Markovchick Vincent J., Pons Peter T., Bakes Katherine M.(ed.) Emergency medicine secrets. 5th ed
Подождите немного. Документ загружается.


Chapter 46 THYROID AND ADRENAL DISORDERS318
4. What lab tests should be ordered in a patient with suspected
hyperthyroidism?
When hyperthyroidism is suspected, the best tests to order are the thyroid-stimulating
hormone (TSH) level and either a free thyroxine (T
4
) level or total T
4
with a triiodothyronine
(T
3
) resin uptake. When hyperthyroidism is caused by overproduction of thyroid hormone,
TSH should be completely suppressed (,0.03 mIU/L). A patient with a suppressed TSH and a
normal T
4
level has subclinical hyperthyroidism.
5. What is apathetic thyrotoxicosis?
A frequently missed presentation of hyperthyroidism seen most commonly in the elderly but
may present at any age, even in children. The typical patient is 70 to 80 years old without
goiter or ophthalmologic findings. The diagnosis should be considered in elderly patients with
chronic weight loss, proximal muscle weakness, depressed affect, new-onset atrial fibrillation,
or congestive heart failure.
6. What is thyroid storm?
Thyroid storm is simply an exaggerated form of hyperthyroidism that carries with it a risk
of serious morbidity or even mortality. The clinical features that are characteristic of
thyroid storm include fever (temperature .100°F [37.7°C]), altered mental status, and
cardiovascular decompensation. A common clinical challenge is to determine if one of
these features is due to the thyroid hyperfunction or some other underlying disease such
as drug or alcohol intoxication, an infectious process, or underlying cardiac disease. A
clinical determination of thyroid storm should be made without necessarily waiting for
confirmatory laboratory tests.
7. Which patients with hyperthyroidism should be admitted to the hospital?
While clinical judgment is needed, patients who are suspected of thyroid storm should be
admitted. Those with atrial fibrillation should be admitted and anticoagulated because there is
an increased risk of atrial thrombus in this condition. Patients who are unable to maintain
adequate oral intake due to nausea need to be admitted. Patients who have serious
hyperthyroidism and signs and symptoms of heart failure should be admitted because it is
often difficult to determine the appropriate dose of b-blockers for these individuals in the
outpatient setting. Tachycardia alone, even if marked, is not an indication for admission in an
individual who is otherwise young and healthy because b-blockade can safely be instituted as
an outpatient.
8. What conditions are included in the differential diagnosis of thyroid storm?
Toxicity caused by cocaine, amphetamines, other sympathomimetics, and anticholinergics;
alcohol withdrawal syndromes; or infections such as encephalitis, meningitis, and sepsis. A
history of goiter, thyroid disease or previous treatment with an antithyroid medication is
helpful in distinguishing thyroid storm from these other conditions.
9. What conditions precipitate thyroid storm?
Thyroid storm typically is precipitated by another problem. Although it is important to treat the
thyroid storm directly, it is also important to identify and treat the underlying precipitant.
Some of the more common precipitating events include:
n
Infection or serious illness
n
Surgery
n
Trauma
n
Childbirth
n
Myocardial infarction
n
Withdrawal of antithyroid therapy
n
Recent
131
I thyroid ablation therapy
Chapter 46 THYROID AND ADRENAL DISORDERS 319
10. How is hyperthyroidism treated in the ED?
For most patients seen in the ED with hyperthyroidism, treatment with a b-blocker can
be initiated. Although propranolol blocks the conversion of T
4
to T
3
and is preferred by
some, it needs to be taken at least three times a day in the hyperthyroid patient because
of more rapid metabolism. Metoprolol or atenolol are reasonable options and can be
given twice a day resulting in better compliance as compared with propranolol. Although
Tapazole or propylthiouracil can be initiated, a thyroid scan cannot be done while the
patient is taking these medications. For this reason, it is typically best to start a b-blocker
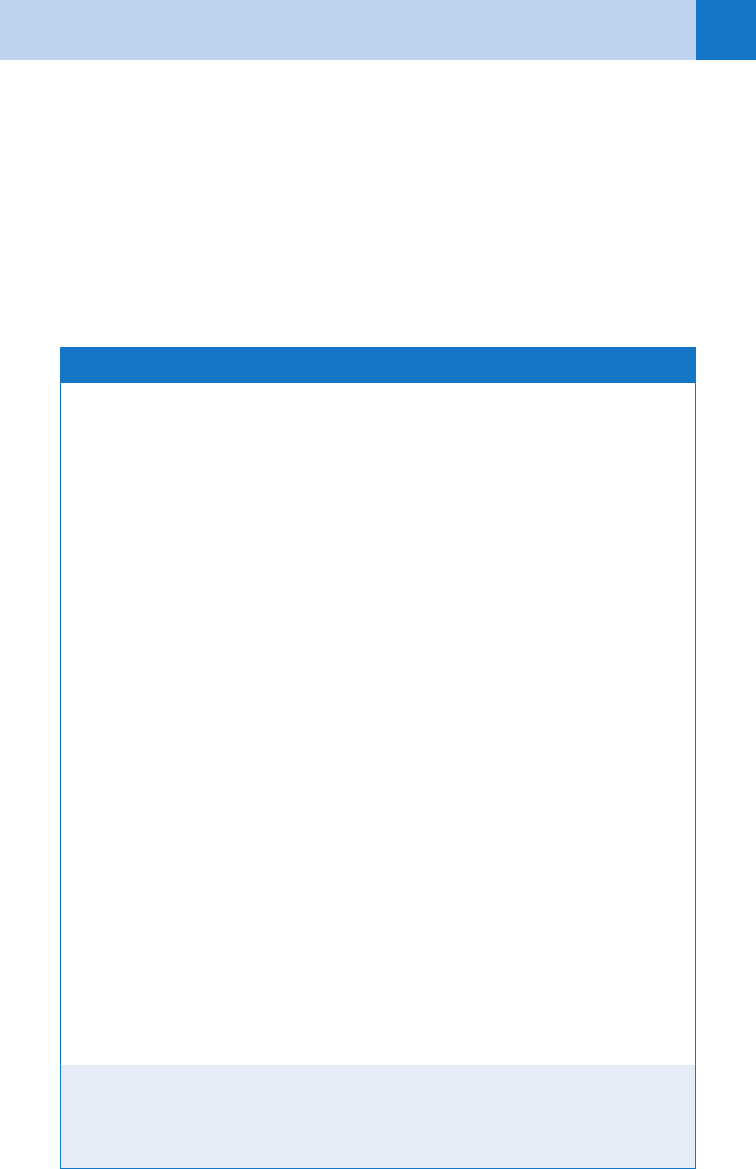
and refer the patient for follow-up. ED management of thyroid storm is outlined on
Table 46-1.
IV, intravenous; PO, per os; PTU, propylthiouracil; T
3
, triiodothyronine; T
4
, thyroxine.
*
Preferred medication.
†Consider.
American Thyroid Association: www.thyroid.org
1. Supportive care
n
General: Oxygen, cardiac monitor
n
Fever: External cooling, acetaminophen (aspirin is contraindicated because it may increase
free T
4
)
n
Dehydration: IV fluids
n
Nutrition: Glucose, multivitamins, including folate (deficient secondary to hypermetabolism)
n
Cardiac decompensation (atrial fibrillation, congestive heart failure): b-blockers.
Atenolol or metoprolol 25 to 100 mg two times per day. Effective dose may be higher,
typically used as the metabolism is increased with hyperthyroidism. Esmolol adminis-
tered intravenously is preferred if there is evidence of congestive heart failure. Begin
with 500 mg/kg load over 1 minute, followed by 50 mg/kg/min intravenously. Repeat
load and double infusion as necessary
n
Treat precipitating event: Therapy as indicated
2. Inhibition of hormone biosynthesis—thionamides
n
PTU,* 1200–1500 mg/day, given as a loading dose of 600–800 mg followed by 200–300 mg
every 6 hours PO, by nasogastric tube, or rectally (also blocks peripheral conversion of T
4
to T
3
)
or
n
Methimazole, up to 120 mg/day, given as 20 mg PO every 4 hours (or 40 mg crushed in
an aqueous solution rectally).
3. Blockade of hormone release—iodides* (at least 1 hour after step 2)
n
Lugol’s solution or supersaturated potassium iodide (SSKI), 30–60 drops/day orally
divided three or four times per day
or
n
Ipodate (Oragrafin), 0.5–3 g/day (especially useful with thyroiditis or thyroid hormone
overdose)
4. Blocking the peripheral conversion of T
4
to T
3
:
n
High-dose steroids: Hydrocortisone 100 mg intravenously every 8 hours or prednisone
60 mg PO daily.
TABLE 46–1. STEP THERAPY OF DECOMPENSATED THYROTOXICOSIS
Chapter 46 THYROID AND ADRENAL DISORDERS320
KEY POINTS: THYROID STORM
1. Thyroid disease is extremely common in the ED population.
2. Thyroid storm and myxedema coma are true medical emergencies.
3. Include thyroid storm in your differential for toxic ingestions.
4. Treatment for thyroid storm is initiated without waiting for laboratory work-up.
11. How is acute thyroid hormone overdose treated?
Fatalities are rare with acute ingestion. Toxicity after massive acute overdose usually occurs
within 4 to 12 hours but may be delayed for days, particularly with T
4
ingestion. Acute
overdose management is as usual, including charcoal and work-up for coingestants.
12. What is Graves ophthalmopathy?
Clinical features include proptosis, injection, chemosis (edema of the conjunctiva), and rarely
diplopia with poor eye movement, especially on upward gaze. A loss in visual acuity is a
particularly concerning finding. Some eye findings are seen in about half of patients with
Graves disease.
13. When is treatment of Graves ophthalmopathy an emergent condition?
Patients with compression of the optic nerve or corneal ulceration require immediate
ophthalmologic consultation. Visual blurring that persists with eye closure and diminished
color brightness suggests compression of the optic nerve. Severe proptosis can cause
keratitis or corneal ulceration presenting as eye pain, photophobia, conjunctival infection,
visual loss, and a flare of cells in the anterior chamber. Optic neuropathy is initially treated
with high-dose steroids (e.g., prednisone, 1–2 mg/kg per os [PO]). Corneal ulcers, with or
without keratitis, require culture and topical antibiotics.
14. What are the common clinical manifestations of hypothyroidism?
n
Constitutional: Fatigue, cold intolerance, weight gain, lethargy, hoarse or deep voice, slow
speech, and drowsiness
n
Neuropsychiatric: Delayed relaxation phase of deep tendon reflexes (hung up reflex),
depression, moodiness, and rarely dementia or psychosis
n
Cardiovascular: Bradycardia and less commonly congestive heart failure, and rarely
pericardial effusion
n
Respiratory: Occasionally dyspnea, hypoventilation, and rarely pleural effusions
n
Musculoskeletal: Joint swelling and muscle cramps
n
Dermatologic: Cool, dry skin and hair loss
n
Gynecologic: Metromenorrhagia
15. What are the most common causes of hypothyroidism?
Primary hypothyroidism due to thyroid gland dysfunction: In these conditions TSH is
increased and T
4
is decreased. A patient with an increased TSH but a normal T
4
has subclinical
hypothyroidism.
n
Autoimmune thyroid destruction: Hashimoto’s thyroiditis (90% of all cases). Thyroid gland
may be firm or small.
n
Thyroiditis: Following a period of hyperthyroidism, the gland may be hypofunctioning
permanently or transiently (1–2 years).
n
Hypothyroidism following thyroidectomy or radioactive iodine treatment.
Pituitary or hypothalamic insufficiency resulting in inadequate TSH secretion: In these
conditions, TSH is typically normal (or low), and T
4
is also low. These patients typically show
Chapter 46 THYROID AND ADRENAL DISORDERS 321
signs and symptoms of follicle-stimulating hormone/luteinizing hormone (FSH/LH) deficiency
(amenorrhea in women, hypogonadism in men).
n
Pituitary tumor
n
Pituitary infarction, Sheehan’s syndrome, or pituitary apoplexy
n
Meningioma or craniopharyngioma near hypothalamus
16. What additional features are present in myxedema coma?
The hallmark clinical features are hypothermia (75%), bradycardia, hypoventilation, and coma
in a patient with a history of thyroid disease. Laboratory evaluation may reveal anemia,
hyponatremia, hypercarbia and a respiratory acidosis, or respiratory failure. Electrocardiogram
(ECG) may show bradycardia with low voltages that may be due to a pericardial effusion. The
chest radiograph may show pleural effusions, or frank congestive heart failure.
17. What precipitates myxedema coma in the hypothyroid patient?
As is true with thyroid storm, myxedema coma is typically precipitated by an intercurrent
illness such as a pulmonary or renal infection, sedatives and anesthetic agents (including
etomidate), trauma, myocardial infarction, cerebrovascular accident, or gastrointestinal
hemorrhage. Even moderate hypothyroidism may be life-threatening in patients with
underlying hypoxia, hypercapnia or congestive heart failure.
18. What is the treatment for myxedema coma?
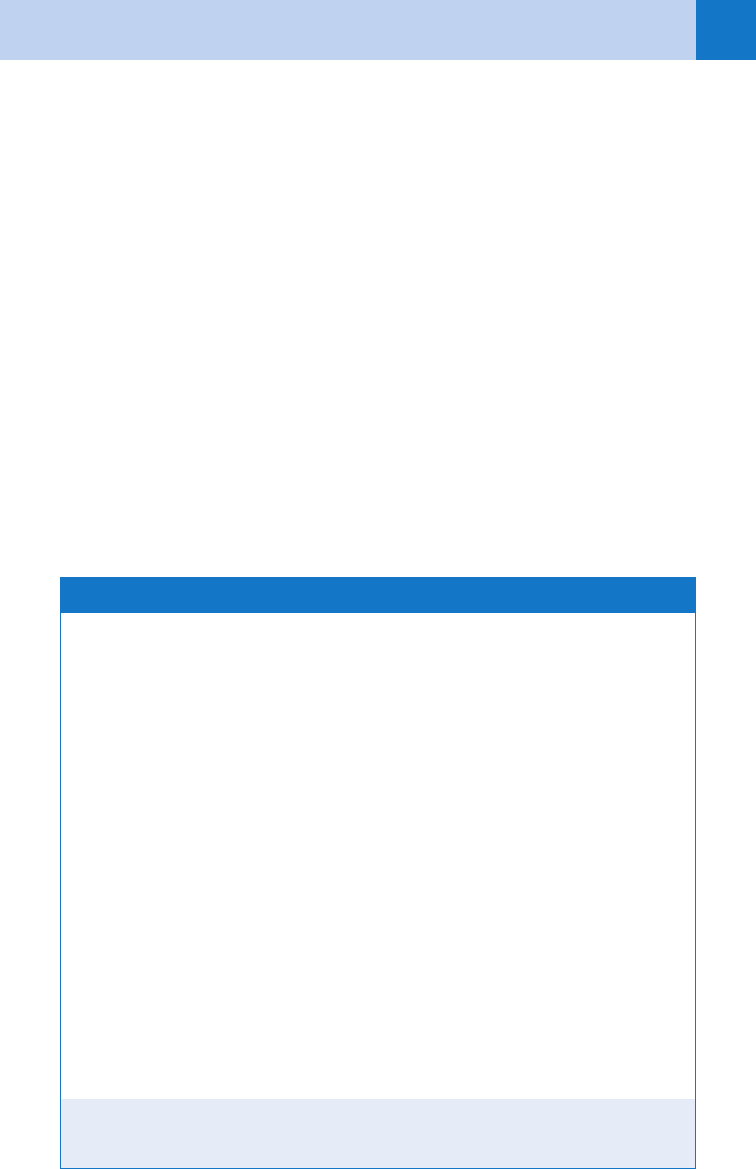
See Table 46-2.
ABCs, airway, breathing, circulation; IV, intravenous; T
3
, triiodothyronine; T
4
, thyroxine.
Citkowitz E: Myxedema coma or crisis, 2004. www.emedicine.com.
1. Supportive care
n
Airway control, oxygen, IV access, and cardiac monitor (ABCs).
n
Hypotension is treated with crystalloids.
n
Vasopressors as indicated (ineffective without thyroid hormone replacement).
n
Baseline thyroid function studies should be sent.
n
Hypothermia is treated with passive rewarming.
n
Perform a Cortrosyn stimulation test and then empirically treat with hydrocortisone
(100 mg intravenously every 8 hours) until results are available. This is because of
increased metabolism of cortisol that will occur when thyroid hormone is replaced, which
may precipitate adrenal insufficiency if there is underlying adrenal insufficiency.
2. Thyroid replacement therapy
n
IV T
4
(4 mg/kg; followed in 24 hours by 100 mg intravenously, then 50 mg intravenously
until oral medication is tolerated)
n
T
3
(liothyronine), at 20 mg intravenously followed by 10 mg intravenously every 8 hours
until the patient is conscious (given because of the risk of decreased T
3
generation from
T
4
in severely hypothyroid patients). This is not widely available and typically IV T
4
is
sufficient.
3. Identify and treat precipitating factors
4. Treat concomitant metabolic abnormalities, including hyponatremia,
hypoglycemia, and hypercalcemia
TABLE 46–2. TREATMENT FOR MYXEDEMA COMA

Chapter 46 THYROID AND ADRENAL DISORDERS322
19. What is the significance of a palpable thyroid nodule in an asymptomatic
patient?
Palpable thyroid nodules are a common physical finding in the general population occurring in
5% to 8% of all adults. Most are benign adenomas that are not a threat to health. Because a
small percentage of solitary nodules are thyroid carcinomas, referral for fine-needle aspiration
biopsy is indicated for all patients with palpable nodules who have normal thyroid function
tests (TSH, free T
4
). Biopsy results identify 70% of nodules to be benign, 5% to be malignant,
and the remainder to be cytologically indeterminate.
20. What advice should be given to the patient when a nonpalpable thyroid
nodule is incidentally found on a radiologic study?
Thyroid nodules smaller than 1 cm are usually not detected on physical examination but may
be identified incidentally on magnetic resonance imaging, computed tomography, or
ultrasound done for another reason. These types of nodules are quite common and may occur
in 30% to 50% of the general population. Serum levels of TSH and T
4
should be measured
and patients should be told of the finding. They should be reassured that the finding is
common and does not definitely indicate the presence of cancer. However, the risk of cancer
is the same in small nodules as it is in large nodules. These patients should ideally have a
formal thyroid ultrasound to look for features such as microcalcification that raise the concern
for cancer. If thyroid function tests are normal and the ultrasound is not concerning, the neck
ultrasound should be repeated in 6 to 12 months to monitor for growth of the nodule.
21. What are the adrenal emergencies that I need to worry about?
There are two serious adrenal emergencies: acute adrenal insufficiency and pheochromocytoma.
Hypercortisolism due to a tumor secreting pituitary adrenocorticotropic hormone (ACTH),
ectopic ACTH secretion, or an adrenal tumor that may present with weight gain, hypertension,
amenorrhea in women, insulin resistance, or frank diabetes. The specific physical findings in this
condition include wide (.1 cm) purple striae, easy bruising, and proximal muscle weakness.
Hyperaldosteronism is an unusual cause of hypertension that may present with spontaneous
hypokalemia.
22. List the signs and symptoms of primary adrenal insufficiency.
n
Fatigue
n
Weakness
n
Weight loss
n
Anorexia
n
Hyperpigmentation: This sign is due to increased melanocyte stimulating hormone (MSH),
which is oversecreted with ACTH when adrenal insufficiency is due to adrenal gland
failure.
n
Gastrointestinal symptoms: Nausea, vomiting, abdominal pain, and diarrhea. Abdominal
pain may be severe and mimic an acute abdomen.
n
Hypotension: This typically presents with orthostatic changes. You should think of adrenal
insufficiency when hypotension does not respond to vasopressors.
n
Fever: Temperatures as high as 40
°
C may be seen in acute adrenal insufficiency.
23. What is the difference between primary and secondary adrenal insufficiency?
Primary adrenal insufficiency is due to destruction of the adrenal gland. Secondary adrenal
insufficiency is due to inadequate production of ACTH.
24. List the causes of adrenal insufficiency.
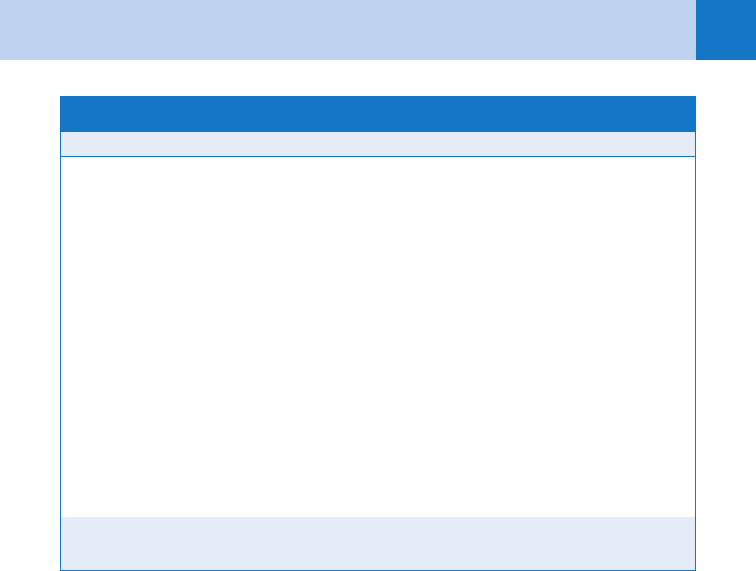
See Table 46-3.
25. What are the most common causes of primary adrenal insufficiency?
Tuberculosis and autoimmune destruction account for 90% of the cases of primary adrenal
insufficiency.
Chapter 46 THYROID AND ADRENAL DISORDERS 323
ACTH, adrenocorticotropic hormone.
Primary adrenal insufficiency Secondary adrenal insufficiency
Idiopathic (autoimmune)
Tuberculosis
Bilateral adrenal hemorrhage or infarction
AIDS
Drugs: Adrenolytic agents (metyrapone, ami-
noglutethimide, or mitotane) or ketoconazole
Infections: Fungal or bacterial sepsis
Infiltrative disorders: Sarcoidosis, hemochro-
matosis, amyloidosis, lymphoma,
or metastatic cancer
Bilateral surgical adrenalectomy
Hereditary: Adrenal hypoplasia, congenital
adrenal hyperplasia, adrenoleukodystrophy,
or familial glucocorticoid deficiency
Exogenous glucocorticoid administration
Pituitary or suprasellar tumor
Pituitary irradiation or surgery
Head trauma
Infiltrative disorders of the pituitary or hypo-
thalamus: sarcoidosis, hemochromatosis, his-
tiocytosis X, metastatic cancer, or lymphoma
Infectious diseases: Tuberculosis, meningitis,
or fungus
Isolated ACTH deficiency
TABLE 46–3. COMMON CAUSES OF ADRENAL INSUFFICIENCY
26. What is the most common cause of secondary adrenal insufficiency?
Long-term therapy with pharmacologic doses of glucocorticoids (e.g., prednisone,
methylprednisolone, and dexamethasone) is the most common cause of secondary adrenal
insufficiency. These drugs are used to treat a wide variety of medical problems, and if they are
used for any significant time, some degree of suppression of the hypothalamic-pituitary-
adrenal (HPA) axis occurs.
27. How long must a patient be treated with steroids to cause suppression of the
HPA axis, and how long does it take them to recover normal function?
The body needs higher levels of glucocorticoids when stressed. For this reason, signs and
symptoms of adrenal insufficiency are most pronounced when patients are sick with an
intercurrent illness and are not able to respond with an adequate level of cortisol. Some
patients who are on maximal stress doses of steroids (e.g., .60 mg/day of prednisone)
for longer than 1 week may have a blunted response to ACTH. This will typically resolve
over a few weeks or months. If a person has been on maximal stress doses of steroids
for many months or years and then is tapered gradually, they may be able to make enough
cortisol for normal daily functioning, but if they are septic, have a myocardial infarction, or
sustain severe trauma, they may exhibit signs and symptoms of adrenal insufficiency even
1 to 2 years later.
28. What are the characteristic laboratory findings of primary adrenal
insufficiency?
Hyperkalemia may be present because of a lack of aldosterone in addition to cortisol
deficiency. Hyponatremia may be present and is due to the SIADH. Cortisol is one of the
counter-regulatory hormones that increase liver glucose production with fasting. In the
setting of adrenal insufficiency hypoglycemia may develop if the patient has not eaten.
Anemia and an increase in eosinophils may be seen. Rarely adrenal insufficiency causes
hypercalcemia.

Chapter 46 THYROID AND ADRENAL DISORDERS324
29. How is the presentation of secondary adrenal insufficiency different from that
of primary adrenal insufficiency?
In secondary adrenal insufficiency, there is no deficiency of aldosterone secretion. As a result
these patients do not have hyperkalemia. Hypotension and hyponatremia can be seen and do
not help distinguish primary from secondary adrenal insufficiency. Patients who have adrenal
insufficiency from a suppressed HPA axis due to chronic steroid use may have a Cushingoid
appearance. If the patient has a pituitary or hypothalamic cause for the adrenal insufficiency,
findings may include symptoms of other pituitary hormone deficiencies, such as
hypothyroidism, amenorrhea in women, or hypogonadism in men.
30. What is adrenal crisis?
Adrenal crisis is an acute and exaggerated form of adrenal insufficiency. It typically presents in
a patient with chronic adrenal insufficiency who undergoes some form of stress, such as an
acute myocardial infarction, a systemic infection, surgery, or trauma, and is unable to mount a
stress response by increasing circulating cortisol levels.
31. What is the most frequent iatrogenic cause of acute adrenal crisis?
Rapid withdrawal of steroids in patients with adrenal atrophy secondary to long-term steroid
administration.
32. Describe the common clinical features of acute adrenal insufficiency.
Patients appear to be profoundly ill. The lack of cortisol makes them vasodilated and makes
them appear significantly volume depleted with hypotension and shock. The presence of
aldosterone deficiency, anorexia, and nausea with vomiting potentiates this picture. Severe
abdominal pain that may mimic an acute abdomen can be present. Fever may occur as a
result of infection or the adrenal insufficiency itself. Central nervous system symptoms of
confusion, disorientation, and lethargy may also be present.
33. How is adrenal crisis diagnosed?
You should suspect adrenal crisis when some of the typical signs and symptoms are present
in a patient who has a reason to have adrenal insufficiency. Although many of the signs and
symptoms are non-specific (e.g., fever, abdominal pain, hypotension, fatigue, anorexia) they
should raise your suspicion if the patient has a history of being treated with steroids, has a
history of a pituitary tumor, has AIDS, or has known metastatic cancer or other predisposing
conditions. When faced with this situation the proper test is the rapid ACTH stimulation test.
Sometimes clinicians simply treat and do not get a test. The problem with this approach is
that a day or two later the patient may be better, but you do not know if they indeed had
adrenal crisis to begin with and unfortunately by then, the steroids used to treat them make
diagnostic testing more difficult. A second approach is to get a random cortisol level with the
thought that “the patient is sick, so the level will probably be high.” The problem with this
approach is that if the cortisol level is 10 to 20 ug/dl, you can neither say the patient is normal
or insufficient. For this reason the best test is the ACTH stimulation test.
34. How is the rapid ACTH stimulation test performed?
A baseline sample of blood is drawn at time 0 for a cortisol level. Then 0.25 mg of
cosyntropin (synthetic ACTH) is given intravenously. Cortisol levels are checked at 30 minutes
and 1 hour later.
35. But what if the patient needs emergent treatment with steroids? Should I
withhold treatment until the rapid ACTH stimulation test has been done?
No! If your patient is unstable, you can begin treatment using a glucocorticoid that will not
cross react with the cortisol assay. A cortisol level can be drawn and then dexamethasone
(6–10 mg) can be administered intravenously. Then cosyntropin 0.25 mg is given
intravenously and serum cortisol levels drawn 30 and 60 minutes later. By using this
approach, the patient has the benefit of receiving stress-dose steroids in a timely manner
Chapter 46 THYROID AND ADRENAL DISORDERS 325
and also has had the appropriate diagnostic test so that the nature of their illness can be
better understood as their clinical course develops.
36. How is acute adrenal insufficiency treated?
Stress-dose steroids should be promptly administered once the diagnosis of acute adrenal
insufficiency is considered and the ACTH stimulation test initiated. IV administration of
hydrocortisone (100 mg minimum) and crystalloid IV fluids containing dextrose is the
standard approach. A detailed history and examination should be done to elicit what may have
precipitated the stress that caused the acute adrenal insufficiency. If a cause is found,
supportive and definitive measures need to be instituted in the ED. If there is uncertainty,
empiric administration of broad-spectrum antibiotics may be prudent while waiting for culture
results. Mineralocorticoid replacement is usually unnecessary if salt and water replacement is
adequate and if the patient receives hydrocortisone—100 mg of hydrocortisone has the salt-
retaining effect of 0.1 mg of fludrocortisone.
KEY POINTS: ADRENAL CRISIS
1. Consider adrenal crisis in all hypotensive patients, especially if unresponsive to pressors.
2. All patients in adrenal crisis require rapid administration of IV steroids.
3. Dexamethasone may be initiated in adrenal crisis without affecting the cosyntropin (ACTH)
stimulation test.
4. Only 2 weeks of high-dose steroid use can cause adrenal suppression, making a patient
more prone to adrenal crisis.
37. What should be done for the patient with chronic adrenal insufficiency who
presents to the ED with a minor illness or injury?
These patients usually require supplemental steroid hormone that is appropriate for their
degree of medical illness. When seeing a patient who has an acute illness, a dose of
hydrocortisone or prednisone that is between the daily replacement dose and the maximal
stress dose that is appropriate for the degree of illness that they are experiencing should be
administered. A usual daily replacement dose of steroids for someone with adrenal
insufficiency who is otherwise healthy would be 20–30 mg/day of hydrocortisone or 5–6 mg
of prednisone. Someone who is critically ill would typically be given 100 mg of hydrocortisone
three times per day (300 mg) or 60 mg per day of prednisone. This increased dose should be
continued for 24–48 hours until symptoms improve. Adding a mineralocorticoid is usually not
necessary. Follow-up care should be coordinated closely with the primary care physician or
endocrinologist. Patients should be told that if nausea or vomiting develops and they are
unable to keep down the medication, they should immediately seek medical attention. Patients
should be reminded that they should have a medic-alert bracelet so that emergency physicians
can treat them appropriately in the future should they be critically ill and not able to
communicate their medical history.
38. What are the signs and symptoms of pheochromocytoma?
Pheochromocytoma is a tumor of the adrenal medulla or sympathetic ganglia that makes
excessive catecholamines (e.g., epinephrine, norepinephrine, or dopamine). The classic
symptoms of a pheochromocytoma include headache that is typically severe, palpitations, and
sweating. These symptoms, occurring in the setting of severe hypertension, especially if the
symptoms are episodic, should raise the question of pheochromocytoma. Other symptoms
include nervousness, tremor, weight loss, and hyperglycemia.
Chapter 46 THYROID AND ADRENAL DISORDERS326
39. When should the diagnosis of pheochromocytoma be considered?
A diagnosis of pheochromocytoma should be considered in a patient who has the typical
symptoms and severe hypertension, especially episodic hypertension, hypertension that requires
four or more medications to control, or hypertension that began before the age of 35 years or
after age 60. Patients who are hypertensive and have a family history of severe episodic
hypertension, or components of multiple endocrine neoplasia type 2 (medullary thyroid cancer,
hyperparathyroidism, and pheochromocytoma) should also be considered at risk.
40. What is unique about the treatment of hypertension in a patient with
pheochromocytoma?
The most important thing to remember is to not use beta blockers as a first-line treatment
when a diagnosis of pheochromocytoma is being considered. This is because b-blockade will
result in unopposed a-receptor activation, which will increase vasoconstriction and worsen
hypertension. Pure vasodilators can be used in the acute setting. It is important to institute
good a-blockade early using medications such as phenoxybenzamine or prazosin. Labetalol
has the advantage of having both a- and b-blocking activities and is also useful in this setting.
WEBSITES
1. Adrenal insufficiency and adrenal crisis: www.emedicine.com.
2. American Association of Clinical Endocrinologists: www.aace.com.
3. American Thyroid Association: www.thyroid.org.
4. Hyperthyroidism, thyroid storm, and Graves disease: www.emedicine.com.
5. Myxedema coma or crisis: www.emedicine.com.
6. Thyroid Disease Manager: www.thyroidmanager.org
BIBLIOGRAPHY
1. Beale MB, Belzberg H: Adrenal insufficiency. In Grenvik A, editor: Textbook of critical care, ed 4, Philadelphia,
2000, W. B. Saunders, pp 806–816.
2. Bravermann LE, Burch HB, Wartofsky L: Life-threatening thyrotoxicosis-thyroid storm. Endocrinol Metab Clin
North Am 22:263–277, 1993.
3. Braverman LE, Utigar RD, Werner SC, et al, editors: Werner and Ingbar’s the thyroid: a fundamental and
clinical text, ed 8, Philadelphia, 2000, Lippincott Williams & Wilkins.
4. Cooper MS, Stewart PM: Corticosteroid insufficiency in acutely ill patients. N Engl J Med 348:727–734, 2003.
5. Hegedus L: The thyroid nodule. N Engl J Med 351:1764–1771, 2004.
6. Hermus AR, Huysmans DA: Treatment of benign nodular thyroid disease. N Engl J Med 338:1438–1446, 1998.
7. Jordan RM: Myxedema coma: pathophysiology, therapy, and factors affecting prognosis. Med Clin North Am
79:185–194, 1995.
8. Lamberts SWJ, Bruining HA, de Jong FH: Corticosteroid therapy in severe illness. N Engl J Med 337:1285–1292,
1997.
9. Loriaux DL, McDonald WJ: Adrenal insufficiency. In DeGroot LJ, editor: Endocrinology, ed 4, vol. 2.
Philadelphia, 2001, W. B. Saunders,, pp 1683–1690.
10. Oelkers W: Adrenal insufficiency. N Engl J Med 335:1206–1212, 1996.
11. Pimentel L, Hansen KN: Thyroid disease in the emergency department: a clinical and laboratory review.
J Emerg Med 28:201–209, 2005.
12. Tietgens ST, Leinung MC: Thyroid storm. Med Clin North Am 79:169–184, 1995.
13. Weetman AP: Medical progress: Grave’s disease. N Engl J Med 343:1236–1248, 2001.
14. Wogan JM: Selected endocrine disorders. In Marx JA, Hockberger R, Walls R, et al, editors: Rosen’s
emergency medicine: concepts and clinical practice, ed 5, St. Louis, 2002, Mosby, pp 1770–1785.
327
2. How is sepsis defined?
In the ED, sepsis is defined clinically as a syndrome that has the presence of both SIRS and
presumed bacteremia.
3. What distinguishes sepsis from severe sepsis?
Severe sepsis is sepsis complicated by organ dysfunction. Severe sepsis is now considered to
be the most common cause of death in noncoronary critical care units. Approximately
150,000 people die annually in Europe and more than 200,000 die annually in the United
States from sepsis.
4. What is the significance of an elevated lactate level in sepsis?
An elevated serum lactate concentration identifies tissue hypoperfusion in patients who are
not hypotensive. Although lactate measurements may be useful and correlate with mortality,
they lack precision as a measure of tissue metabolic status.
5. What organ systems can become dysfunctional, suggesting severe sepsis?
n
Cardiovascular: Vasodilation, poor myocardial contractility and increased cardiac oxygen
demand, systemic hypotension, or cardiac ischemia
n
Central nervous system: Altered mental status
n
Global tissue hypoperfusion: Elevated lactate > 4.0 mmol/L
n
Hematologic: Increasing prothrombin time (PT), international normalized ratio (INR),
partial thromboplastin time (PTT), hemolysis and thrombocytopenia, or disseminated
intravascular coagulopathy (DIC)
n
Liver: Coagulopathy, jaundice, or elevated transaminases
n
Renal: Acute renal failure determined by increase in blood urea nitrogen (BUN) and
creatinine or decreased urine output to less than 0.5 mL/kg/h
n
Pulmonary: Acute respiratory distress syndrome, respiratory failure, or unexplained
hypoxia
SEPSIS SYNDROMES
CHAPTER 47
Stephen J. Wolf, MD
XI. INFECTIOUS DISEASE
1. What is systemic inflammatory response syndrome (SIRS)?
As its name implies, it is a syndrome of inflammation, not necessarily infection.
KEY POINTS: SIRS CRITERIA
(Two of Four Needed for Diagnosis)
1. Temperature .38°C or ,35°C
2. Heart rate .90 beats per minute
3. Respiratory rate .20 breaths per minute or PaCO
2
,32 mm Hg
4. Serum white blood cell count .12,000 mm
3
or ,4,000 mm
3
or 10% band forms