file his stone
to small pieces, which he was then able to void (28). The first truly effective drilling
instrument was made by Civale of France and used in 1824. This instrument, known as
a trilabe or lithontripteur, consisted of two straight metal tubes, one inside the other; the
inner had three curved arms that projected when the outer sheath was retracted and by
which the stone was seized. It was held in position by advancing the outer sheath. An iron
rod with a sharp point was passed through the inner tube to bore a hole into the stone This
was uncomfortable for the patient and treatment sessions were limited to 5 min with
Chapter 1 / Stone Nomenclature and History 17
several sessions required to break the stone into small enough fragments that the patient
could void (29). With this minimally invasive approach, mortality was reduced to a mere
3%. Ambroïse Paré put teeth in the blades of his crushing forceps and a thumbscrew in
the handle so as to increase the power of the instrument to crush large stones, but this also
increased mortality. The introduction of ether anesthesia in 1842 allowed surgeons to
perform longer and more precise operations. Bigelow in 1878 added to the development
of this procedure by the use of suction irrigation and renamed the lithotrity procedure
litholapaxy. The use of anesthesia coupled with suction enabled complete removal of the
stone in a single session, which could last 2 h. However, without the ability to visualize
the stone, this technique was not popularized until cystoscopy was developed, where-
upon the lithotrite was combined with a cystoscope into a single instrument.
Cystoscopy
The desire to look into the cavities of the body to diagnose and treat disease occupied
many medical specialists throughout the 18th century, especially as the alternative was
extensive surgery, not yet possible without the development of anesthesia. The first
instruments designed for urologic evaluation were designed for the female, because of
the shorter length and greater diameter of the urethra. Initially various specula were
developed to inspect the female urethra, mostly by dilating it, but they were painful when
widely opened and provided only a limited viewing ability (30). The biggest hindrance
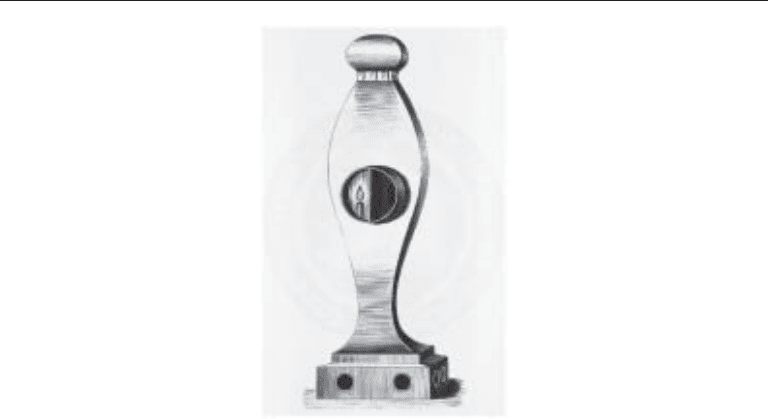
to viewing ability was insufficient illumination. To solve this problem, in 1805 Phillip
Bozzini, from Germany, developed the “lichtleiter,” or light conductor (31). This instru-
ment, made of silver and covered in sharkskin, contained a tallow candle balanced on a
spring to keep the position of the flame constant (Fig. 8). The observer applied his eye
to the body of the instrument and was able to see past the mirror down a series of fittings,
or specula: a narrow tube for the urethra, a bigger one for the rectum, a four-valved one
Fig. 8. The “lichtleiter” or light conductor of Bozzini. One can see the candle used for illumina-
tion immediately next to the eyepiece for viewing.
18 Master, Meng, and Stoller
for the vagina, and a fitting with a mirror on the end for laryngoscopy. Bozzini, an
obstetrician, wanted to use endoscopy for operating on the uterus and to remove foreign
bodies and stones from the bladder (32). The lichtleiter was successfully tested in Vienna,
but it was also clear that candlelight did not have enough illumination to view the
bladder. Moreover, because of local medical politics, further development was blocked.
The lichtleiter certainly accomplished one goal—it spurred the development of endos-
copy by other physicians. Although many other physicians worked on developing endo-
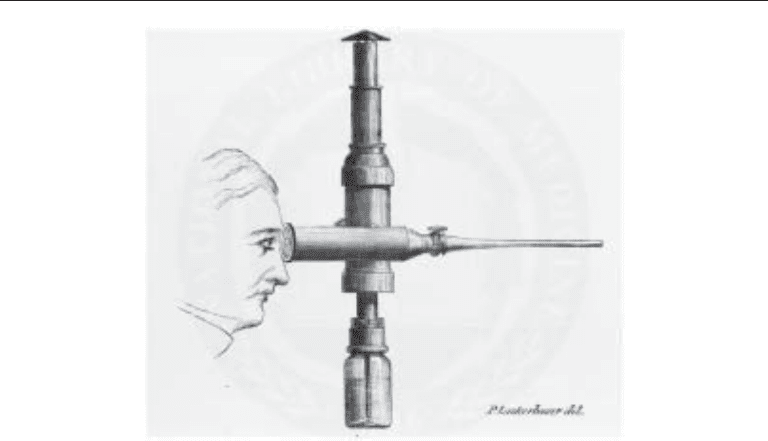
scopic instrumentation, the next leap forward was by Desormeaux, who in 1853
introduced his “l’endoscope” (Fig. 9). This instrument had the advantage of a stronger
light source (initially a paraffin or kerosene lamp), the use of a mirror as a light reflector,
and the ability to introduce working instruments. He was able to make sketches of the
bladder and bladder calculi using this device. Additionally, he diagnosed and treated
urethritis, carried out direct vision internal urethrotomy, and even removed a papilloma
from the urethra. One major problem with this device was the constant fear of burning
the surgeon’s face or the patient’s legs. Francis Cruise of Dublin, a friend of Desormeaux,
encased the instrument in a mahogany box, which allowed for safety from heat but made
it even more unwieldy. The second problem was that illumination still could not reliably
provide for inspection of the entire bladder. Nevertheless, this research spurred others
to develop analogous instruments such that in 1861, Joseph Grunfeld, a dermatologist,
was able to remove a bladder papilloma.
Investigators focused their attention on changing the light source from an external
source to an internal source, which would prove pivotal to the advancement of endos-
copy. In 1867, Julius Bruck, a dentist from Dresden used an electrically heated platinum
loop, inserted into the rectum, to transilluminate the bladder, although Gustave Trouve
of Paris is also credited with this work. Cooling of the loop was a problem, resulting in
rectal burns.
Fig. 9. “L’endoscope” of Desormeaux devised in 1865.
Chapter 1 / Stone Nomenclature and History 19
Finally, in 1877 the potential of Bruck’s theoretical advance was realized, and, in
combination with other advances, essentially established the form of a clinically useful
cystoscope as it is used today. The 28-yr-old urologist responsible for this synthesis was
Maximilian Nitze of Berlin. Nearly 90 yr had passed since Bozzini first described his
lichtleiter. Nitze, working with a mechanic and an optician, devised an instrument with
a platinum wire light source at the tip that also had a glass optic system similar to that
of a microscope, allowing for a larger, magnified view of the bladder. This instrument
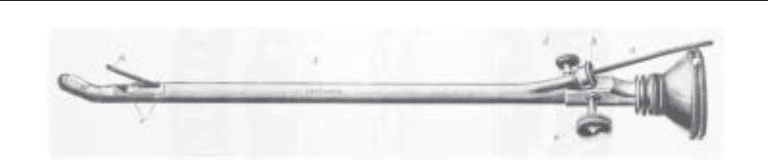
still produced a good deal of heat and required water cooling. However, once Edison
invented the incandescent electric bulb in 1880, Nitze, as well as Joseph Leiter, produced
the first practical cystoscope in the late 1880s, which was an affordable instrument
(Fig. 10). Additional major design changes took place in the early 1900s and included
the use of water instead of air to distend the bladder and the use of hemispherical lenses
to increase the viewing area (33). The development of fiberoptic instrumentation and the
use of the Hopkins “rod-lens” in the 1950s enabled the clarity of endoscopic images that
we see today. Reviewing this remarkable story, one notes the consistent theme running
through this development, the integration of advancements in physics and optics by
surgeons themselves to make better instruments.
In terms of specific use of instrumentation for stone disease, Kelly published the use
of endoscopy to remove a ureteral calculus, albeit small, in 1895. Kolischer later used
a primitive endoscope and ureteral catheter to inject sterile oil below a stone in order to
facilitate stone passage (32).
The history of flexible urological instrumentation is a recent one. Basil Hirschowitz,
a South African gastroenterologist, again in collaboration with the physicist Hopkins,
produced a flexible fiberoptic endoscope, which enabled him to perform endoscopy in
1957 on a dental student’s wife who was suffering from a duodenal ulcer (34). Interest-
ingly and fortuitously for urologists, American Cystoscope Makers Inc. (ACMI) was the
only company interested in commercializing this instrument. The first reported use of
flexible instrumentation in the urinary tract was actually ureteroscopy and is detailed
later (35).
L
ITHOTRIPTICS
With the severe complications of sepsis, hemorrhage, rectal injury, and death from
surgery, many patients turned to various substances said to be capable of dissolving
stones in vivo. These drugs, taken orally or injected into the bladder with special devices
(Fig. 11), were called lithotriptics, literally “stone-breakers (36).” One of the most
famous, or rather infamous, was sold by Mrs. Joanna Stephens. This resourceful lady has
been reviled as perpetrating a fraud on England in 1739 by her claims of being able to
Fig. 10. Maximilian Nitze’s cystoscope, showing the probe channel, urethral probe, and bulb
illumination.