Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

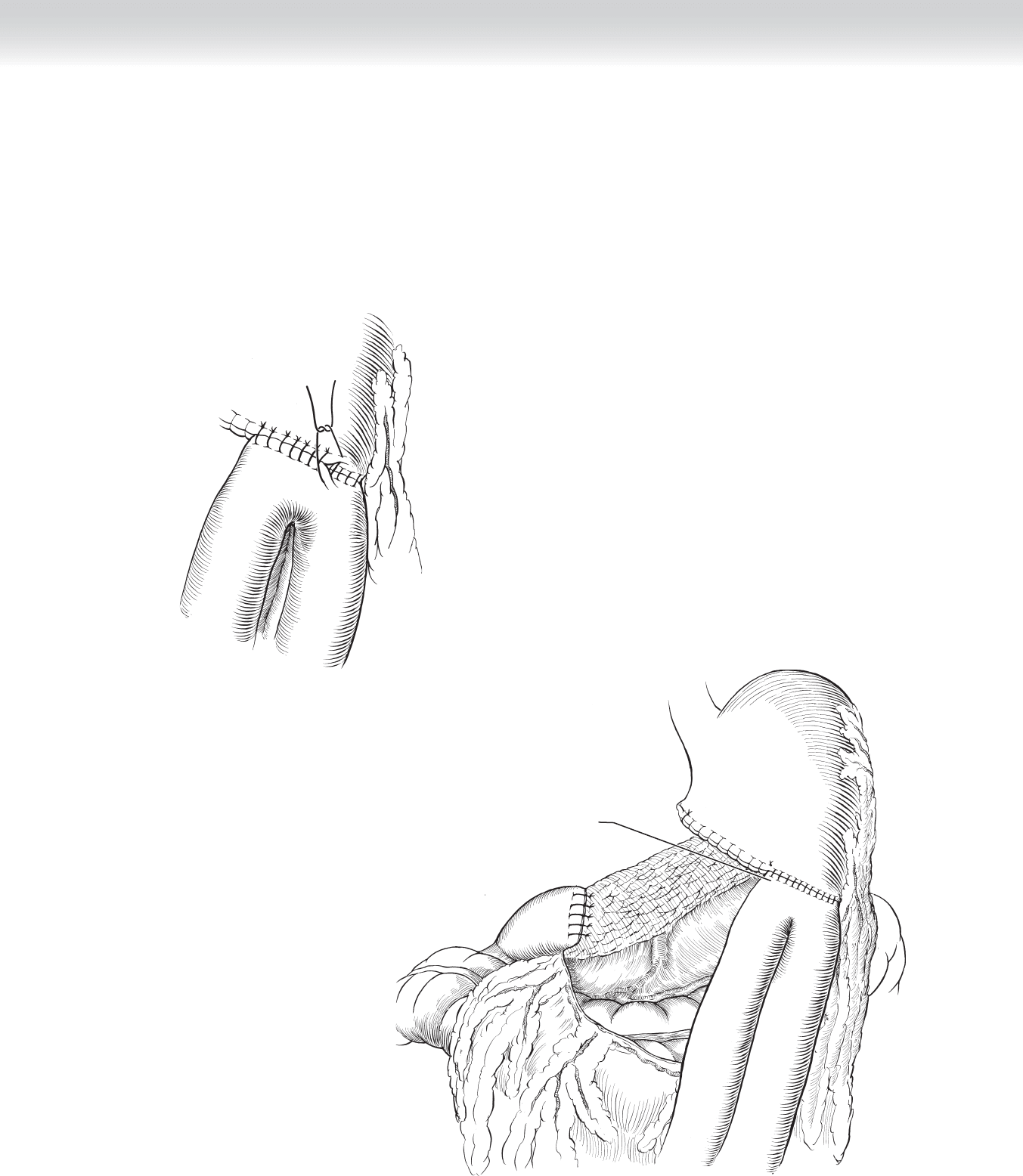
◆ The anastomosis is then completed anteriorly using interrupted 3-0 silk sutures placed in a
Lembert fashion (Figure 27-11).
◆ Figure 27-12 demonstrates the completed Billroth II anastomosis (Hofmeister method).
FIGURE 27–11
Gastrojejunal
anastomosis
FIGURE 27–12
CHAPTER 27 • Gastric Resection: Billroth II 299
300 Section IV • The Abdomen
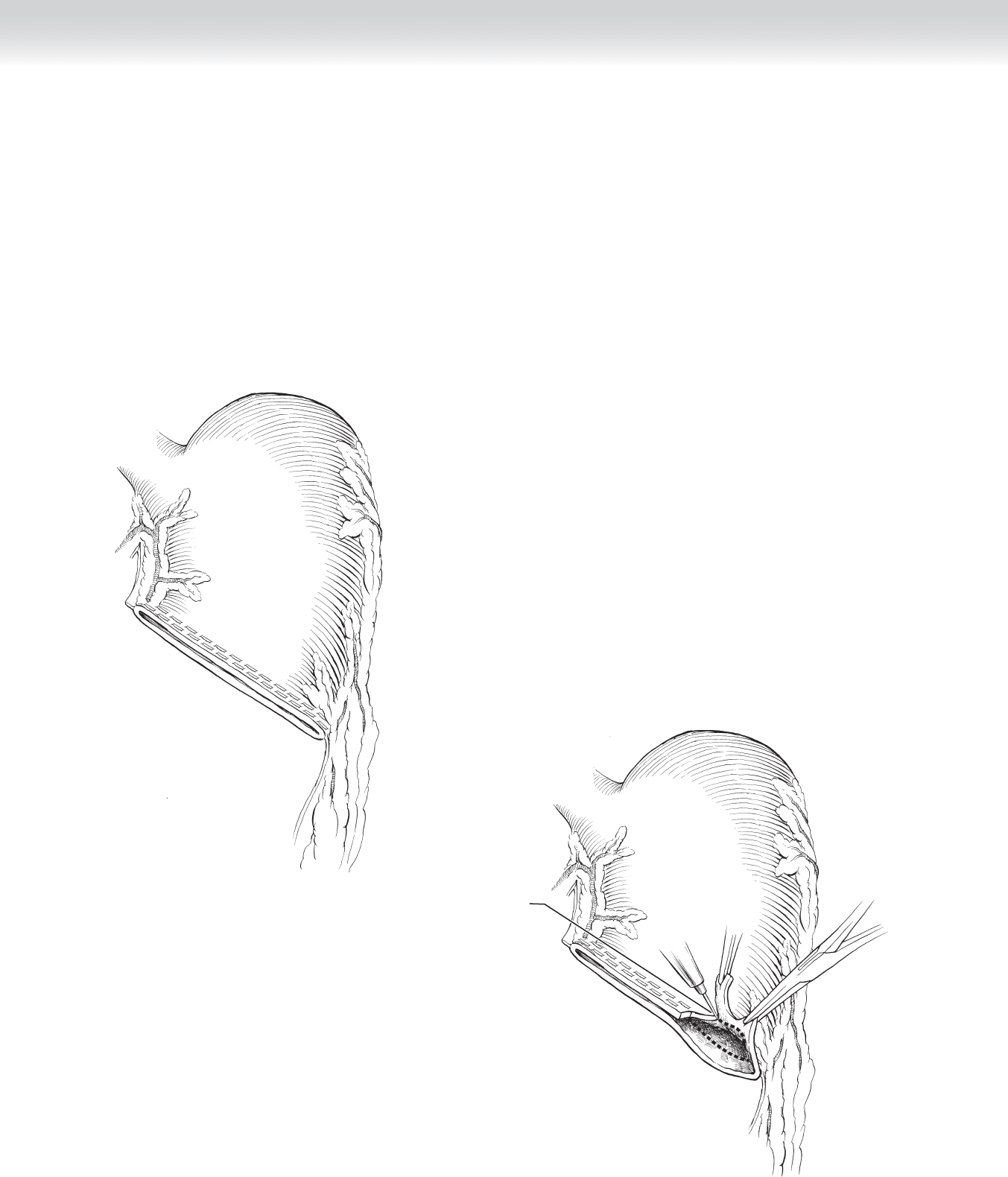
◆ Figure 27-13 shows the stapled end of the stomach, and in preparation for the gastrojejunal
anastomosis, the end adjacent to the greater curvature is opened using electrocautery and
excess gastric tissue is trimmed (Figure 27-14).
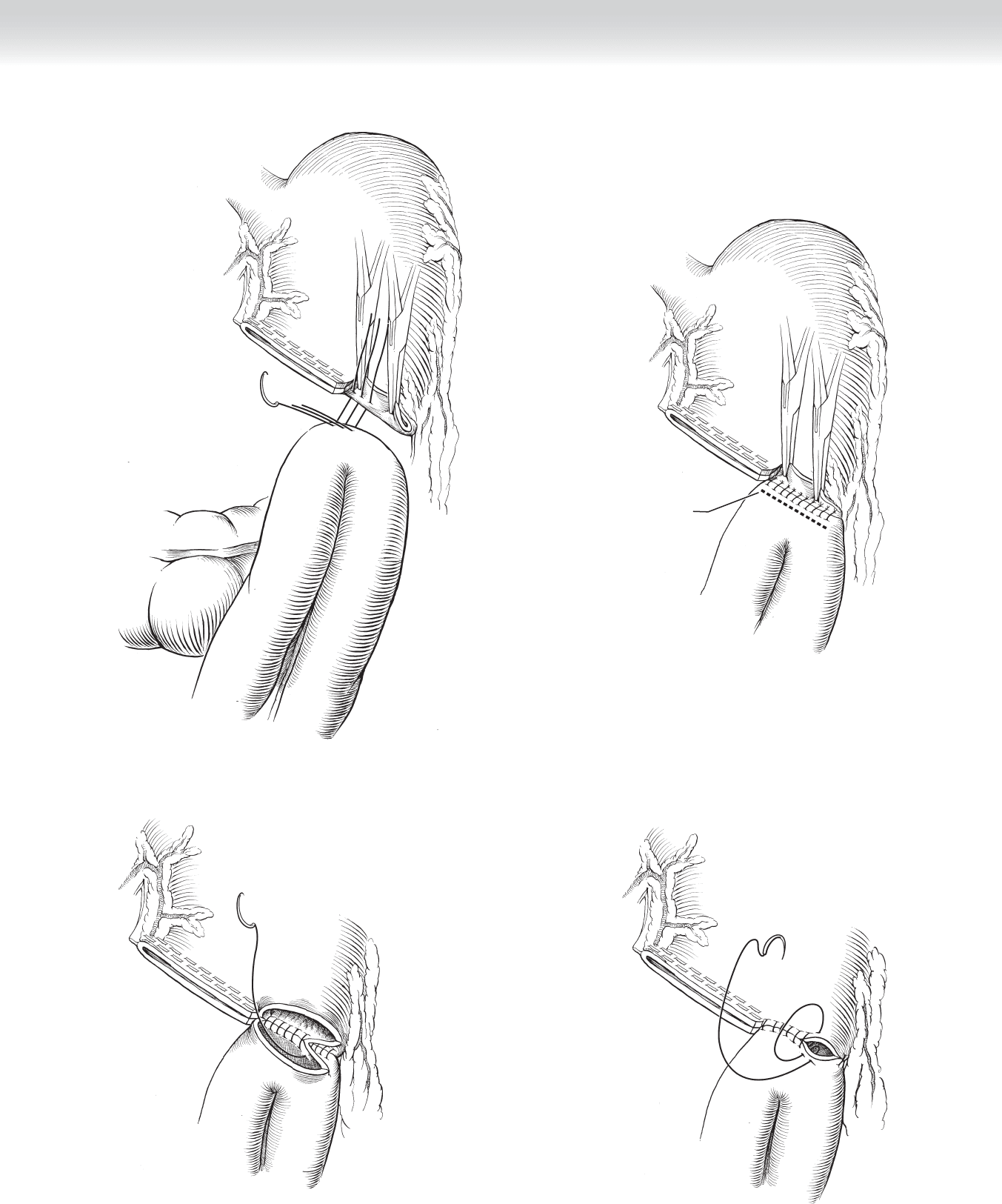
◆ The gastrojejunal anastomosis is performed as previously described in two layers with an
outer layer of 3-0 silk (Figure 27-15), followed by opening the jejunum at the dashed line
(Figure 27-16) and performing the inner layer of the anastomosis in a running fashion
using a 3-0 nonabsorbable suture (Figure 27-17), which is carried anteriorly in a Connell
fashion (Figure 27-18).
FIGURE 27–13
Removing excess
gastric tissue
FIGURE 27–14
CHAPTER 27 • Gastric Resection: Billroth II 301
Incision in jejunum
for anastomosis
FIGURE 27–16
FIGURE 27–17
FIGURE 27–18
FIGURE 27–15
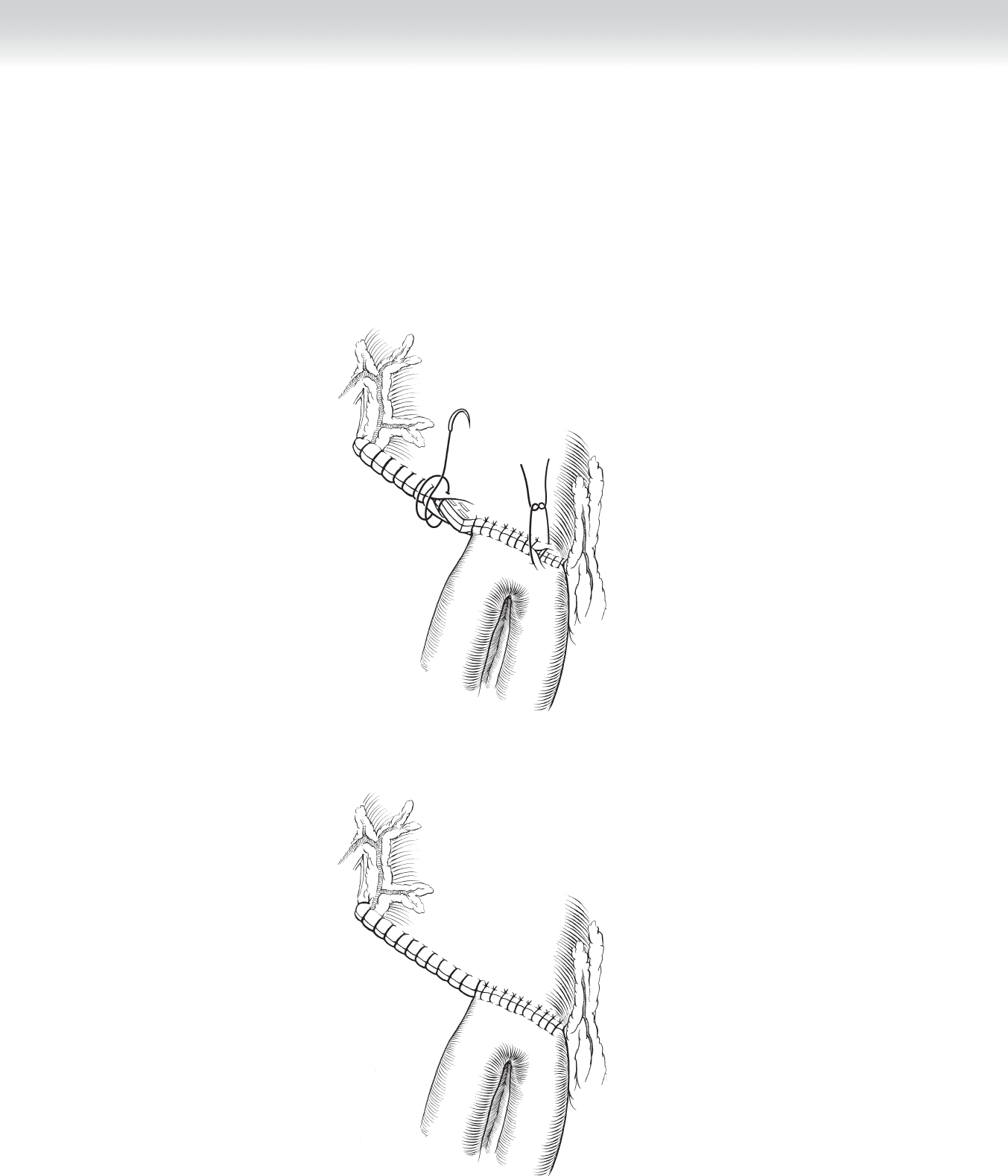
◆ The anterior suture line is then oversewn using 3-0 silk interrupted sutures, and likewise,
the staple line is oversewn using running nonabsorbable sutures (Figure 27-19).
◆ Figure 27-20 demonstrates the completed Billroth II anastomosis.
FIGURE 27–19
FIGURE 27–20
Section IV • The Abdomen302

3. CLOSING
◆ The upper midline or subcostal incision is closed in the usual fashion.
STEP 4: POSTOPERATIVE CARE
◆ A nasogastric tube is positioned proximal to the suture line, and once bowel function has
resumed the nasogastric tube can be removed and a liquid diet started. If there is no gastric
retention, the diet can be rapidly advanced.
STEP 5: PEARLS AND PITFALLS
◆ In performing the Billroth II anastomosis, some surgeons prefer to use the Polya method,
which uses the entire gastric opening for the gastrojejunal anastomosis. The choice between
a Hofmeister or Polya method depends on the surgeon’s preference.
◆ In operations for cancers of the stomach, most surgeons prefer the Billroth II anastomosis
because local recurrence of the cancer would tend to cause earlier obstruction of a gastro-
duodenostomy.
◆ In performing the Billroth II anastomosis, the choice of where the jejunal loop is brought
anterior to the transverse colon or brought posterior to the transverse mesocolon is also a
matter of the surgeon’s preference.
SELECTED REFERENCES
1. Mercer DW, Robinson EK: Stomach. In Townsend CM Jr (ed): Sabiston Textbook of Surgery: The Biological
Basis of Modern Surgical Practice, 18th ed. Philadelphia, Saunders, 2008, pp 1223-1277.
2. Thompson JC: Subtotal gastrectomy with stapled Billroth II anastomosis. In Thompson JC (ed): Atlas of
Surgery of the Stomach, Duodenum and Small Bowel. St Louis, Mosby-Year Book, 1992, pp 61-65.
CHAPTER 27 • Gastric Resection: Billroth II 303

304
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the vascular anatomy of the stomach is required, and
this is shown in Figure 26-1.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Total gastrectomies are performed predominantly for gastric cancer. Total gastrectomy is
now rarely performed for bleeding or Zollinger-Ellison syndrome, given the success with
current medical regimens.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ An upper midline incision carried inferior to the umbilicus, if needed, is commonly used for
total gastrectomy (Figure 28-1). As an alternative incision, some surgeons prefer a bilateral
subcostal incision, which affords excellent exposure to the stomach and distal esophagus.
2. DISSECTION
◆ Wide exposure is accomplished with various self-retaining retractors. A laparotomy pad is
placed under the liver, and the liver is gently retracted cephalad (Figure 28-2).
CHAPTER
28
Total Gastrectomy
B. Mark Evers
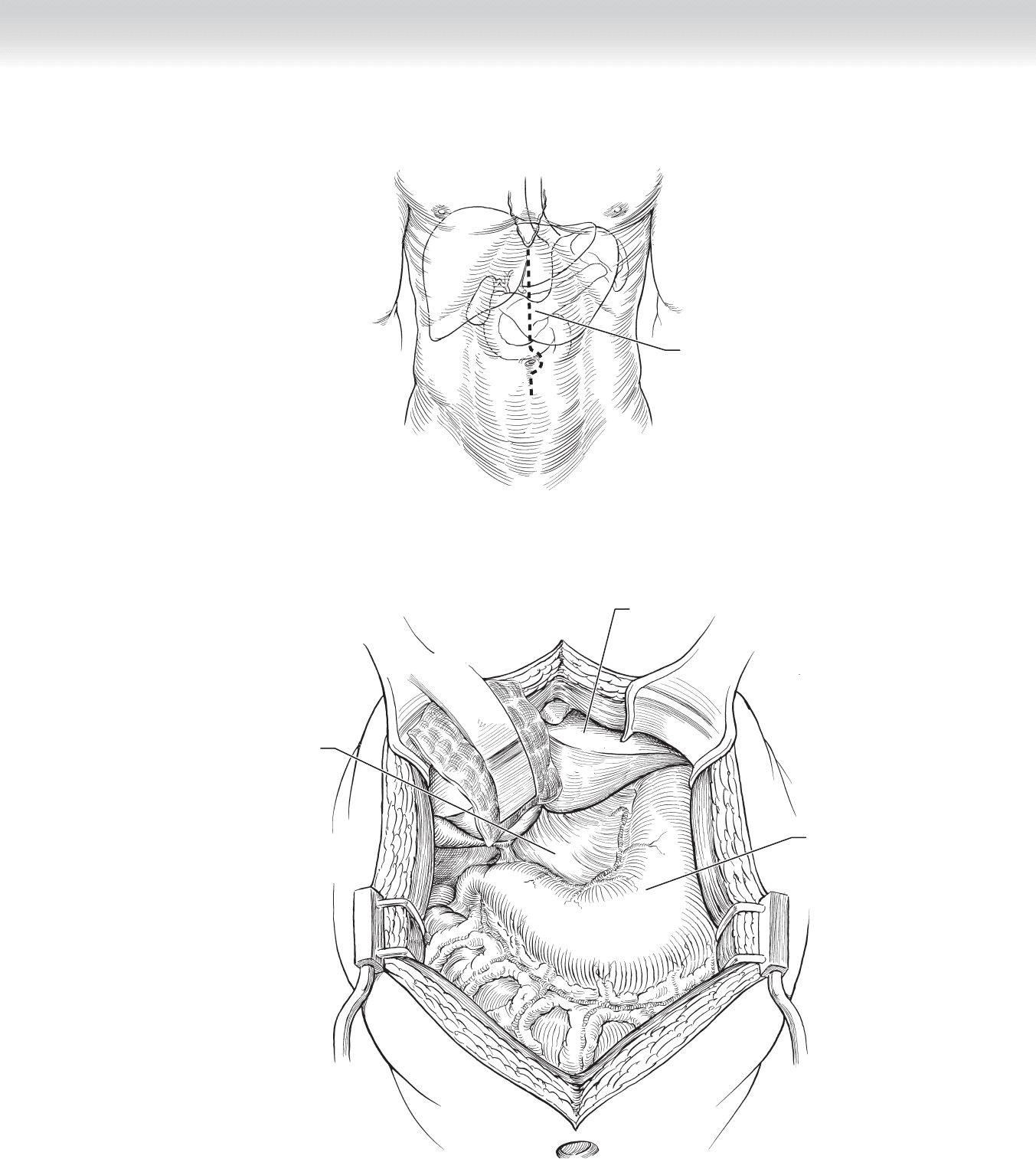
Midline
incision
FIGURE 28–1
Liver
Stomach
Gastrohepatic
ligament
FIGURE 28–2
CHAPTER 28 • Total Gastrectomy 305
306 Section IV • The Abdomen
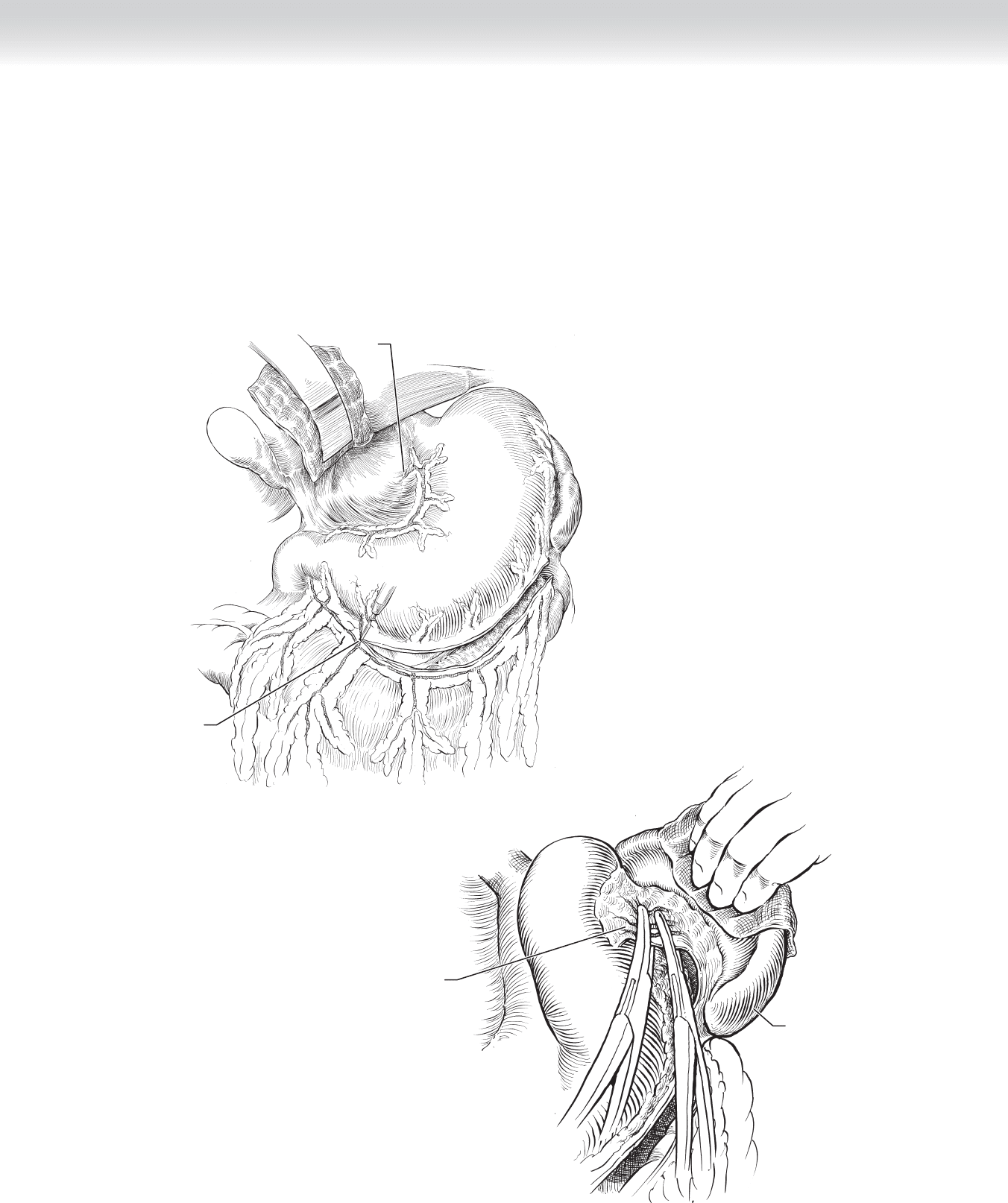
◆ The greater curvature of the stomach is mobilized by dividing the gastroepiploic vessels in
the gastrocolic ligament and ligating with silk sutures. Likewise, the lesser curvature is
mobilized by division of the gastrohepatic ligament (Figure 28-3, A).
◆ The short gastric vessels are divided between clamps and ligated with silk sutures. The spleen
is gently retracted laterally to clearly identify the short gastric vessels (Figure 28-3, B).
B
Dividing short
gastric vessels
Spleen
FIGURE 28–3
Incision through
omentum,
freeing stomach
A
Left gastric
artery
CHAPTER 28 • Total Gastrectomy 307
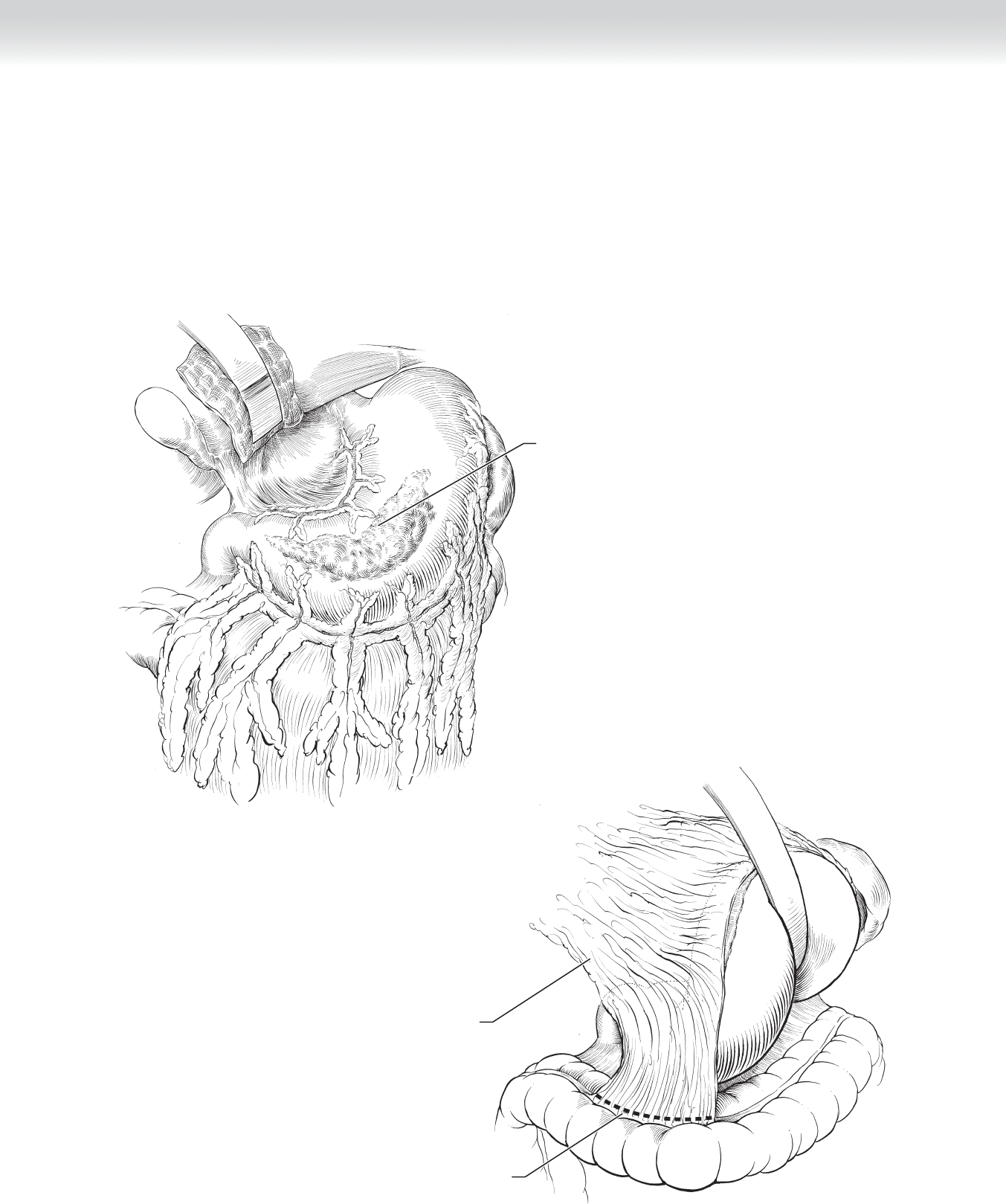
◆ As shown in Figure 28-4, the tumor is visualized in the distal and mid stomach.
◆ For an effective oncologic resection, the omentum is usually resected along with the stomach. The
omentum is divided at its attachment to the transverse colon and then retracted cephalad. The
stomach is likewise retracted cephalad to divide any remaining posterior attachments (Figure 28-5).
Incision through
omentum
Omentum swung
cephalad
FIGURE 28–5
Tumor
FIGURE 28–4
308 Section IV • The Abdomen
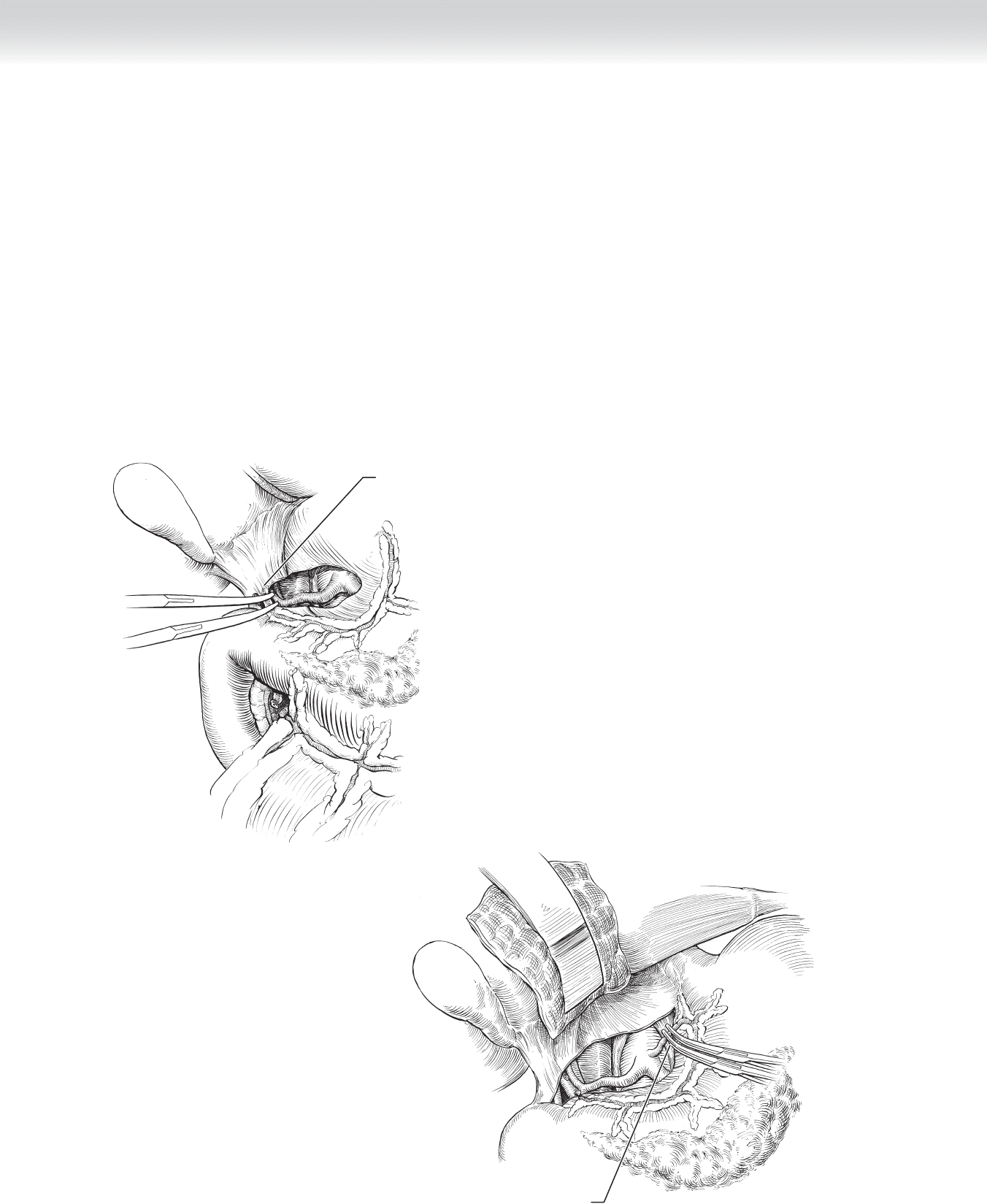
◆ Figure 28-6 demonstrates dividing the right gastric artery to allow complete mobilization
of the distal stomach and proximal duodenum.
◆ The division of the left gastric artery is accomplished for mobilization of the lesser curva-
ture and access to the distal esophagus (Figure 28-7).
◆ As shown in Figure 28-8, A, the duodenum is transected distal to the pylorus using a
gastrointestinal anastomosis (GIA) stapling device and, likewise, the distal esophagus is
transected using the GIA device proximal to the gastroesophageal junction. Figure 28-8, B
demonstrates suture closure of the duodenal stump, and Figure 28-8, C shows a stapled
closure of the stump. Interrupted sutures are then placed over either the running suture
(Figure 28-8, D) or the staple line (Figure 28-8, E).
Dividing left
gastric artery
FIGURE 28–7
Dividing right
gastric artery
FIGURE 28–6