Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 717
Allen
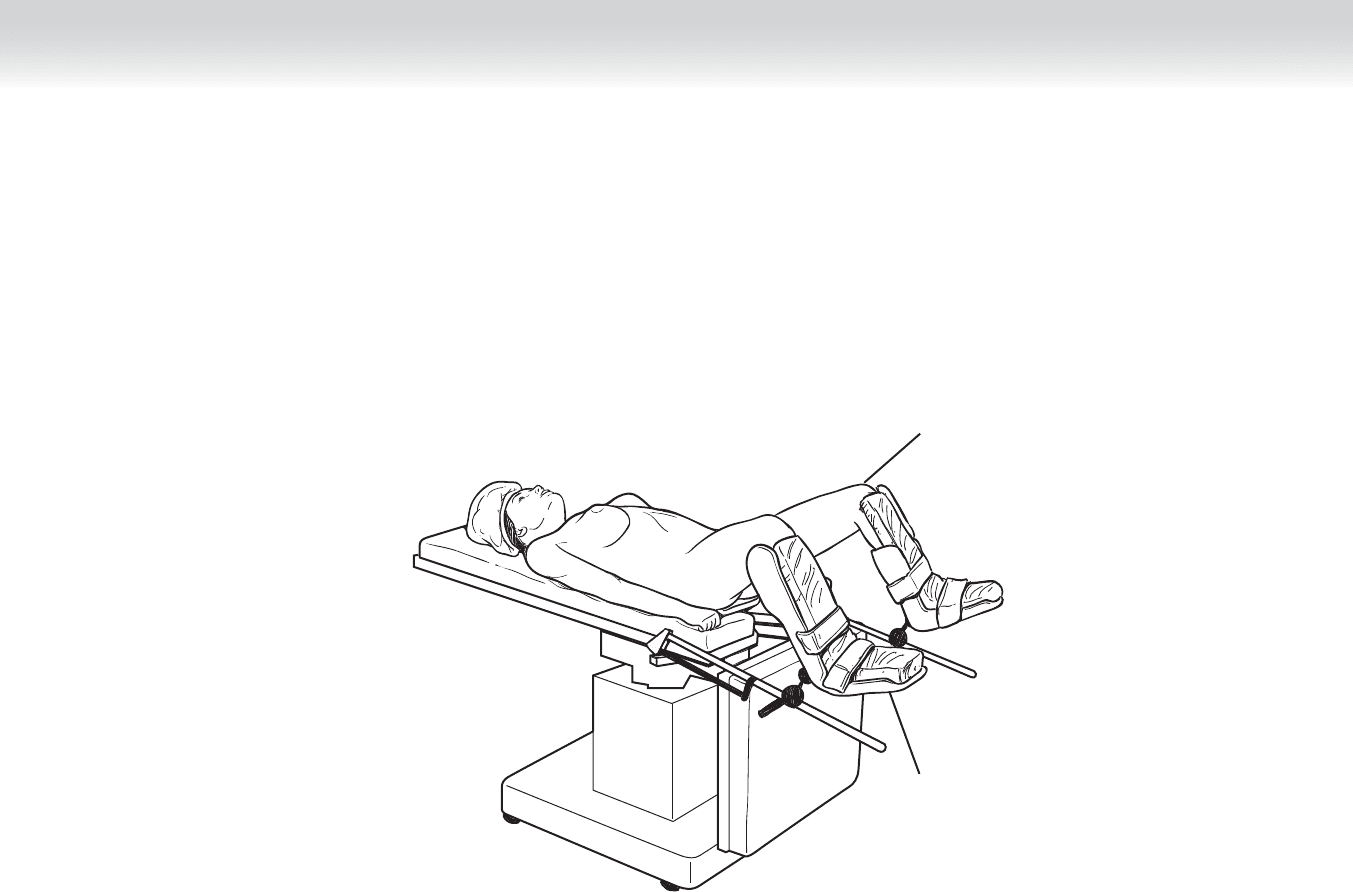
stirrups
Low lithotomy
position
FIGURE 63 –1

718 Section IX • Colon
STEP 3: OPERATIVE STEPS
1. INCISION
◆ A standard midline incision is made using a no. 10 blade knife from a point 2 cm above the
umbilicus, through midline, and down to the pubic symphysis.
◆ The abdomen is entered sharply and dissection is carried around the bladder obliquely. The
pubic symphysis is palpated, and the incision is extended through the pyramidalis muscle
as the inferior boundary of the incision.
◆ The abdomen is explored for additional pathologic fi ndings. The terminal ileum is identi-
fi ed, and the entire small bowel is run proximally to the ligament of Treitz. The liver is pal-
pated for the presence of masses.
Exposure
◆ A Bookwalter retractor is set up so that the arm attaches to the right side of the table.
◆ Moist laparotomy pads are folded in half and placed along the length of each side of the
abdominal wall. Two ratcheted Richardson retractors are positioned opposite each other in
lower oblique fashion, taking care not to impinge on the femoral canal.
◆ The small bowel is packed upward using a moist blue towel with a radiopaque loop attached
to it, and a wide Deaver ratcheted retractor is bent and placed to maintain exposure without
compression of the aorta or inferior vena cava.
◆ In female patients, the uterus should be retracted by placing a fi gure-of-eight stitch with
2-0 Vicryl through the posterior wall of the uterus as a retraction stitch. A ratcheted blad-
der blade is then placed to retract the uterus and bladder.
2. DISSECTION
◆ Total abdominal colectomy is performed according to the steps outlined in Chapter 62.
Please refer to that chapter for procedural details.
◆ The recess at the base of the mesosigmoid, called the intersigmoid fossa, is identifi ed and
delicately incised. The left ureter lies just deep to intersigmoid fossa and is identifi ed and
mobilized laterally. The ureter courses medially and parallel to the gonadal vessels, another
important landmark to identify.
◆ The inferior mesenteric pedicle is isolated. This is done by identifying the avascular window
at the base of the mesosigmoid while tenting the mesentery up. The window is incised and
extended proximally to the pelvic brim and distally down to the level of the sacral promon-
tory bilaterally.
CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 719
◆ The pedicle is thinned, clamped, divided, and ligated in standard fashion. Identifi cation of the
left ureter should be made before this to ensure it has not been drawn up into the pedicle.
◆ The posterior avascular mesorectal plane is entered, and sharp dissection is carried down to
the levator muscles. Care is taken to ensure that the superior and inferior hypogastric nerve
plexus running deep to this fascial plane is not damaged (see comments in Pearls and Pit-
falls section).
◆ Lateral dissection is then carried down in the appropriate avascular plane. Care is taken dur-
ing division of the lateral rectal stalks. The pelvic plexus named nervi erigentes—affecting
erectile function—as well as the middle rectal artery, are in close proximity to these stalks.
◆ Anterior dissection is carried between the anterior avascular plane of Denonvillier and the
reproductive structures. This is done down to the levator ani muscles.
◆ The decision to staple or hand sew the ileal pouch anastomosis is determined by the clini-
cal scenario. For example, patients with ulcerative colitis who do not have high-grade dys-
plasia may have a stapled anastomosis with mucosal surveillance on a regular basis. Patients
at high risk for developing malignancy (presence of cancer or high-grade dysplasia) should
have mucosectomy and hand-sewn ileal anal anastomosis.
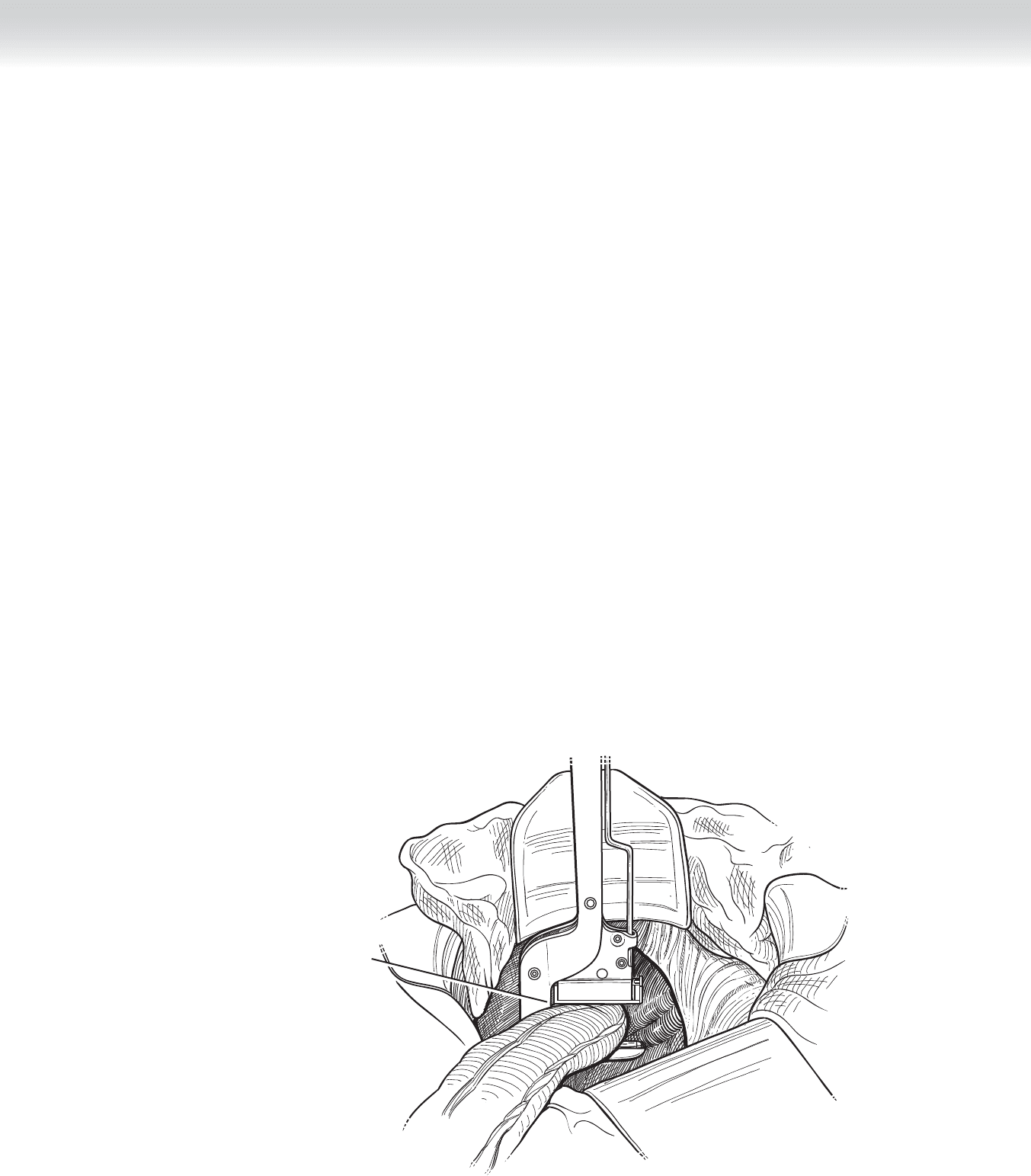
◆ A stapled anastomosis may be placed as low to the dentate line as anatomically possible
(Figure 63-2). The posterior mesorectum tapers distally, so there should not be excess vas-
cular tissue posteriorly, once the appropriate level of dissection has been reached.
Division below the level
of the levator muscles
FIGURE 63 –2
720 Section IX • Colon
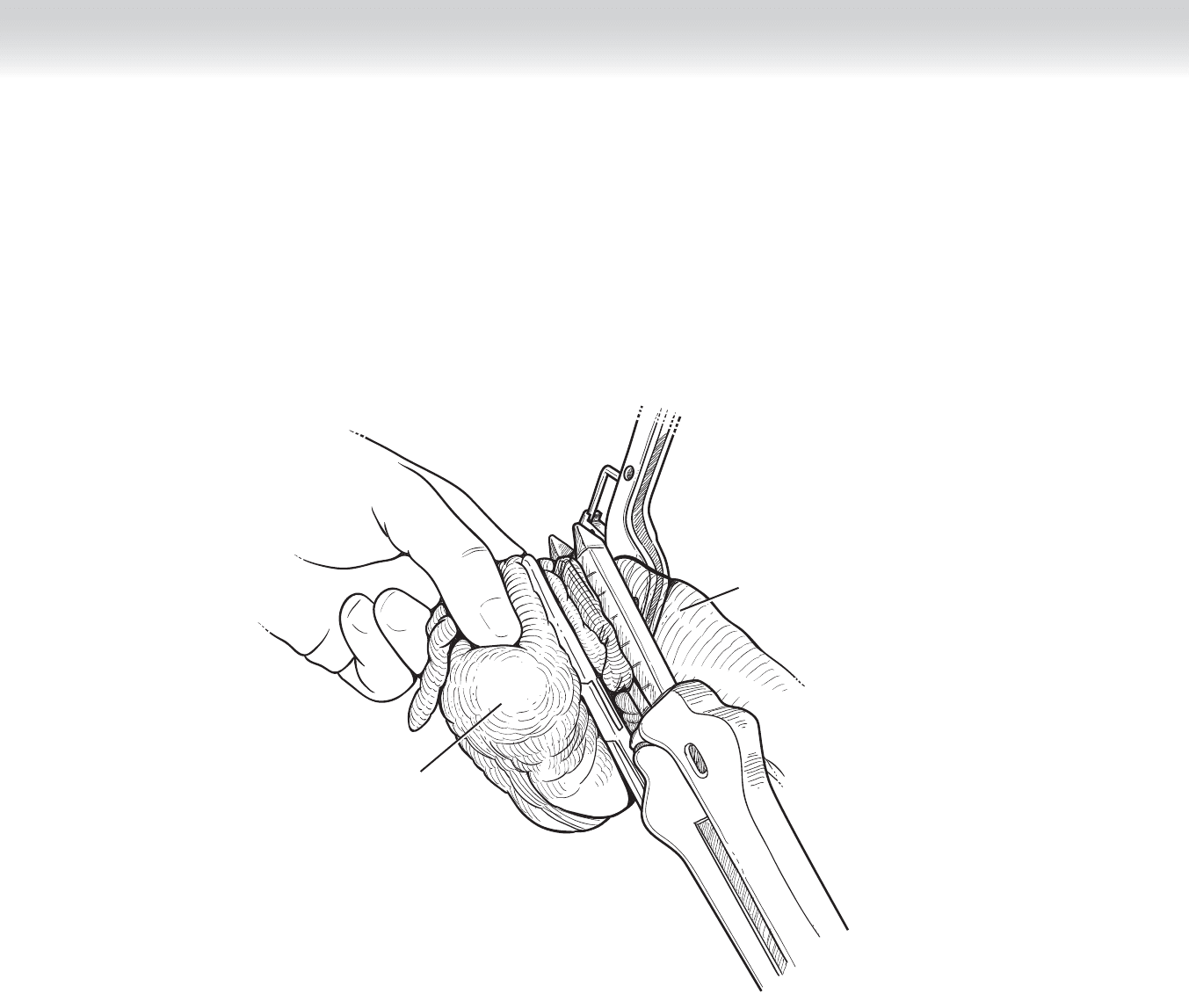
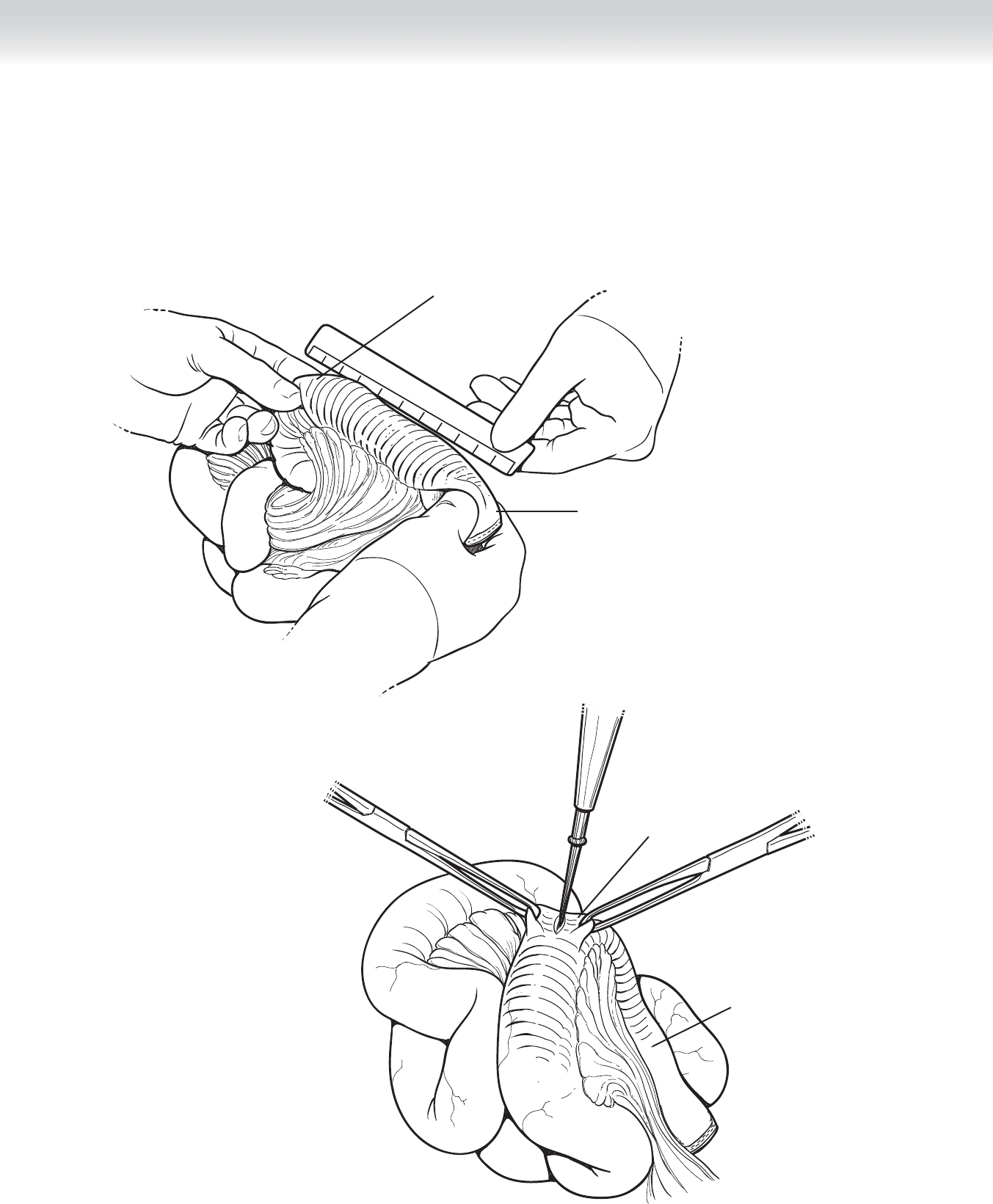
◆ The specimen is detached from the proximal small bowel using a 75-mm linear stapler
(Figure 63-3).
Terminal ileum
Cecum
FIGURE 63 –3
CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 721
Creation of the Ileal Pouch
◆ Attention to the method of pedicle ligation of the ileocolic artery is of paramount impor-
tance when performing proctocolectomy with the possibility of ileal pouch creation. The
ileocolic artery should be preserved through its entire distance, taking care to hug the mes-
enteric border of the cecum and distal terminal ileum before division of the bowel.
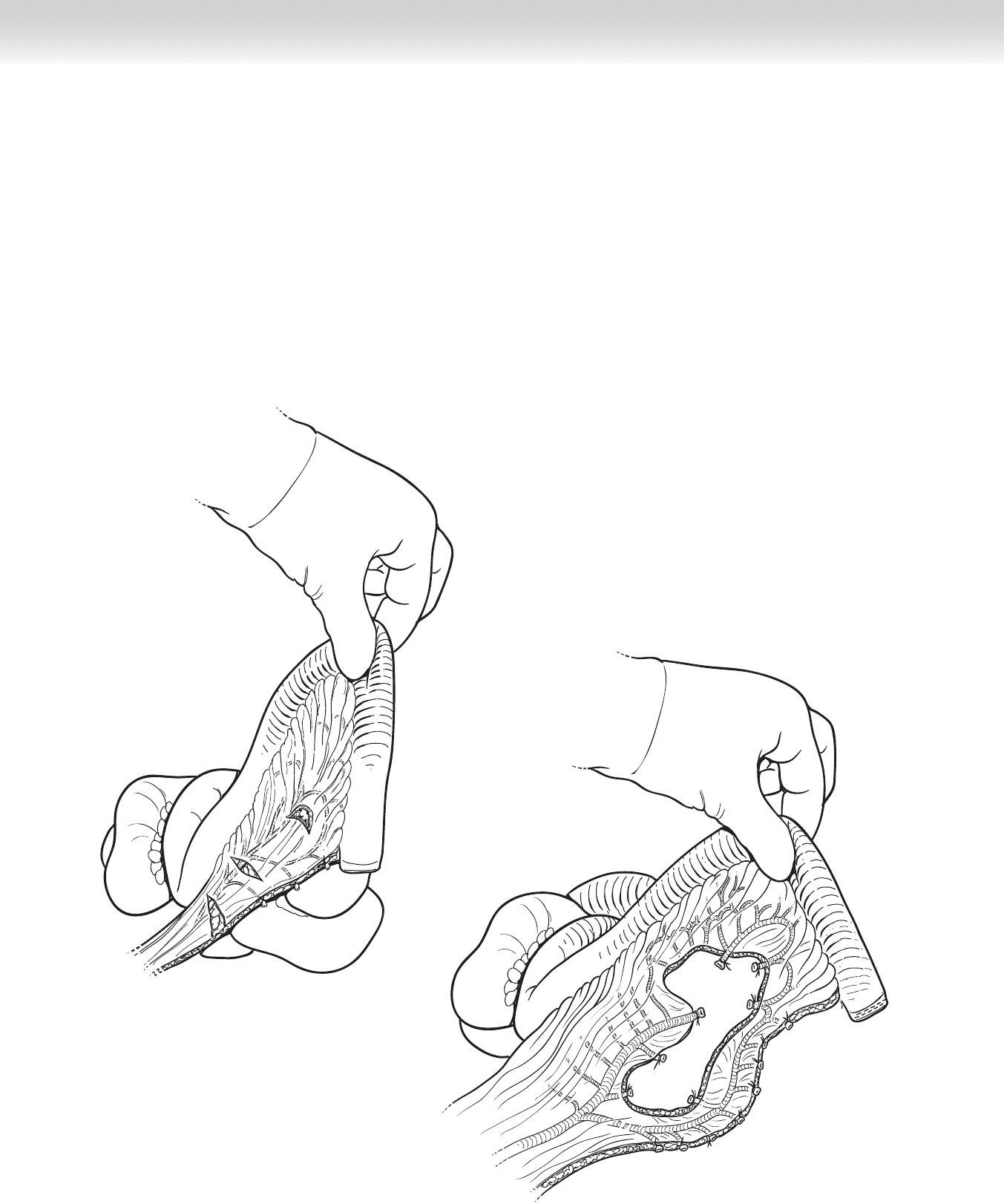
◆ Adequate length of the mesentery will dictate reach to the pelvis. A good preliminary length
is 1 to 2 cm distal to the pubic symphysis when measuring the apex of the pouch. Inade-
quate length may be regained by scoring the peritoneum or by distal ligation of the superior
mesenteric artery (SMA), provided adequate collateral fl ow exists through the ileal branch
(Figures 63-4 and 63-5).
FIGURE 63 –4
FIGURE 63 –5
722 Section IX • Colon
◆ The apex of the pedicle is identifi ed, and the pouch is measured so that it is approximately
15 to 20 cm from the apex (Figure 63-6).
◆ The apex of the pouch is entered using Bovie electocautery (Figure 63-7).
Terminal ileum
Apex of ileocolic
artery and pouch
Terminal ileum
Enterotomy
FIGURE 63 –6
FIGURE 63 –7
CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 723
Placement of linear
75-mm stapler
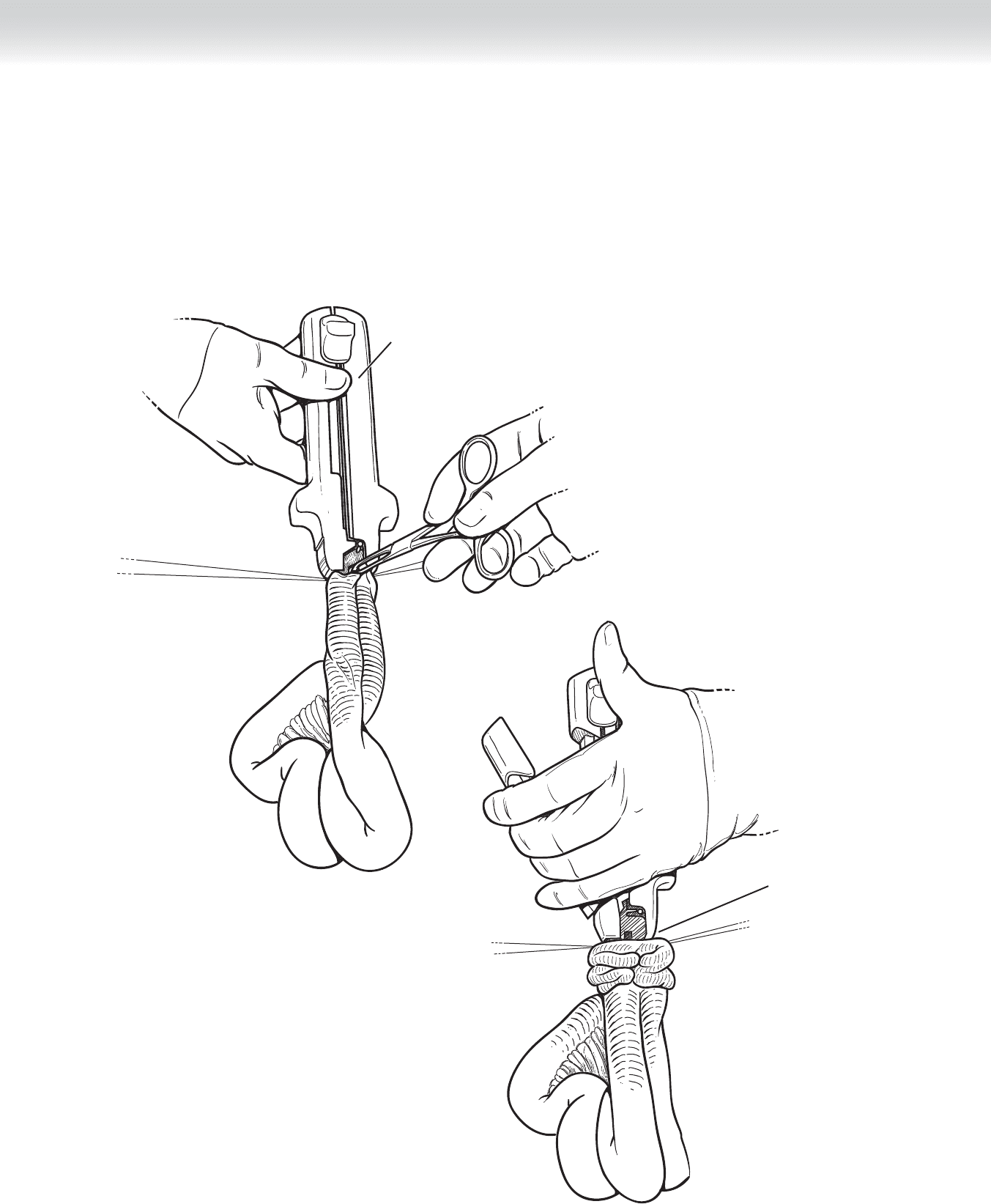
◆ The mesentery is positioned anterior to the pouch, because this is the shortest distance to the pelvis
with the least amount of tension on the pedicle.
◆ A 75-mm linear blue-load stapler is sequentially used to fi re between the two limbs at the antimes-
enteric border, thus creating the pouch (Figures 63-8 and 63-9).
FIGURE 63 –8
Firing of
second 75-mm
linear stapler to
create common wall
FIGURE 63 –9

724 Section IX • Colon
Hand-Sewn Anastomosis
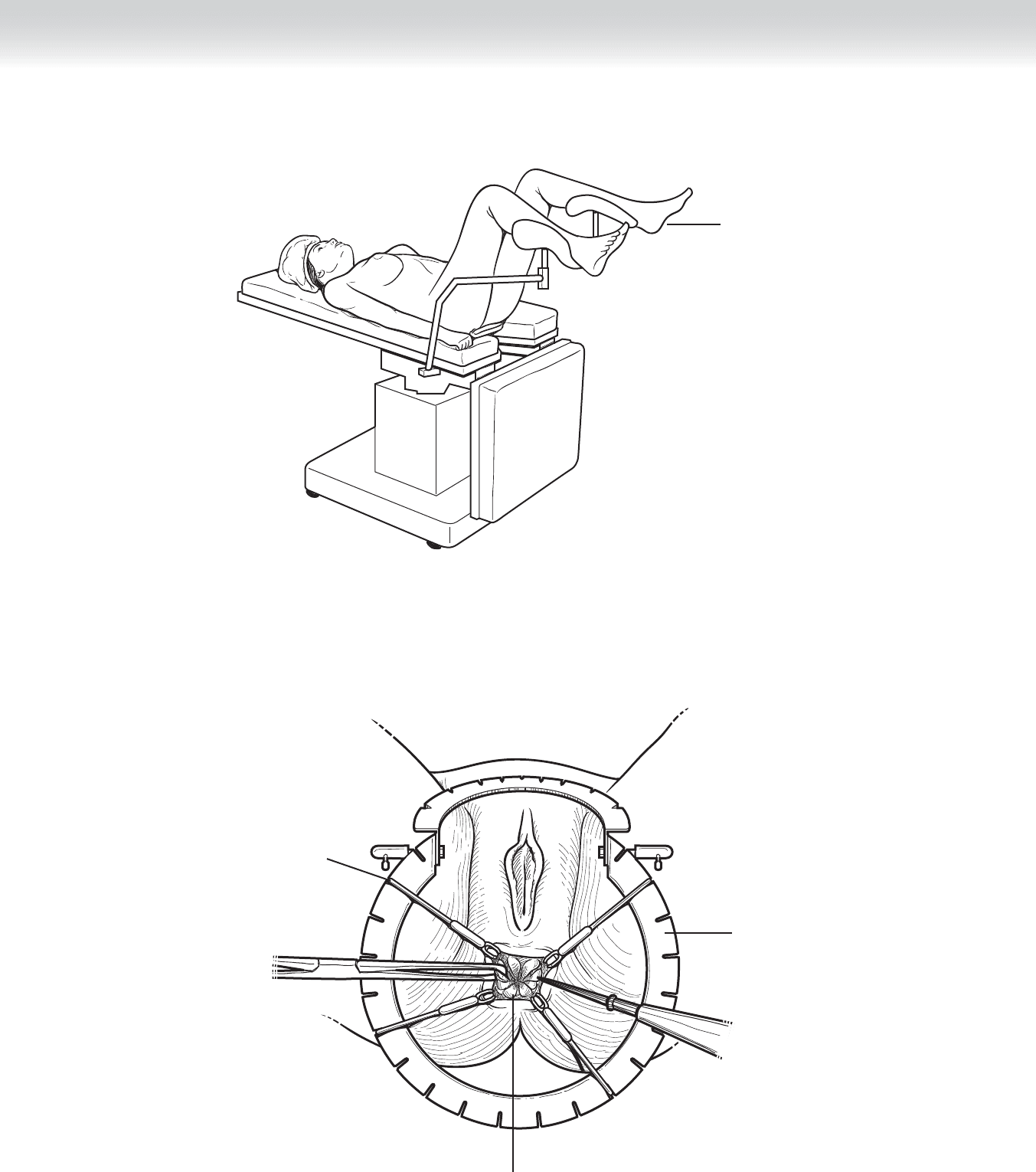
◆ The patient is positioned from low to high lithotomy (Figure 63-10). The perineal opera-
tor places a Lone Star retractor in the anal canal. The dentate line is drawn down to the
anal verge by sequential placement of retractor hooks (Figure 63-11). A Parks anal retrac-
tor may be placed to improve visualization of the anal canal. Mucosectomy is initiated fi rst
by infi ltrating 10 to 20 mL of 0.25% bupivacaine (Marcaine) with 1:200,000 epinephrine
circumferentially, raising the mucosa off the longitudinal muscle. The mucosa is circumfer-
entially incised using electrocautery or sharp dissection. Metzenbaum scissors are used to
lift the mucosa off the muscle proximally. Once the mucosa falls back circumferentially, a
full-thickness incision is made laterally and carried circumferentially around the distal
rectum. Once the specimen is free, the ileal pouch is prepared for anastomosis.
CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 725
High lithotomy
position
FIGURE 63 –10
Lone Star
retractor
Exposure of dentate line
Hooks placed
at dentate line
FIGURE 63 –11

726 Section IX • Colon
◆ A full-thickness stitch using a long 2-0 Vicryl suture is taken at the antimesenteric edge of
the pouch opening (posterior) and passed to the perineal operator through the anal canal
(Figure 63-12). Using the same suture, a full-thickness stitch is taken through the dentate
line posteriorly. This process is repeated for both lateral sides, and fi nally the anterior side.
The pouch is cinched down into the pelvis, and each suture is tied down (Figure 63-13).
Circumferential sutures are placed between each stitch in full-thickness fashion, taking care
to incorporate an edge of pouch with the dentate line. The anastomosis and mesentery
should be checked to ensure both are free from tension and there are no twists.
◆ The Lone Star retractor is removed, and the dentate is allowed to retract back into the anal
canal. Proctoscopy is performed, and the anastomosis is checked for air leaks by insuffl ating
while the proximal small bowel is clamped under saline.