Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

584 Section VII • Pancreas
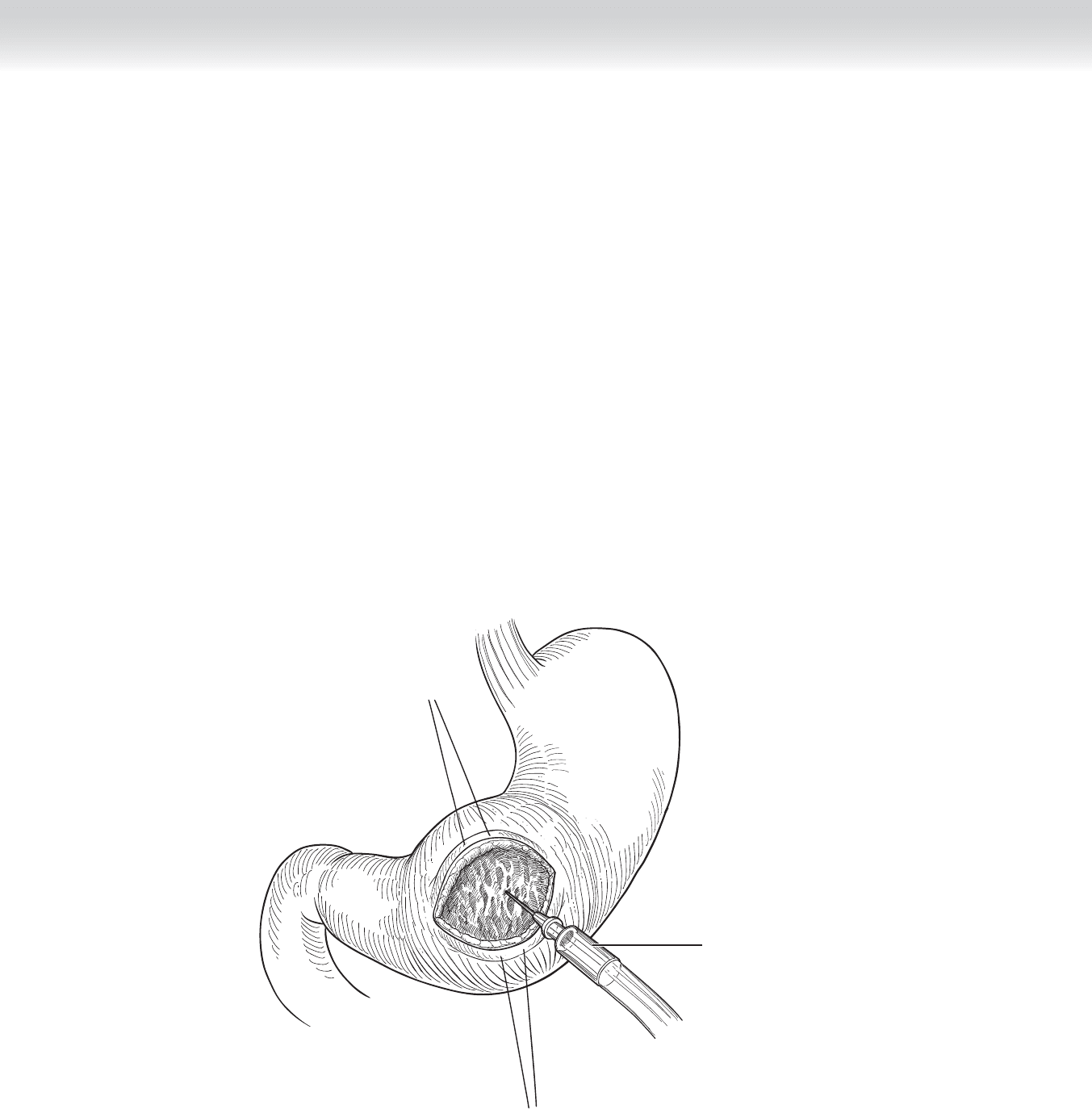
◆ At this point, a 20-gauge angiocatheter is placed into the cyst to confi rm that cyst fl uid will
be encountered (Figure 51-3). Finally, electrocautery is used to begin an entryway through
the posterior wall of the stomach into the cyst. We then take a long, delicate hemostat such
as the Seurat clamp and gently place it through the posterior wall of the stomach and
through the anterior wall of the cyst. Typically a large amount of fl uid will be evacuated. In
most cases, this will result in fairly signifi cant collapse of the pseudocyst. At this point of
entry, a larger orifi ce can be made, and at the same time a biopsy of the wall of the cyst can
be obtained (Figure 51-4). This should be sent for frozen section analysis to confi rm that it
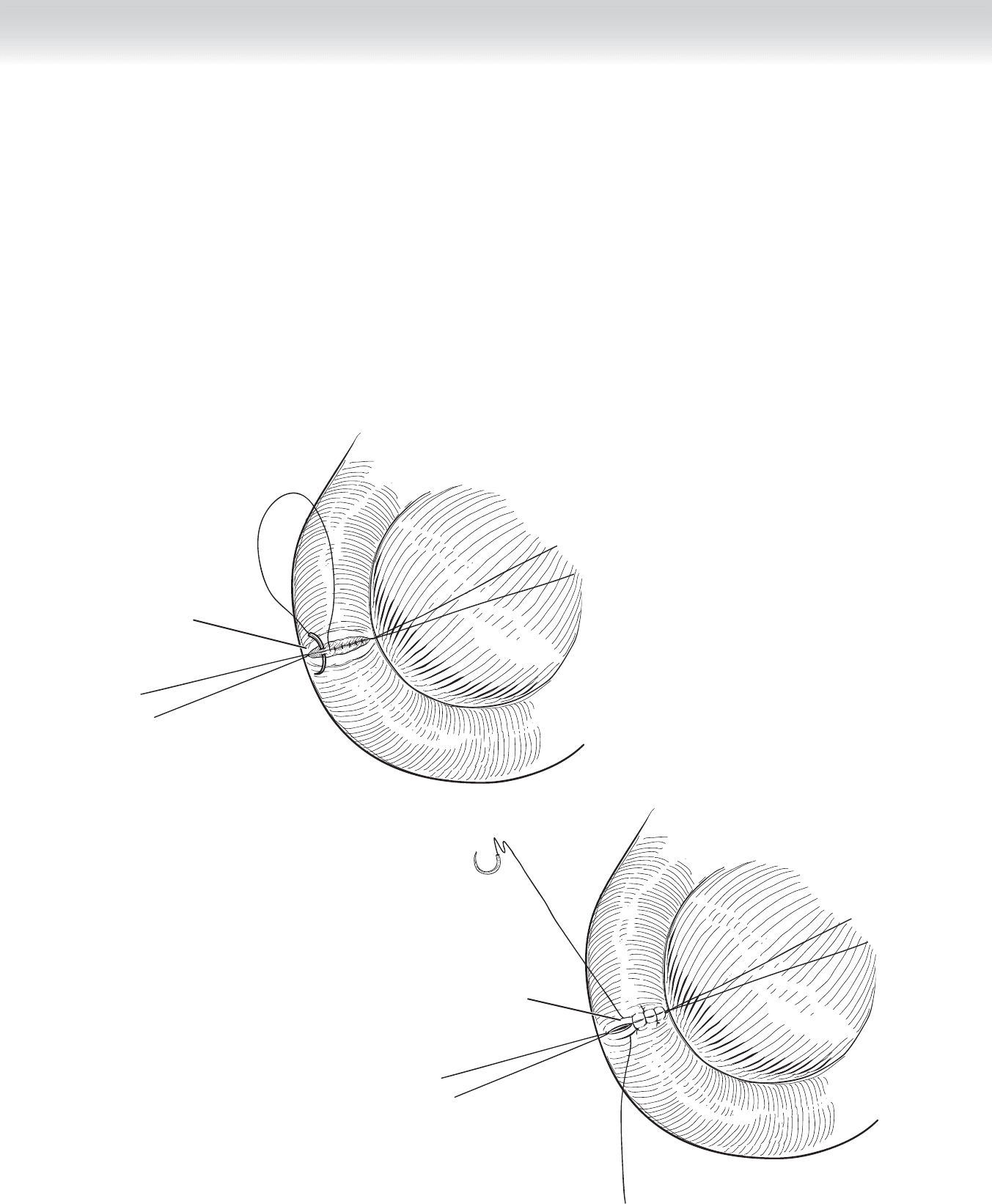
is not a neoplastic cyst. We fi nally work with approximately 3-cm-diameter entry into the
cyst. Next, 2-0 Prolene sutures are used in a running fashion to complete the connection
between the cyst and posterior wall of the stomach (Figure 51-5). After this is complete,
one evacuates any solid material within the cyst and irrigates the cyst. For all cysts, we
believe it is vital to evacuate as much of this debris as possible. Any hemorrhage encoun-
tered in the wall of the cyst or in the gastric wall should be suture ligated to prevent post-
operative hemorrhage.
Angiocatheter
FIGURE 51 –3
Posterior wall
gastrotomy
Biopsy
2-0 running sutures
FIGURE 51 –4
FIGURE 51 –5
CHAPTER 51 • Pseudocysts 585

586 Section VII • Pancreas
◆ We often will take a culture of the fl uid in the cyst on the chance that the cyst fl uid has
been colonized (which is common) and the patient develops signs of sepsis in the postoper-
ative period.
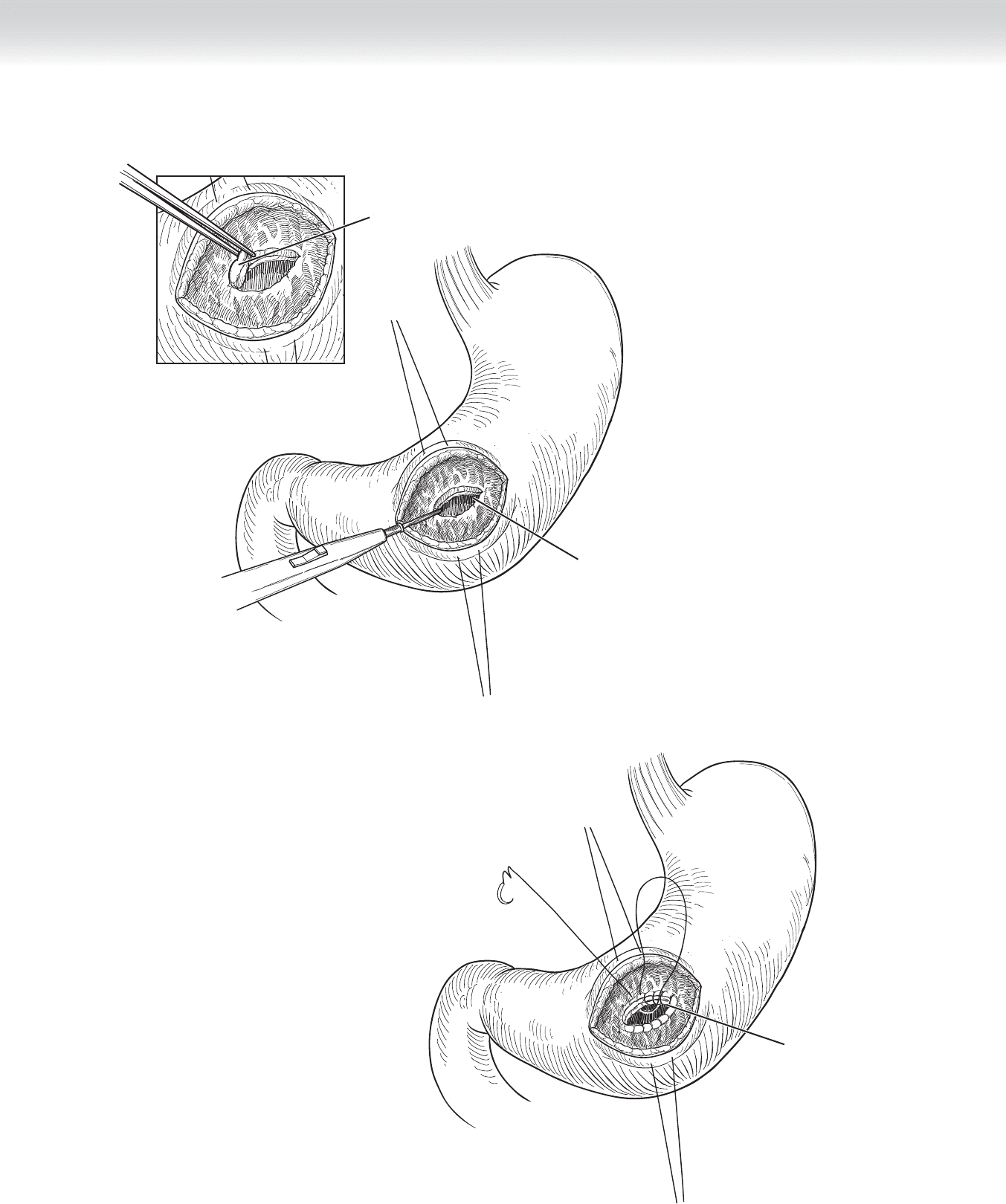
◆ The anterior gastrotomy is then closed in two layers with an outer layer of interrupted 3-0
silk stitch and an inner layer of a Connell type of absorbable suture, such as polydioxanone
(PDS) or Vicryl. Lembert sutures of 3-0 silk are placed at the two corners of the gastrotomy,
tied, and left long on a hemostat for traction. Two 3-0 Vicryl sutures are placed and tied at
each corner with the knot on the inside. A Connell type of running inverted stitch is used,
starting at each corner and meeting in the middle of the gastrotomy and tied (Figure 51-6).
Finally, an interrupted 3-0 silk stitch is used in an interrupted fashion to complete the ante-
rior layer of the gastrotomy closure (Figure 51-7).
◆ We do not use drains. The peritoneal cavity is irrigated.
◆ Fascia is reapproximated in the normal fashion, and subcuticular sutures are placed in
the skin.
Inner row of
Connell sutures
Outter row of
interrupted sutures
FIGURE 51 –6
FIGURE 51 –7
CHAPTER 51 • Pseudocysts 587
588 Section VII • Pancreas
Cystoduodenostomy
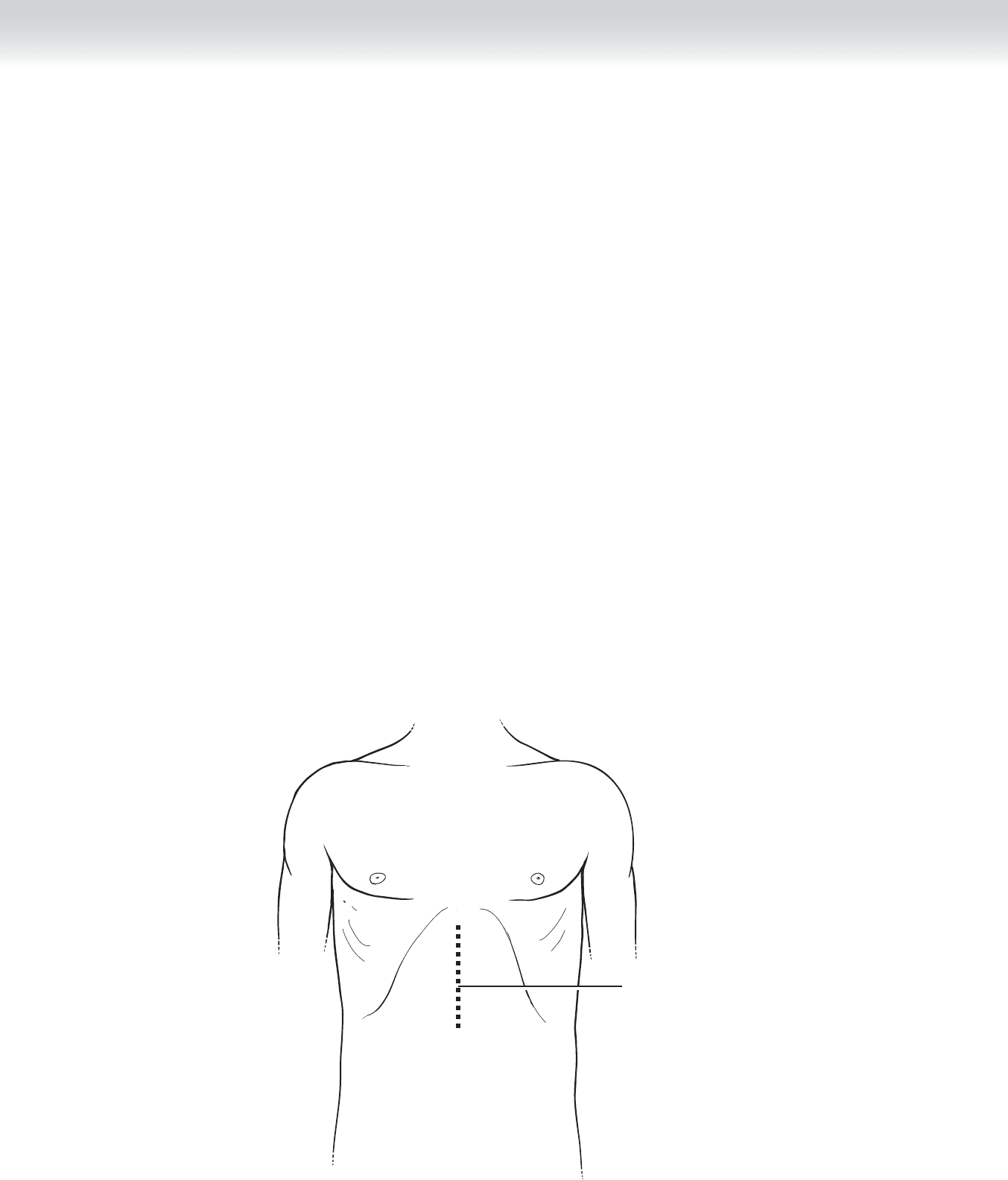
◆ If preoperative evaluation convinces the surgeon that a cystoduodenostomy is best, we
again use a midline incision (Figure 51-8). The dissection is carried out by entering the
lesser sac. This can typically be done by separating the gastrocolic omentum from its attach-
ments along the transverse colon. Obviously, this technique is restricted to patients with
pseudocysts located in the head of the pancreas, abutting the medial wall of the duodenum
(Figure 51-9).
◆ In the event the adhesions resulting from the acute pancreatitis and the pseudocyst have
made entry into the lesser sac unfeasible, one may simply divide the omental attachments
overlying the head of the pancreas between clamps. Care should be taken to avoid injury
to the right gastroepiploic arteries and to the vessels of the transverse mesocolon, should
this access point be chosen. At this point, one should be able to palpate the pseudocyst
(Figure 51-10). Throughout this discussion it should be made clear that the extent of ad-
hesions will dictate much of this dissection. If infl ammatory adhesions are excessive, then
alternative approaches must be sought. I would also caution that simply fi nding the pseu-
docyst may be challenging, and intraoperative ultrasound may be useful.
Incision
FIGURE 51 –8
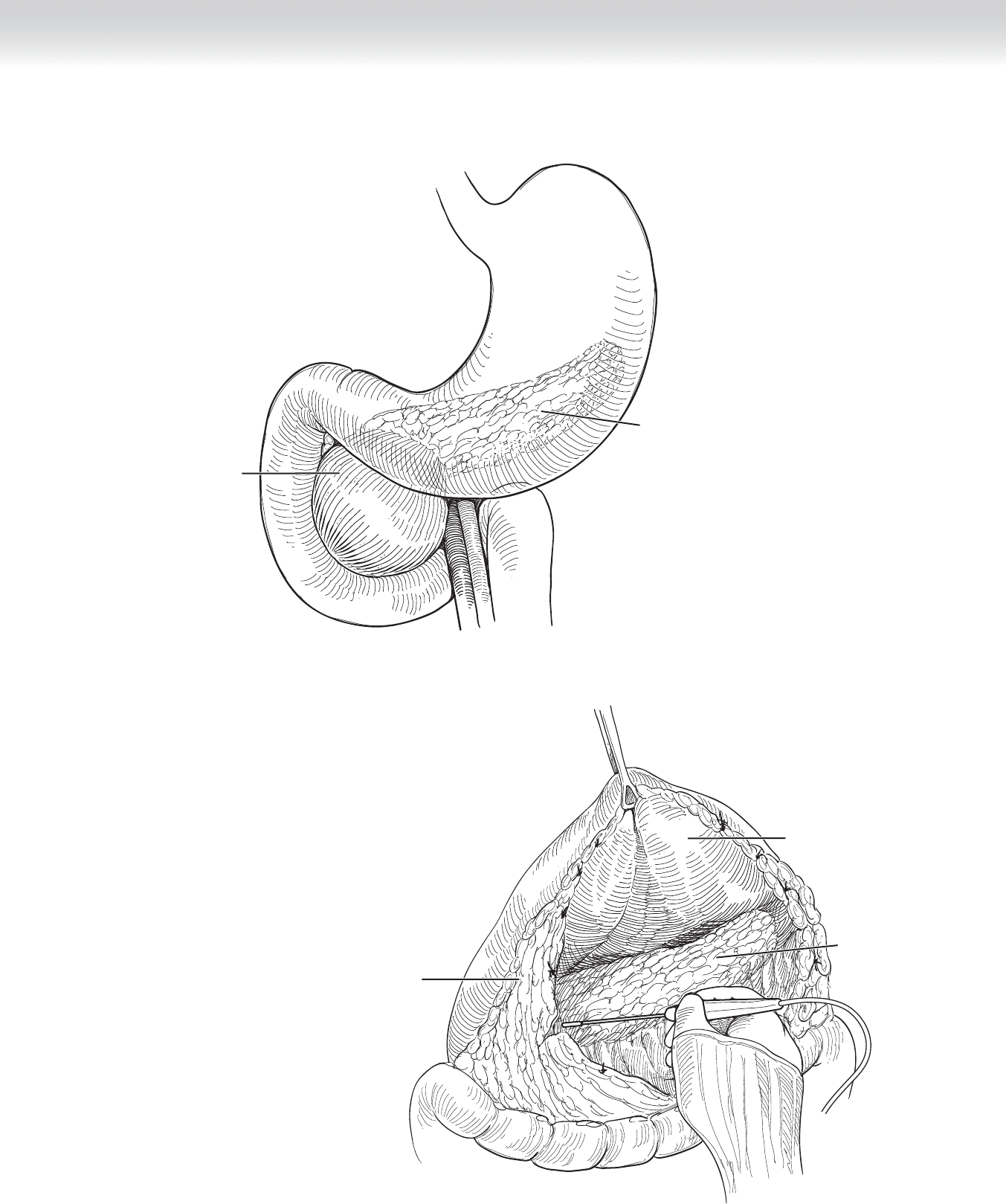
Pseudocyst
Stomach
Pancreas
FIGURE 51 –9
CHAPTER 51 • Pseudocysts 589
Pseudocyst
Stomach
Pancreas
FIGURE 51 –10
590 Section VII • Pancreas
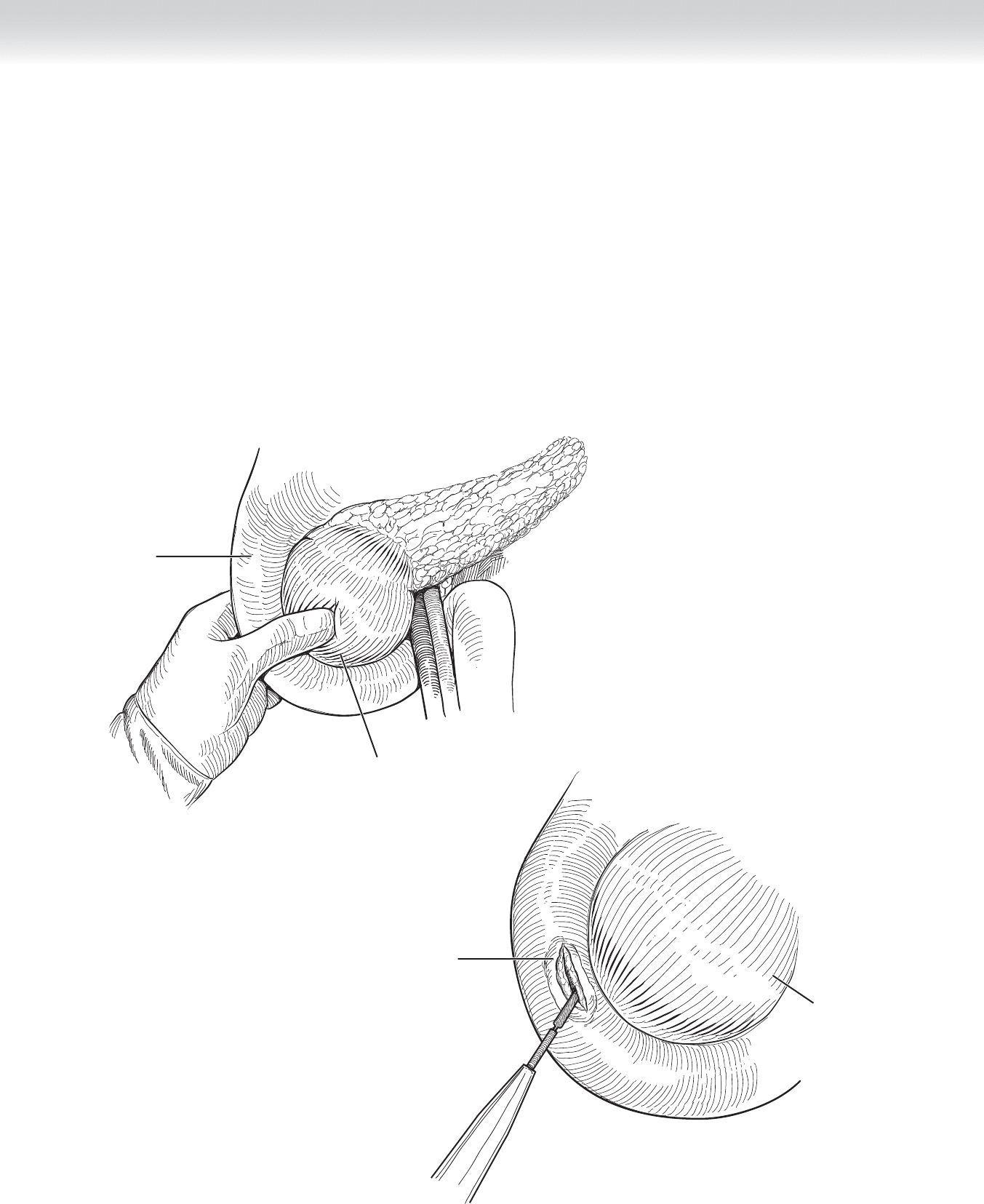
◆ We then perform a Kocher maneuver by incising the peritoneum along the line outlining
the lateral border of the C-loop of the duodenum and mobilizing the duodenum and the
head of the pancreas toward the left, teasing the loose the areolar tissue in the retroperito-
neum. This permits bimanual palpation of the head of the pancreas and permits the sur-
geon to ascertain the exact location of the cyst (Figure 51-11). Having ascertained the area
of the duodenum most closely approximating the location of the cyst, the surgeon performs
a duodenotomy. Stay sutures of 3-0 silk stitch are placed well away from the margin of the
duodenum to the head of the pancreas, and after these have been placed, a longitudinal in-
cision is made in the duodenum for the length of approximately 4 cm (Figure 51-12).
With proper palpation, one can confi rm the area of the posterior wall of the duodenum as
it abuts the cyst. At this point, we place an angiocatheter into the cyst and confi rm that cyst
fl uid aspirates (Figure 51-13). We then use electrocautery to carefully dissect through the
posterior wall of the duodenum into the cyst. We excise a small portion of the wall of the
cyst and send for frozen section analysis to exclude a neoplasm (Figure 51-14).
Duodenum
Kocherized
Palpation of pseudocyst
FIGURE 51 –11
Duodenectomy
Pseudocyst
FIGURE 51 –12
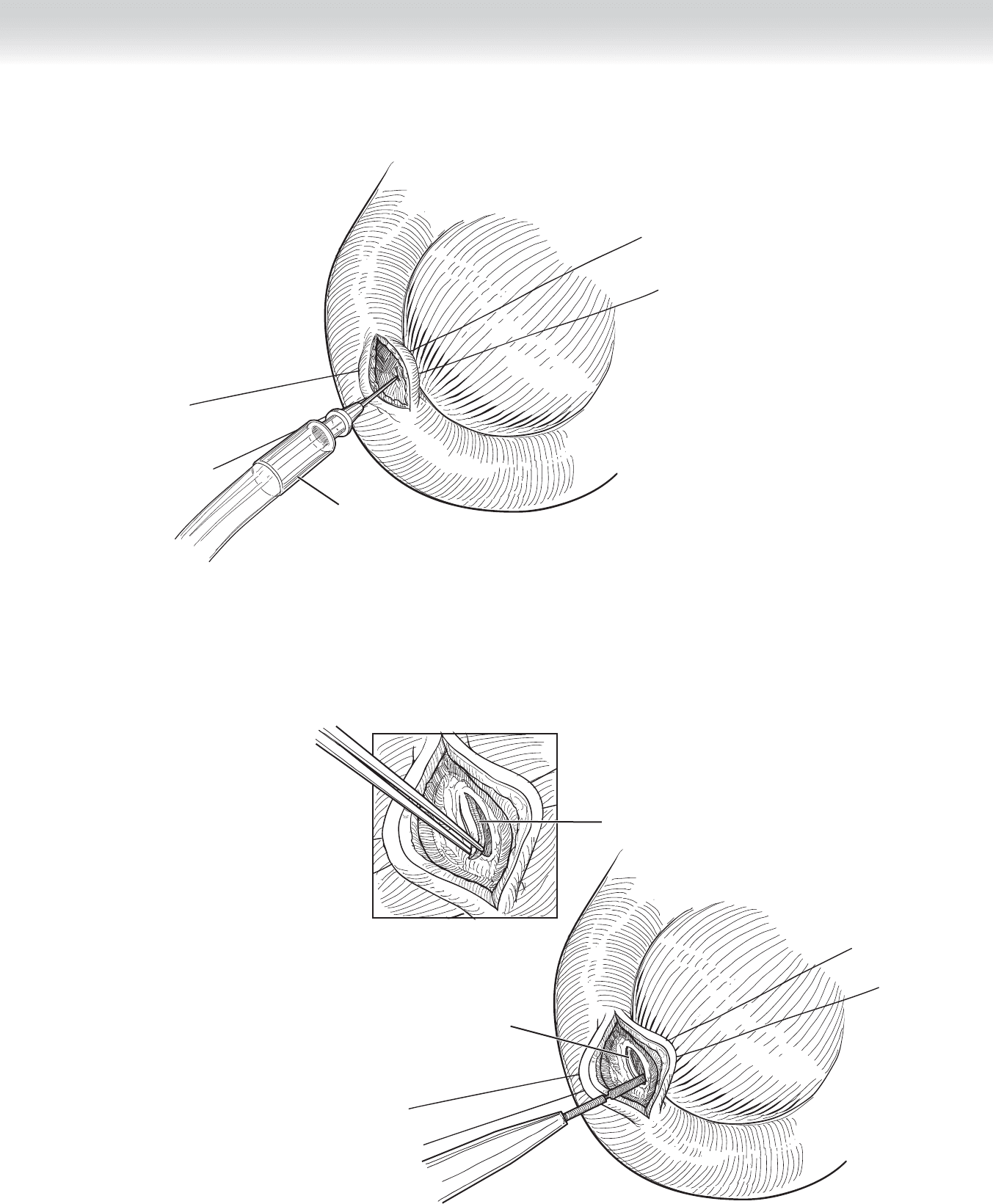
Angiocatheter
FIGURE 51 –13
Dissection through
wall of duodenum
Biopsy
FIGURE 51 –14
CHAPTER 51 • Pseudocysts 591
592 Section VII • Pancreas
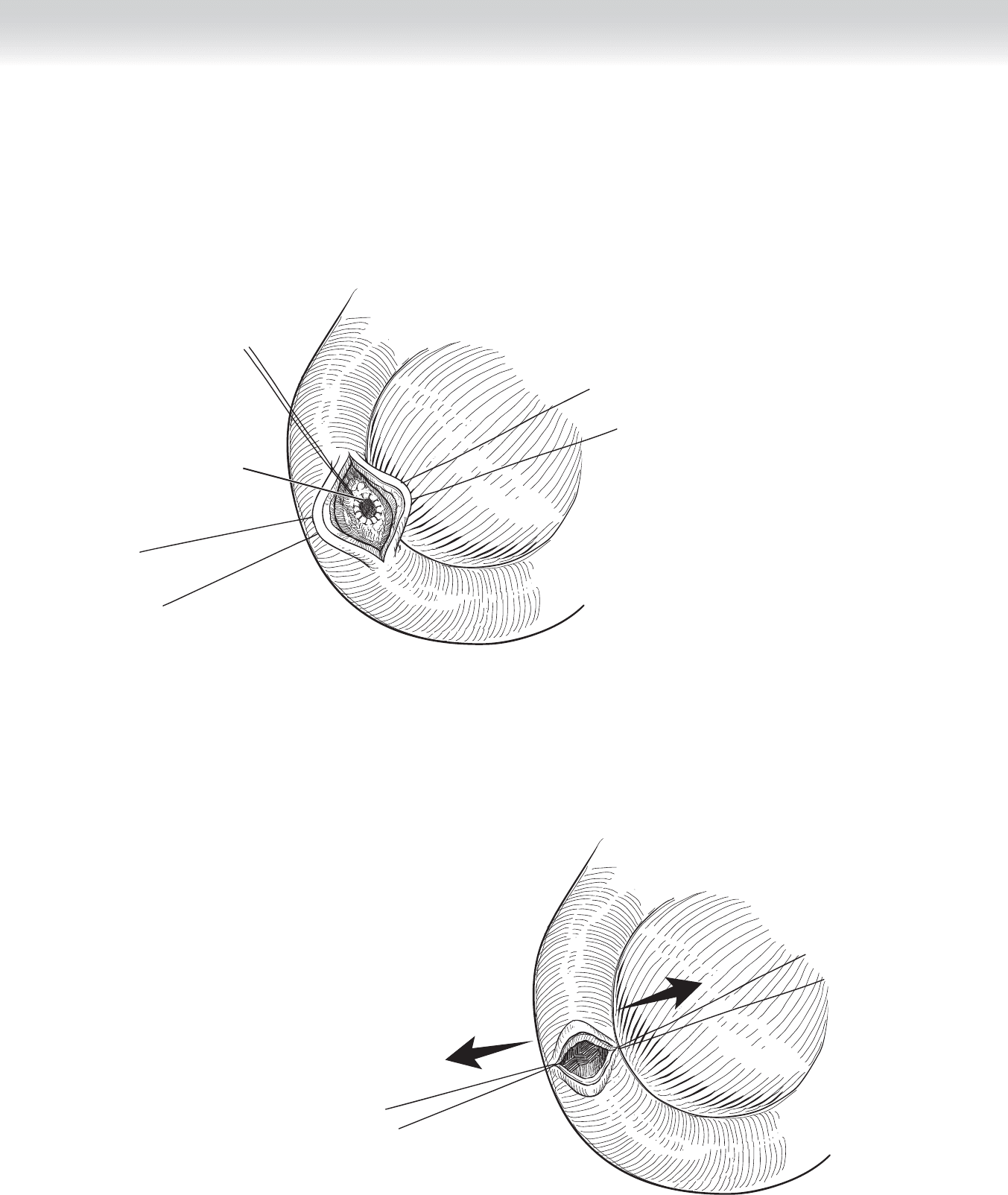
◆ We then open the cyst for a diameter of approximately 2 cm and place 3-0 Prolene sutures
in a running fashion circumferentially around the duodenotomy into the cyst (Figure 51-15).
In a cross-sectional view, one can see the orientation of the cystoduodenostomy to the pan-
creas and duodenum (Figure 51-16). Any solid material in the cyst is removed. We again
obtain culture of the cyst fl uid.
Running circumferential
sutures
FIGURE 51 –15
FIGURE 51 –16
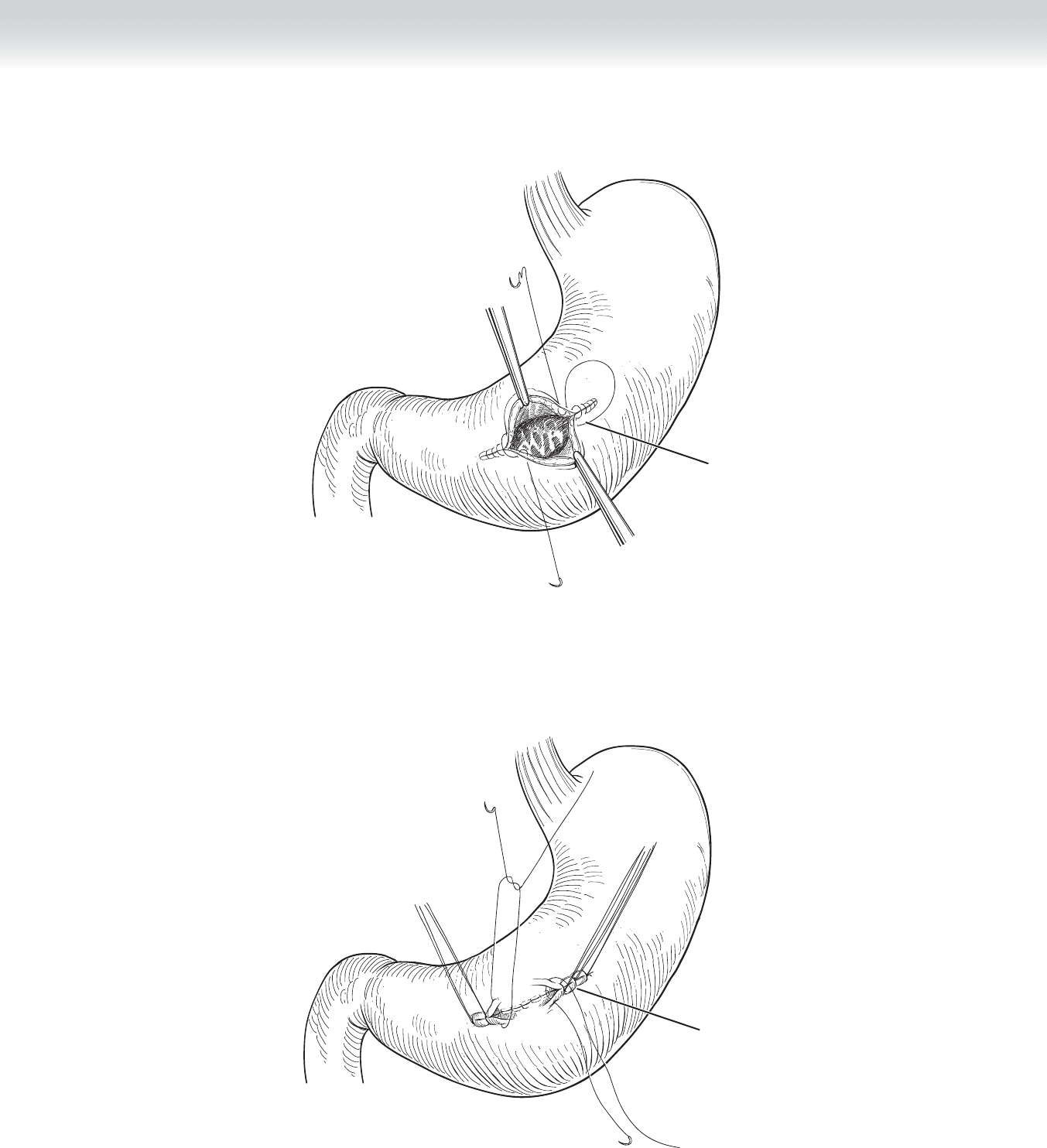
◆ After this has been done, the longitudinal incision in the duodenum is closed in a trans-
verse fashion similar to a technique of closure fi rst described by Heineke and Mikulicz in
their description of a pyloroplasty. This closure is performed in two layers with an outer
layer of interrupted 3-0 silk stitch and an inner layer of a Connell type of stitch. Just as in
the closure of the gastrotomy, the running absorbable suture line is again taken from each
corner and tied in the middle. In this anastomosis, however, the superior and the inferior
extent of the duodenotomy are sutured together at the midpoint of the transverse closure.
To start, place a Lembert-type stitch with 3-0 silk at exactly the midpoint of the duodeno-
tomy on both the lateral and the medial edges. These will be the new corners. Complete
the Connell sutures and then place interrupted silk sutures to complete the closure
(Figures 51-17 and 51-18). At completion, the closure should look to be at right angles to
the course of the duodenum. This is performed to prevent any signifi cant narrowing of the
duodenum after the duodenotomy.
3-0 continuous sutures to
close mucosa
FIGURE 51 –17
Interrupted sutures to
close seromuscularis
FIGURE 51 –18
CHAPTER 51 • Pseudocysts 593