Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 26 • Gastric Resection: Billroth I 289
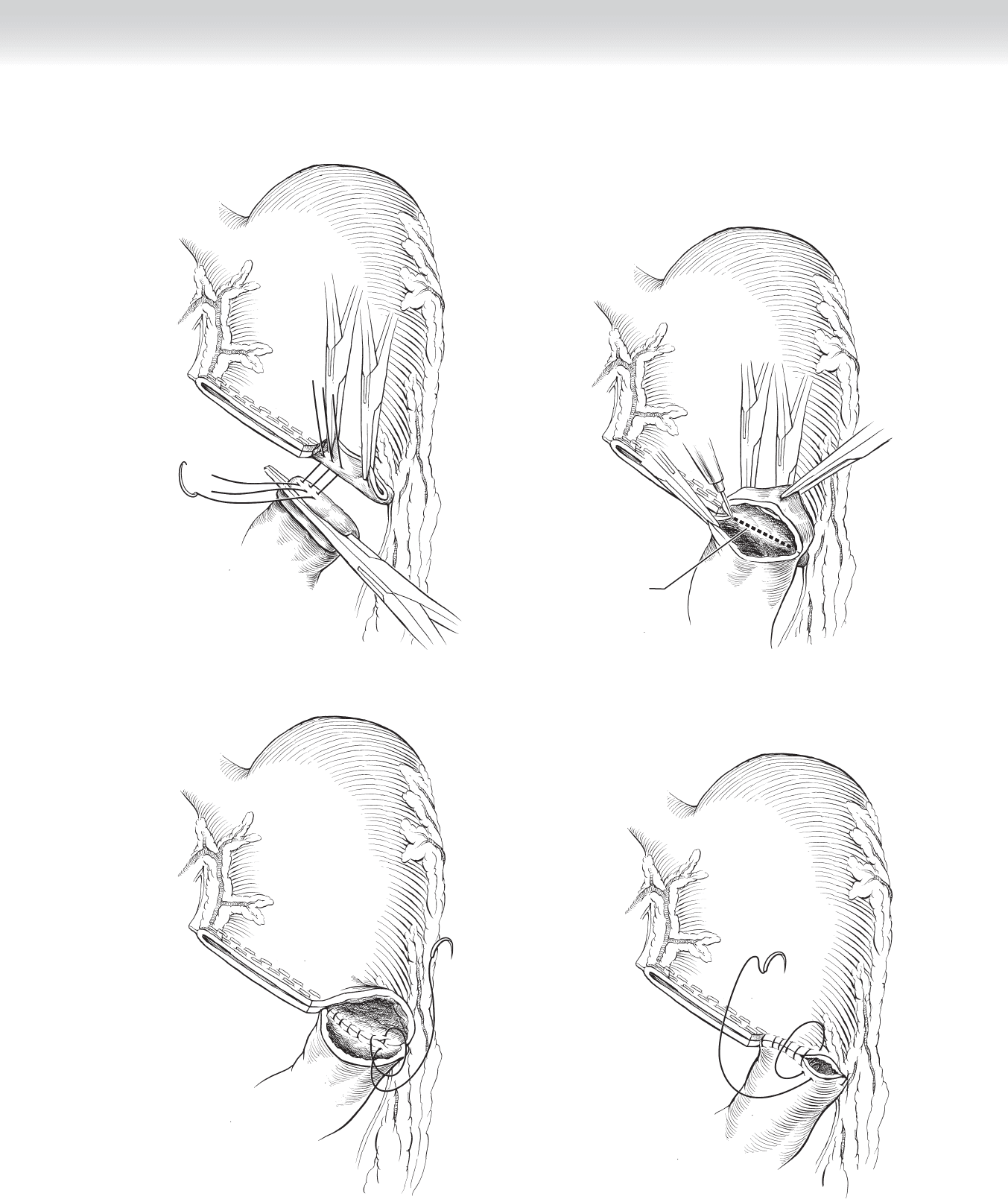
FIGURE 26 –18
Removing excess
duodenal tissue
FIGURE 26 –19
FIGURE 26 –20
FIGURE 26 –21
290 Section IV • The Abdomen
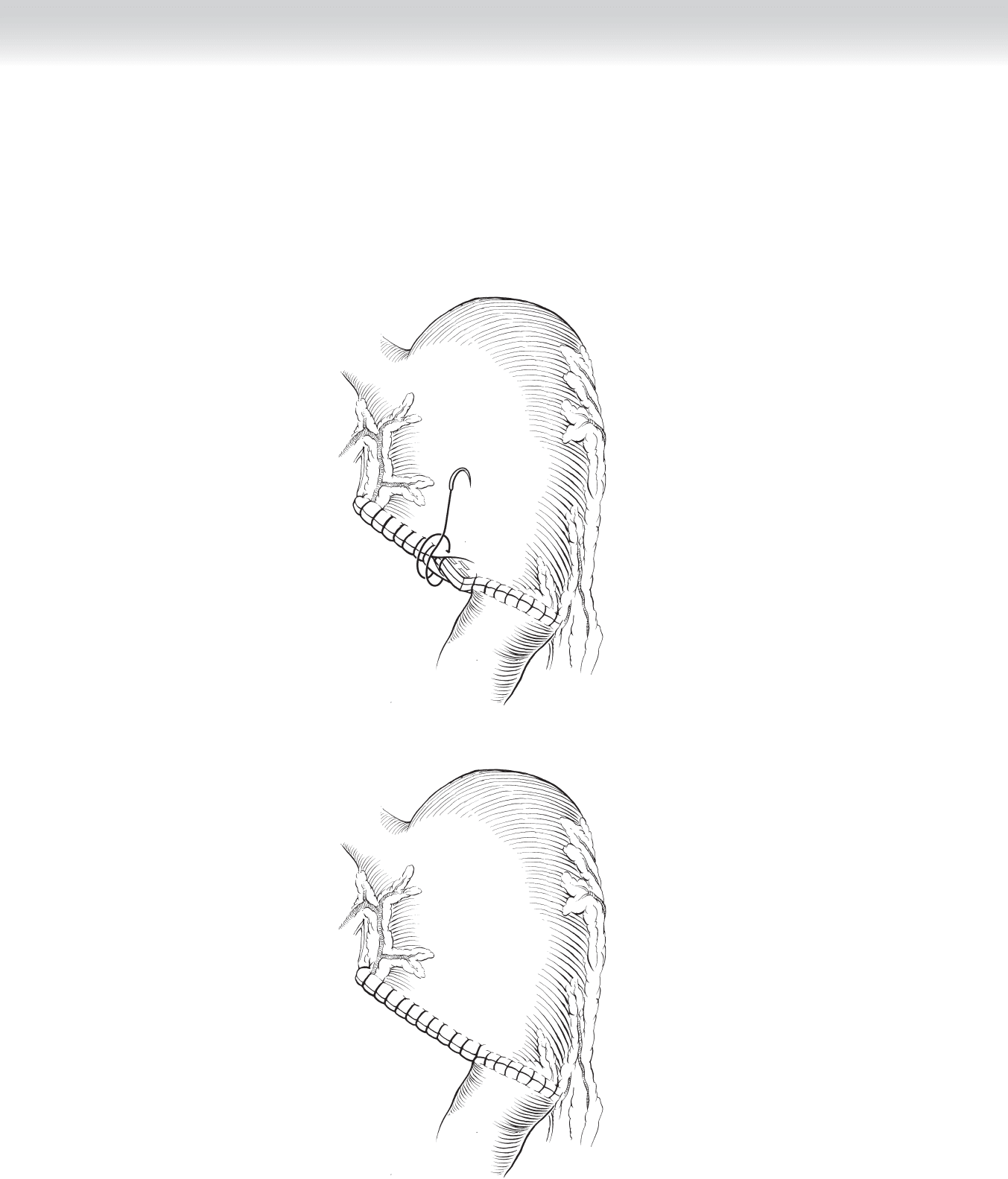
◆ The staple line is secured by running 3-0 silk sutures (Figure 26-22).
◆ Figure 26-23 shows the completed gastroduodenal anastomosis.
FIGURE 26 –22
FIGURE 26 –23

CHAPTER 26 • Gastric Resection: Billroth I 291
3. CLOSING
◆ The upper midline or subcostal incision is closed in usual fashion.
STEP 4: POSTOPERATIVE CARE
◆ Before closure, a nasogastric tube is positioned proximal to the suture line. When bowel
activity has resumed, the nasogastric tube can be removed and clear liquids initiated. If
there is no evidence of gastric retention, the feeding regimen can be progressed.
STEP 5: PEARLS AND PITFALLS
◆ The stomach and duodenum must be thoroughly mobilized for performance of the
anastomosis.
◆ Duodenal edema, shortening, or deformity may prevent performance of a Billroth I anasto-
mosis and require a Billroth II anastomosis for safe closure.
SELECTED REFERENCES
1. Mercer DW, Robinson EK: Stomach. In Townsend CM Jr (ed): Sabiston Textbook of Surgery: The
Biological Basis of Modern Surgical Practice, 18th ed. Philadelphia, Saunders, 2008, pp 1223-1277.
2. Thompson JC: Subtotal gastrectomy with stapled Billroth I anastomosis (also resection for benign distal
gastric ulcer). In Thompson JC (ed): Atlas of Surgery of the Stomach, Duodenum and Small Bowel.
St Louis, Mosby-Year Book, 1992, pp 45-53.
3. Thompson JC: Subtotal gastrectomy with stapled Billroth I anastomosis. In Thompson JC (ed): Atlas of
Surgery of the Stomach, Duodenum and Small Bowel. St Louis, Mosby-Year Book, 1992, pp 55-59.

292
STEP 1: SURGICAL ANATOMY
◆ The vascular supply to the stomach has been previously described (see Figure 26-1).
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The Billroth II gastric resection is one of the most commonly performed procedures for
cancer of the stomach and is also used for operative treatment of duodenal ulcer disease if
gastric resection is required.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The patient is placed supine on the table, and an upper midline incision or subcostal
incision is used as described for the Billroth I anastomosis.
2. DISSECTION
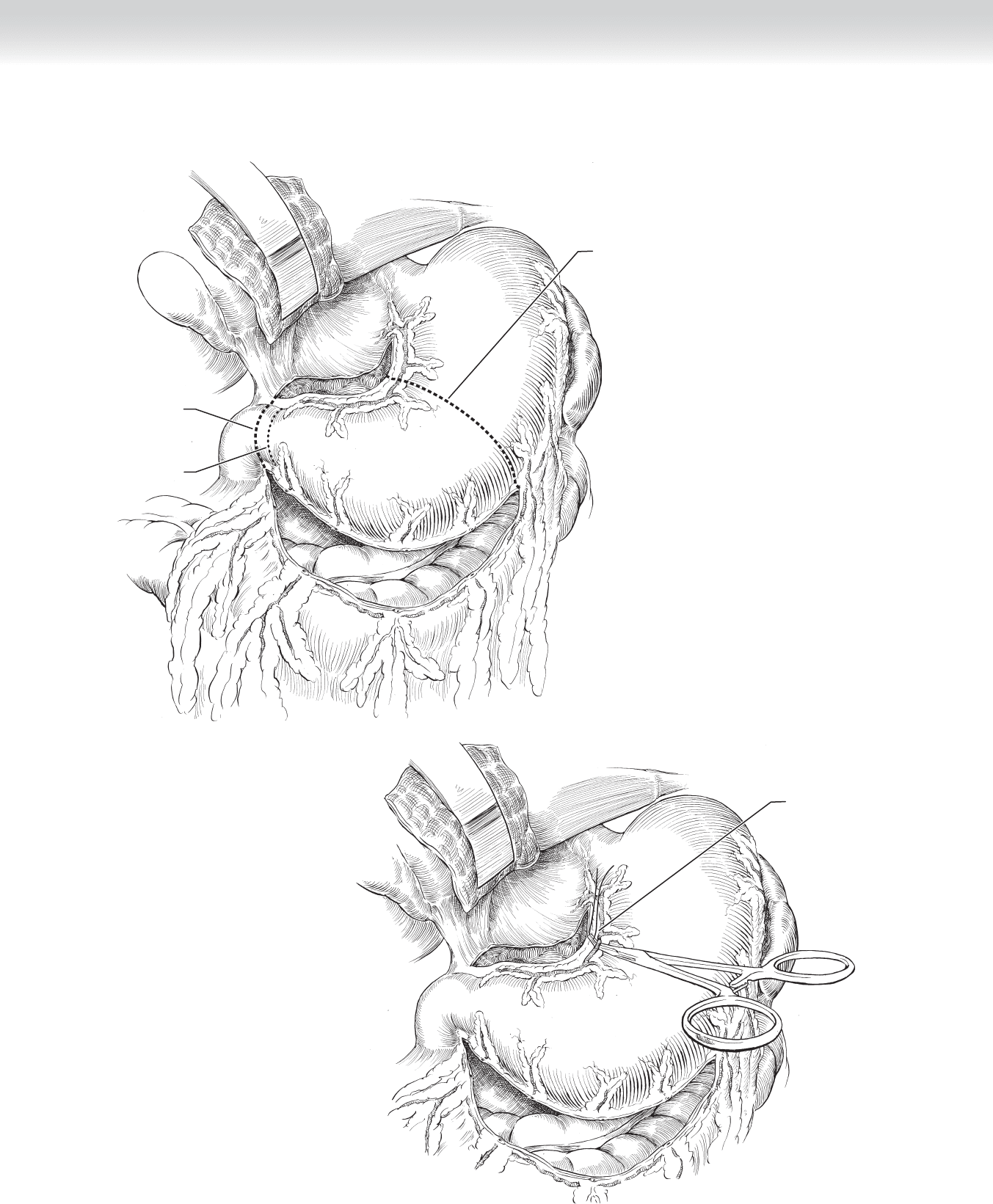
◆ Figure 27-1 demonstrates transection of the stomach, indicating a 50% distal gastric
resection, starting at the incisura on the lesser curvature as noted by the dashed line.
The duodenum is transected distal to the pylorus. The greater curvature is mobilized by
dividing the gastroepiploic vessels and is ligated with 2-0 silk sutures.
◆ The lesser curvature is then likewise mobilized to the incisura (see Figure 27-1).
◆ The left gastric artery and vein are ligated in continuity with 2-0 silk sutures and divided
(Figure 27-2).
CHAPTER
27
Gastric Resection: Billroth II
B. Mark Evers
CHAPTER 27 • Gastric Resection: Billroth II 293
Ligate and divide
gastric artery
Incision line
Pylorus
Incision
line
FIGURE 27 –1
FIGURE 27 –2
294 Section IV • The Abdomen
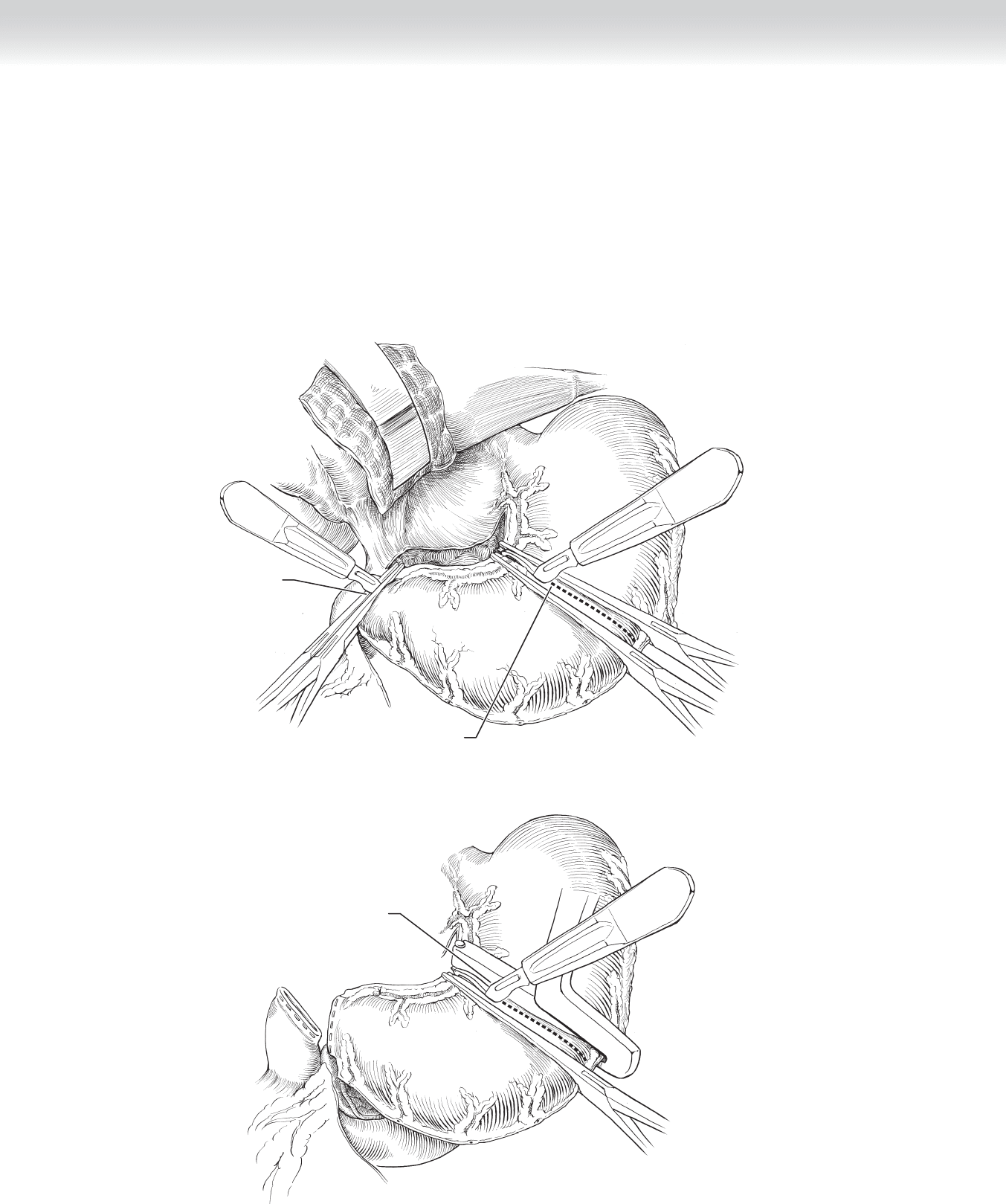
◆ The stomach is transected between Kocher or Payr clamps using the scalpel, and likewise,
the fi rst portion of the duodenum is transected between Kocher clamps (Figure 27-3).
◆ Figure 27-4 demonstrates a stapled division of the stomach and duodenum with the duo-
denum stapled using a gastrointestinal anastomosis (GIA) stapler device and the stomach
stapled using a transanastomotic (TA)-30 or TA-55 stapler. The stomach is then transected
using the scalpel staying right on the staple line.
Dividing stomach
Incising just
beyond pylorus
FIGURE 27 –3
Dividing stomach
FIGURE 27 –4
CHAPTER 27 • Gastric Resection: Billroth II 295
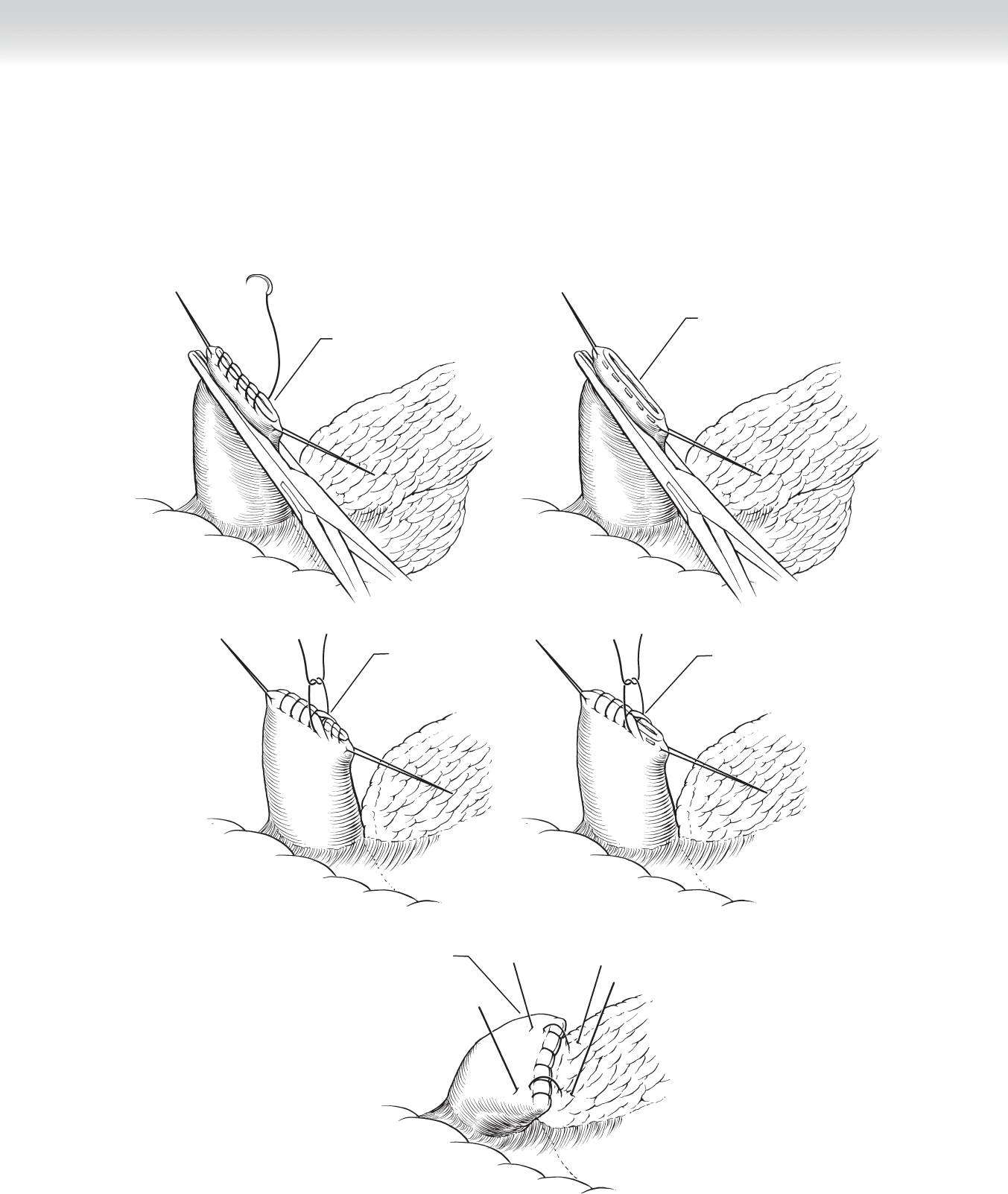
◆ Figure 27-5, A shows the duodenal stump closure performed using running nonabsorbable
sutures. Figure 27-5, B shows a stapled closure of the duodenal stump. Interrupted sero-
muscular sutures are then placed over the fi rst row of running sutures (Figure 27-5, C) or
over the staple line (Figure 27-5, D). Some surgeons prefer to secure the duodenal stump
to the pancreas as shown in Figure 27-5, E.
Suture closure
A
Staple closure
B
C
Interrupted suture
over first row of
running sutures
D
Interrupted suture
over stapled closure
E
Securing duodenum
to pancreas
FIGURE 27–5
296 Section IV • The Abdomen
◆ Excess gastric tissue that had been crushed with the clamp is trimmed using the scalpel or
electrocautery (Figure 27-6, A). Starting on the lesser curvature side, the stomach is closed
with running nonabsorbable sutures (Figure 27-6, B). This is accomplished to the level of
the Kocher clamp (Figure 27-6, C).
Removing excess
gastric tissue
A
FIGURE 27–6
B
C
CHAPTER 27 • Gastric Resection: Billroth II 297
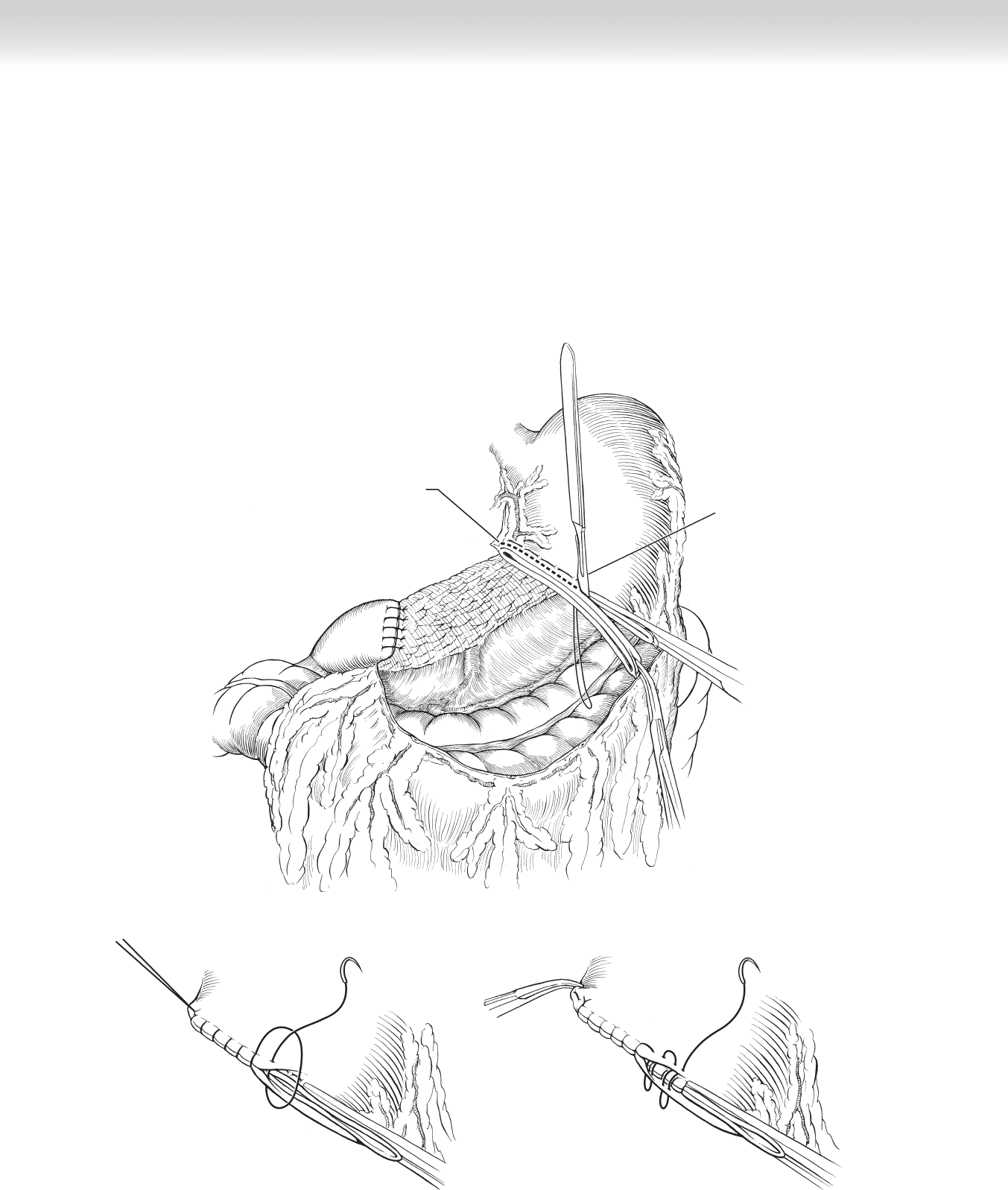
◆ A loop of proximal jejunum is brought up in an antecolic fashion, and the anastomosis
is performed in two layers. The outer layer is performed with interrupted 3-0 silk su-
tures placed in a Lembert fashion (Figure 27-7).
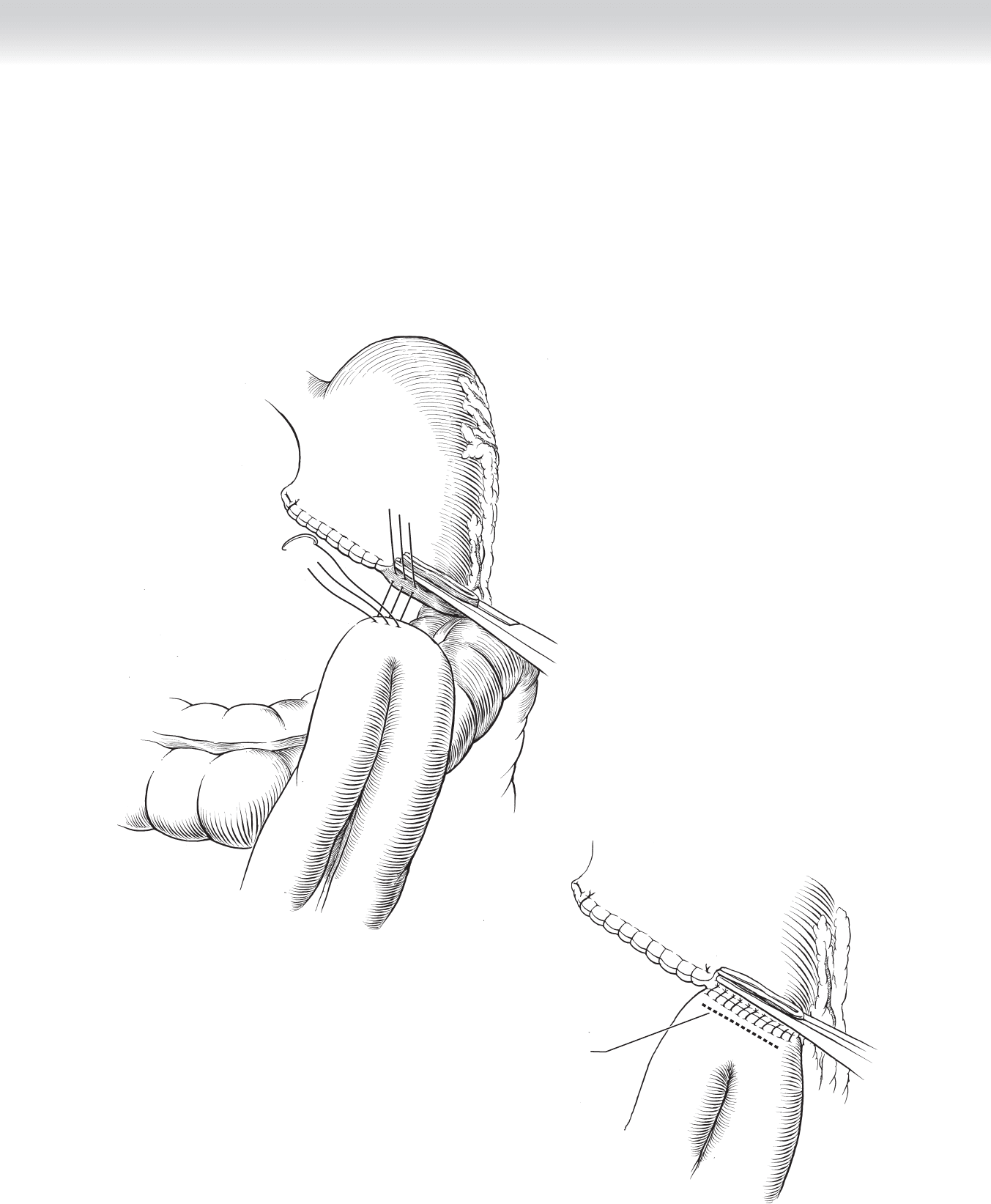
◆ The electrocautery is then used to open the jejunum at the dashed line as shown in
Figure 27-8.
FIGURE 27–7
Incision in jejunum
for anastomosis
FIGURE 27–8
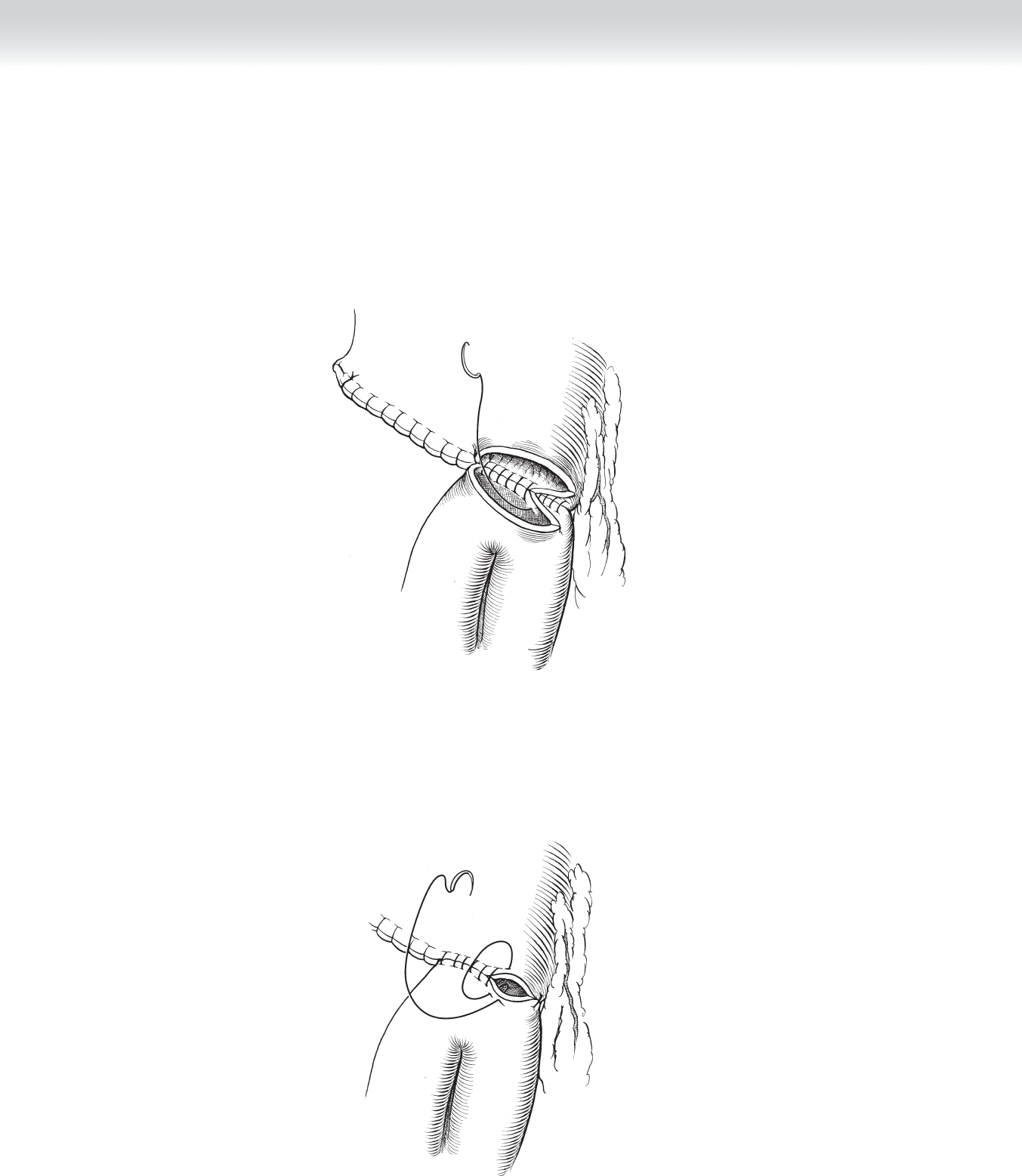
◆ The inner row of the anastomosis is performed in a running fashion using a 3-0 nonabsorb-
able suture such as chromic or Vicryl. The suture is carried anteriorly in a Connell fashion
(Figures 27-9 and 27-10).
FIGURE 27–9
FIGURE 27–10
Section IV • The Abdomen298