Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

574 Section VII • Pancreas
◆ A side-to-side pancreaticojejunostomy is performed in one layer using interrupted 3-0 silk
stitch. The inferior suture line is placed before the jejunum is opened, and these sutures are
tied. After the jejunum is opened, the superior row of sutures in the pancreaticojejunos-
tomy is completed by placing a corner stitch to the left and right boundaries and by placing
a stitch midway through the longitudinal incision in the body of the pancreas and midway
through the incision in the jejunum (Figure 50-10). Immediately tying the sutures on the
superior suture line prevents any mismatch in size between the jejunal incision and the
pancreatic duct incision. It should be noted that typically the jejunum tends to open much
larger than one can anticipate, so care should be taken to place the inferior sutures in the
jejunum somewhat closer than they are placed in the inferior aspect of the incision in the
wall of the pancreas. After the middle suture on the superior suture line is placed, sutures
are placed that bisect the area to the left and right. Finally, individual sutures are placed as
appropriate to complete the anastomosis (Figures 50-11 and 50-12).
Completed Roux-en-Y
FIGURE 50 –10

CHAPTER 50 • Pancreaticojejunostomy (Puestow) 575
Cross-section
Pancreatic duct
Pancreaticojejunostomy
FIGURE 50 –11
FIGURE 50 –12

576 Section VII • Pancreas
3. CLOSING
◆ At completion of the pancreaticojejunostomy, the limb of jejunum is fi xed in place as it tra-
verses the transverse mesocolon with an interrupted 3-0 silk stitch. Finally, 40 cm distal to the
pancreaticojejunostomy, a side-to-side jejunojejunostomy is performed in two layers, with an
outer layer of interrupted 3-0 silk stitch and an inner layer of running locking 3-0 Vicryl
stitch posteriorly, which converts to a Connell type of stitch anteriorly (see Figure 50-12).
◆ We do not use drains. The fascia is reapproximated in the normal fashion, and the skin is
closed using subcuticular suture.
STEP 4: POSTOPERATIVE CARE
◆ Patients will have had a nasogastric tube placed. This is removed on the fi rst postoperative
day. The patient starts with a clear liquid diet, and if tolerated, this is advanced to a regular
diet.
◆ Care should be taken in the immediate postoperative period to monitor blood glucose,
because these patients often have borderline insuffi ciency or frank diabetes, and for that
reason the stress of surgery may result in signifi cant hyperglycemia.
◆ The only signifi cant postoperative complication that can be anticipated in the fi rst 24 to
48 hours is hemorrhage. For that reason, one should carefully monitor hemoglobin levels.
Once these have proved to be stable, it is not necessary to continue to monitor these.
STEP 5: PEARLS AND PITFALLS
◆ It can be challenging to fi nd the pancreatic duct in some patients. Although the duct is
easily palpable in most, it is not in some. On rare occasions, it may be necessary to perform
a vertical incision in the mid-portion of the anterior surface of the body of the pancreas as a
means of searching for the actual pancreatic duct. Care should be taken not to
extend this incision to either the superior or the inferior border of the pancreas. It is also
often possible to express some of the pancreatic juice by massaging either the anterior sur-
face of the tail of the pancreas or the anterior surface of the head of the pancreas. The
pancreatic juice is crystal clear and should be easily recognized during this palpation.
◆ As mentioned during the operative procedure, the mismatch between the opening in the
jejunum and the opening in the pancreatic duct can be problematic. Care should be taken
to limit the size of the opening in the jejunum until one can be certain that it is does not
greatly exceed the length of the opening in the main pancreatic duct.

CHAPTER 50 • Pancreaticojejunostomy (Puestow) 577
◆ It is not uncommon to have associated bile duct stricture in patients undergoing Puestow
procedure, and consideration should be given to the possible need for a hepaticojejunos-
tomy at the same time as the pancreaticojejunostomy.
◆ One may typically encounter stones either within the main pancreatic duct or easily palpa-
ble in some of the dilated side branches. We advocate removing these stones when possible.
Instruments such as Fogarty catheters and some instruments typically used for biliary lithia-
sis may be helpful in this event.
SELECTED REFERENCES
1. Katz MH, Wang H, Fleming JB, et al. Long-term survival after multidisciplinary management of resected
pancreatic adenocarcinoma. Ann Surg Oncol 2009;16:836-847.
2. Kow AW, Chan SP, Earnest A, et al. Striving for a better operative outcome: 101 Pancreaticoduodenecto-
mies. HPB (Oxford) 2008;10:464-471.
3. Katz MH, Fleming JB, Pisters PW, et al. Anatomy of the superior mesenteric vein with special reference to
the surgical management of fi rst-order branch involvement at pancreaticoduodenectomy. Ann Surg
2008;248:1098-1102.

578
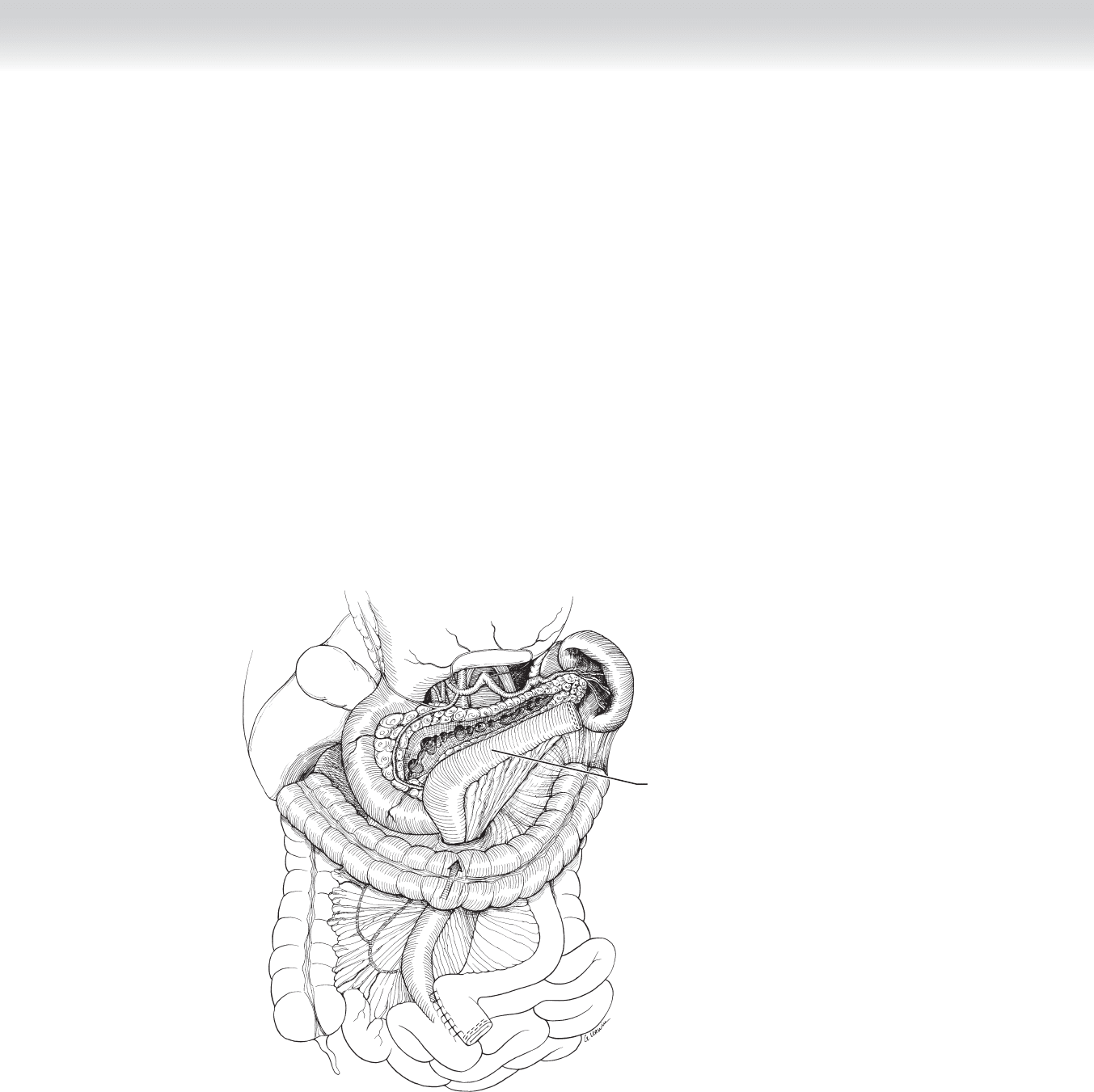
STEP 1: SURGICAL ANATOMY
◆ All pancreatic surgery requires an understanding of the anatomic relationships in the lesser
sac (see Figure 47-1). After either an upper midline or a bilateral subcostal (chevron) inci-
sion, one enters the lesser sac by dissecting along the avascular plane at the points of attach-
ment of the gastrocolic omentum to the transverse colon. The proper plane is between the
anterior and posterior leafl ets. This is my favored point of entry. The alternative entry is by
transversely dividing and ligating the vascular structures embedded in the omentum while
preserving the gastroepiploic vessels located along the greater curvature of the stomach.
◆ Upon entering the lesser sac, one will encounter varying amounts of adhesions between the
posterior wall of the stomach and the anterior surface of the pancreas. These fetal adhesions
do not imply prior infl ammatory events. Considerable dense adhesions may be encountered
in pathologic states.
◆ The pancreas is essentially encased in a sandwich of major blood vessels. The vena cava and
aorta occupy the posterior surface in the midline. The splenic artery courses along the supe-
rior surface from the aorta toward the tail. The splenic vein occupies the posterior superior
surface of the body and tail of the pancreas. It meets the superior mesenteric vein, which is
oriented vertically in the groove created by the uncinate process in the posterior aspect of the
head of the pancreas and the right lateral and anterior components of the head. The confl u-
ence of these two veins constitutes the portal vein, which traverses this uncinate groove and
emerges to join the bile duct and the hepatic artery in the hepatoduodenal ligament.
◆ The superior mesenteric artery is located in a plane posterior and slightly medial to the su-
perior mesenteric vein. The common hepatic artery, another branch of the celiac trunk
(along with the splenic artery and left gastric artery), courses along the superior border of
the head of the pancreas to join the hepatoduodenal ligament. Its fi rst branch is the typi-
cally miniscule right gastric artery. Just distal is the more substantial gastroduodenal artery,
which emerges at a right angle to the hepatic artery from its inferior surface and courses be-
neath the pylorus, and after sending the right gastroepiploic artery in the plane between the
inferior aspect of the pylorus and the superior surface of the head of the pancreas, the gas-
troduodenal artery pierces the head of the pancreas.
CHAPTER
51
Pseudocysts—Cystogastrostomy,
Cystoduodenostomy, and
Cystojejunostomy
William H. Nealon

◆ The anterior superior and the posterior superior pancreaticoduodenal arteries also arise
from branches of the gastroduodenal artery. These arteries form an arch medial to the
C-loop of the duodenum, and they collateralize with branches of the anterior and posterior
inferior pancreaticoduodenal arteries, which are branches of the superior mesenteric artery.
Small branches from these arteries provide blood supply to the duodenum.
◆ Key anatomic features in pancreatic head resections are the network of tributaries projecting
between the superior mesenteric vein/portal vein confl uence and the uncinate process.
These tributaries are located at the right lateral aspect of the veins. These tiny veins exit the
pancreas at the mid-portion of the groove in which the major veins reside.
◆ Viewed in cross-sectional imaging, the uncinate process forms a C-shaped structure. The
terminal posterior extent of the uncinate process projects in a medial direction as a liga-
mentous structure and contains a variable number of arterial branches from the superior
mesenteric artery that project at right angles to the major artery and provide blood supply
to the uncinate process. Division of the tiny venous tributaries and the arterial branches are
key steps in respective procedures. This uncinate margin is the most problematic in
managing malignant tumors in the head of the pancreas.
◆ The pancreas is entirely retroperitoneal, and therefore operative procedures will require mo-
bilization of the pancreas from its retroperitoneal position. The plane lateral to the C-loop
of the duodenum is incised in nearly all procedures, and this plane is avascular and its mo-
bilization is termed the Kocher maneuver. This exposes the vena cava and aorta and it per-
mits “bimanual palpation” of the head of the pancreas. The dissection may be easily ex-
tended to the fourth portion of the duodenum and the ligament of Treitz .
◆ The inferior border of the body of the pancreas is also avascular, although the inferior mes-
enteric vein may be encountered to the right of the spine.
◆ Peritoneum overlies the hepatoduodenal ligament. Dissection reveals the triad in gross ana-
tomic terms, which corresponds to the microscopic portal triad—with portal, hepatic arte-
rial, and biliary structures. The common bile duct is located in an anterior lateral position,
and the hepatic artery is anterior medial. The portal vein is positioned in the posterior
groove created by the apposition of these anterior structures.
◆ Although lymph nodes may be seen at a wide array of locations, there is a constant lymph
node in the groove created by the lateral border of the second portion of the duodenum
and the hepatoduodenal ligament. Dissection of this lymph node is necessary to fully visu-
alize the proximal hepatic artery. Other common sites of lymph nodes are on the lateral
aspect of the mid-portion of the hepatoduodenal ligament, in the fi brovascular bundle sur-
rounding the right gastroepiploic complex, and on the superior border of the confl uence of
the head and body of the pancreas. Beneath this lymph node one fi nds the origins of the
common hepatic artery and the splenic artery.
CHAPTER 51 • Pseudocysts 579

580 Section VII • Pancreas
◆ On the inferior border of the pancreatic head, just where the duodenum dives beneath the
superior mesenteric vein and artery, one may dissect the peritoneum and visualize the supe-
rior mesenteric vein as it passes in a superior direction beneath the head of the pancreas.
◆ The ligament of Treitz is a signifi cant anatomic structure, and it can be accessed by lifting
the transverse colon and omentum in an anterior direction. The ligament can be seen to the
left of the spine.
◆ The main pancreatic duct originates in the tail of the pancreas and traverses the length of
the pancreas to exit in the duodenum through both main ampulla (Vater) and the accessory
ampulla, which is located more proximally in the duodenum. The main pancreatic duct
(Wirsung) and the minor or accessory duct (Santorini) fuse during fetal development at
what is termed the genu or “knee” of the duct.
◆ It should be understood that pseudocysts can form at any location including sites quite re-
mote from the pancreas itself. Thus certain pseudocysts may involve anatomy not included
in this review.
INDICATIONS
◆ The indication for operation in pseudocysts is somewhat complex.
◆ First, one must confi rm that the pseudocyst has persisted long enough to be certain that the
cyst will not simply spontaneously resolve.
◆ Although not uniformly accepted, there is literature suggesting that only symptomatic pseu-
docysts should be treated. Thus one indication for surgery is symptoms (daily pain or diffi -
culty eating, or recurrent attacks of acute pain).
◆ The generally stated indication for surgery or some form of intervention is the development
of the complications of pseudocysts (obstruction of intestine or bile duct, hemorrhage into
the pseudocysts, infection in the pseudocysts, and rupture of the pseudocysts). Rupture of a
pseudocyst will present as ascites, an entity termed pancreatic ascites. A ruptured pseudo-
cyst should be suspected when this entity is identifi ed.
◆ An additional indication may be rapid expansion in a pseudocyst.
◆ An important distinction that should be made in the preoperative evaluation is the possibility
that a cyst actually represents a neoplastic cyst. In this case, suspicions may be raised by the
fact that a cyst has septations; a cyst has what appears to be wall thickening within the cyst;
and the patient may have an elevation in the tumor marker, which is known as CA 19-9.
Particularly in the setting of acute pancreatitis, one cannot automatically exclude a cystic
neoplasm, because 37% of patients with a diagnosis of intraductal papillary mucinous neo-
plasm (IPMN) present with pancreatitis. In the event that a neoplastic cyst is suspected, then

preoperative aspiration, typically by means of endoscopic ultrasound, is useful. This cyst fl uid
should be examined for the presence of mucin confi rmed by mucicarmine staining, measured
for carcinoembryonic antigen (CEA) level, and sent for cytopathologic evaluation.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ We strongly advocate identifi cation of the pancreatic ductal anatomy before intervention for
pseudocyst, and we have published several papers delineating the reasons. One particularly
signifi cant reason to evaluate the ductal anatomy is to help direct the choice of modality to
treat the pseudocyst. At this time, there is literature supporting three separate modalities to
treat pseudocysts (surgery, endoscopy, and interventional radiology). Our data suggest that
certain ductal injuries will make the likely success of these nonoperative modalities unac-
ceptably low. We also advocate defi ning ductal anatomy to recognize the possible coexis-
tence of a diagnosis of chronic pancreatitis, which should be addressed with operative pro-
cedures intended to treat that diagnosis rather than simply treating the cyst.
◆ We generally advocate a cystojejunostomy over the use of cystogastrostomy. There are
strong data to suggest that a very large cyst has a high likelihood of sepsis after cystogas-
trostomy, and there are softer data suggesting that cystogastrostomy has a higher risk of
postoperative hemorrhage compared with cystojejunostomy.
◆ If one is considering a cystogastrostomy, cross-sectional imaging is vital to confi rm a
fusion of the plane between the pseudocyst and the posterior wall of the stomach. Cross-
sectional imaging will also confi rm a close adherence between the pseudocyst and duo-
denum if a cystoduodenostomy is considered. Finally, cross-sectional imaging may help
in directing dissection for entering a cyst for cystojejunostomy. For example, the presence
of a cyst posteriorly toward the tail of the pancreas may be best addressed by traversing
the transverse mesocolon in order to access the cyst. If the cyst is posterior to most of the
parenchyma of the pancreas, it may be necessary to dissect beneath the pancreas rather
than to incise through normal pancreatic parenchyma to access the cyst.
◆ Be sure that your imaging is recent. In the event that a month or more has elapsed since
the last imaging, there is a possibility that the cyst has changed or disappeared entirely.
◆ We perform a bowel preparation and a colonic cleansing in all patients.
◆ Within 1 hour of surgery, a single intravenous dose of a second-generation cephalosporin is
given.
STEP 3: OPERATIVE STEPS
1. INCISION AND EXPOSURE
◆ We use an upper abdominal midline incision, although subcostal or transverse incisions
may be preferable depending on the location of the cyst and the anticipated mode of
bypass. We use self-retaining retractors to afford visualization.
CHAPTER 51 • Pseudocysts 581

582 Section VII • Pancreas
2. DISSECTION
Cystogastrostomy
◆ When the decision is made to proceed with cystogastrostomy, the operative procedure is
fairly simple (Figure 51-1). Two stay sutures of 3-0 silk stitch are placed in the anterior
wall of the stomach after palpating the cyst to confi rm the incision will be placed exactly
over the primary palpable body of the pseudocyst. After these two sutures are placed on the
superior and inferior margin of the anticipated gastrotomy, electrocautery is used to perform
an anterior gastrotomy for a length of approximately 8 cm. After this is done, one can easily
palpate the connection between the pseudocyst and the posterior wall of the stomach
(Figure 51-2).
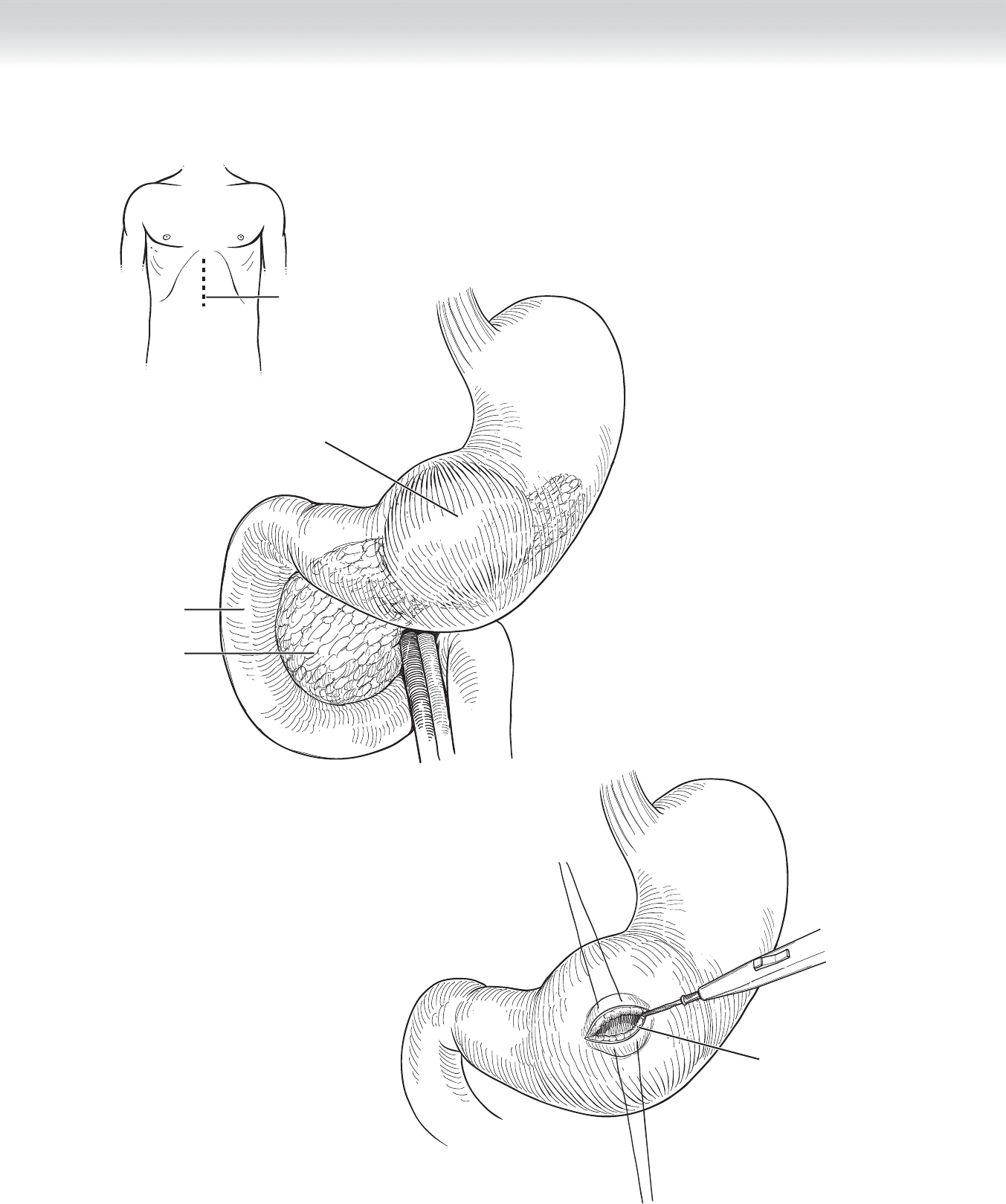
Duodenum
Pseudocyst
Stomach
Pancreas
Incision
Anterior wall gastrotomy
FIGURE 51 –1
FIGURE 51 –2
CHAPTER 51 • Pseudocysts 583