Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


747
CHAPTER
65
Miles Abdominoperineal
Resection with Total
Mesorectal Excision
Tien C. Ko
STEP 1: SURGICAL ANATOMY
◆ For the total mesorectal excision, please see the discussion on pelvic autonomic nerves in Chapter 64.
◆ The seminal vesicles, prostate, and urethra are located ventral to Denonvillier’s fascia cranially and
the superfi cial transverse perineal muscle caudally.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Miles abdominoperineal resection with total mesorectal excision is indicated for rectal cancer near
the levator ani muscle or persistent or recurrent squamous cell cancer of the anus after chemoradia-
tion treatment.
◆ Preoperative chemoradiation treatment is indicated for T3, T4 lesions or those tumors with enlarged
pelvic lymph nodes on pelvic computed tomography (CT) scan or endorectal ultrasound.
◆ Appropriate bowel preparation such as GOLYTELY or four bisacodyl (Dulcolax) tablets followed by
HalfLytely should be administered the day before surgery. Preoperatively, a single dose of broad-
spectrum antibiotic (such as ertapenem) is administered.
◆ The permanent colostomy site is marked by an enterostomal nurse preoperatively to ensure the best
placement of the colostomy.

748 Section IX • Colon
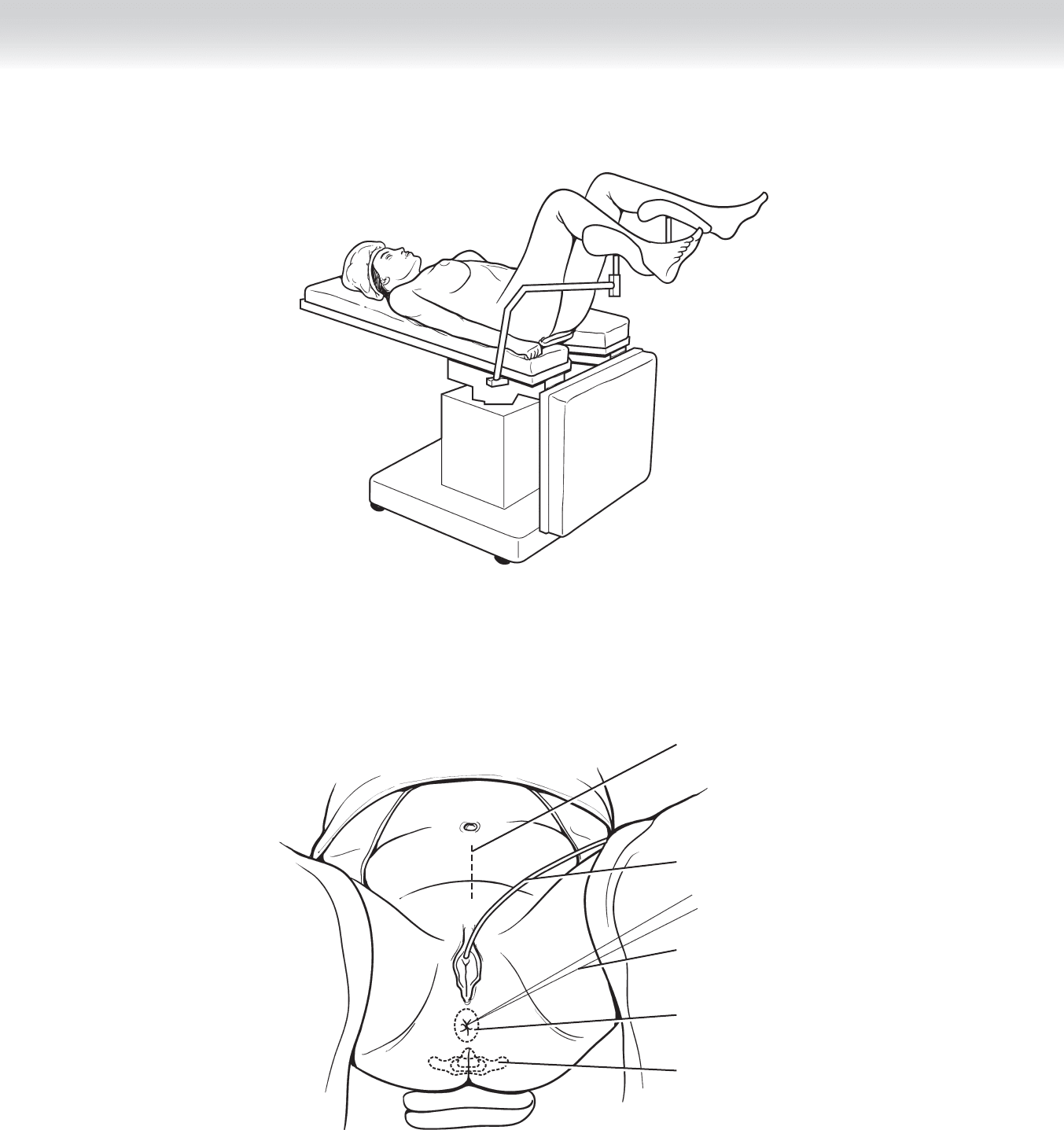
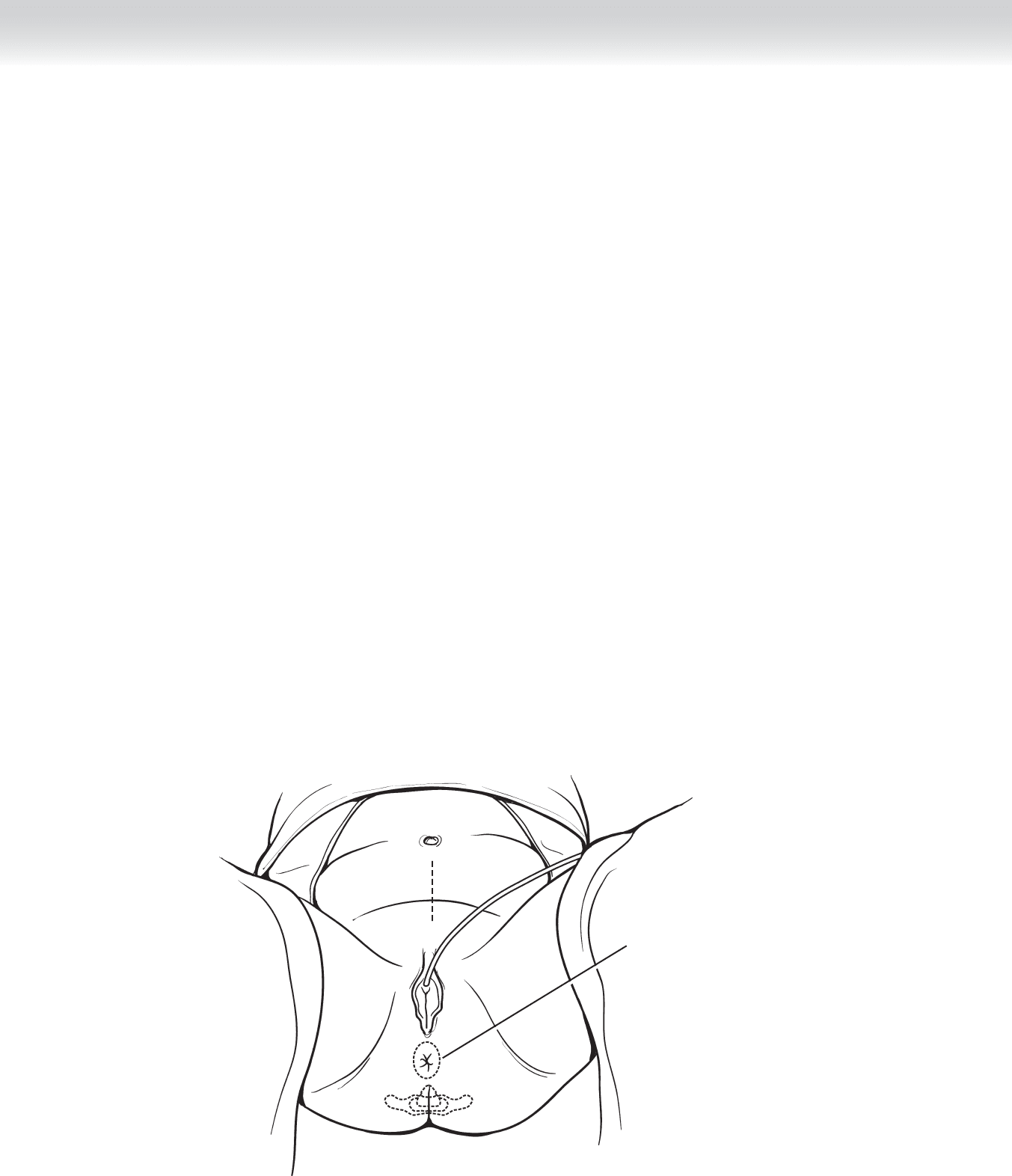
◆ After induction of general anesthesia, the patient is placed in a lithotomy position with the
legs in padded stirrups at 30-degree abduction. The coccyx is placed near the end of the
table and elevated with a stack of towels (Figure 65-1). A nasogastric tube is placed to pre-
vent gastric distention, and a urinary catheter is placed to decompress the bladder. The
rectum is irrigated with povidone-iodine (Betadine) solution until clear. The anus is closed
with a 0 silk purse-string suture (Figure 65-2).
STEP 3: OPERATIVE STEPS
1. INCISION
◆ A midline abdominal incision is made from the pubic symphysis to approximately 5 cm
cranial to the umbilicus.
◆ The midline fascia is divided with electrocautery. The peritoneum is elevated with tissue
forceps, and after ensuring that no bowel is entrapped by the graspers, the peritoneum is
incised sharply with a scalpel.
◆ For the perineal dissection, an elliptical incision is made 2 cm away from the closed anus
(see Figure 65-2).
CHAPTER 65 • Miles Abdominoperineal Resection with Total Mesorectal Excision 749
Patient lithotomy position
FIGURE 65 –1
Midline incision
Foley catheter
Purse-string suture
closing anus
Line of incision for
perianal dissection
Coccyx
FIGURE 65 –2
750 Section IX • Colon
2. DISSECTION
◆ Once the peritoneum has been entered, a systematic exploration is performed to search for
metastases in the peritoneal cavity, including the liver and the preaortic and iliac lymph
nodes.
◆ A fi xed retractor is placed to retract small bowel superiorly and laterally out of the operative
fi eld. Retraction of small bowel is aided by placing the patient in a Trendelenburg position.
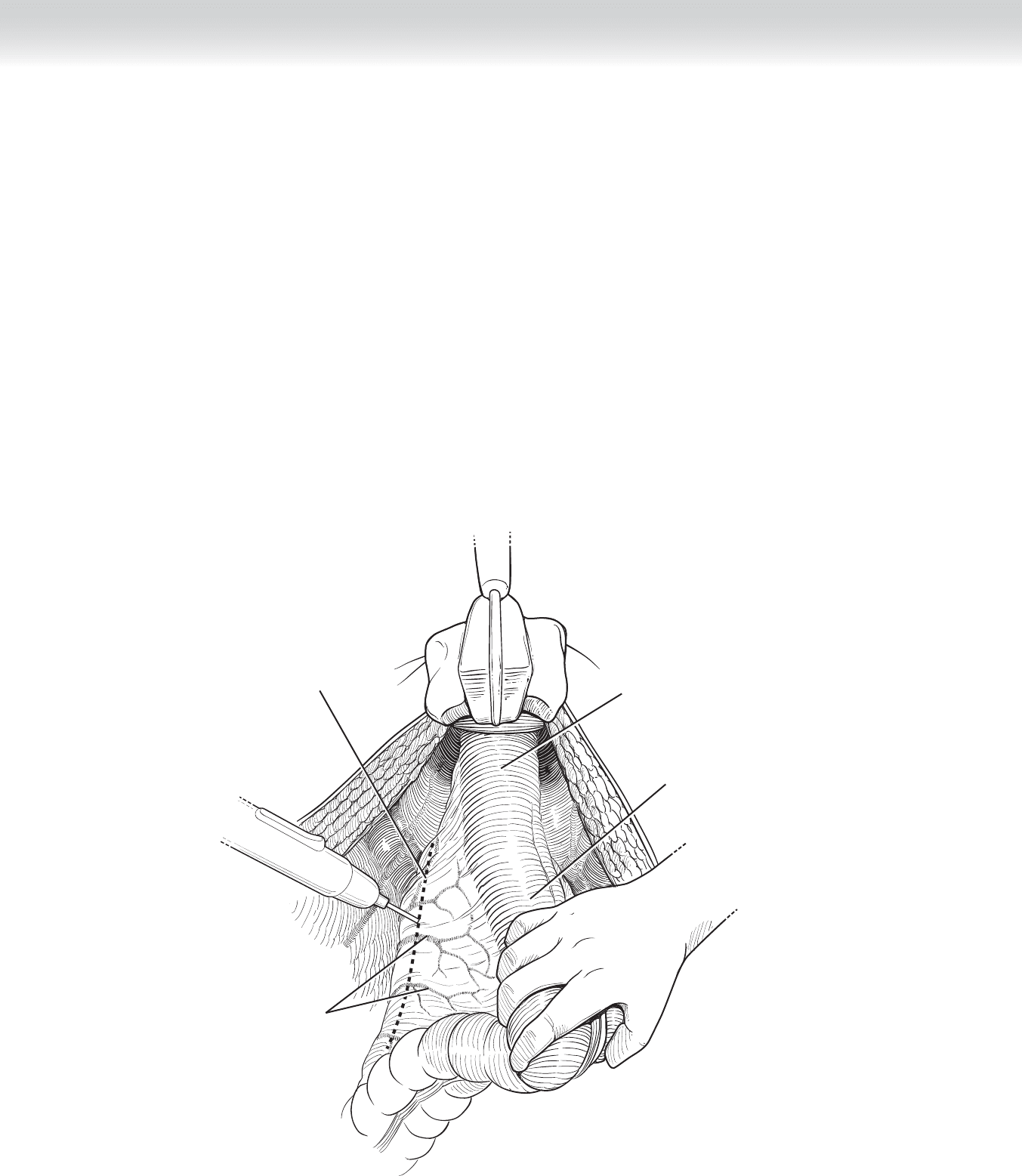
◆ Mobilization of the sigmoid colon is achieved by using electrocautery to incise the lateral
visceral fascia covering the mesosigmoid along the white line of Toldt, which can be easily
visualized by retracting the sigmoid colon medially (Figure 65-3). The left ureter is identi-
fi ed along its course over the left iliac vessels into the pelvis.
Line of transection
through peritoneum
and mesocolon
Inferior
mesenteric
vessles
Rectum
Sigmoid colon
FIGURE 65 –3
CHAPTER 65 • Miles Abdominoperineal Resection with Total Mesorectal Excision 751
Line of peritoneal incision
for abdominoperineal
resection
Iliac vessels
Ureter
Inferior mesenteric vein
Inferior mesenteric artery
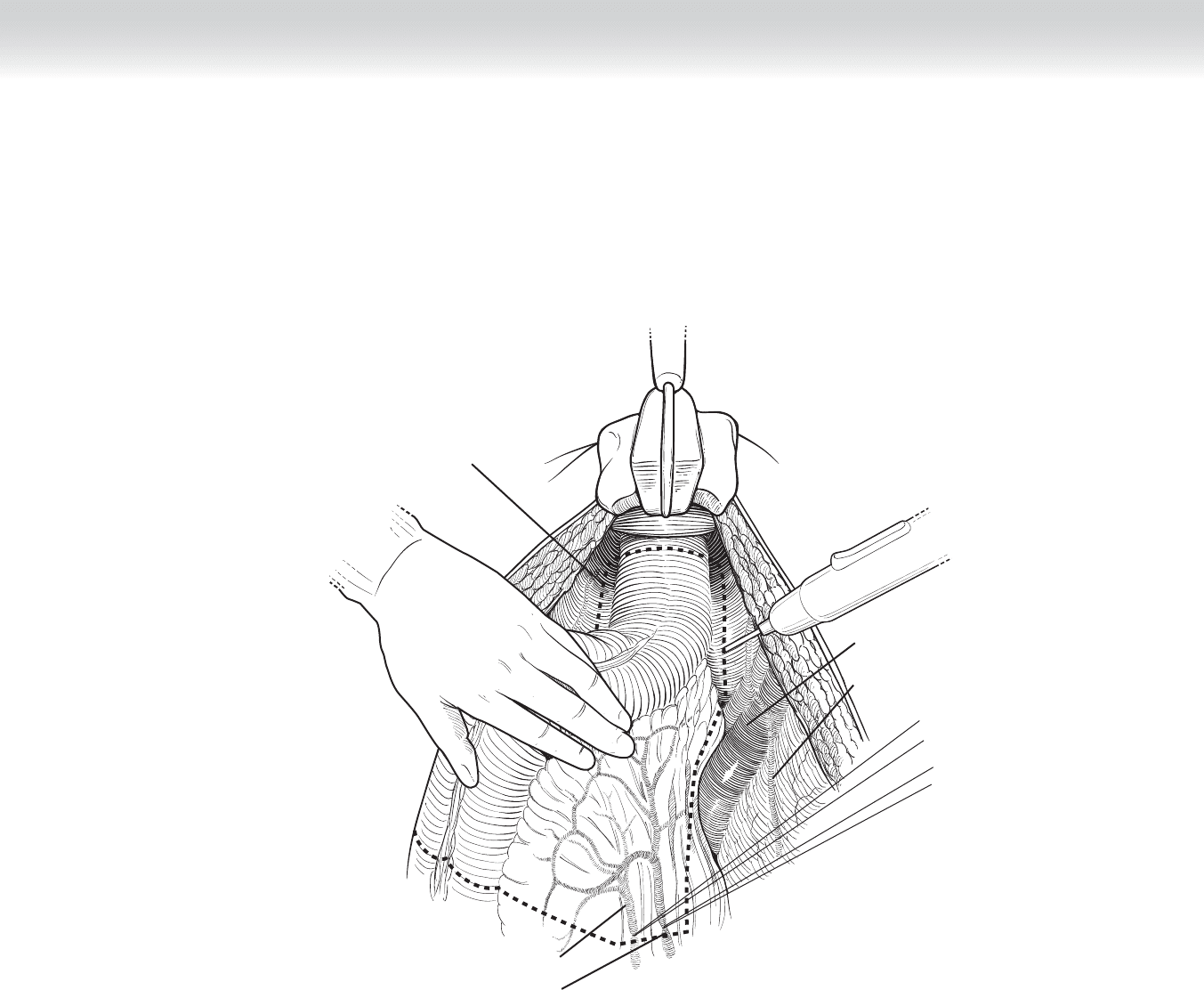
◆ The medial visceral fascia is incised with electrocautery, and the right ureter is visualized as
it courses over the right iliac vessels (Figure 65-4). The line of proximal resection is also
outlined but not carried out until the tumor is able to be fully mobilized.
FIGURE 65 –4
752 Section IX • Colon
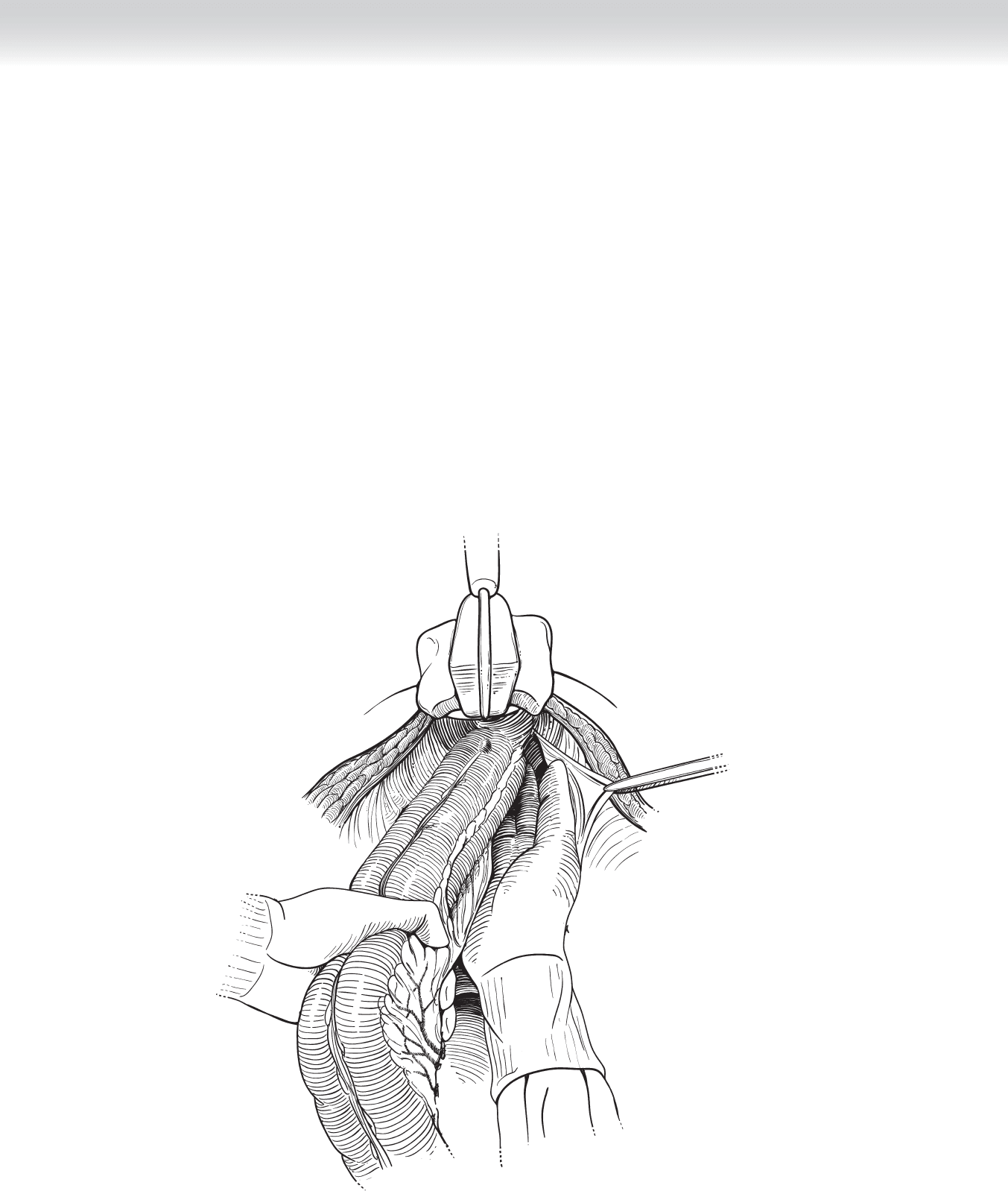
◆ The presacral space is entered by dividing the loose areolar tissue at the level of the sacral
promontory. The presacral space is developed sharply with electrocautery caudally toward
the levator ani muscle under direct vision. A fi ber-optic pelvic retractor is used for retraction
of the bladder and the rectum to facilitate visualization in the pelvis. Mobilization of the
rectum continues caudally to the levator ani muscle. After the sharp posterior pelvic dissec-
tion is completed, the distal extent of dissection can be manually evaluated (Figure 65-5).
Care must be taken to avoid injuring the presacral plexus of veins during the posterior
dissection.
FIGURE 65 –5
CHAPTER 65 • Miles Abdominoperineal Resection with Total Mesorectal Excision 753
◆ The mesorectum is mobilized laterally toward the right and left pelvic side wall, preserving the
hypogastric nerves on the sacrum. The lateral attachments to the pelvic wall containing the
mesorectum are divided either with clamps and sutures (Figure 65-6) or with a vessel-sealer
device, such as LigaSure.
◆ The rectum is mobilized ventrally by dividing the rectovaginal septum or the rectovesicle
space. In males, the dissection plane is ventral to Denonvillier’s fascia, preserving the
seminal vesicles.
◆ Attention is directed toward the resection of proximal sigmoid colon. First, the inferior
mesenteric artery is divided just distal to the origin of the left colic artery either with
clamps and sutures or with a vessel-sealer device. Next, the proximal sigmoid colon is
divided with a gastrointestinal anastomosis (GIA) stapler (Figure 65-7).
GIA stapler used for
transection of proximal
sigmoid colon
FIGURE 65 –7
Division of lateral
attachments
FIGURE 65 –6
754 Section IX • Colon
◆ A colostomy site is created in the left lower quadrant at either the premarked site or
halfway between the umbilicus and the left anterior superior iliac spine. A 2 cm in diameter
circle of skin is excised with a scalpel, and the subcutaneous tissue is divided with electro-
cautery. A cruciate incision is made in the anterior rectus abdominis fascia, and 2 cm of the
rectus abdominis muscle is divided with electrocautery. The peritoneum is incised with
electrocautery to complete the colostomy site, which should be approximately 2 fi nger-
breadths in diameter.
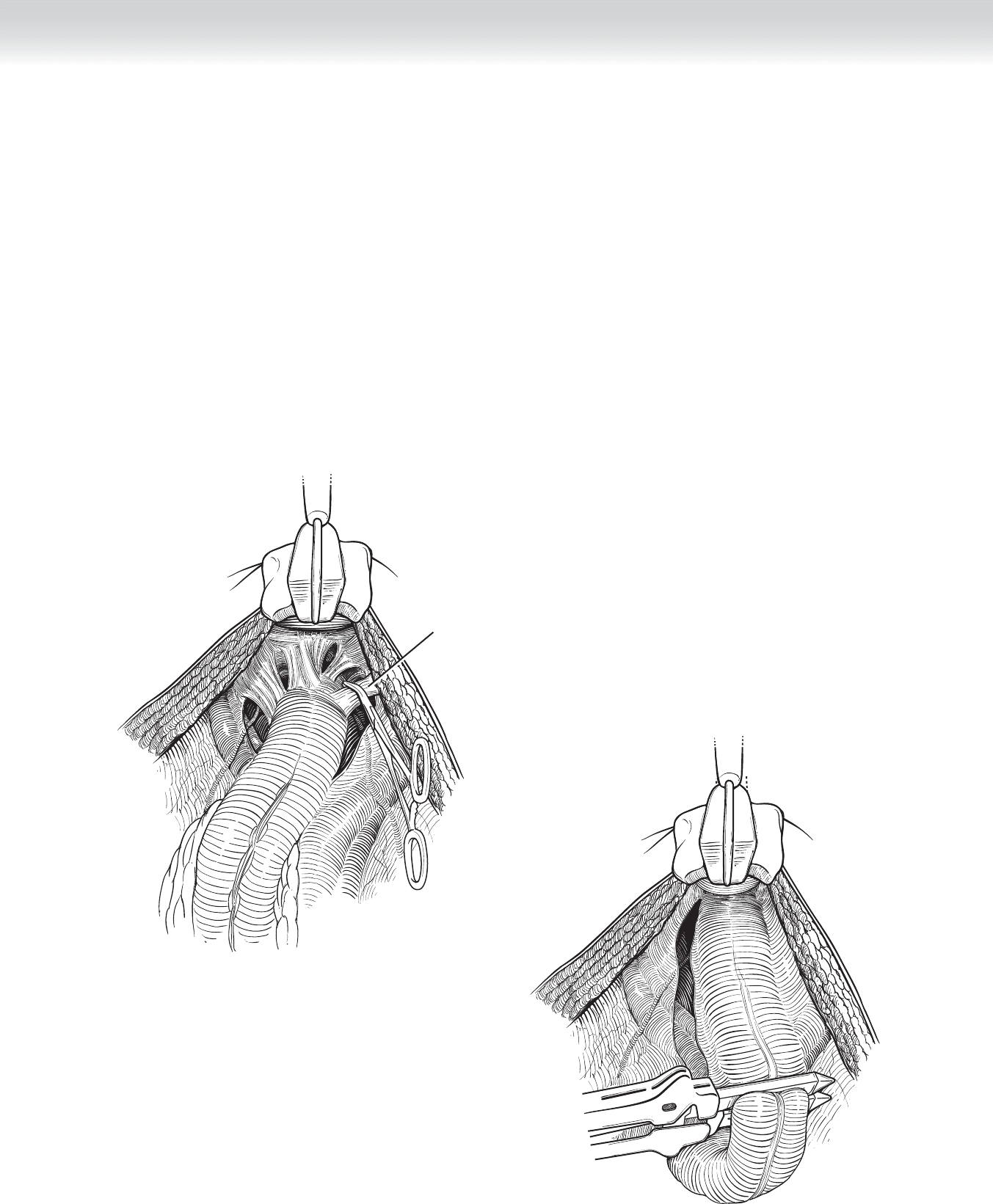
◆ The perineal dissection may be performed sequentially or simultaneously by a second team.
After skin incision, the laterally ischiorectal space is entered. The skin and subcutaneous
tissue is retracted with a self-retaining retractor to facilitate deep dissection (Figures 65-8
and 65-9). Inferior hemorrhoidal vessels are secured with sutures and divided. The coccyx
is identifi ed posteriorly, and the anococcygeal ligament located posteriorly is divided. Later-
ally, the levator ani muscle is divided with electrocautery and the perineal fossa is entered.
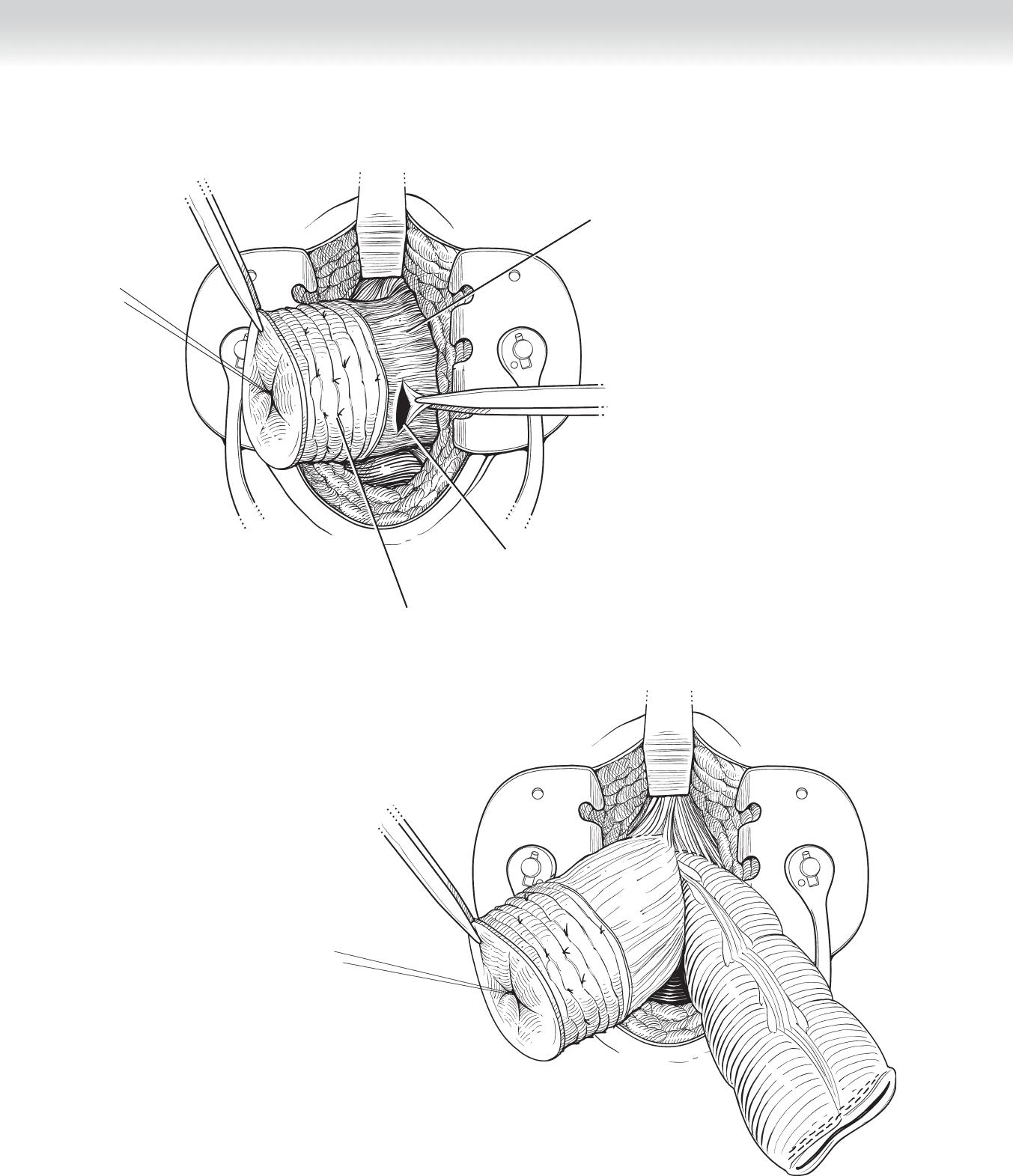
◆ The distal stump of the transected sigmoid colon and the proximal rectum is delivered cau-
dally through the opening of the levator ani muscle (Figure 65-10). Ventral mobilization of
the rectum is facilitated by the anterior retraction of the skin and subcutaneous tissue and
the posterior retraction of the sigmoid colon and rectum. The superfi cial transverse perineal
muscle is divided with electrocautery to completely mobilize the rectum. In males, the ure-
thra courses ventrally to the superfi cial transverse perineal muscle and can be identifi ed and
protected by palpating the urinary catheter. The sigmoid colon and rectum are removed
through the perineal wound.
Line of incision for
perianal dissection
FIGURE 65 –8
CHAPTER 65 • Miles Abdominoperineal Resection with Total Mesorectal Excision 755
Levator ani muscle
and vessels
Perineal fossa
Ligated hemorrhoidal
vessels
FIGURE 65 –9
Transected stump of sigmoid colon
and proximal rectum drawn through
opening in levator ani muscle and
peritoneum
FIGURE 65 –10

756 Section IX • Colon
3. CLOSING
◆ The pelvis is irrigated with saline, and hemostasis is obtained. Two Silastic 10-mm drains
are placed in the pelvis through stab incisions in the right and left gluteal regions, lateral to
the perineal wound, and secured with sutures of 2-0 nylon. The levator ani muscle is reap-
proximated with a running suture of 2-0 Vicryl (Figure 65-11).
◆ The subcutaneous tissue of the perineum is reapproximated with a running suture of
3-0 Vicryl. The skin is closed with interrupted vertical mattress sutures of 2-0 nylon
(Figure 65-12). The perineal incision is covered with povidone-iodine ointment and
nonadhesive gauze.
◆ A pedicle of the greater omentum is mobilized from the transverse colon and placed into
the pelvis to promote healing and prevent small bowel adhesions in the pelvis (Figure
65-13). The proximal end of the resected colon is brought through the colostomy site, and
the serosa of the colon is secured to the peritoneum with several interrupted sutures of
3-0 silk.
◆ The midline abdominal incision is closed by reapproximating the fascia in one layer with
two running absorbable sutures of loop 0 polydioxanone (PDS), beginning at the cranial
and caudal end of the incision. The skin is reapproximated with staples.
◆ The colostomy is matured by fi rst removing the staple line with electrocautery. The full-
thickness colonic mucosa is sutured to the dermis of the colostomy site circumferentially
with interrupted sutures of 3-0 Monocryl. The colostomy is covered with a stoma
appliance.
◆ The nasogastric tube is removed before the patient awakes from anesthesia.