Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

THE USE OF ANTISEPTICS IN PERIODONTAL THERAPY •
465
feature of periodontal disease management for almost
a century (for reviews see Fischman 1992, 1997). The
consensus appears to be that the use of preventive
agents should be as adjuncts and not replacements for
the more conventional and accepted effective me-
chanical methods and only then when these appear
partially or totally ineffective alone.
Mechanical tooth cleaning through toothbrushing
with toothpaste is arguably the most common and
potentially effective form of oral hygiene practiced by
peoples in developed countries (for reviews see
Frandsen 1986, Jepsen 1998); although,
per capita in
the
world, wood sticks are probably more commonly
used.
Interdental cleaning is a secondary adjunct and
would
seem particularly important in individuals who,
through the presence of disease, can be
retrospectively assessed as susceptible (for reviews
see Hancock 1996, World Workshop on Periodontics
1996a, Kinane 1998). Unfortunately, it is a fact of life
that a significant proportion of all individuals fail to
practice a high enough standard of plaque removal
such that gingivitis is highly prevalent and from an
early age (Laystedt et al. 1982, Addy et al. 1986). This,
presumably, arises either or both from a failure to
comply with the recommendation to regularly clean
teeth or lack of dexterity with tooth cleaning habits (
Frandsen 1986). Certainly, many individuals remove
only around half of the plaque from their teeth even
when brushing for 2 minutes (de la Rosa 1979). Pre-
sumably this occurs because certain tooth surfaces
receive little or no attention during the brushing cycle
(
Rugg-Gunn & MacGregor 1978, MacGregor & Rugg-
Gunn 1979). The adjunctive use of chemicals would
therefore appear a way of overcoming deficiencies in
mechanical tooth cleaning habits as practiced by
many individuals. This chapter will consider the past
and present status and success of chemical suprag-
ingival plaque control to the prevention of gingivitis
and thereby periodontitis. Since chemical agents are
usually considered as adjuncts, some aspects of me-
chanical plaque control will be considered.
Supragingival plaque control
The formation of plaque on a tooth surface is a dy-
namic and ordered process, commencing with the
attachment of primary plaque forming bacteria. The
attachment of these organisms appears essential for
initiating the sequence of attachment of other organ-
isms such that, with time, the mass and complexity of
the plaque increases (see Chapter 3). Left undisturbed,
supragingival plaque reaches a quantitative and
qualitative level of bacterial complexity that is incom-
patible with gingival health, and gingitivis ensues.
Even though, as yet, the microbiology of gingivitis is
poorly understood, the sequencing of plaque forma-
tion highlights how interventions may prevent the
development of gingivitis. Thus, any method of
plaque
control which prevents plaque achieving the
critical point where gingival health deteriorates, will
stop gingivitis. Unfortunately, the lack of knowledge
of bacterial specificity for gingivitis does not allow
targeting of the control of particular organisms except
for perhaps the primary plaque formers. Plaque inhi-
bition has, therefore, targeted plaque formation at
particular points – bacterial attachment, bacterial pro
-
liferation and plaque maturation – and these will be
discussed in more detail in the later section "Ap-
proaches to chemical supragingival plaque control".
The mainstay of supragingival plaque control has
been regular plaque removal using mechanical meth-
ods which, in developed countries, means the tooth-
brush, manual or electric, and in less well developed
countries the use of wood or chewing sticks (for re-
view see Frandsen 1986, Hancock 1996). These devices
primarily access smooth surface plaque and not inter
-
dental deposits. Interdental cleaning devices include
wood sticks, floss, tape, interdental brushes and, more
recently, electric interdental devices (for review see
Egelberg & Claffey 1998, Kinane 1998). Regular me-
chanical tooth cleaning is directed towards maintain-
ing a level of plaque, quantitatively and/or qualita-
tively, which is compatible with gingival health, and
not rendering the tooth surface bacteria free. Theoreti
-
cally, mechanical cleaning of teeth could prevent car-
ies but workshops have concluded that tooth brush-
ing
per se
and interdental cleaning as performed by the
individual do not prevent caries (for review see Frand-
sen 1986). Clearly, but outside the scope of this chapter,
the toothbrush and other mechanical devices do pro-
vide a vehicle whereby anticaries agents, such as fluo
-
ride, can be delivered to the tooth surface. Under the
conditions of clinical experimentation, tooth cleaning
performed once every two days was shown to prevent
gingivitis (Lang et al. 1973, Kelner et al. 1974, McNabb
et al. 1992). However, the professional recommenda-
tion has been to brush twice per day, for which there
is evidence of a benefit to gingival health over less
frequent cleaning with no additional benefit for more
frequent brushing (for review see Frandsen 1986). The
duration of brushing is somewhat controversial given
that most surveys or studies reveal average brushing
time of 60 s or less (Rugg-Gunn & MacGregor 1978,
MacGregor & Rugg-Gunn 1979). However, it is worth
noting that one study showed less than 50% plaque
removal after 2 minutes brushing (de la Rosa 1979).
This perhaps highlights that many individuals spend
little or no time during the brushing cycle at some
tooth surfaces, notably lingually (Rugg-Gunn &
MacGregor 1978, MacGregor & Rugg-Gunn 1979).
Oral hygiene, oral hygiene instruction and the ef-
fect of supragingival plaque control alone on sub-
gingival plaque and therefore periodontal disease are
the subject of other chapters. Nevertheless, some fur-
ther comments on mechanical tooth cleaning are per-
tinent in this chapter, particularly in respect of com-
parative efficacy of devices. The manual toothbrush
as known today – man-made filaments in a plastic
head –was invented as recently as the 1920s. Evidence
466 • CHAPTER 22
for such devices dates back to China approximately
1000 years ago, re-emerging in the 1800s in Europe,
but too expensive for common usage (for reviews see
Fischman 1992, 1997). Numerous changes in manual
toothbrush design have occurred, particularly re-
cently, and similarly numerous claims have been
made for the efficacy of individual designs. Despite
this, researchers, workshop reports and consensus
views have repeatedly concluded that there is no best
design of manual toothbrush nor an optimal method
of tooth cleaning, the major variable being the person
using the brush (for reviews see Frandsen 1986, Jepsen
1998). Limited evidence is available comparing the
modern toothbrush with chewing sticks but what is
available suggests similar efficacy (Norton & Addy
1989), perhaps not surprisingly if indeed the user is
the important factor. Interdental cleaning is consid-
ered important particularly for those individuals who
are known to be susceptible to or have periodontal
disease (for reviews see Egelberg & Claffey 1998, Ki-
nane 1998,). Here again, there is little evidence sup-
porting one interdental cleaning method over another,
leaving patients and professionals to hold subjectively
related preferences (for review see Kinane 1998). Elec
-
tric toothbrushes of the counter rotation type found
prominence for a short time in the 1960s and 1970s
but
were unreliable and proven of no greater efficacy
over
manual brushes, except for handicapped
individuals
(for reviews see Frandsen 1986). More
recently, ranges
of new electric brushes have appeared
with a variety
of head, tuft and filament actions. For
these, consensus
reports conclude that there is
evidence for greater
efficacy over manual brushes
particularly when pro
fessional advice in their use is
provided (for reviews see Hancock 1996, World
Workshop on Periodontics 1996a, Egelberg & Claffey
1998, van der Weijden et al.
1998). There is, at this
time, no evidence for concern
over potential harmful
effects to hard and soft tissues
because the force
applied to electric brushes tends to
be less than with
manual brushes (for review see van
der Weijden et al.
1998). Finally, there is no evidence
that any one
electric toothbrush design is superior and, again, the
user appears the major variable.
Chemical supragingival plaque control
History of oral hygiene products
The terminology "oral hygiene products" is recent but
there is evidence dating back at least 6000 years that
formulations and recipes existed to benefit oral and
dental health (for reviews see Fischman 1992, 1997).
This includes the written Ebers Papyrus 1500 BC con
-
taining recipes for tooth powders and mouthrinses
dating back to 4000 BC. A considerable number of
formulations can be attributed to the writer and scien
-
tist Hippocrates (circa 480 BC). By today's standards
the early formulations appear strange if not disgust-
ing but they were not always without logic. Thus,
bodies or body parts of animals perceived to have
good or continuously erupting teeth were used in the
belief that they would impart health and strength to
the teeth of the user. Hippocrates, for example, recom
-
mended the head of one hare and three whole mice,
after taking out the intestines of two, mixing the pow-
der derived from burning the animals with greasy
wool, honey, anise seeds, myrrh and white wine. This
early toothpaste was to be rubbed on the teeth fre-
quently.
Mouthrinses similarly contained ingredients which
would have had some salivary flow stimulating effect,
breath odor masking and antimicrobial actions, albeit
not necessarily formulated with all these activities in
mind. Alcohol-based mouthrinses were particularly
popular with the Romans and included white wine
and beer. Urine, as a mouthrinse, appeared to be popu
-
lar with many peoples and over many centuries. There
even appeared differences in opinion, with the Cant-
abri and other peoples of Spain preferring stale urine,
whereas Fauchard (1690-1761) in France recom-
mended fresh urine. The Arab nations were purported
to prefer children's urine and the Romans to prefer
Arab urine. Anecdotal reports suggest the use of urine
as a mouthrinse to this very day with individuals
rinsing with their own urine. There could, indeed, be
benefits to oral health from rinsing with urine by
virtue of the urea content; however this has never been
evaluated, and given today's Guidelines for Good
Clinical Practice, it is unlikely that study protocols
would receive ethical approval.
Throughout the centuries, most tooth powders,
toothpastes and mouthrinses appear to have been
formulated for cosmetic reasons including tooth
cleaning and breath freshening rather than the control
of dental and periodontal diseases. Many formula-
tions contain very abrasive ingredients and/or acidic
substances. However, ingredients with antimicrobial
properties were used, perhaps not intentionally, and
included arsenic and herbal materials. Herbal extracts
are, perhaps, increasingly being used in toothpastes
and mouthrinses, although there are little data to sup
-
port efficacy for gingivitis and none for caries. Many
agents prescribed well into the twentieth century, usu
-
ally as rinses, had the potential to cause local damage
to tissues, if not systemic toxicity, including aromatic
sulfuric acid, mercuric perchloride, carbolic acid and
formaldehyde (Dilling & Hallam 1936).
Perhaps the biggest change to toothpastes came
with the chemo-parasitic theory of tooth decay of W.
D. Miller in 1890. The theory that organic acids were
produced by oral bacteria acting on fermentable car-
bohydrates in contact with enamel led to both the
introduction of agents into toothpaste, which might
influence this process, and the production of alkaline
products. Shortly after, and at the beginning of the
twentieth century, various potassium and sodium
salts were added to toothpaste as a therapy for peri-
odontal disease. The first half of the twentieth century
saw numerous claims for toothpastes for oral health
benefits, including tooth decay and periodontal dis-
THE USE OF ANTISEPTICS IN PERIODONTAL THERAPY • 467
ease. For example, with the early recognition that
periodontal diseases were associated with microor-
ganisms, emetin hydrochloride was added to tooth-
paste to treat possible amoebic infections. Perhaps
with the exception of the well-known essential oil
mouthrinse marketed at the end of the nineteenth
century, the addition of antimicrobial and/or antisep
-
tic agents to toothpastes and mouthrinses is a rela-
tively recent practice by manufacturers. During the
nineteenth and twentieth centuries, toothpastes also
became less abrasive. Interestingly, the importance of
a
level of abrasivity in toothpastes to the prevention
of
extrinsic dental stain became apparent when one
manufacturer marketed a non-abrasive liquid denti-
frice. The unsightly brown tooth staining that devel-
oped in many users resulted in the early removal of
this product from the marketplace. More recently also,
standards organizations, notably the British Stand-
ards Institute and the International Standards Organi
-
zation, have laid down standards for toothpastes (BS
5136: 1981, ISO 11609: 1995) and a standard for
mouthrinses is under development. Such standards
are concerned with safety rather than efficacy.
Throughout the ages, and until relatively recently,
scientific evaluations of agents and formulations for
gum health were not performed and claims for effi-
cacy appear based on anecdotal reports at best. In-
deed, given the nature of many ingredients and the
recipes recommended in the past for oral hygiene
benefits, it is unlikely that efficacy will ever be tested.
In the 6000 years history of oral hygiene products,
scientific evaluation must be seen as an extremely
recent event – an observation which can, of course, be
applied to almost all aspects of chemo-prevention and
chemo-therapy of human diseases. Indeed, perhaps
the first ever, double-blind, randomized cross-over
design clinical trial in dentistry was just over 40 years
ago (Cooke & Armitage 1960).
Rationale for chemical supragingival plaque
control
The epidemiological data and clinical research (Ash et
al. 1964, Loe et al. 1965) directly associating plaque
with gingivitis perhaps, unfortunately, led to a rather
simplistic view that regular tooth cleaning would pre-
vent gingivitis and thereby periodontal disease. Theo-
retically correct, this concept did not appear to con-
sider the multiplicity of factors which influence the
ability of individuals to clean their teeth sufficiently
well to prevent disease, not the least of which are those
factors which affect individual compliance with ad-
vice and dexterity in performing such tasks. The need
for research into those psychosocial factors which
might influence attitude to and performance in oral
hygiene, was stated in a workshop report on plaque
control and oral hygiene practices (Frandsen 1986) but
appears not to have been heeded to this day. Moreover,
and as described in other chapters, epidemiological
data suggest that not all individuals are particularly
susceptible to periodontal disease. The most severe
disease is accounted for by a relatively small propor-
tion of any population and then by only a proportion
of sites in their dentition (Baelum et al. 1986). Even
accepting that a considerable proportion of middle-
aged adults will have one or more sites in the dentition
with moderate periodontal disease, this will be of the
chronic adult type and a minimal threat to the longev
-
ity of their dentition (Papapanou 1994). This requires
that prevention, through improved oral hygiene prac-
tices, will be grossly overprescribed.
Given our knowledge concerning the microbiologi-
cal specificity of periodontal disease and, more par-
ticularly host susceptibility to the disease, it is at
present difficult, if not impossible, to predict probable
future disease in the, as yet unaffected, host. At pre-
sent, host susceptibility is described retrospectively in
the already diseased individual but, even here, an
explanation for their susceptibility, except for a few
risk factors, cannot be made. These risk factors include
smoking, diabetes and polymorph defects and possi-
ble stress (for review see Johnson 1994, Porter & Scully
1994). Genetic markers for periodontal disease have
been identified but, at present, appear to be applied
retrospectively rather than prospectively (Kornman et
al. 1997) and the value to early onset disease has been
questioned (Hodge et al. 2001).
One definition of periodontal disease is chronic
gingivitis with loss of attachment. This is a particu-
larly useful definition since not only does it describe
the pathogenic processes occurring but also alludes to
the approach to prevent, treat or prevent re-occur-
rence of the disease. Therefore prevention through
supragingival plaque control still remains the main-
stay of controlling gingivitis and therefore the occur-
rence or re-occurrence of periodontitis (for review see
Addy & Adriaens 1998). As alluded to, the importance
of oral hygiene to outcome and long-term success of
therapy for periodontal disease is hampered by the
often ineffectiveness of mechanical cleaning to spe-
cific sites using a toothbrush and the limited or lack of
use of interdental cleaning by many individuals (for
reviews see Axelsson 1994). Despite the encouraging
improvements in oral hygiene, gingivitis and, to some
extent, periodontitis in developed countries, gingival
inflammation is still highly prevalent (for reviews see
Baehni & Bourgeois 1998). Taken with the microbial
etiology of both gingivitis and periodontitis, this sup-
ports the concept of employing agents to control
plaque which require minimal compliance and skill in
their use. This is the concept that underlies chemical
supragingival plaque control, but as with oral hygiene
instruction in mechanical methods, it will have to be
vastly overprescribed if periodontal disease preven-
tion is to be achieved in susceptible individuals.
Chemical supragingival plaque control has thus been
the subject of extensive research using scientific meth
-
odologies for approximately 40 years. The question to
be addressed here is whether a chemical or chemicals
468 • CHAPTER 22
have been discovered and proven efficacious in,
firstly, the prevention of gingivitis and, secondly, pe-
riodontitis.
Conclusions
•
Gingivitis and periodontitis are highly prevalent
diseases and prevention of occurrence or re-occur
-
rence is dependent on supragingival plaque control.
•
Tooth cleaning is largely influenced by the compli-
ance and dexterity of the individual and little by
design features of oral hygiene appliances and aids.
•
The concept of chemical plaque control may be
justified as a means of overcoming inadequacies of
mechanical cleaning.
•
Gingivitis is highly prevalent and from a young age
in all populations, but the proportion of individuals
susceptible to tooth loss through periodontal dis-
ease is small.
•
Prediction of susceptibility to periodontal disease
from an early age is at present impossible.
•
Mechanical and/or chemical supragingival plaque
control measures for prevention of periodontitis
will have to be greatly overprescribed.
Approaches to chemical supragingival
plaque control
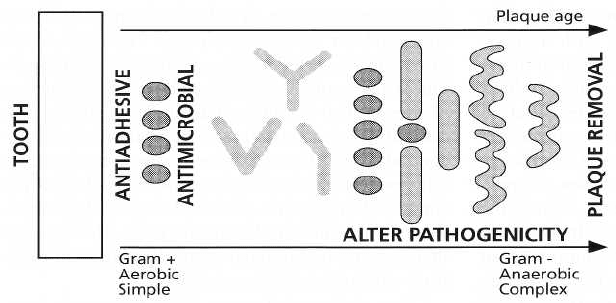
The well-ordered and dynamic process of plaque for-
mation as described previously and in other chapters,
can be summarized in Fig. 22-1. It is apparent that this
process can be interrupted, interfered with, reversed
or modified at several points and before the plaque
mass and/or complexity reaches a level whereby gin-
gival health deteriorates. Mechanical cleaning aims to
regularly remove sufficient microorganisms to leave a
"
healthy plaque" present, which cannot induce gingi-
val inflammation. Chemical agents, on the other hand,
could influence plaque quantitatively and qualita-
tively via a number of processes and these are sum-
marized in Fig. 22-1. The action of the chemicals could
fit into four categories:
1.
Antiadhesive
2.
Antimicrobial
Fig. 22-1. Bacterial succession
plaque formation. There is increas
-
ing mass and bacterial complexity
as plaque bacteria attach and pro
-
liferate. Ideal sites of action for
chemicals which might influence
plaque accumulation are shown.
Acknowledgement to Dr William
Wade for permission to publish
this diagram.
3.
Plaque removal
4.
Antipathogenic
Antiadhesive agents
Antiadhesive agents would act at the pellicle surface
to prevent the initial attachment of the primary plaque
forming bacteria. Such antiadhesive agents would
probably have to be totally preventive in their effects,
acting most effectively on an initially clean tooth sur-
face. Antiadhesive agents do exist and are used in
industry, domestically and in the environment. Such
chemicals prevent the attachment and development
of a variety of biofilms and are usually described as
antifouling agents. Unfortunately the chemicals
found in such applications are either too toxic for oral
use or ineffective against dental bacteria plaques.
Nevertheless, the concept of antiadhesives continues
to attract research interest (Moran et al. 1995, for re-
view see Wade & Slayne 1997). To date, effective for-
mulations or products with antiadhesive properties
are not available to the general public, although the
amine alcohol, delmopinol, which appears to interfere
with bacterial matrix formation and therefore fits
somewhere between the concepts of antiadhesion and
plaque removal, has been shown effective against
plaque and gingivitis (Collaert et al. 1992, Claydon et
al. 1996). Were antiadhesive agents to be discovered,
a
secondary benefit to extrinsic stain prevention of
teeth may be expected (Addy et al. 1995a).
Antimicrobial agents
The bacterial nature of dental plaque, not surprisingly,
attracted interest in prevention of plaque formation
through the use of antimicrobial agents. Antimicrobial
agents could inhibit plaque formation through one of
two mechanisms alone or combined. The first would
be the inhibition of bacterial proliferation and would
be directed, as with antiadhesive agents, at the pri-
mary plaque forming bacteria. Antimicrobial agents
therefore could exert their effects either at the pellicle
coated tooth surface before the primary plaque form-
ers attach or after attachment but before division of
these bacteria. This plaque inhibitory effect would be
bacteriostatic in type, with the result that the lack of
bacterial proliferation would not allow attachment of
THE USE OF ANTISEPTICS IN PERIODONTAL THERAPY • 4
6
9
subsequent bacterial types on to the primary plaque
forming bacteria. The second effect could be bacte-
riocidal whereby the antimicrobial agent destroys all
of the microorganisms either attaching or already at-
tached to the tooth surface. Many antimicrobial agents
exist which could produce this effect; however, as will
be discussed, to be effective in inhibiting plaque, the
bacteriocidal effect would have to be absolute or per-
sistent. If not, other bacteria within the oral environ-
ment would colonize the tooth surface immediately
following the loss of the bacteriocidal effect and the
biofilm would be re-established. For the most part
biofilms in themselves are fairly resistant to total bac-
teriocidal effects of antimicrobial agents and, thus far,
there does not appear to have been any agent discov-
ered which effectively would sterilize the tooth sur-
face after each application. If such an agent were
found it could, of course, have potentially dangerous
implications for the oral cavity since it would almost
certainly destroy most of the commensal bacteria
which normal colonize the oral cavity. This would
open up the potential for exogenous microorganisms,
with dangerous pathogenic potential, colonizing the
oral cavity. In the event, it is probable that antimicro-
bial agents exert both a bacteriocidal effect followed
by a bacteriostatic action of variable duration. The
bactertiocidal effect will occur when the antimicrobial
agent is at high concentration within the oral cavity
and usually this will represent the time when the
formulation is actually within the oral cavity. The
bacteriocidal effect would be expected to be lost very
soon after expectoration.
As will be discussed in respect of chlorhexidine, it
is almost certainly the persistence of the bacteriostatic
action of antimicrobial agents which accounts for their
plaque inhibitory activity. Calculations by Stralfors
(
1961) indicated that plaque inhibition through a bac
-
teriocidal effect would require the immediate killing
of
99.9% of the oral bacteria to effect a plaque inhibi-
tory action of significant duration. Antimicrobial
agents for plaque inhibition, to date, are the only
agents that have found common usage in oral hygiene
products. The efficacy of these agents and products
varies at the extremes (for reviews see Addy 1986,
Kornman 1986, Mandel 1988, Addy et al. 1994, Addy
& Renton-Harper 1996a, Rolla et al. 1997).
Plaque removal agents
The idea of employing a chemical agent which would
act in an identical manner to a toothbrush and remove
bacteria from the tooth surface, is an attractive propo
-
sition. Such an agent, contained in a mouthrinse,
would be expected to reach all tooth surfaces and
thereby be totally effective. For this reason, the idea of
chemical plaque removal agents has attracted the ter
-
minology of "the chemical toothbrush". As with an-
tiadhesives, there are potentially agents, such as the
hypochlorites, which might be expected to remove
bacterial deposits and are commonly employed within
the domestic environment. Again, such chemi-
cals would be potentially toxic were they to be applied
within the oral cavity. Perhaps the nearest success was
with enzymes directed at both the pellicle, e.g. pro-
teases, or the bacterial matrices, e.g. dextranase and
mutanase (for review see Kornman 1986). Again, as
will be discussed, these enzymes, albeit potentially
effective, lacked substantivity within the oral cavity.
Antipathogenic
agents
It is theoretically possible that an agent could have an
effect on plaque microorganisms, which might inhibit
the expression of their pathogenicity without neces-
sarily destroying the microorganisms. In some re-
spects antimicrobial agents, which exert a bacte-
riostatic effect, achieve such results. At present the
understanding of the pathogenesis of gingivitis is so
poor that this approach has received no attention.
Were our knowledge on the microbial etiology of gin-
givitis to improve, clearly there exists the possibility
of an alternative, but related, approach: the introduc-
tion into the oral cavity of organisms which have been
modified to remove their pathogenic potential to the
gingival tissues. This is not a new concept and was an
approach experimented with to replace pathogenic
staphylococci within the nasal cavities of surgeons
with the idea of reducing the potential for wound
infection caused by the operator. At present such an
approach within the oral cavity for either gingivitis or
caries is perhaps within the realms of science fiction.
Conclusions
•
At present most antiplaque agents are
antimicrobial
and prevent the bacterial
proliferation phase of
plaque development.
•
Plaque formation could be controlled by antiadhe-
sive or plaque removal agents, but these are not, as
yet, available or safe for oral use.
•
Alteration of bacterial plaque pathogenicity through
chemical agents or bacterial modification would
require a greater understanding of the bacterial eti-
ology of gingivitis.
Vehicles for the delivery of chemical agents
The carriage of chemical agents into the mouth for
supragingival plaque control has involved a small but
varied range of vehicles (for reviews see Addy 1994,
Cummins 1997).
Toothpaste
By virtue of common usage the ideal vehicle for the
carriage of plaque control agents is toothpaste. Anum
-
ber of ingredients go to make up toothpaste and each
has a role in either influencing the consistency and
stability of the product or its function (for reviews see
Davis 1980, Forward et al. 1997).
The major ingredients may be classified under the
following headings:
470 • CHAPTER 22
1. Abrasives,
such as silica, alumina, dicalcium phos-
phate and calcium carbonate either alone, or more
usually today, in combination. Abrasives affect the
consistency of the toothpaste and assist in the con
-
trol of extrinsic dental staining.
2. Detergents:
the most common detergent used in
toothpaste is sodium lauryl sulfate, which imparts
the foaming and "feel" properties to the product.
Additionally, detergents may help dissolve active
ingredients and the anionic detergent sodium lau-
ryl sulfate has both antimicrobial and plaque in-
hibitory properties (Moran et al. 1988, Jenkins et al.
1991a,b). Certain toothpaste products cannot em-
ploy anionic detergents as they interact with cat-
ionic substances that may be added to the product
such as chlorhexidine or polyvalent metal salts
such as strontium used in the treatment of dentine
hypersensitivity.
3. Thickeners,
such as silica and gums.
4. Sweeteners,
including saccharine.
5. Huniectants,
notably glycerine and sorbitol to pre-
vent drying out of the paste once the tube has been
opened.
6. Flavors,
of which there are many but mint or pep-
permint are popular in the western world although
rarely found in toothpaste in the Indian subconti-
nent where herbal flavors are more popular.
7. Actives,
notably fluorides for caries prevention, but
for plaque control triclosan and stannous fluoride
have been the most common examples.
As stated, the addition of cationic antiseptics to tooth
-
pastes is difficult but chlorhexidine has been formu-
lated into toothpastes and shown to be effective
(
Gjermo & Rolla 1970, 1971, Yates et al. 1993, Sanz et
al. 1994).
Mouthrinses
Despite the ideal nature of the toothpaste vehicle,
most chemical plaque control agents have been evalu
-
ated and later formulated in the mouthrinse vehicle.
Mouthrinses vary in their constituents but are usually
considerably less complex than toothpastes. They can
be simple aqueous solutions, but the need for prod-
ucts, purchased by the general public, to be stable and
acceptable in taste usually requires the addition of
flavoring, coloring and preservatives such as sodium
benzoate. Anionic detergents are included in some
products but, again, cannot be formulated with cat-
ionic antiseptics such as cetylpyridinium chloride or
chlorhexidine (Barkvoll et al. 1989). Ethyl alcohol is
commonly used both to stabilize certain active ingre-
dients and to improve the shelf-life of the product.
Concerns over the possible association of alcohol in-
take and pharyngeal cancer have been extended to
include alcohol-containing mouthrinses. Whether
these concerns are scientifically valid has not been
established. Also, since at present there seems little
support for the long-term chronic use of mouthrinses
for gingival health benefits, when correctly prescribed
the risk from contained alcohol is probably minuscule.
This, however, does not obviate the possible risk from
self-prescription, the chronic use of mouthrinses, or
the ingestion of alcoholic mouthrinses by children.
The proportion of alcohol is usually less than 10% but
some rinses have in excess of 20% alcohol. Some
manufacturers are now producing alcohol-free
mouthrinses.
Spray
Spray delivery of chemical plaque control agents has
attracted both research interest and the development
of products by some manufacturers in some countries.
Sprays have the advantage of focusing delivery on the
required site. The dose is clearly reduced and for
antiseptics such as chlorhexidine this has taste advan
-
tages. When correctly applied chlorhexidine sprays
were as effective as mouthrinses for plaque inhibition
although there was no reduction in staining (Francis
et al. 1987a, Kalaga et al. 1989a). Chlorhexidine sprays
were found particularly useful for plaque control in
physically and mentally handicapped groups (Francis
et al. 1987a,b, Kalaga et al. 1989b).
Irrigators
Irrigators were designed to spray water, under pres-
sure, around the teeth. As such they only removed
debris, with little effect on plaque deposits (for review
see Frandsen 1986). Antiseptics and other chemical
plaque control agents, such as chlorhexidine, have
been added to the reservoir of such devices. A variety
of dilutions of chlorhexidine have been employed to
good effect (Lang & Raber 1981).
Chewing gum
Over a relatively short period there has been interest
in employing chewing gum to deliver a variety of
agents for oral health benefits. Also, there appear to be
significant benefits to dental health through the use of
sugar-free chewing gum. Unfortunately, chewing
gums alone appear to have little in the way of plaque
control benefits particularly at sites prone to gingivitis
(
Addy et al. 1982a). Nonetheless, the vehicle has been
used to deliver chemical agents such as chlorhexidine
and, when used as an adjunct to normal toothbrush-
ing, reduced plaque and gingivitis levels have been
shown (Ainamo & Etemadzadeh 1987, Ainamo et al.
1990, Smith et al. 1996).
Varnishes
Varnishes have been employed to deliver antiseptics
including chlorhexidine, but the purpose has been to
prevent root caries rather than as a reservoir for plaque
control throughout the mouth.
Conclusions
•
Many vehicles may be used to deliver antiplaque
agents but most information relates to mouthrinses
and toothpaste.
•
Toothpaste appears the most practical and cost ef-
THE USE OF ANTISEPTICS IN PERIODONTAL THERAPY • 47
1
fective method for chemical plaque control for most
individuals.
•
In formulating antiplaque agents into toothpaste,
potential inactivation by other ingredients must be
considered.
•
Minority groups, such as the handicapped, may
benefit from other delivery systems.
CHEMICAL PLAQUE CONTROL
AGENTS
Over a period of more than three decades there has
been quite intense interest in the use of chemical
agents to control supragingival plaque and thereby
gingivitis. The number and variation of chemical
agents evaluated are quite large but most have anti-
septic or antimicrobial actions and success has been
variable at the extreme. It is important to emphasize
that formulations based on antimicrobial agents pro-
vide a considerably greater preventive than therapeu-
tic action. The most effective agents inhibit the devel-
opment of plaque and gingivitis but are limited or
slow to affect established plaque and gingivitis. Were
they available, antiadhesive agents would similarly
be
expected to provide preventive rather than thera-
peutic effects, although plaque removal agents would
almost certainly provide both preventive and thera-
peutic actions. Chemical plaque control agents have
been the subject of many detailed reviews since 1980
(Hull 1980, Addy 1986, Kornman 1986, Mandel 1988,
Gjermo 1989, Addy et al. 1994, Heasman & Seymour
1994, Jackson 1997). Based on knowledge derived
from chlorhexidine, the most effective plaque inhibi-
tory agents in the antiseptic or antimicrobial group are
those showing persistence of action in the mouth
measured in hours. Such persistence of action, some
-
times termed substantivity (Kornman 1986), appears
dependent on several factors:
1.
Adsorption and prolonged retention on oral sur-
faces including, importantly, pellicle coated teeth.
2.
Maintenance of antimicrobial activity once ad-
sorbed primarily through a bacteriostatic action
against the primary plaque forming bacteria.
3.
Minimal or slow neutralization of antimicrobial
activity within the oral environment or slow
desorption from surfaces.
The latter concepts will be discussed later under chlor
-
hexidine.
Antimicrobial activity in
vitro
of antiseptics
per se is
not a reliable predictor of plaque inhibitory activity
in
vivo
(Gjermo et al. 1970, 1973). Early studies on a
number of antiseptics revealed similar antimicrobial
profiles but a large variation in clinical effects. For
example, compared to chlorhexidine, the cationic qua
-
ternary ammonium compound, cetylpyridinium
chloride, has a similar antimicrobial profile
in vitro
(Gjermo et al. 1970, 1973, Roberts & Addy, 1981) and
is initially adsorbed in the mouth to a considerably
greater extent (Bonesvoll & Gjermo 1978). However,
the persistence of action of cetylpyridinium chloride
is
much shorter than chlorhexidine (Schiott et al. 1970,
Roberts & Addy, 1981), and plaque inhibition consid-
erably less (for review see Mandel 1988). Several rea-
sons may explain these apparent anomalies, including
poor retention of cetylpyridinium chloride within the
oral cavity (Bonesvoll & Gjermo 1978), reduced activ-
ity once adsorbed, and neutralization in the oral envi-
ronment (Moran & Addy 1984), or a combination of
these factors. Attempts to improve efficacy of ce-
tylpyridinium chloride can, of course, include increas
-
ing the frequency of use, but this is likely to incur
compliance problems and side effects (Bonesvoll &
Gjermo 1978). Alternatively, substantivity could be
improved by combining antimicrobials or using
agents to increase the retention of antimicrobials (for
review see Cummins 1992, Gaffar et al. 1992). Individ
-
ual groups of compounds, together with the specific
agents within the group, are listed in Table 22-1 and
discussed under the following headings.
Antibiotics (for reviews see Addy 1986, Kornman 1986)
Despite evidence for efficacy in preventing caries and
gingivitis or resolving gingivitis, the opinion today is
that antibiotics should not be used either topically or
systemically as preventive agents against these dis-
eases. The risk-to-benefit ratio is high and even anti-
biotic use in the treatment of adult periodontitis is
open to debate (for reviews see Genco 1981, Slots &
Rams 1990, Addy & Renton-Harper 1996b and Chap
-
ter 23). Thus, antibiotics have their own specific side
effects not all of which can be avoided by topical
application. Perhaps of greatest importance is the de-
velopment of bacterial resistance within human popu
-
lations, for example the methycillin-resistant
Staphy-
lococcus
aureas
(MRSA), which causes serious and life-
threatening wound infections, particularly within
hospitalized patients.
Enzymes
(for reviews see Addy 1986)
Enzymes fall into two groups. Those in the first group
are not truly antimicrobial agents but more plaque
removal agents in that they have the potential to
disrupt the early plaque matrix, thereby dislodging
bacteria from the tooth surface. In the late 1960s/early
1970s enzymes such as dextranase, mutanase and
various proteases were thought to be a major break-
through in dental plaque control that might prevent
the development of both caries and gingivitis. Such
agents, unfortunately, had poor substantivity and
were not without unpleasant local side effects, notably
mucosal erosion. The second group of enzymes em-
ployed glucose oxidase and amyloglucosidase to en-
hance the host defense mechanism. The aim was to
catalyse the conversion of endogenous and exogenous
thiocyanate to hypothiocyanite via the salivary lac-
toperoxydase system. The hypothiocycanite produces

472 • CHAPTER 22
Table 22-1. Groups of agents used in the control of dental plaque and/or gingivitis
Group
Examples of agents
Action
Used now/product
Antibiotics
Penicillin
Vancomycin
Kanamycin
Niddamycin
Spiromycin
Antimicrobial
No
Enzymes
Protease
Lipase
Nuclease
Dextranase
Mutanase
*Glucose oxidase
*Amyloglucosidase
Plaque removal
Antimicrobial
No
*Yes
Toothpaste
Bisbiguanide antiseptics
*Chlorhexidine
Alexidine
Octenidine
Antimicrobial
*Yes
Mouthrinse
Spray
Gel
Toothpaste
Chewing gum
Varnish
Quaternary ammonium
compounds
*Cetylpyridinium chloride
*Benzalconium chloride
Antimicrobial
*Yes
Mouthrinse
Phenols & essential oils
*Thymol
*Hexylresorcinol
*Ecalyptol
*Triclosan+
*Antimicrobial
+Anti-inflammatory
*Yes
Mouthrinse
Toothpaste
Natural products *Sanguinarine
Antimicrobial
*Yes
Mouthrinse
Toothpaste
Fluorides
(*)Sodium Fluoride
(*)Sodium monofluoro-
phosphate
*Stannous fluoride+
+Amine fluoride
*Antimicrobial
( )minimal
+?
+*Yes
Toothpaste
Mouthrinse
+Gel
Metal salts
*Tin+
*Zinc
Copper
Antimicrobial
*Yes
Toothpaste
Mouthrinse
+Gel
__
Oxygenating agents
Li
*Hydrogen peroxide
*Sodium peroxyborate
*Sodium peroxycarbonate
Antimicrobial
?Plaque removal
*Yes
Mouthrinse
Detergents
*Sodium lauryl sulfate
Antimicrobial
?plaque removal
*Yes
Toothpaste
Mouthrinse
Amine alcohols
Octapinol
Delmopinol
Plaque matrix
Inhibition
No
inhibitory effects upon oral bacteria, particularly paste products containing the enzymes and thiocy-
streptococci, to interfere with their metabolism. This
anate were produced but equivocal results for benefits
approach is a theoretical possibility and the chemical
to gingivitis were obtained and there are no convinc-
processes can be produced in the laboratory. Tooth- ing long-term studies of efficacy.
THE USE OF ANTISEPTICS IN PERIODONTAL THERAPY • 473
Bisbiguanide
antiseptics (for review see Addy et al.
1986, 1994, Kornman 1986, Gjermo 1989, Jones 1997)
Chlorhexidine is thus far the most studied and effec-
tive antiseptic for plaque inhibition and the preven-
tion of gingivitis. Consequent upon the original pub-
lication (Loe & Schiott 1970), chlorhexidine, arguably
perhaps, represents the nearest that research has come
to identifying a chemical agent that could be used as
a replacement for, rather than an adjunct to, mechani
-
cal oral hygiene practices. Other bisbiguanides such
as alexidine and octenidine have less or similar activ-
ity, respectively, to chlorhexidine but bring with them
no improvement in local side effects and have less
toxicity data available. Chlorhexidine has thus re-
mained the only bisbiguanide used in a number of
vehicles and available in commercial products. In
view of the importance of this antiseptic within pre-
ventive dentistry, a separate section later in the chap-
ter will be devoted to considering its activity and
usage in the mouth.
Quaternary ammonium compounds
(for review see
Mandel 1988)
Benzylconium chloride and, more particularly, ce-
tylpyridinium chloride are the most studied of this
family of antiseptics. Cetylpyridinium chloride is
used
in a wide variety of antiseptic mouthrinse products
usually at a concentration of 0.05%. At oral pH
these
antiseptics are monocationic and adsorb readily
and
quantitatively, to a greater extent, than chlor
hexidine
to oral surfaces (Bonesvoll & Gjermo 1978).
However,
the substantivity of cetylpyridinium chlo
ride appears
to be only 3-5 hours (Roberts & Addy 1981) due
either to loss of activity once adsorbed or
rapid
desorption. Cetylpyridinium chloride in
mouthrinses
has some chemical plaque inhibitory ac-
tion but
evidence for gingivitis benefits is equivocal,
particularly when formulations are used alongside
toothbrushing with toothpaste. Long-term home use
studies, given the large number of rinse products
containing this antiseptic, are surprisingly few. Those
that are available, with one exception, failed to dem-
onstrate any adjunctive benefits to toothbrushing
with toothpaste, of cetylpyridinium chloride mouth-
rinses. The one exception (Allen et al. 1998) was pecu
-
liar in that there was a lack of the expected Hawthorne
effect in the control group (see section "Evaluation of
chemical agents and products" later in this chapter)
and the plaque reduction in the active group, 28%, was
as great as seen in chemical plaque inhibition studies.
As will be discussed, it is not unusual to find chemi-
cals that provide modest, even moderate, plaque inhi-
bition in no brushing studies but fail to show effects
in adjunctive home use studies. This occurs because
the range over which to show a benefit of the chemical
is limited by the mechanical oral hygiene practices of
the study subjects. The efficacy of cetylpyridinium
chloride can be increased by doubling the frequency
of rinsing to four times per day (Bonsvoll & Gjermo
1978), but this increases local side effects, including
tooth staining, and would affect compliance.
Mouthrinses combining cetylpyridinium chloride with
chlorhexidine are available and compare well
with
established chlorhexidine products (Quirynen et
al.
2001). Whether the cetylpyridinium chloride actu
ally
contributed to the activity of the chlorhexidine
cannot
be assessed. There is limited information on
quaternary ammonium compounds in toothpastes
and very few products are available.
Phenols and essential oils
(for review see Mandel
1988)
Phenols and essential oils have been used in mouth-
rinses and lozenges for many years. One mouthrinse
formulation dates back more than 100 years and al-
though not as efficacious as chlorhexidine, has anti-
plaque activity supported by a number of short and
long-term home use studies. Combining essential oils
with cetylpyridinium chloride has been attempted
and with promising results from initial studies
(
Hunter et al. 1994).
The non-ionic antimicrobial triclosan is usually
considered to belong to the phenol group and has been
widely used over many years in a number of medi-
cated products including antiperspirants and soaps.
More recently, it has been formulated into toothpaste
and mouthrinses and, for the former, has accumulated
an impressive amount of literature, some of which is
conflicting. In simple solutions, at relatively high con-
centrations (0.2%) and dose (20 mg twice per day),
triclosan has moderate plaque inhibitory action and
antimicrobial substantivity of around 5 hours (Jenkins
et al. 1991a,b). The dose response against plaque of
triclosan alone is relatively flat (Jenkins et al. 1993)
although significantly greater benefits are obtained at
20 mg doses twice daily compared to 10 mg doses. In
terms of plaque inhibition, a 0.1% triclosan concentra
-
tion (10 mg dose twice per day) was considerably less
effective than a 0.01% chlorhexidine mouthrinse (1 mg
twice per day) (Jenkins et al. 1994).
The activity of triclosan appears to be enhanced by
the addition of zinc citrate or the co-polymer, poly-
vinylmethyl ether maleic acid (for reviews see Cum-
mins 1992, Gaffar et al. 1992). The co-polymer appears
to enhance the retention of triclosan whereas the zinc
is thought to increase the antimicrobial activity. Only
triclosan toothpastes with the co-polymer or zinc cit-
rate have shown antiplaque activity in long-term
home use studies (Svatun et al. 1989, Garcia-Gadoy et
al. 1990, Stephen et al. 1990, for review see Jackson
1997). Some home use studies showed little or no
effect for one or other of the products on plaque alone,
gingivitis alone or both (Palomo et al. 1994, Kancha-
nakamol et al. 1995, Renvert & Birkhed 1995, Binney
et al. 1996, Owens et al. 1997). Triclosan toothpastes
appear to provide greater gingivitis benefits in some
studies than plaque reductions and this could be ex-
plained by a possible anti-inflammatory action for this
agent (Barkvoll & Rolla 1994).
More recently, long-term studies have suggested
474 • CHAPTER 22
that triclosan-containing toothpaste can reduce the
progress of periodontitis, although the effects were so
small as to be of questionable clinical relevance (
Rosling et al. 1997, Ellwood et al. 1998). Mouthrinses
containing triclosan and the co-polymer are available,
with some evidence of adjunctive benefits to oral hy-
giene and gingival health when used alongside nor-
mal tooth cleaning (Worthington et al. 1993). This
latter study was again interesting with, unusually, no
clear Hawthorne effect in the control group. Other
studies on the plaque inhibitory properties of a tri-
closan/co-polymer mouthrinse showed effects sig-
nificantly less than an essential oil mouthrinse prod-
uct (Moran et al. 1997).
Natural
products (for review see Mandel 1988)
Herb and plant extracts have been used in oral hy-
giene products for many years if not centuries. Unfor-
tunately, there are few data available and such tooth-
paste products provide no greater benefits to oral
hygiene and gingival health than conventional fluo-
ride toothpaste does (Moran et al. 1991). The plant
extract sanguinarine has been used in a number of
formulations. Zinc salts are also incorporated, which
makes it difficult to evaluate the efficacy of sangui-
narine alone. However, even when it is combined with
zinc, data are equivocal for benefits (Moran et al.
1988a, 1992a, Quirynen et al. 1990). Some positive
findings were reported for the combined use of san-
guinarine/zinc toothpaste and mouthrinses (Kopczyk
et al. 1991), but the benefit-to-cost ratio must be
low.
Importantly and very recently, sanguinarine-con-
taining mouthrinses have been shown to increase the
likelihood of oral precancerous lesions almost ten-fold
even after cessation of mouthrinse use. The manufac-
turer of the most well-known product has replaced
sanguinarine in the mouthrinses with an alternative
agent.
Fluorides
The caries preventive benefits for a number of fluoride
salts are well established but the fluoride ion has no
effect against the development of plaque and gingivi-
tis. Amine fluoride and stannous fluoride provide
some plaque inhibitory activity, particularly when
combined; however, the effects appear to be derived
from the non-fluoride portion of the molecules. A
mouthrinse product containing amine fluoride and
stannous fluoride is available and there is some evi-
dence from home use studies of efficacy against
plaque and gingivitis (Brecx et al. 1990, 1992), but less
so than chlorhexidine.
Metal salts
(for reviews see Addy et al. 1994, Jackson
1997)
Antimicrobial actions including plaque inhibition by
metal salts have been appreciated for many years,
with most research interest centered on copper, tin and
zinc. Results have been somewhat contradictory but
appear dependent on the metal salt used, its concen-
tration and use. Essentially, polyvalent metal salts
alone are effective plaque inhibitors at relatively high
concentration when taste and toxicity problems may
arise. Stannous fluoride is an exception but is difficult
to formulate into oral hygiene products because of
stability problems, with hydrolysis occurring in the
presence of water (Miller et al. 1969). Stable anhydrous
gel and toothpaste products are available with evi-
dence of efficacy against plaque and gingivitis
(
Beiswanger et al. 1995, Perlich et al. 1995). Stannous
pyrophosphate at 1% has been added to some stan-
nous fluoride toothpaste to good effect (Svatun et al.
1978). Indeed, it appears that the concentration of
available stannous ions is the most significant factor
in determining efficacy (Addy et al. 1997). Dental
staining, however, occurs with stannous formulations
and appears to occur by the same mechanism as for
chlorhexidine and other cationic antiseptics, involv-
ing interaction with dietary chromogens (for reviews
see Addy & Moran 1995, Watts & Addy 2001). Com-
bining metal salts with other antiseptics produces
added plaque and gingivitis inhibitory effects, for
example zinc and hexetidine (Saxer & Muhlemann
1983) and, as already described, zinc and triclosan.
Copper also causes dental staining but is not available
in oral hygiene products. Zinc, at low concentration,
has no side effects and is used in a number of tooth-
pastes and mouthrinses; however, alone it has little
effect on plaque (Addy et al. 1980) except at higher
concentrations.
Oxygenating
agents (for review see Addy et al. 1994)
Oxygenating agents have been used as disinfectants
in various disciplines of dentistry, including endodon
-
tics and periodontics. Hydrogen peroxide has been
employed for supragingival plaque control and more
recently has become important as a bleach in tooth
whitening. Similarly, peroxyborate may be used in the
treatment of acute ulcerative gingivitis (Wade et al.
1966). Products containing peroxyborate and peroxy
-
carbonate are available in Britain and Europe with
evidence of antimicrobial and plaque inhibitory activ-
ity (Moran et al. 1995). There are little data from long
-
term home use studies and such evaluations would
seem warranted before conclusions about true anti-
plaque activity can be drawn.
Detergents
Detergents, such as sodium lauryl sulfate, are com-
mon ingredients in toothpaste and mouthrinse prod-
ucts. Besides other qualities and, for that matter, side
effects, detergents such as sodium lauryl sulfate have
antimicrobial activity (Moran et al. 1988b) and prob-
ably provide most of the modest plaque inhibitory
action of toothpaste (Addy et al. 1983). Alone, sodium
lauryl sulfate was shown to have moderate substan-
tivity measured at between 5 and
7
hours and plaque
inhibitory action similar to triclosan (Jenkins et al.
1991a,b). Detergent only formulations are not avail-