Markovchick Vincent J., Pons Peter T., Bakes Katherine M.(ed.) Emergency medicine secrets. 5th ed
Подождите немного. Документ загружается.


Chapter 48 SOFT-TISSUE INFECTIONS338
BIBLIOGRAPHY
1. Anaya DA, Dellinger EP: Necrotizing soft-tissue infection: diagnosis and management. Clin Infect Dis 44:705,
2007.
2. Crum-Cianflone NF: Infection and musculoskeletal conditions: infectious myositis. Best Pract Res Clin
Rheumatol 20:1083, 2006.
3. Frazee BW, Lynn J, Charlebois ED, et al: High prevalence of methicillin-resistant Staphylococcus aureus in
emergency department skin and soft tissue infections. Ann Emerg Med 45:311–320, 2005.
4. Fridkin SK, Hageman JC, Morrison M, et al: Methicillin-resistant Staphylococcus aureus disease in three
communities. N Engl J Med 352:1436–1444, 2005.
5. Hankin A, Everett WW: Are antibiotics necessary after incision and drainage of a cutaneous abscess?
Ann Emerg Med 50:49, 2007.
6. Kilic A, Aksoy Y, Kilic L: Fournier’s gangrene: etiology, treatment, and complications. Ann Plast Surg 47:523–527,
2001.
7. Llera JL, Levy RC: Treatment of cutaneous abscess: a double-blind clinical study. Ann Emerg Med 14:15–19,
1985.
8. Meislin HW, Guisto JA: Soft-tissue infections. In Rosen P, Barkin RM, editors: Emergency medicine: concepts
clinical practice, ed 5, St. Louis, 2002, Mosby, pp 1944–1957.
9. Meislin HW, Lerner SA, Graves MH, et al: Cutaneous abscesses: anaerobic and aerobic bacteriology and
outpatient management. Ann Intern Med 87:145(149, 1977.
10. Meislin HW, McGehee MD, Rosen P: Management and microbiology of cutaneous abscesses. J Am Coll
Emerg Physicians 7:186–191, 1978.
11. Mills AM, Chen EH: Are blood cultures necessary in adults with cellulitis? Ann Emerg Med 45:548–549, 2005.
12. Stevens DL: The flesh eating bacterium: what’s next? J Infect Dis 179(Suppl 2):S366–S374, 1999.
13. Struk DW, Munk PL, Lee MJ, et al: Imaging of soft tissue infections. Radiol Clin North Am 39:277–303, 2001.
14. Wong CH, Wang YS: The diagnosis of necrotizing fasciitis. Curr Opin Infect Dis 18:101–106, 2005.
339
SEXUALLY TRANSMITTED DISEASES
AND HIV INFECTION
CHAPTER 49
Kerry B. Broderick, MD, Erica Douglass, MD, and Jason Haukoos, MD, MSc
1. What are the most common sexually transmitted diseases (STDs)?
The true incidence of most STDs is unknown because not all cases are reported. The
Centers for Disease Control and Prevention (CDC) estimate that 19 million new STD
infections occur annually in the United States, nearly half of them among persons aged
15 to 24 years.
n
Chlamydia is estimated to infect 3 million people annually and is a major health problem
for young women because of the sequelae of infertility and ectopic pregnancy. In 2007,
over 1.1 million cases were reported to the CDC.
n
The incidence of gonorrhea peaked at more than 1 million cases per year in the late 1970s.
In 2007, 355,991 cases were reported to the CDC. The rate of gonococcal infections is
highest among adolescent girls.
n
Trichomoniasis is the most common curable STD in young sexually active women. An
estimated 7.4 million new cases occur each year.
n
Genital human papillomavirus (HPV) is estimated to have a prevalence of over 26%
in women. More than 30 types of HPV can cause genital tract infection. Genital warts
usually are caused by HPV type 6 or 11. Several types are associated with cervical
dysplasia. There is now a vaccine that prevents the types of genital human papillomavirus
(HPV) that cause most cases of cervical cancer and genital warts. The vaccine, Gardasil
®
,
is given in three shots over 6 months. The vaccine is routinely recommended for 11- and
12-year-old girls. It is also recommended for girls and women age 13 through 26 who
have not yet been vaccinated or completed the vaccine series. With the implementation
of this vaccine, it is expected that the number of HPV cases will begin to decline in
upcoming years.
n
Genital herpes occurs in 1 in 5 adolescents and adults.
n
Syphilis was on the decline with an all-time low in 2000. Since 2001, however, the rate
of both primary and secondary syphilis has risen every year. In 2007, 11,466 cases of
syphilis were reported. The greatest increase was seen in males having sex with males
(MSM). Syphilis is substantially more common in non-Hispanic blacks than in other
ethnic groups with an estimated occurrence rate of over seven times that seen in non-
Hispanic whites.
n
Cases of HIV—the most deadly STD—continue to rise. Worldwide, it is estimated that
approximately 56 million people are infected with HIV, and more than 26 million have died
of AIDS. An estimated 1.1 to 1.2 million people in the United States are living with HIV, of
which there are approximately 250,000 individuals who do not know they are infected. In
2006, 56,300 people were newly diagnosed with HIV. It is estimated that more than 36,000
patients currently live with AIDS in the United States.
2. How should I evaluate abnormal vaginal discharge?
The first thing to do is to take a complete sexual history:
a. How many partners has the patient had in the last several months (male or female)?
b. Has she used protective barriers such as condoms and dental dams with each
episode?

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION340
c. Ask about previous STDs.
d. Obtain a pregnancy test to decide on the most appropriate method of treatment if needed.
n
The appearance of the discharge on pelvic examination is important. Always take a
sample for wet preparation and potassium hydroxide.
n
Vulvovaginal candidiasis (not an STD) causes a white, curdlike discharge that clings to
vaginal walls. Hyphae are present on potassium hydroxide preparation. Recent antibiotic
use is a risk factor for this, as are diabetes and HIV. Treatment is single-dose oral
fluconazole or any of the topical imidazoles.
n
Bacterial vaginosis is not an STD but an alteration of the microbial ecosystem with
overgrowth of Gardnerella vaginalis and other species. Diagnosis is made by noting clue
cells on the wet preparation, and treatment is with metronidazole.
n
Trichomonas vaginitis, the third common cause, is a true STD. It causes a green, frothy
discharge, and the cervix may be erythematous and friable (strawberry cervix).
Diagnosis is based on finding the motile trichomonads on wet preparation or in urine.
Treatment is with metronidazole.
n
A discharge with significant leukocytes that does not include yeast, clue cells, or
Trichomonas may be due to mucopurulent cervicitis (MPC).
3. A sexually active young man presents with dysuria. How likely is it that it
resulted from a urinary tract infection?
About as likely as getting gonorrhea from sitting on a toilet seat. Dysuria in young men almost
always is due to urethritis from an STD. The urinalysis will be positive for leukocytes, making
a urinalysis not helpful and confusing to the novice. The likely pathogens include gonorrhea,
Chlamydia, Ureaplasma, Trichomonas, and herpes simplex virus (HSV). A purulent discharge
most likely is caused by gonorrhea, whereas a mucoid discharge most likely is caused by
infection with Chlamydia. The patient should be tested for both of these pathogens. Chlamydia
also can infect the urethra of women, and they may present only with dysuria. Consider this
diagnosis in a woman with dysuria and no bacteria on urinalysis, and do a pelvic examination.
4. Are there any single-dose treatment regimens for uncomplicated chlamydial
infections?
Yes, a single 1-g dose of azithromycin is an effective treatment for lower tract chlamydial
infections, including urethritis and cervicitis. Single-dose therapy is not appropriate for upper
tract disease, such as epididymitis and pelvic inflammatory disease (PID) or in patients who
have had a recent chlamydial infection and may be a treatment failure. This simplified therapy
should lead to more effective treatment in noncompliant patients.
5. Are there suitable oral alternatives to parenteral therapy for gonorrhea?
Uncomplicated urethral, endocervical, or rectal gonorrheal infections can be treated adequately
with a single intramuscular (IM) injection of ceftriaxone (125 mg) or an equivalent third-
generation cephalosporin antibiotic such as cefixime (400mg). Fluoroquinolones are no longer
recommended for the treatment of gonorrheal infections given the high rates of resistance and
rise in fluoroquinolone-resistant Neisseria gonorrhoeae (QRNG).
6. What is the significance of finding mucopurulent cervicitis (MPC) in a woman
with lower abdominal pain?
The normal endometrial secretion, as noted on exit from the endocervical canal, should be
transparent. The presence of a mucopurulent secretion from the os, which may appear yellow
when viewed on a white cotton-tipped swab (positive Q-Tip sign), suggests MPC. MPC, most
commonly caused by gonorrhea or Chlamydia, is a precursor to upper genital tract infection.
7. How do I evaluate a sexually active young person who presents with
an acutely swollen, warm, painful right ankle?
This patient, with acute monarticular arthritis, should be presumed to have disseminated
gonococcal infection. This is a syndrome of gonococcal bacteremia that leads to peripheral

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION 341
manifestations of disease, including dermatitis, tenosynovitis, and septic arthritis.
Arthrocentesis should be done on the involved joint, and the fluid should be sent for Gram
stain, culture for gonococcus (GC) and regular aerobic cultures, and cell count. GC is
cultured from less than 50% of joints. A genitourinary examination must be done to culture
the cervix, rectum, and urethra as appropriate for GC. A patient suspected of having
disseminated gonococcal infection should be admitted initially and treated with parenteral
antibiotics (ceftriaxone, 25–50 mg/kg/day intravenously [IV] or intramuscularly in a single
daily dose for 7 days).
8. What are the most common causes of genital ulcers?
Genital ulcers can represent infection with HSV, chancroid, or syphilis. It is difficult to make a
diagnosis based solely on history and physical examination. Always ask about travel history
and exposure to prostitutes. Genital ulcers are an important risk cofactor for HIV
transmission.
n
HSV. Genital herpes due to HSV is the most common cause of genital ulcers in the United
States. Primary HSV infection results in severely ill patients who are toxic with fever,
malaise, and inguinal adenopathy. Diagnosis is made by viral culture or antigen testing.
HSV is a recurrent disease, and patients may shed the virus while they are asymptomatic.
It cannot be cured, but treatment with antiviral agents can shorten the duration of
symptoms. Long-term suppressive therapy can prevent outbreaks of ulcers.
n
Chancroid. Also called soft sore, this disease is caused by Haemophilus ducreyi, a
bacterium that is difficult to culture. Clinically, this syndrome causes a painful nonindurated
papule that erodes into an ulcer. Painful inguinal adenopathy is found in more than 50% of
cases. Treatment options include single-dose azithromycin or ceftriaxone or 3 days of
ciprofloxacin or 1 week of erythromycin.
n
Syphilis. Primary syphilis presents with a painless indurated ulcer called a chancre.
Diagnosis is best made by dark-field examination for spirochetes, although this is usually
available only in public health laboratories. A Venereal Disease Research Laboratory (VDRL)
test should be done on anyone with possible syphilis. Treatment for primary syphilis is
penicillin G benzathine, 2.4 million U intramuscularly.
9. What is the Jarisch-Herxheimer reaction?
After initiation of treatment for syphilis, onset of fever, chills, myalgias, headache,
tachycardia, increased respirations, increased neutrophil count, and mild hypotension. This
occurs approximately 2 hours after initiation of treatment with peak temperatures at
approximately 7 hours, with defervescence at 12 to 24 hours. This reaction occurs in 50% of
primary syphilis, 90% of secondary syphilis, and 25% of early latent syphilis patients. In
secondary syphilis patients, the mucocutaneous lesions may become more edematous and
erythematous.
10. Proctitis is a problem primarily seen in men who have sex with men. Discuss
the approach and treatment.
Any individual, male or female, with the onset of acute proctitis symptoms (e.g., rectal
pain, discharge, tenesmus) who recently has had unprotected, receptive anal intercourse is
at risk for an STD-related problem. These patients should be examined by anoscopy and
should be tested for gonorrhea, Chlamydia, and HSV. All patients should have serologic
testing for syphilis. These patients should have empirical treatment for gonorrhea and
Chlamydia. If ulcers are apparent on anoscopy, consider empirical antiviral therapy with
acyclovir.
11. Do I need to report STD cases to the health department?
Yes. Accurate reporting of STDs is essential to national and local STD control efforts. HIV,
gonorrhea, and syphilis are reportable infections in every state. Chlamydial infection is
reportable in most states. It is the responsibility of each clinician to know his or her local
reporting requirements. If you are unsure of what to report about a specific patient, contact
your local health department.
Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION342
12. What are the important points to address in the discharge instructions for
STD patients?
a. Education about STDs is the responsibility of every ED physician because you may be the
only contact the patient has with the medical system.
b. Instruct patients to refer all their sexual partners for evaluation and treatment. Some
physicians in the United States routinely provide additional antibiotic prescriptions for
sexual partners. Although it is well intentioned, it is controversial to provide a prescription
for a person you have not interviewed or examined. That person may be allergic to the
medication or may have additional infections that you are not treating.
c. All patients should be instructed to avoid sexual contact with their partners until all parties
have finished treatment. Because it is unrealistic to expect all patients to follow this advice,
explain the importance of using condoms with every sexual contact to avoid further
infections and to prevent infection with HIV.
13. What is the significance of HIV infection in patients seen in the ED?
Disease caused by HIV infection, ranging from asymptomatic infection to AIDS, with serious,
possibly life-threatening complications, is encountered commonly in the ED. Seroprevalence
among ED patients varies greatly, depending on the location and type of hospital. Among
inner-city ED patients, seroprevalence ranges from approximately 5% to 10%. Knowledge of
HIV infection and its related diseases is essential to diagnose and treat patients and to ensure
adequate protection of health care workers.
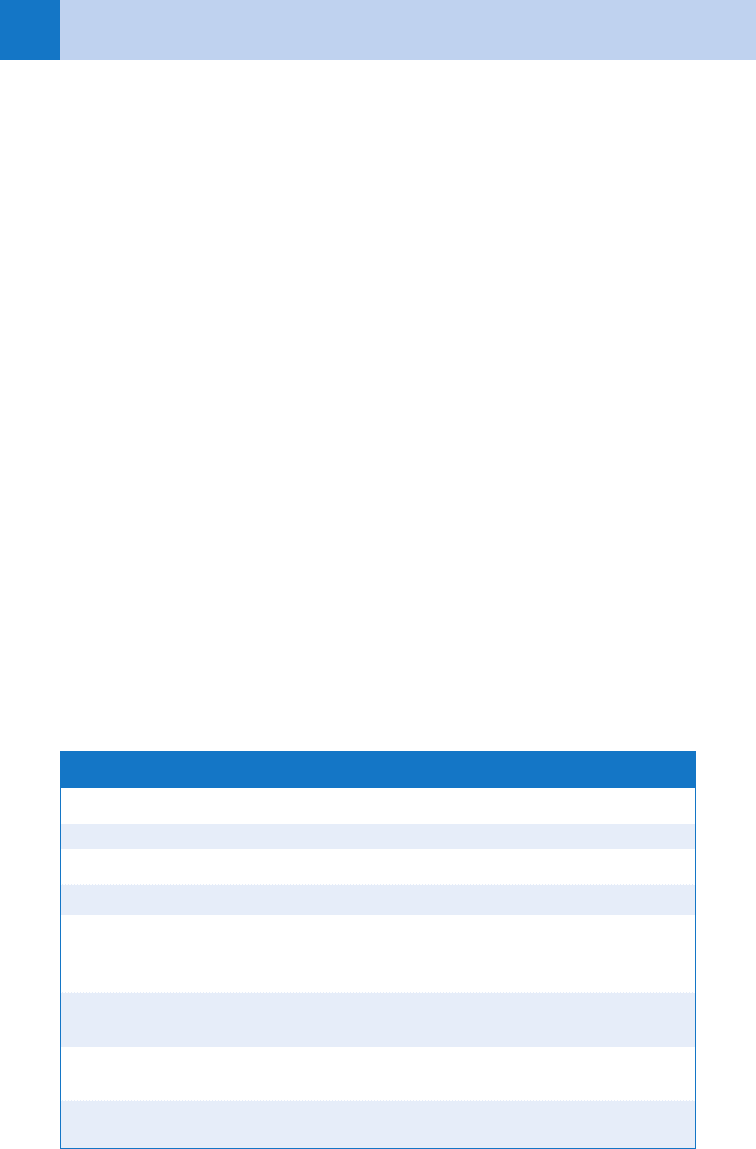
14. How is the diagnosis of AIDS made?
AIDS is diagnosed by laboratory evidence of HIV infection and the presence of one of the
AIDS-defining illnesses, some of which are listed in Table 49-1. HIV infection should be
suspected in all patients with known behavioral risk factors or with presenting symptoms
suggestive of an opportunistic infection. Questioning the patient directly about risk factors
may be crucial to diagnosing HIV-related disease. High-risk behaviors commonly associated
with HIV infection include unprotected sexual intercourse, unprotected insertive or receptive
sex between men, and injection drug use.
Laboratory evidence of HIV infection plus any of the following:
Esophageal candidiasis Brain lymphoma HIV wasting syndrome
Cryptococcosis Mycobacterium avium complex Disseminated histoplasmosis
Cryptosporidiosis Pneumocystis carinii pneumonia Isosporiasis
Cytomegalovirus Progressive multifocal Disseminated Mycobacterium
retinitis leukoencephalopathy
tuberculosis disease
Herpes simplex virus Brain toxoplasmosis Recurrent Salmonella
septicemia
Kaposi’s sarcoma HIV encephalopathy CD4 lymphocyte count
,200/mL
Pulmonary tuberculosis Invasive cervical cancer
TABLE 49-1. AIDS-DEFINING CONDITIONS

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION 343
15. Should EDs test for HIV infection?
Testing for HIV has not been traditionally performed in the ED because of difficulty in
maintaining confidentiality and ensuring appropriate reporting and counseling. An increasing
number of EDs are now performing HIV testing, recognizing that integrating HIV testing into
ED operations is possible. The most common HIV testing approach is diagnostic testing
(i.e., where physicians are able to test patients based on clinical signs or symptoms), although
others, including the CDC, have advocated for performing routine opt-out rapid HIV screening.
Several rapid tests are available that are highly accurate and have quick turn-around times.
Reactive rapid tests should be confirmed on an outpatient basis by performing an enzyme-
linked immunoassay (EIA) and a Western blot (WB). Regardless of whether or not HIV testing
is performed in the ED, outpatient referral for high-risk patients is appropriate.
16. How do patients with HIV infection present to the ED?
Patients may present with involvement of virtually any organ system. HIV infection should be
suspected in any patient thought to be immunocompetent but with an infectious disease
(e.g., community-acquired pneumonia or cellulitis in an otherwise healthy adult), those with
unexplained leukopenia or lymphopenia, and those who present with chronic symptoms (e.g.,
weight loss, fever, or diarrhea) or with symptoms of opportunistic infection. Among patients with
HIV infection, systemic infection, or malignancy always must be considered and may present
with malaise, anorexia, fever, weight loss, gastrointestinal (GI) complaints, or other symptoms.
Because of the wide spectrum of disease related to HIV infection, many specific diagnoses
cannot be made definitively in the ED; treatment focuses on recognition of disease, institution of
initial therapy, and admission to the hospital or close outpatient follow-up.
17. What tests should be done for the HIV-infected patient with systemic
symptoms?
In addition to a complete history and physical examination, appropriate laboratory
investigations may include electrolytes, complete blood count, blood cultures (i.e., aerobic,
anaerobic, and fungal), urinalysis and culture, lactate dehydrogenase, liver function tests,
chest radiography, serologic testing for syphilis, blood tests for cryptococcal antigen, and
Toxoplasma and Coccidioides serologies. Lumbar puncture also may be appropriate if no
other source of fever is identified.
18. Explain the significance of fever in patients with HIV infection.
Fever may indicate bacterial, fungal, viral, or protozoal infection. The most common causes of
fever include HIV-related fever, systemic infections such as Mycobacterium avium complex,
cytomegalovirus, Hodgkin’s disease, and non-Hodgkin’s lymphoma.
Many HIV-infected patients with fever may be managed as outpatients, although this will
depend heavily on the patient’s CD4 count. A CD4 count less than 200 cells/uL defines AIDS,
and these patients should be hospitalized for further evaluation. Patients with high CD4 counts
(e.g., .350 cells/uL) may be managed as an outpatient if the patient appears clinically well.
Outpatient management may be attempted if the fever source is found and does not dictate
admission, if appropriate laboratory studies have been initiated, if the patient is able to
function adequately at home (able to ambulate and tolerate oral intake), and if appropriate
close medical follow-up can be arranged.
19. What are the common neurologic complications of AIDS?
The most common acute symptoms are altered mental status, seizures, and headache.
Because these patients are immunosuppressed, they commonly do not manifest symptoms
thought to be associated with central nervous system (CNS) infections. For example,
meningismus is rare and patients with meningitis may only present with mild headache.
ED evaluation should include a complete neurologic examination and, when appropriate,
computed tomography (CT) or magnetic resonance imaging (MRI), and lumbar puncture.
Specific cerebrospinal fluid studies that may be of value include cell count, glucose,

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION344
protein, Gram stain, cryptococcal antigen bacterial culture, viral culture, fungal culture,
Toxoplasma and cryptococcal antigen, and coccidioidomycosis titer. The most common
causes of neurologic symptoms include Cryptococcus neoformans, Toxoplasma gondii,
HIV encephalopathy, and CNS lymphoma.
20. What is HIV encephalopathy?
Also referred to as AIDS dementia, it is an organic brain syndrome manifested by decline in
attention, cognitive reasoning, speech, motor function, and motivation. HIV encephalopathy is
the most common neurologic problem and affects 33% to 60% of patients. It may be the
presenting sign of overt AIDS in 25% of patients. Other causes of dementia and altered mental
status must be ruled out.
21. What are the pulmonary complications of HIV infection? How are they
managed?
Common presenting pulmonary complaints are cough, hemoptysis, shortness of breath, and
chest pain. After history and lung examination, arterial blood gases, chest radiography,
sputum culture, Gram stain, acid-fast stain, and blood cultures should be obtained if clinically
indicated. The most common pulmonary infection is Pneumocystis carinii pneumonia, which
occurs in 70% to 80% of seropositive patients and typically presents with dyspnea, dyspnea
with exertion, nonproductive cough, fever, and weight loss. Rapid institution of therapy with
IV trimethoprim-sulfamethoxazole (TMP-SMX), based on weight for dosing (dapsone or
pentamidine if TMP-SMX allergic), and oral steroids may prevent excessive morbidity and
mortality. Other causes include Mycobacterium tuberculosis pneumonia, Histoplasma
capsulatum, other traditional community-acquired pneumonia organisms, and neoplasm.
ED management includes administration of supplemental oxygen, volume repletion if
indicated, and antibiotic therapy. Admission should be considered for patients with new-onset
pulmonary symptoms or patients with a significant deterioration in respiratory status.
Patients with Pneumocystis pneumonia should be treated with intravenous TMP-SMX,
15 to 20 mg/kg/day in divided doses. Alternate treatments may be used with primaquine plus
clindamycin, or atovaquone, or pentamidine. Patients with hypoxemia (pO
2
,70) or a large
Aa gradient (.35) should also be treated with corticosteroids (such as prednisone taper of
40 mg twice daily for 5 days followed by prednisone 40 mg daily for 5 days followed by
prednisone 20 mg daily for 11 days).
22. How should GI complaints be managed?
Approximately 50% of AIDS patients present with GI complaints at some time during their
illness. Esophageal complaints are common and may be most commonly caused by Candida
esophagitis or herpes simplex esophagitis. Patients with esophagitis should receive a
2-week empiric course of oral antifungal agents, followed by endoscopy if not successfully
treated. The most common presenting symptoms are abdominal pain, bleeding, and
diarrhea. Diarrhea is the most common GI complaint and is estimated to occur in 50% to
90% of AIDS patients. Helpful laboratory studies include microscopic examination of stool
for leukocytes, acid-fast stain, examination for ova and parasites, and bacterial culture of
stool and blood. Cryptosporidium and Isospora infections in particular are common causes
and are associated with prolonged watery diarrhea. Other common infectious agents include
Candida, Kaposi’s sarcoma, M. avium complex, HSV, cytomegalovirus, Campylobacter
jejuni, Entamoeba histolytica, Shigella, Salmonella, Giardia, Cryptosporidium, and Isospora.
Management should be directed at repletion of fluid and electrolytes and appropriate
antibiotic coverage.
23. What are the common cutaneous presentations of AIDS and how are they
treated?
Kaposi’s sarcoma is the most common unique cutaneous manifestation of AIDS. Usually it is
widely disseminated and may involve mucous membranes. Exacerbation of underlying
dermatologic conditions is common in the HIV-infected population. Complaints such as

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION 345
xerosis (dry skin) and pruritus are common and may be manifested before development of
opportunistic infections. Xerosis may be treated with emollients and, if necessary, with mild
topical steroids. Pruritus may respond to oatmeal baths and, if necessary, antihistamines.
Infections, including Staphylococcus aureus (presenting as bullous impetigo, ecthyma, or
folliculitis), Pseudomonas aeruginosa (which may present with chronic ulcerations and
macerations), herpes simplex, herpes zoster, syphilis, and scabies are common and should be
treated with standard therapies.
Other dermatologic conditions that occur with increased frequency in HIV-infected patients
include seborrheic dermatitis, psoriasis, atopic dermatitis, and alopecia. Dermatologic
consultation generally is indicated. Admission may be indicated for patients with any
disseminated cutaneous infection requiring IV antibiotics or antiviral agents.
24. Describe ophthalmologic emergencies that occur in AIDS patients.
Eye complaints such as change in visual acuity, photophobia, redness, and pain are common
and may represent retinitis or invasion of eye or periorbital tissues with a malignant or
infectious process. Cytomegalovirus retinitis occurs in 30% of AIDS patients and accounts for
most retinitis among AIDS patients. It has a characteristic appearance of fluffy white retinal
lesions, often perivascular (sometimes referred to as “tomato and cheese pizza” appearance).
Ophthalmology consultation is indicated, followed by treatment with foscarnet or ganciclovir
for 2 weeks and long-term maintenance therapy.
25. Should HIV-infected patients receive tetanus and other immunizations?
According to the U.S. Public Health Service Immunizations Practices Advisory Committee,
routine immunization recommendations for diphtheria (DPT); tetanus (Td); and measles,
mumps, and rubella (MMR) are unchanged for HIV-infected patients. Smallpox and polio
vaccines are not recommended in the HIV-infected population.
26. How should symptoms of side effects from drugs be managed?
Reactions to pharmacologic therapy are common in HIV-infected patients and always must
be considered as the cause of new symptoms. In one study, 30% of hospitalized patients
with HIV disease had an identified probable or definite adverse drug reaction. The most
common type of reaction was cutaneous. Certain commonly used pharmaceutical agents
cause a particularly high incidence of adverse drug reactions, including TMP-SMX, which has
a 65% incidence of adverse drug reactions in AIDS patients, and pentamidine, which has a
50% incidence of adverse reactions. A decision about discontinuing therapy depends on
balance between the benefit of the drug and the severity of side effects.
27. How can health care providers protect themselves from acquiring HIV?
Health care workers often are exposed to HIV-infected patients and their body fluids.
Precautions in handling potentially infectious fluids are crucial. Because HIV infection is
often undiagnosed at the time of the ED encounter, the use of universal precautions is
imperative and should be performed without exception, including the appropriate use of
gown, gloves, mask, and goggles for procedures performed in all patients. The Needlestick
Safety and Prevention Act of 2000 mandates that safety-engineered devices be used
whenever possible and that institutions maintain exposure control plans. With the use of
universal precautions, the risk of acquiring HIV infection by occupational exposure is
extremely low.
28. What constitutes high-risk exposure to HIV?
n
Substantial risk from nonoccupational exposures are those from an HIV-infected source
with blood, semen, vaginal or rectal secretions, breast milk, or any body fluids with visible
blood, through the vagina, rectum, eye, mouth, or other mucous membrane, nonintact skin,
or percutaneous contact.
n
For occupational exposures, higher-risk percutaneous exposures associated with an
increased likelihood of transmission include deep injuries, visible blood on a device, and
Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION346
www.cdc.gov/std/hpv/STDFact-HPV-vaccine-young-women.htm
www.cdc.gov/std/treatment
www.ucsf.edu/hivcntr/PEPline/index.html
injuries sustained when placing a catheter in a vein or artery. Percutaneous exposures
that are superficial or involve solid needles are considered lower-risk exposures. High-
risk sources are patients with symptomatic HIV, AIDS, acute seroconversion, or high viral
load. Patients with asymptomatic HIV or viral load ,15,000 copies/mL are considered
lower risk.
29. Should postexposure prophylaxis (PEP) be administered after exposure to
blood and body fluids?
PEP should be considered following all occupational and nonoccupational exposures.
Decisions to treat should be based on the type of exposure, the risk of HIV in the source
patient, and careful consideration of the risks and benefits of therapy. PEP is most effective if
administered within 30 minutes of the exposure. PEP may consist of a basic regimen (such as
zidovudine plus lamivudine) or an expanded regimen for high-risk exposures (such as
zidovudine, lamivudine plus either indinavir or nelfinavir). Ideally, each health care institution
should have written protocols that are formulated in consultation with occupational medicine
and infectious disease specialists for occupational exposures in health care workers and
patients with nonoccupational exposures.
30. What is highly active antiretroviral therapy (HAART)?
HAART is recommended for HIV-infected patients with CD4 counts less than 200 cells/uL or
those with symptomatic disease. The use of HAART has led to significant reductions in
morbidity and mortality. HAART should be prescribed by infectious disease specialists and
typically includes nonnucleoside reverse transcriptase inhibitors (NNRTIs) such as efavirenz,
nucleotide reverse transcriptase inhibitors (NRTIs) such as zidovudine or lamivudine, and
protease inhibitors such as lopinavir or ritonavir. Adverse reactions to HAART are common
and may include bone marrow suppression, cutaneous reactions, GI distress, jaundice,
nephrolithiasis, abnormal lipid profiles, neuropathy, and others.
KEY POINTS: SEXUALLY TRANSMITTED DISEASES
1. STDs affect 19 million people a year in the United States.
2. Single-dose therapy for Chlamydia and GC is effective for treatment of uncomplicated
cervicitis and urethritis.
3. The most common causes of genital ulcers include herpes simplex, chancroid (H. ducreyi),
syphilis, and HPV.
4. Patients with suspected Pneumocystis pneumonia should be treated with TMP-SMX
(weight-based) and corticosteroids (if hypoxic).
5. All patients with high-risk HIV exposure should be considered for postexposure prophylaxis
therapy.
WEBSITES

Chapter 49 SEXUALLY TRANSMITTED DISEASES AND HIV INFECTION 347
BIBLIOGRAPHY
1. Bonacini M: Medical management of benign oesophageal disease in patients with human immunodeficiency
virus infection. Dig Liver Dis 33:294, 2001.
2. Carpenter CC, Cooper DA, Fischl MA, et al: Antiretroviral therapy in adults: updated recommendations of the
International AIDS Society-USA Panel. JAMA 283:381, 2000.
3. CDC National AIDS Hotline: 1-800-342-2437.
4. CDC Sexually Transmitted Diseases Treatment Guidelines, 2006.
5. Center for Disease Control and Prevention: Revised recommendations for HIV testing of adults, adolescents,
and pregnant women in health-care settings 2006. MMWR 55: 1–17, 2006.
6. Centers for Disease Control and Prevention: Sexually transmitted diseases treatment guidelines 2006.
MMWR 55, 2006.
7. Centers for Disease Control and Prevention. Update to CDC’s sexually transmitted diseases treatment
guidelines, 2006. Fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR,
2007; 56:332–336.
8. Hall HI, Ruiguang S, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA 300:520–529,
2008.
9. Harb GE, Alldredge BK, Coleman R, et al: Pharmacoepidemiology of adverse drug reactions in hospitalized
patients with human immunodeficiency disease. J Acquir Immune Defic Syndr 6:919–926, 1993.
10. Kendrick SR, Kroc KA, Couture E, et al: Comparison of point-of-care rapid HIV testing in three clinical venues.
AIDS 18:2208–2210, 2004.
11. McKenna M: HIV testing: should the emergency department take part? Ann Emerg Med 49: 190–192, 2007.
12. Moran GJ: Emergency department management of blood and body fluid exposures. Ann Emerg Med 35:47,
2000.
13. Palacio H, Li X, Wilson TE, et al: Healthcare use by varied highly active antiretroviral therapy (HAART) strata:
HAART use, discontinuation, and naivety. AIDS 18:621–630, 2004.
14. Rothman RE: Current Centers for Disease Control and Prevention guidelines for HIV counseling, testing, and
referral: critical role of a call to action for emergency physicians. Ann Emerg Med 44:21–42, 2004.
15. Rothman RE, Ketlogetswe KS, Dolan T, et al: Preventive care in the emergency department: should emergency
departments conduct routine HIV screening? A systematic review. Acad Emerg Med 10:278–285. 2003.
16. Smith DK, Grohskopf LA, Black RJ: US Department of Health and Human Services. Antiretroviral
postexposure prophylaxis after sexual, injection-drug use, or other nonoccupational exposure to HIV in
the United States: Recommendations from the US Department of Health and Human Services. MMWR 54
(RR-2):1–19, 2005.
17. Thomas CF, Limper AH: Pneumocystis pneumonia. N Engl J Med 350:2478–2498, 2004.
18. Wei LL, Park SS, Skiest DJ: Prevalence of visual symptoms among patients with newly diagnosed
cytomegalovirus retinitis. Retina 22:278, 2002.
19. Yeni PG, Hammer SM, Hirsch MS, et al: Treatment for adult HIV infection: 2004 recommendations of the
International AIDS Society-USA Panel. JAMA 292:251–265, 2004.