Cui Dongmei. Atlas of Histology: with functional and clinical correlations. 1st ed
Подождите немного. Документ загружается.

CHAPTER 15
■
Digestive Tract
295
Secretory
Secretory
granules
granules
Secretory
granules
Gland of
Gland of
Lieberkühn
Lieberkühn
Gland of
Lieberkühn
Nuclei of the
Nuclei of the
paneth cells
paneth cells
Nuclei of the
paneth cells
A
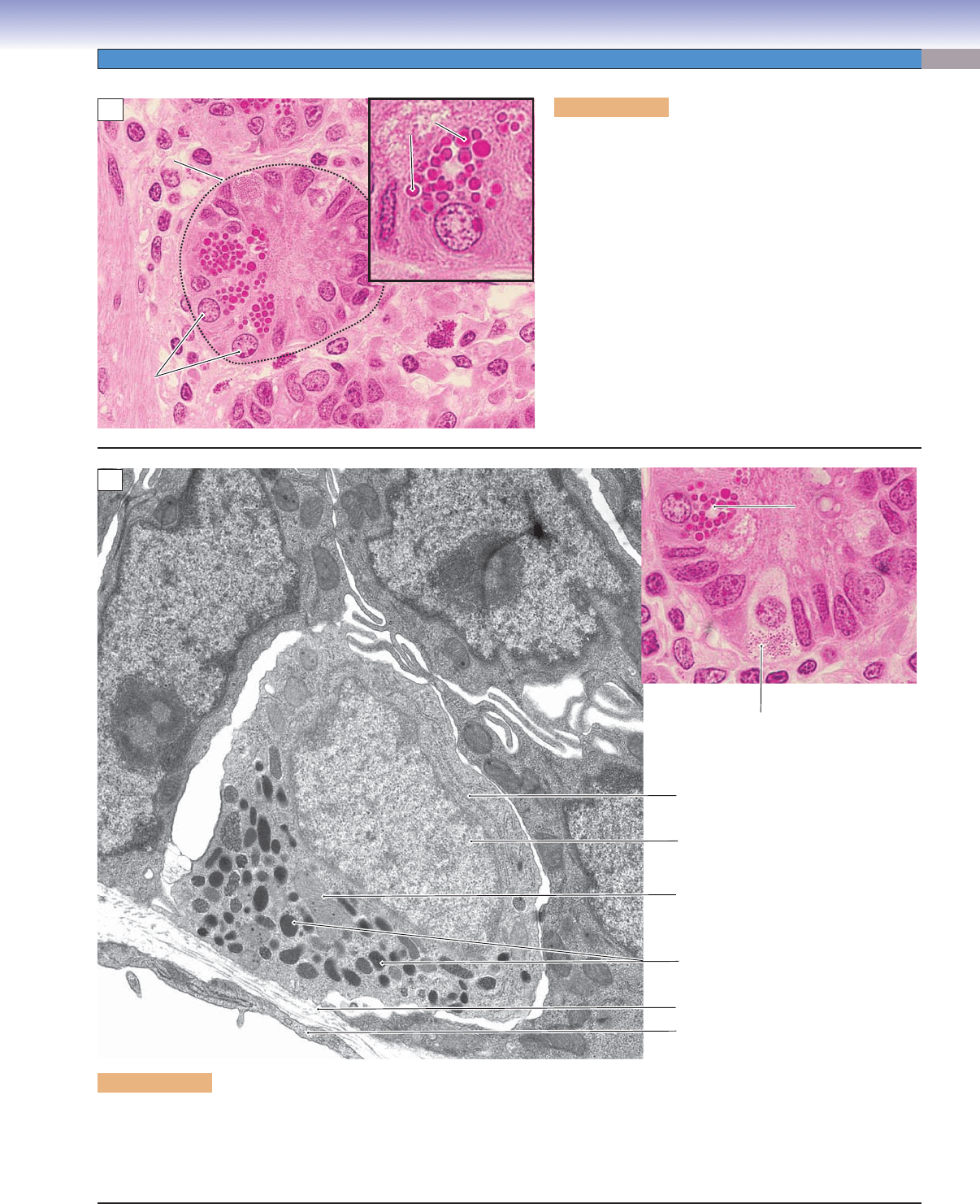
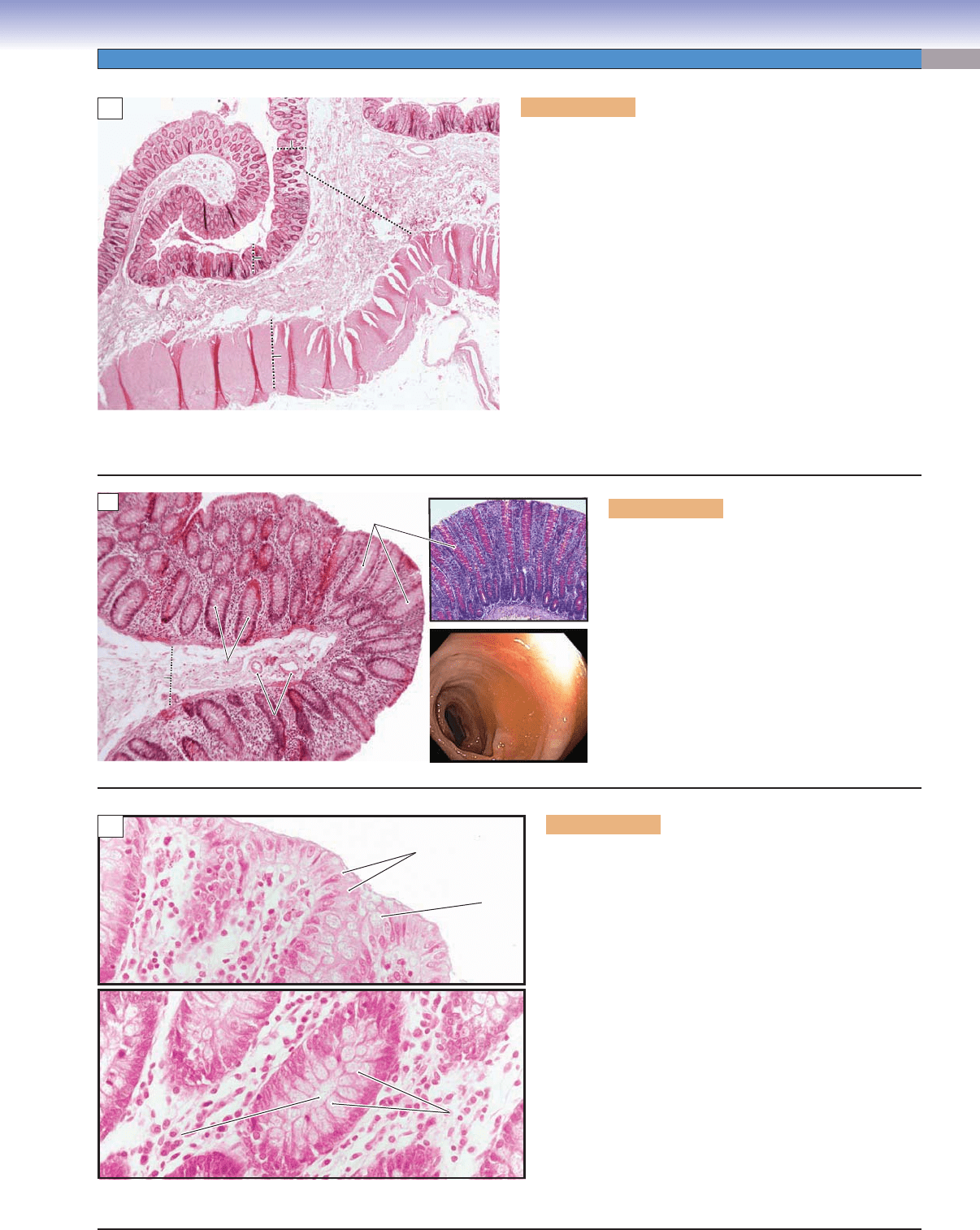
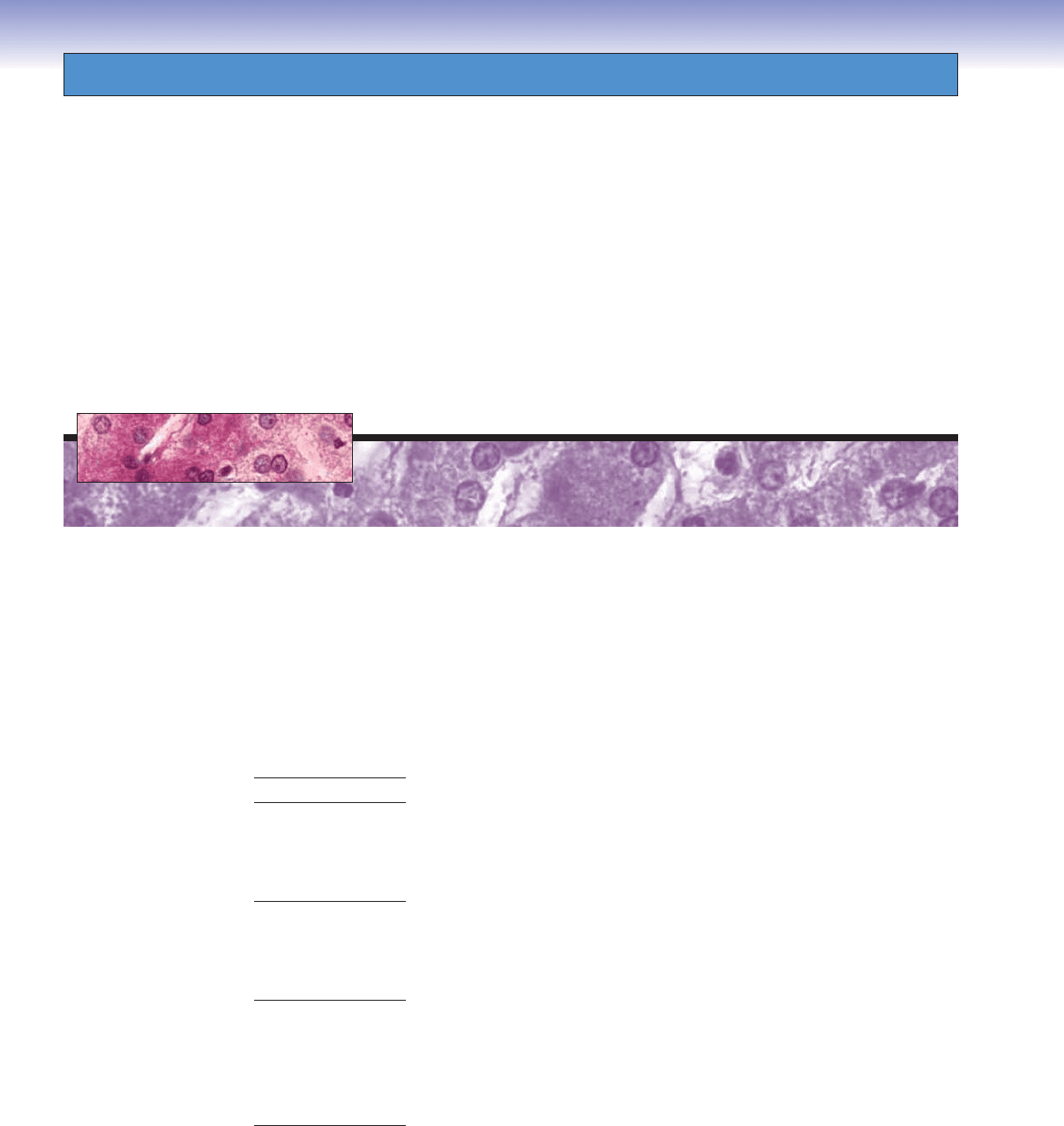
Figure 15-13A. Paneth cells, small intestine. H&E,
702; inset 1,488
Paneth cells have basally positioned nuclei and contain
acidophilic-secretory granules in the apical region of the
cytoplasm. These granules appear bright red in H&E stains.
Paneth cells are located at the base of the glands (crypts) of
Lieberkühn. Their secretory granules contain lysozymes,
tumor necrosis factor-a, and defensins (cryptidins). These
are antibacterial enzymes that help to regulate the normal
bacterial fl ora of the intestine. Paneth cells are protein-
secretory cells and have well-developed rough endoplasmic
reticulum (RER) and Golgi complexes. Like other epithelial
cells, the Paneth cells are derived from stem cells located at
the base of the intestinal glands of Lieberkühn. A gland of
Lieberkühn is indicated by the dashed line at left. Its lumen
is fi lled with secretory material and is not easy to see.
Figure 15-13B. Enteroendocrine cells, small intestine. EM, 10,611; (color) 1,028
There are many types of enteroendocrine cells, which are also called diffuse neuroendocrine cells, in the digestive tract. They are recog-
nized as hormone-releasing cells, and the various types of enteroendocrine cells are similar in appearance. They are often found at the
base of glands of Lieberkühn and have many mitochondria, abundant RER, and well-developed Golgi complexes (see Fig. 15-11A).
Their secretory granules are located at the basal cytoplasm. Each type of enteroendocrine cell releases one particular hormone.
Paneth cell
Paneth cell
Paneth cell
Enteroendocrine cell
Enteroendocrine cell
Enteroendocrine cell
Nucleus of enteroendocrine cell
Rough endoplasmic reticulum
Secretory granules
Basal lamina
Endothelial cell of capillary
Mitochondria
B
CUI_Chap15.indd 295 6/2/2010 3:24:25 PM
296
UNIT 3
■
Organ Systems
Inner circular muscle
Inner circular muscle
Inner circular muscle
Neuron cell bodies
Neuron cell bodies
Neuron cell bodies
Outer longitudinal muscle
Outer longitudinal muscle
Outer longitudinal muscle
Auerbach
Auerbach
plexuses
plexuses
Auerbach
plexuses
Glial cells
Glial cells
Glial cells
C
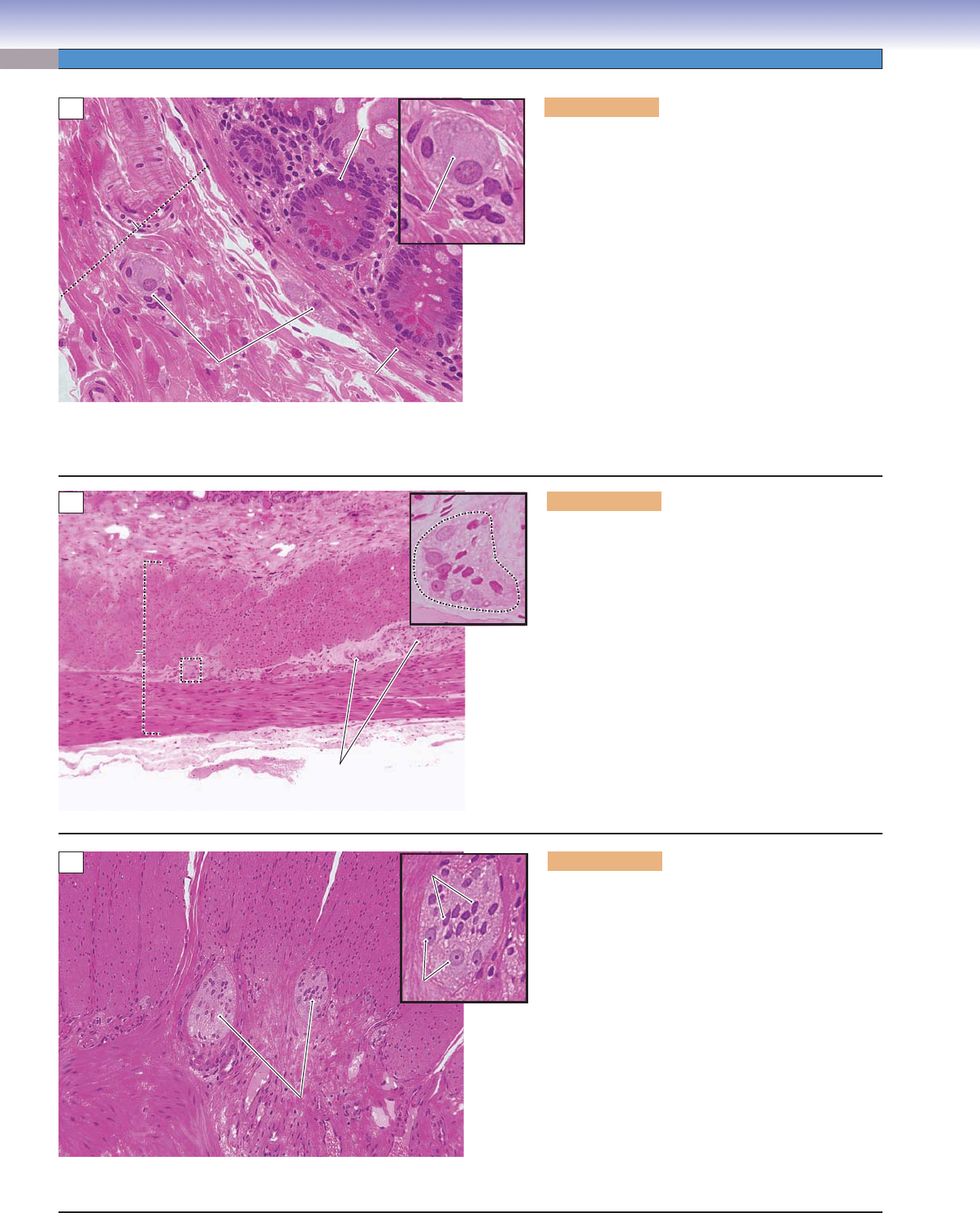
Figure 15-14A. Submucosal/Meissner plexus, small
intestine. H&E, 272; inset 544
The enteric nervous system is able to operate indepen-
dently, although it is usually infl uenced by the para-
sympathetic and sympathetic nervous systems. The
two types of ganglia of the enteric nervous system are
found in the wall of the digestive tract. (1) Submu-
cosal plexuses (Meissner plexuses) are located in the
submucosal layer. (2) Myenteric plexuses (Auerbach
plexuses) are located between the two layers of the
muscularis externa. Here is an example of a submu-
cosal plexus in the submucosa of the wall of the small
intestine. Submucosal plexuses are scattered small
groups of neuron cell bodies (sensory and motor neu-
rons and interneurons) and unmyelinated nerve fi bers.
The axons of the sensory neurons receive mechanical
and chemical signals from the glandular epithelium;
the axons of the motor neurons innervate the muscu-
laris mucosae and glandular epithelium.
S
S
u
u
b
b
m
m
u
u
c
c
o
o
s
s
a
a
Submucosa
Neuron cell body
Neuron cell body
Neuron cell body
Submucosal
Submucosal
plexus
plexus
Submucosal
plexus
Glandular
Glandular
epithelium
epithelium
Glandular
epithelium
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
A
Submucosa
Submucosa
Submucosa
Inner circular muscle
Inner circular muscle
Inner circular muscle
Outer longitudinal muscle
Outer longitudinal muscle
Outer longitudinal muscle
Auerbach
Auerbach
plexus
plexus
Auerbach
plexus
Auerbach plexus
Auerbach plexus
Auerbach plexus
Muscularis
Muscularis
enterna
enterna
Muscularis
enterna
B
Figure 15-14B. Muscularis externa, small intestine.
H&E, 68; inset 354
Here is an example of the muscularis externa of the
small intestine, which contains two layers of smooth
muscle. (1) Inner circular muscle layer: When the
smooth muscle fi bers in this layer contract, the diame-
ter of lumen of the small intestine decreases. (2) Outer
longitudinal muscle layer: This layer surrounds the
inner circular muscle layer. When the smooth muscle
fi bers in this layer contract, the length of the intestine
is reduced. These two layers of muscle work together
to make successive waves of involuntary movements
called peristalsis, which force digestive contents to
move downward into the large intestine. The inner
circular and outer longitudinal muscles are innervated
by axons from neurons in the myenteric/Auerbach
plexuses of the enteric nervous system (see Fig. 7-14).
Figure 15-14C. Myenteric/Auerbach plexus, mus-
cularis externa of the small intestine. H&E, ×136;
inset ×317
Myenteric plexuses (Auerbach plexuses) are found
between the inner circular muscle and the outer longi-
tudinal muscle layers. Myenteric (Auerbach) plexuses
are much larger than submucosal plexuses. The inset
shows several neuron cell bodies and enteric glial cells
surrounded by connective tissues in a myenteric plexus.
Neurons in both the submucosal plexuses and the
myenteric plexuses are multipolar in shape. Like sub-
mucosal plexuses, they may have little or no encapsula-
tion and contain unmyelinated nerve fi bers and gangli-
onic neurons mainly belonging to the enteric nervous
system. The enteric nervous system coordinates peri-
staltic refl exes, which evoke waves of contraction and
relaxation of the gut wall, moving the contents toward
the anus and also regulates enteroendocrine cells.
CUI_Chap15.indd 296 6/2/2010 3:24:31 PM
CHAPTER 15
■
Digestive Tract
297
Goblet
Goblet
cells
cells
Goblet
cells
Germinal center
Germinal center
of lymphatic nodules
of lymphatic nodules
Germinal center
of lymphatic nodules
C
Glands of
Glands of
Lieberkühn
Lieberkühn
Glands of
Lieberkühn
Submucosa
Muscularis externa
Villi
Villi
Villi
Mucosa
Mucosa
Mucosa
Inner circular muscle
Outer longitudinal muscle
Muscularis
mucosae
Glands of
Glands of
Lieberkühn
Lieberkühn
Glands of
Lieberkühn
Villus
Villus
Villus
A
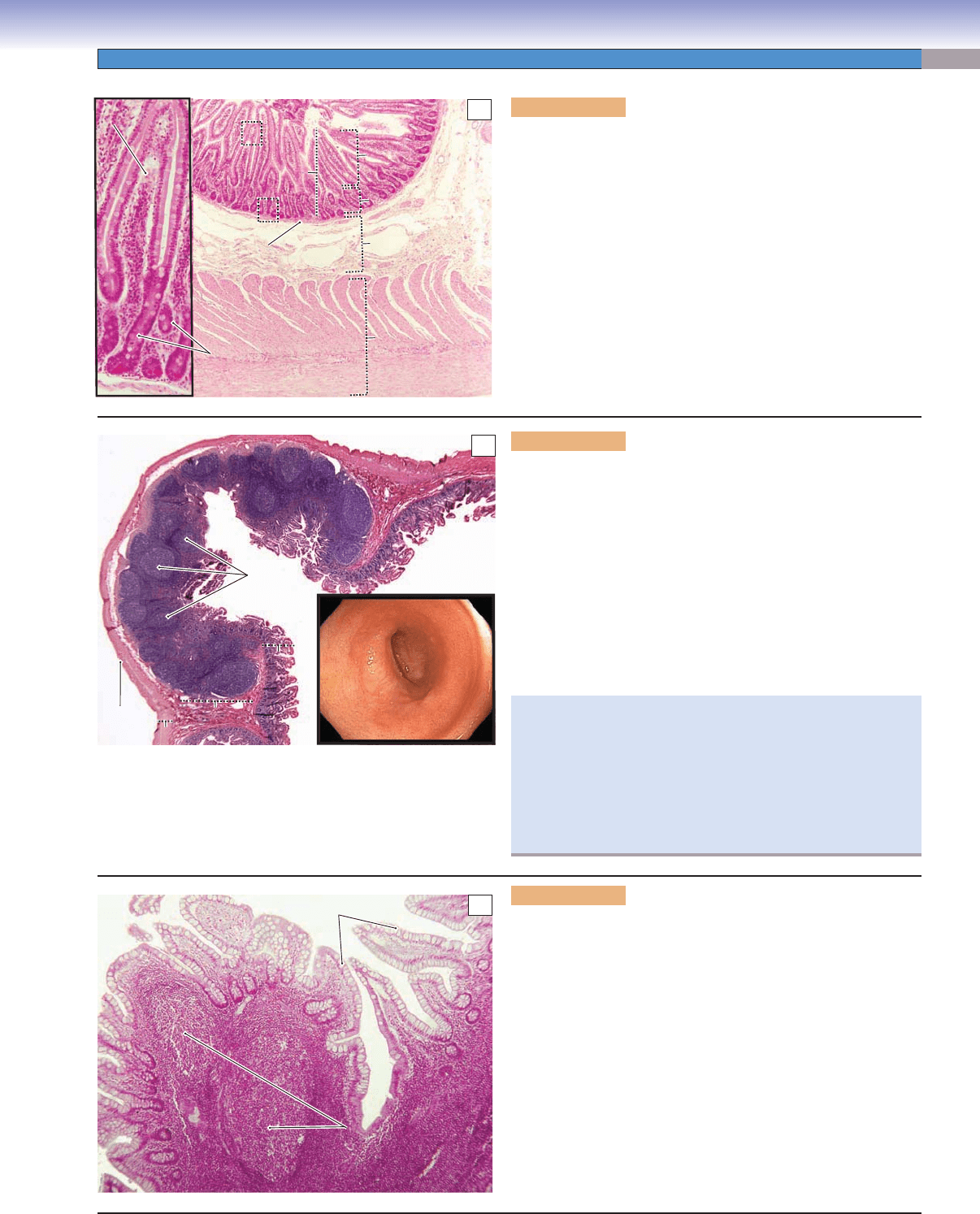
Figure 15-15A. Jejunum, small intestine. H&E, 34; inset
103
The jejunum is a segment of small intestine between the duode-
num and the ileum. It is similar in general structure and layers to
the other regions of the small intestine. It contains mucosa, sub-
mucosa, muscularis externa, and serosa. The jejunum has neither
Brunner glands nor Peyer patches. The cells of the epithelium of
the mucosa are similar to those of the epithelium of other regions
of the small intestine (see Figs. 15-12A to 15-13B). Goblet cells
steadily increase in number along the entire length of the small
intestine from the duodenum to the ileum. Paneth cells are often
found at the base of the glands of Lieberkühn (lower inset). The
glands of Lieberkühn are intestinal glands (simple tubular glands),
which extend from the spaces between the bases of the villi deep
into the lamina propria.
Figure 15-15C. Mucosa of the ileum, small intestine. H&E, 68
Here is an example of the mucosa of the ileum showing numerous
goblet cells in the surface epithelium. In this section, two lym-
phatic nodules are located in the lamina propria. These lymphatic
nodules have germinal centers and are, therefore, secondary
lymphatic nodules. These nodules may extend into the submu-
cosa (Fig. 15-15B). The lymphatic nodules and Peyer patches
are locations where lymphocytes can interact with antigens and,
therefore, play important roles in immunological function. Naive
B cells (B lymphocytes) within these lymphoid patches are primed
and awaiting exposure to unique epitopes. When stimulated by a
specifi c antigen from the intestinal mucosa, they differentiate into
plasma cells and memory B cells. In response, the plasma cells pro-
duce large quantities of immunoglobulins ([Ig] antibodies), espe-
cially IgA to combat mucosal infection. The memory B cells live
on in the Peyer patches to retain immunity to a specifi c antigen.
Peyer
Peyer
patch
patch
Peyer
patches
Mucosa
Mucosa
Mucosa
Submucosa
Submucosa
Submucosa
Muscularis enterna
Muscularis enterna
Muscularis externa
Serosa
Serosa
Serosa
B
Figure 15-15B. Ileum with Peyer patches, small intestine.
H&E, 13
The ileum is the longest segment of the small intestine making up
three fi fths of the 6 to 7 m length of the small intestine. One of the
unique features of the ileum is the presence of clusters of lymphatic
nodules called Peyer patches. These are most numerous in the dis-
tal portion of the ileum. Some isolated lymphatic nodules may be
found in other parts of the digestive tract but not in aggregations
of clusters of nodules like Peyer patches. The villi in the ileum are
shorter and smaller than in other parts of the small intestine. The
numbers of goblet cells are greatly increased in the ileum. The inset
shows an endoscopic image of the ileum with its relatively smooth
surface.
Vitamin K is absorbed in both the jejunum and the ileum, but
vitamin B12 is only absorbed in the ileum (especially the ter-
minal ileum). The absorption of vitamin B12 requires coupling
with gastric intrinsic factor, which is produced by parietal cells in
the stomach; these two substances become intimately associated
with the wall of the ileum. If a large portion of the stomach or
ileum is surgically removed, vitamin B12 defi ciency may result,
leading to megaloblastic anemia and neurologic symptoms.
CUI_Chap15.indd 297 6/2/2010 3:24:39 PM
298
UNIT 3
■
Organ Systems
Colon
Descending
colon
Sigmoid
colon
Rectum
Transverse colon
Ascending
colon
Cecum
Appendix
Appendix
Appendix
Teniae coli
Adipose tissue
Serosa/adventitia
Mucosa
Epithelium
Lamina
propria
Muscularis
mucosae
Teniae coli
Circular muscle
Longitudinal muscle
band (teniae coli)
Submucosa
Muscularis
externa
Vein
Artery
Nerve
Rectum
Rectum
Rectum
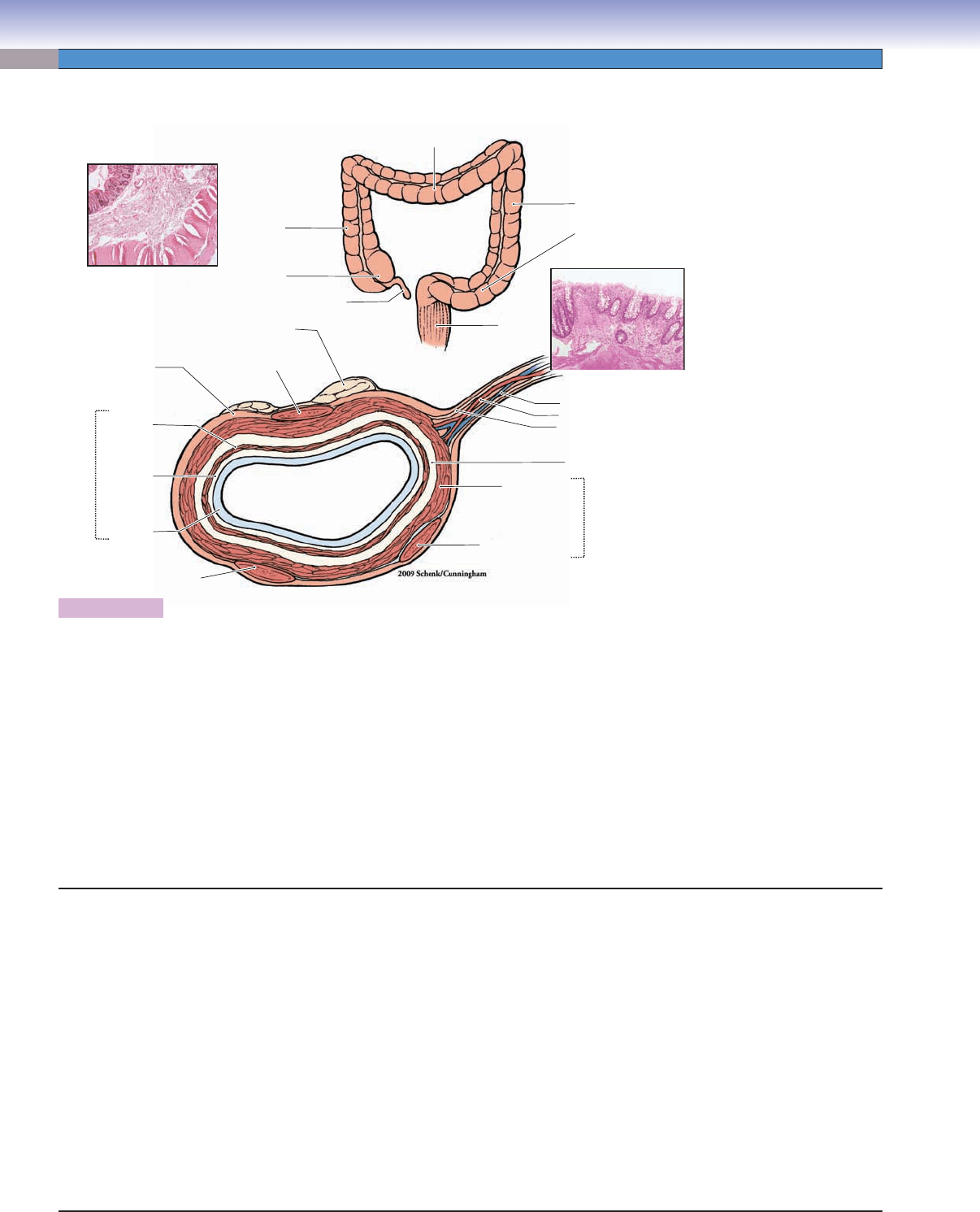
Figure 15-16.
Overview of the large intestine. H&E (left), 14; (right) 36
The large intestine connects the small intestine to the anal canal. The large intestine is about 1.5 m long, much shorter than the
small intestine. It consists of the cecum, appendix, colon, rectum, and anal canal. (1) The cecum is a small blind pouch of the large
intestine, at the junction of the ileum and the ascending colon. The ileum and cecum are separated by the ileocecal valve, which
prevents feces from backing up into the small intestine. (2) The appendix is a very short, small-diameter blind end tube that attaches
to the posterior-medial wall of the cecum. It contains aggregates of lymphatic nodules in the lamina propria. (3) The colon is the
longest part of the large intestine and includes ascending, transverse, descending, and sigmoid colons. (4) The rectum connects the
sigmoid colon to the anal canal. (5) The anal canal is externally surrounded by a layer of skeletal muscle called the exterior sphincter.
The junction between the rectum and the anal canal is called the anorectal junction, also called the dentate line, which marks the
transitional epithelium change from simple columnar epithelium to stratifi ed squamous epithelium. The large intestine has the same
general structure of mucosa, submucosa, muscularis externa, and serosa/adventitia as the small intestine. However, the large intestine
has a large lumen (excepting the appendix) and a large number of goblet cells lining the surface of the mucosa. It has crypts (intestinal
glands) but no villi, and the outer longitudinal muscle layer of the muscularis externa has become three narrow bands called teniae
coli. Functions of the large intestine include the absorption of water and salts and the formation, storage, and elimination of feces.
Large Intestine
Large Intestine
I. Cecum
A. Mucosa (crypts/glands; no villi)
B. Submucosa
C. Muscularis externa (inner circular muscle; teniae coli)
D. Serosa
II. Appendix
A. Mucosa (aggregated lymphatic nodules)
B. Submucosa
C. Muscularis externa (inner circular and outer longitudinal
muscles)
D. Serosa
III. Colon: ascending, transverse, descending, and sigmoid portions
A. Mucosa (crypts/glands; no villi)
B. Submucosa
C. Muscularis externa (inner circular muscle; teniae)
D. Serosa/adventitia
IV. Rectum
A. Mucosa
B. Submucosa
C. Muscularis externa (inner circular and outer longitudinal
muscles)
D. Adventitia
V. Anal Canal
A. Mucosa (stratifi ed squamous)
B. Submucosa
C. Muscularis externa (internal and external sphincters)
D. Adventitia
CUI_Chap15.indd 298 6/2/2010 3:24:47 PM
CHAPTER 15
■
Digestive Tract
299
Submucosa
Submucosa
Submucosa
Mucosa
Mucosa
Mucosa
Mucosa
Mucosa
Mucosa
S
S
u
u
b
b
m
m
u
u
c
c
o
o
s
s
a
a
Submucosa
Circular muscle of
Circular muscle of
muscularis externa
muscularis externa
Circular muscle of
muscularis externa
A
Figure 15-17A. Colon, large intestine. H&E, 15
The colon is the longest part of the large intestine. It contains an
ascending colon, transverse colon, descending colon, and sigmoid
colon. The colon receives digestive contents from the small intes-
tine and absorbs a large volume of water and electrolytes from the
contents. Bacteria in the colon make large quantities of vitamins
K and B12, but absorption is limited. The colon also forms and
stores feces, the waste matter leftover after the digestion process
has been completed. The movement of the contents in the large
intestine is slower than in the small intestine, taking 8 to 15 hours
to move the chyme (thick, semifl uid mass) from the cecum to the
rectum, where feces are stored. The mucosa of the colon has a
smooth surface (no villi) and contains glands of Lieberkühn. The
submucosa contains blood vessels, lymphatic vessels, and nerve
fi bers as well as submucosal plexuses, but no glands are present.
The muscularis externa includes the circular muscle (shown here).
The longitudinal muscle is aggregated into three bands called
teniae coli (Fig. 15-16). The myenteric (Auerbach) plexuses are
located between these two muscle layers.
Glands of
Glands of
Lieberkuhn
Lieberkuhn
Glands of
Lieberkühn
Glands of
Glands of
Lieberkühn
Lieberkühn
Glands of
Lieberkühn
S
S
u
u
b
b
m
m
u
u
c
c
o
o
s
s
a
a
Submucosa
Blood
Blood
vessels
vessels
Blood
vessels
Normal colon
B
Figure 15-17B. Colon, large intestine. H&E,
×68 (left); mucous stain, ×44 (upper right)
The glands of Lieberkühn are intestinal glands
that are straight tubular glands and are located
in the lamina propria of the mucosa. The glands
of Lieberkühn in the large intestine are similar to
those of the small intestine, but they contain no
Paneth cells. They are composed of great numbers
of goblet cells, columnar absorptive cells, and
some enteroendocrine cells. A thin layer of the
muscularis mucosae is found beneath the lamina
propria; it is part of the mucosa. The upper right
image shows the goblet cells, which appear red
because of the mucous stain.
Goblet
Goblet
cells
cells
Goblet
cells
Goblet
Goblet
cell
cell
Goblet
cell
Lumen of the
Lumen of the
gland of Lieberkühn
gland of Lieberkühn
Lumen of the
gland of Lieberkühn
Columnar
Columnar
absorptive cell
absorptive cell
Columnar
absorptive cells
C
Figure 15-17C. Mucosa of the colon, large intestine.
H&E, 272
Upper: The superior part and surface of the mucosa of the
colon consists of columnar absorptive cells and goblet cells.
These absorptive cells play an important role in the absorp-
tion of water and electrolytes. Water enters the absorptive
cells entirely by diffusion. Most water absorption occurs in
the colon, especially in the proximal colon. Goblet cells pro-
duce mucus, which protects the wall of the large intestine,
glues fecal material together, and lubricates the passage.
The surface of the large intestine is much smoother than the
small intestine because there are no villi.
Lower: The inferior part of the mucosa in the colon contains
straight tubular glands, glands of Lieberkühn, which are cut
in cross section here. Most cells in these glands are goblet cells
with basally positioned nuclei. The secretory (mucinogen)
granules located at the apical ends of the cells appear white
here. Enteroendocrine cells and stem cells also can be found.
The stem cells are located at the base of the glands (crypts) of
Lieberkühn and can be differentiated from other cell types of
epithelia. Paneth cells are not present in the large intestine.
CUI_Chap15.indd 299 6/2/2010 3:24:50 PM
300
UNIT 3
■
Organ Systems
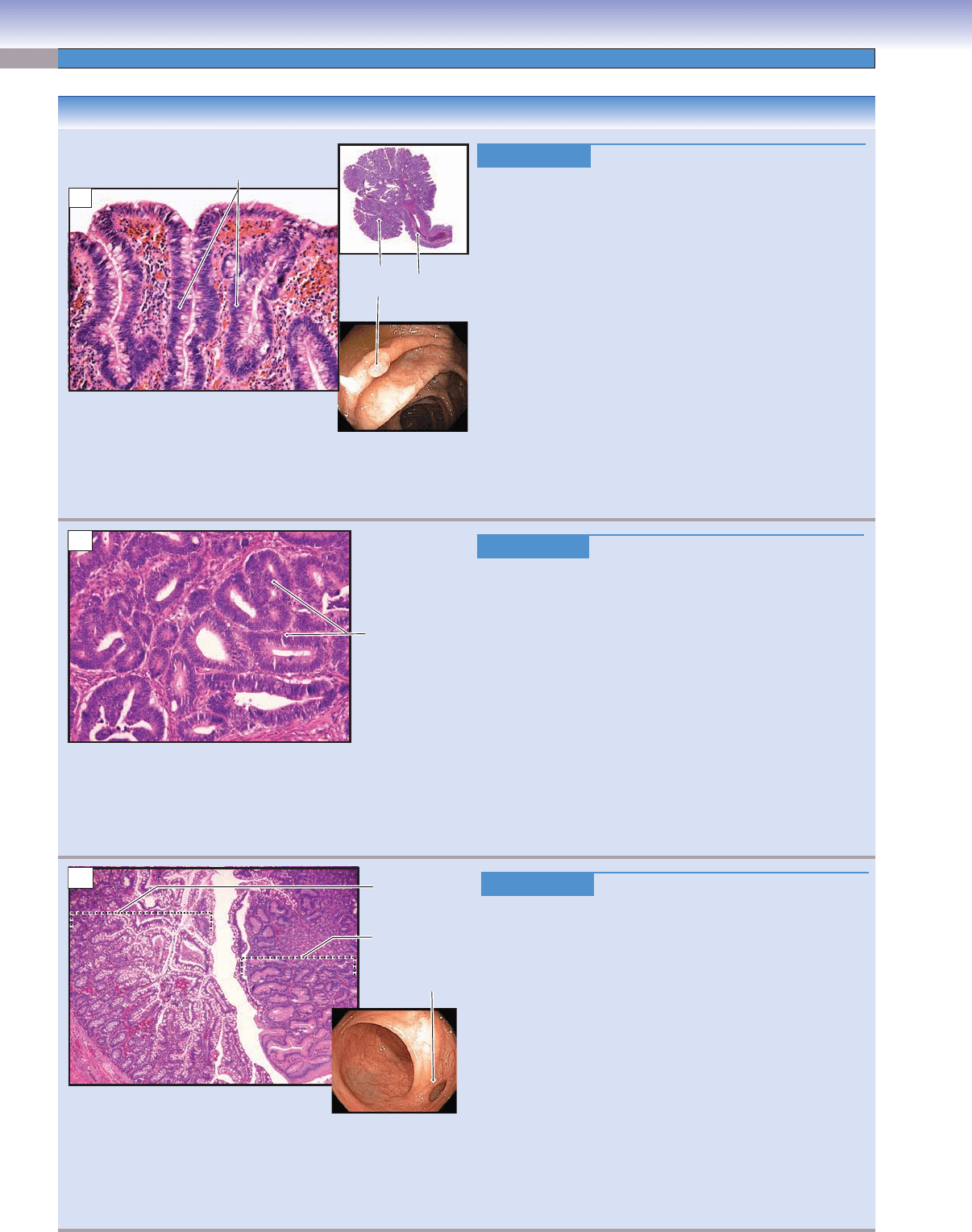
Figure 15-18A. Colon Polyps. H&E, 97; inset (upper) 1.3
Colon polyps are tissue masses that grow on the inner
mucosal surface and protrude into the lumen of the colon.
Polyps may contain a stalk or may be sessile, without a stalk.
There are several types of polyps, the most common of which
are adenomatous and hyperplastic. Adenomatous polyps are
benign neoplasms, subdivided based on morphologic fea-
tures into tubular adenomas, tubulovillous adenomas, and
villous adenomas. Although adenomatous polyps are them-
selves benign, they should be considered as having malignant
potential, because adenocarcinoma may arise in these polyps.
Hyperplastic polyps, which are common in the descending
colon and rectum, are considered benign with minimal risk for
progression to cancer
. Pseudopolyps may be seen in infl am-
matory bowel disease, particularly ulcerative colitis. Polyps
may be removed during colonoscopy by endoscopic mucosal
resection and sent for pathologic evaluation. These images
show a large, pedunculated tubular adenoma (inset) and a
higher power view of the adenomatous epithelium featuring
pseudostratifi cation of the crypt cells.
Figure 15-18B. Colorectal Cancer. H&E, 97
Colorectal cancer is a malignant neoplasm of the colon or the
rectum. Risk factors include genetics, infl ammatory bowel
disease—especially ulcerative colitis—adenomatous polyps,
high-fat and low-fi ber diets, and excessive red meat consump-
tion. Adenocarcinoma is the most common type of colon cancer
(98% of cases), arising from the mucosal glandular epithelium,
often in adenomatous polyps. Colorectal carcinomas invade
through the layers of the intestinal wall and metastasize pre-
dominantly through the lymphatic system. Depending on the
location, colorectal cancers may be asymptomatic for years.
Presenting symptoms may be a change in bowel habits due to
bowel obstruction, blood in the stool, or iron defi ciency ane-
mia. Surgical resection is the fi rst choice for early-stage cancer,
although chemotherapy may be considered. This photomicro-
graph shows a moderately differentiated adenocarcinoma of
the colon infi ltrating the muscularis propria.
Figure 15-18C. Meckel Diverticulum. H&E, ×19
Meckel diverticulum is a congenital abnormality characterized
by an outpouching in the small bowel due to failure of the
vitelline duct to close or involute. As a true diverticulum, it
contains all three layers (mucosa, submucosa, and muscu-
laris propria) of the normal bowel wall and is found on the
antimesenteric aspect of the bowel. Meckel diverticula occur
in 2% of the population, are usually located within 2 ft of
the ileocecal valve, and are about 2 in length. Some Meckel
diverticula contain heterotopic rests of pancreatic or gastric
mucosa. Most people with a Meckel diverticulum are asymp-
tomatic. Bleeding, infl
ammation, and peptic ulceration and
perforation can occur, producing signs and symptoms simi-
lar to appendicitis. Surgery is the appropriate treatment for
symptomatic patients. This image shows a section of a Meckel
diverticulum showing normal ileal mucosa with goblet cells
on the left side and ectopic gastric mucosa on the right side.
This gastric mucosa increases the risk of perforation because
of the elaboration of acid.
CLINICAL CORRELATIONS
Pseudostratified
columnar epithelium
Stalk
Colon
polyp
A
Adenocarcinoma
(malignant glands)
B
Ectopic
gastric
mucosa
Meckel
diverticulum
Ileal
mucosa
C
CUI_Chap15.indd 300 6/2/2010 3:24:57 PM
CHAPTER 15
■
Digestive Tract
301
Serosa
Submucosa
Submucosa
Submucosa
Mucosa
Mucosa
Mucosa
Muscularis externa
Muscularis externa
Muscularis externa
Lymphatic
nodules
Lumen
A
Anal canal
Anal canal
Anal canal
Stratified
squamous
epithelium
Simple
columnar
epithelium
Rectum
Rectum
Rectum
Glands (crypts) of
Glands (crypts) of
Lieberkühn
Lieberkühn
Glands (crypts) of
Lieberkühn
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
Large
Large
vein
vein
Large
vein
B
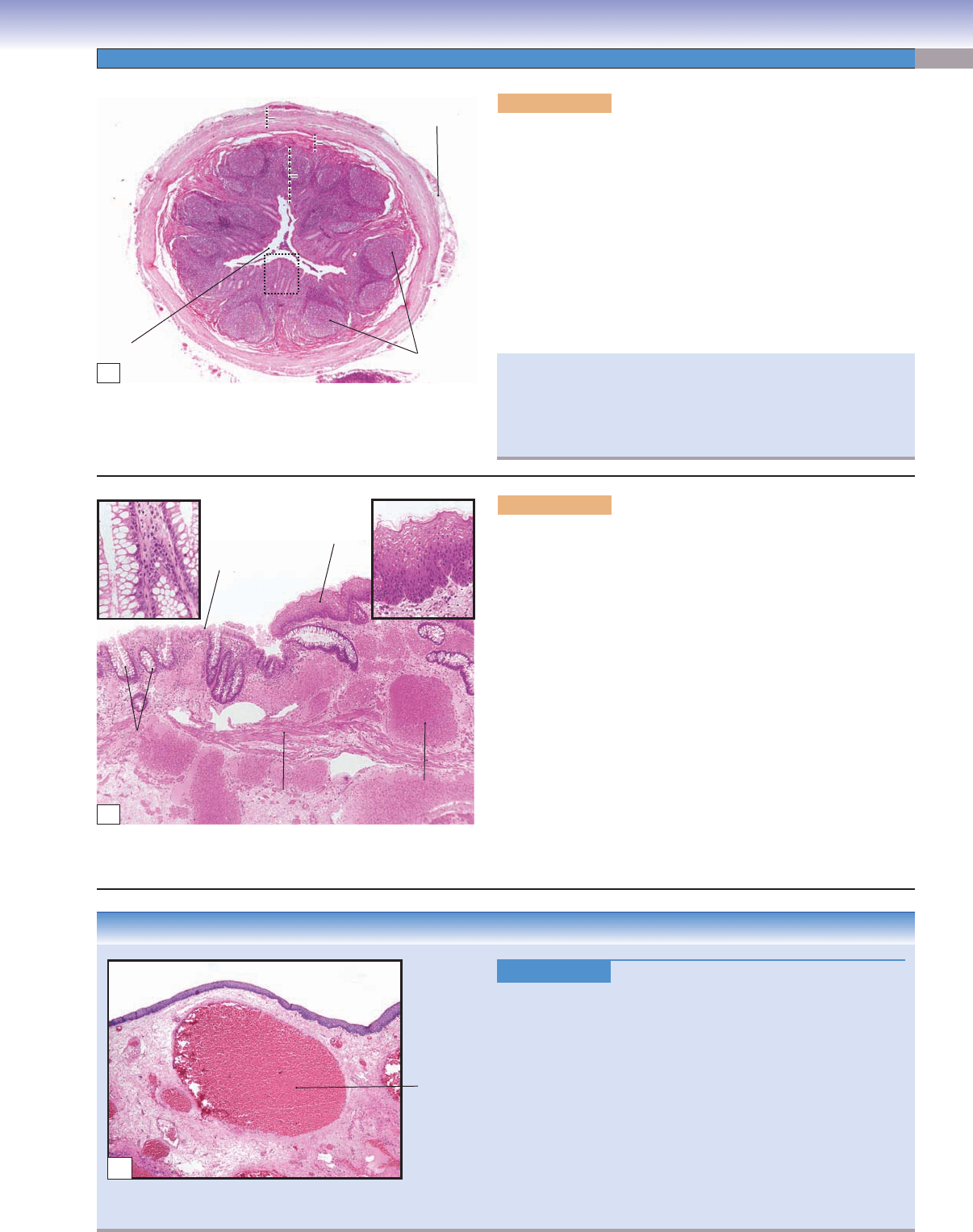
Figure 15-19A. Appendix and cecum. H&E, 17
The appendix is a fi ngerlike blind-ended tubular structure, about
10 cm in length, extending from the cecum distal to the ileocecal
valve. The cecum is the fi rst segment of the large intestine, where it
connects with the ileum. The small and large intestines are separated
by the ileocecal valve. The appendix has a small, irregular lumen
and many lymphatic nodules in the mucosa. Although its role in
digestion is not clear, it may participate in immunological func-
tion and help maintain normal bacteria fl ora in the large intestine.
The epithelium of the appendix is simple columnar epithelium, and
lymphatic nodules are located in the lamina propria of the mucosa,
which may extend into the submucosa. The muscularis externa
contains inner circular and outer longitudinal smooth muscles.
Figure 15-19B. Anorectal junction. H&E, 34; insets (left)
131, (right) 87
The junction between the rectum and the anal canal is called the
anorectal junction. The rectum connects the sigmoid colon to the anal
canal. The rectum is the distalmost portion of the large intestine and
functions mainly to store feces until elimination. The mucosa of the
rectum is similar to that of the colon, but it has fewer intestinal glands
of Lieberkühn. The anal canal is a continuation of the large intes-
tine and has longitudinal folds (anal columns) in the gross view. The
mucosa of the anal canal is covered by stratifi ed squamous epithe-
lium. The lamina propria contains many large veins (venous plexus).
The muscularis mucosae is visible here. The muscularis externa con-
tains inner circular and outer longitudinal smooth muscle layers (not
shown here). The inner circular smooth muscle becomes thicker and
forms the internal anal sphincter. The external anal sphincter sur-
rounds the anal canal. It is a thick layer of skeletal muscle that vol-
untarily controls the elimination of feces. On the left in the photomi-
crograph is the distal end of the rectum; on the right is the proximal
portion of the anal canal. Sebaceous glands and apocrine glands may
be found in the distal end of the anal canal.
CLINICAL CORRELATION
Figure 15-19C.
Hemorrhoids. H&E, 19
Hemorrhoids are swollen, infl amed
veins in the anal region deep
in the anal mucosa and are classifi ed as internal hemorrhoids and
external hemorrhoids, based on whether the hemorrhoids are
above (internal) or below (external) the anorectal (line) junction
(dentate/pectinate line). Causes include repeated pregnancy, con-
stipation, and portal hypertension. Common symptoms include
bleeding, itching, and pain. Pathologically, hemorrhoids are thin-
walled varicose veins that extend into the submucosal layer. In time,
thrombosis (clotting) may occur with resultant infarct and fi ssure
formation. Treatments include surgical removal of hemorrhoids,
coagulation therapy, and a procedure in which a rubber band is
used to tie off the hemorrhoids. This photomicrograph shows anal
squamous mucosa with underlying dilated anorectal veins.
Appendicitis usually results from a bacterial infection and may
develop slowly or acutely. A cardinal sign is pain in the lower
right abdominal quadrant or when pressure is applied to the
Mc Burney point. The most common treatment is surgical exci-
sion of the appendix.
Dilated
anorectal
vein
C
CUI_Chap15.indd 301 6/2/2010 3:25:04 PM
302
UNIT 3
■
Organ Systems
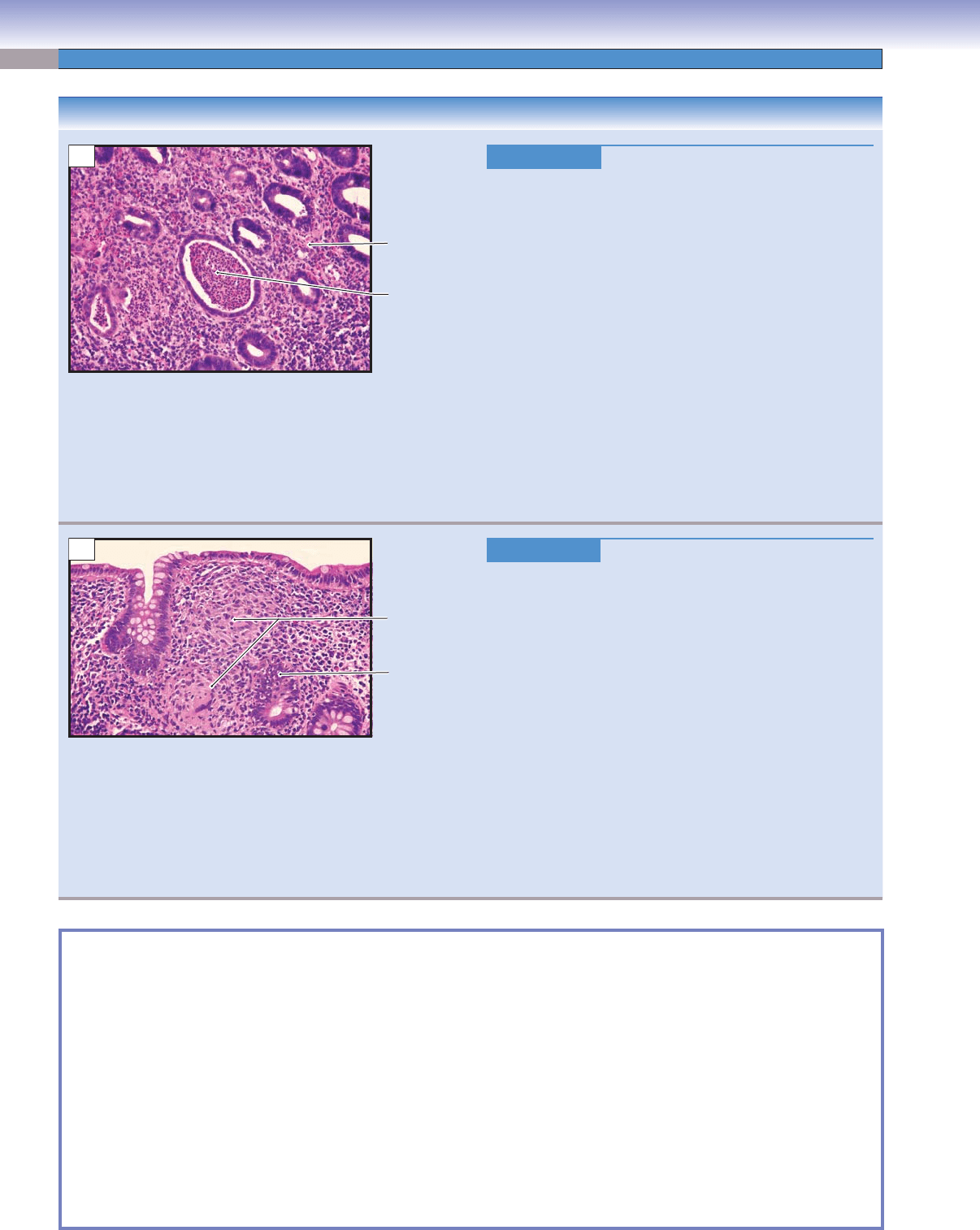
Figure 15-20A. Ulcerative Colitis. H&E, 97
Ulcerative colitis is an infl ammatory bowel disease
that causes ulcers in the lining of the colon and rectum
characterized by intermittent exacerbations alternating with
complete symptomatic remission. Major symptoms include
abdominal pain, diarrhea, anemia, weight loss, bleeding
from the rectum, and passage of mucus. Pathologically, the
infl ammation is predominantly confi ned to the mucosa and
submucosa in contrast to Crohn disease, which is transmu-
ral. Grossly, ulcerative colitis produces shallow ulcers and
pseudopolyps. Histologic features include acute and chronic
colitis, crypt abscesses, atrophy of glands, and loss of mucin
in goblet cells. Treatment includes anti-infl ammatory drugs
and immunosuppressants to control the symptoms and
achieve remission. The risk for the development of adeno-
carcinoma is high in patients with ulcerative colitis, so sur-
veillance colonoscopy with biopsy is necessary to detect
early dysplasia of the glandular epithelium. Surgical removal
of the colon is necessary in severe refractory cases or in cases
where severe dysplasia or adenocarcinoma is detected.
Figure 15-20B. Crohn Disease. H&E, 97
Crohn disease is a chronic autoimmune infl ammatory disease
of the gastrointestinal tract that may affect any location, from
the oral cavity to the anus, but mostly involves the distal
small intestine and colon. Crohn disease is characterized by
asymmetric and segmental infl ammation extending through
the intestinal wall (transmural) from the mucosa to the
serosa. Crohn disease characteristically involves areas of the
bowel separated by intervening uninvolved areas or “skip”
lesions. Symptoms include abdominal pain, diarrhea, vom-
iting, and weight loss. Pathologic changes include mucosal
neutrophil and mononuclear cell infi ltration, ulceration,
mucosal fi ssures, fi stulae, serosal adhesions, abscesses, pseu-
dopolyps, and noncaseating granulomas. Treatment focuses
on relieving symptoms through immunosuppressive agents
to prevent relapse and complications. This image shows
colonic mucosa with depletion of goblet cells, noncaseating
granulomas within the lamina propria, chronic infl amma-
tion, and neutrophils invading the crypt cells.
Intestinal metaplasia
■ : the reversible change of one mature type of epithelium to an intestinal type epithelium; may be seen
in chronic gastritis when goblet cells are present within the gastric mucosa; considered a risk factor for the development of
gastric adenocarcinoma (Fig. 15-8B).
Dyspepsia
■ : general term for abdominal pain or indigestion associated with the intake of food (Fig. 15-10C).
Gastric metaplasia
■ : the reversible change of one mature type of epithelium to a gastric type epithelium; seen in peptic
duodenitis when the normal epithelial lining with goblet cells is replaced with a gastric foveolar–type mucosa in response
to exposure to increased levels of stomach acid (Fig. 15-10C).
Pseudopolyp
■ : found in cases of chronic infl ammatory bowel disease; consists of polypoid mounds of mucosa created by
regenerating glandular epithelium; not considered true polyps, hence the name (Figs. 15-18A and 15-20A,B).
Crypt abscess
■ : an aggregate of neutrophils present within a colon crypt, usually associated with infl ammatory bowel
disease, particularly ulcerative colitis (Fig. 15-20A).
Cryptitis
■ : an indicator of acute colitis; appreciated histologically by the infi ltration of neutrophils with the crypt cells of
the colon (Fig. 15-20B).
SYNOPSIS 15-1 Pathological and Clinical Terms for the Digestive Tract
CLINICAL CORRELATIONS
Crypt
abscess
Acute and
chronic
inflammation
A
Cryptitis
Noncaseating
granulomas
B
CUI_Chap15.indd 302 6/2/2010 3:25:10 PM
CHAPTER 15
■
Digestive Tract
303
Regions Mucosa (Epithelium,
Lamina Propria,
Muscularis Mucosae)
Submucosa
(Submucosal
Plexuses Present
in this Layer)
Muscularis Externa
(Myenteric Plexuses
Present between
Smooth Muscle Layers)
Serosa/
Adventitia
Main Functions
Esophagus
Upper
esophagus
Nonkeratinized stratifi ed
squamous
Esophageal glands Inner circular and outer
longitudinal skeletal
muscles
Adventitia Transport food bolus
Middle
esophagus
Nonkeratinized stratifi ed
squamous
Esophageal glands Inner circular and outer
longitudinal mixed skeletal
and smooth muscles
Adventitia Transport food bolus
Lower
esophagus
Nonkeratinized stratifi ed
squamous; esophageal
cardiac glands in lamina
propria
Esophageal glands Inner circular and outer
longitudinal skeletal
muscles
Serosa Transport food bolus
Stomach (Rugae and Gastric Pits)
Cardia Surface mucous cells
and gastric pits; mucus-
secreting cells of cardiac
glands in lamina propria
No glands Inner oblique, middle
circular, and outer
longitudinal smooth
muscles
Serosa Add mucus and
lysozyme; churn food
by peristalsis
Fundus and
body
Surface lining cells and
gastric pits; parietal
and chief cells of gastric
glands in lamina propria
No glands Inner oblique, middle
circular, and outer
longitudinal smooth
muscles
Serosa Same as above; add
acidic gastric juice (e.g.,
HCl, mucus, enzymes);
process food into chyme
Pylorus Surface lining cells and
gastric pits; mucus-
secreting cells of pyloric
glands in lamina propria
No glands Inner oblique, middle
circular, and outer
longitudinal smooth
muscles
Serosa Add mucus; churn
food and pass chyme to
duodenum
Small Intestine (Villi and Crypts)
Duodenum Columnar absorptive
and goblet cells; Paneth,
enteroendocrine, goblet,
and absorptive cells in
glands (crypts) of Lieberkühn
Brunner glands Inner circular and outer
longitudinal smooth
muscles
Serosa/
adventitia
Allow bile and pancreatic
juice to enter small
intestine; release mucus;
regulate rate of emptying
of stomach; absorption
Jejunum Similar to above No glands Inner circular and outer
longitudinal smooth
muscles
Serosa Absorption of
carbohydrates, proteins,
lipids, and vitamin K
Ileum Similar to above with
increased goblet cells; Peyer
patches in lamina propria
Peyer patches may
extend into this
layer
Inner circular and outer
longitudinal smooth
muscles
Serosa Similar to above;
absorption of vitamins
K and B12 and bile salts
Large Intestine (Crypts, no Villi)
Cecum/colon Goblet cells and
columnar absorptive
cells; goblet, columnar,
and enteroendocrine cells
in glands of Lieberkühn
No glands Inner circular smooth
muscle; outer longitudinal
smooth muscle layer forms
three teniae coli
Serosa/
adventitia
Absorption of water
and electrolytes;
formation of feces
Rectum
Similar to above; fewer
glands of Lieberkühn
No glands Inner circular and outer
longitudinal smooth
muscles
Adventitia Store feces; sensory
receptors signal brain of
the need to evacuate
Anal canal Nonkeratinized to
keratinized stratifi ed
squamous
Sebaceous glands
(distal portion);
venous
Inner circular (thickened to
become internal sphincter)
and thin outer longitudinal
smooth muscles
Adventitia Internal sphincter and
external sphincter
(skeletal muscle); relax
to release feces
TABLE 15-1 Digestive Tract
Note: Simple columnar epithelium lines most of the digestive tract, including the stomach and the small and large intestines. It does not line the
esophagus and the anal canal, however.
CUI_Chap15.indd 303 6/2/2010 3:25:12 PM
304
Introduction and Key Concepts for the Digestive Glands and Associated Organs
Figure 16-1 Overview of the Digestive Glands and Associated Organs
Figure 16-2 Orientation of Detailed Digestive Glands and Associated Organs Illustrations
Salivary Glands
Figure 16-3A General Structure of the Major Salivary Glands
Figure 16-3B Parotid Gland
Figure 16-4A Parotid Glands
Figure 16-4B Clinical Correlation: Pleomorphic Adenoma
Figure 16-4C Clinical Correlation: Parotid Cyst
Figure 16-5A Submandibular Glands
Figure 16-5B Serous Acinus, Submandibular Gland
Figure 16-6A Mucous Acinus, Submandibular Gland
Figure 16-6B Clinical Correlation: Squamous Cell Carcinoma of the Tongue
Figure 16-7A Striated Duct, Submandibular Gland
Figure 16-7B Intralobular Duct, Submandibular Gland
Figure 16-8A,B Sublingual Glands
Figure 16-8C Clinical Correlation: Sialadenitis
Pancreas
Figure 16-9A A Representation of the Exocrine Pancreatic Duct System
Figure 16-9B Exocrine and Endocrine Pancreas
Figure 16-9C Clinical Correlation: Acute Pancreatitis
Figure 16-10A Pancreatic Acinar Cells
Figure 16-10B Centroacinar Cells, Pancreas
Liver
Figure 16-11 General Structure of the Liver
Synopsis 16-1 Functions of the Liver
Digestive Glands
and Associated
Organs
16
CUI_Chap16.indd 304 6/2/2010 6:42:10 PM