Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 52 • Splenectomy/Splenic Repair 605
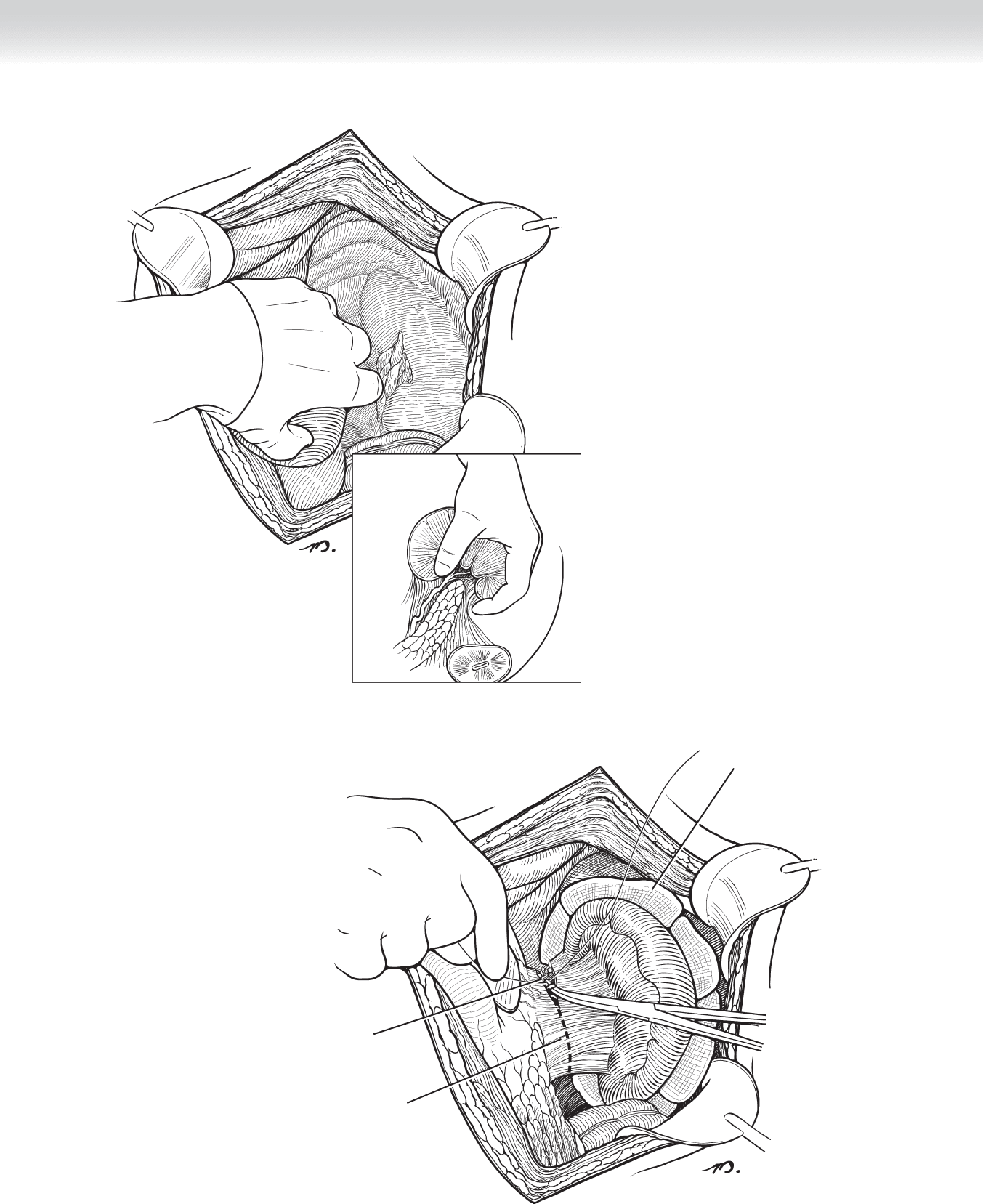
Retropancreatic, prenephric plane
of dissection manually dissected
FIGURE 52 –3
Laparotomy pads packed
behind spleen to tamponade
bleeding
Short gastric
vessels ligated
Splenocolic ligament
divided
FIGURE 52 –4
606 Section VIII • Spleen
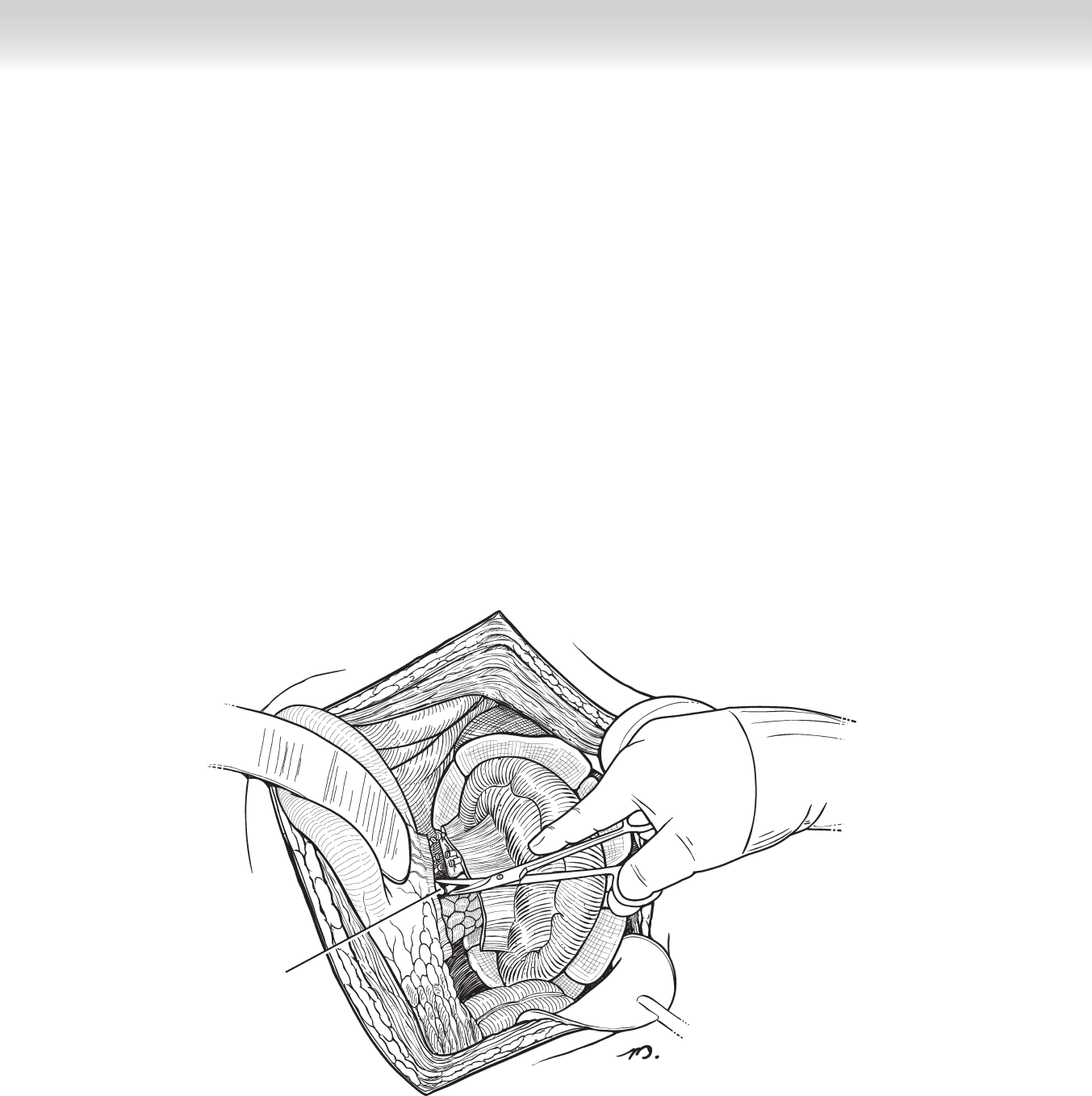
◆ After the spleen is mobilized to the midline, it can be rapidly determined whether the in-
jury has active hemorrhage that will require splenectomy or is a more modest injury ame-
nable to splenorrhaphy or mesh wrapping. If the patient is hypotensive, coagulopathic,
acidotic, or hypothermic or has multiple other injuries that contribute to or are worsened
by ongoing hemorrhage (closed head injury), the decision to control hemorrhage by sple-
nectomy is straightforward and should be made rapidly (Figure 52-5).
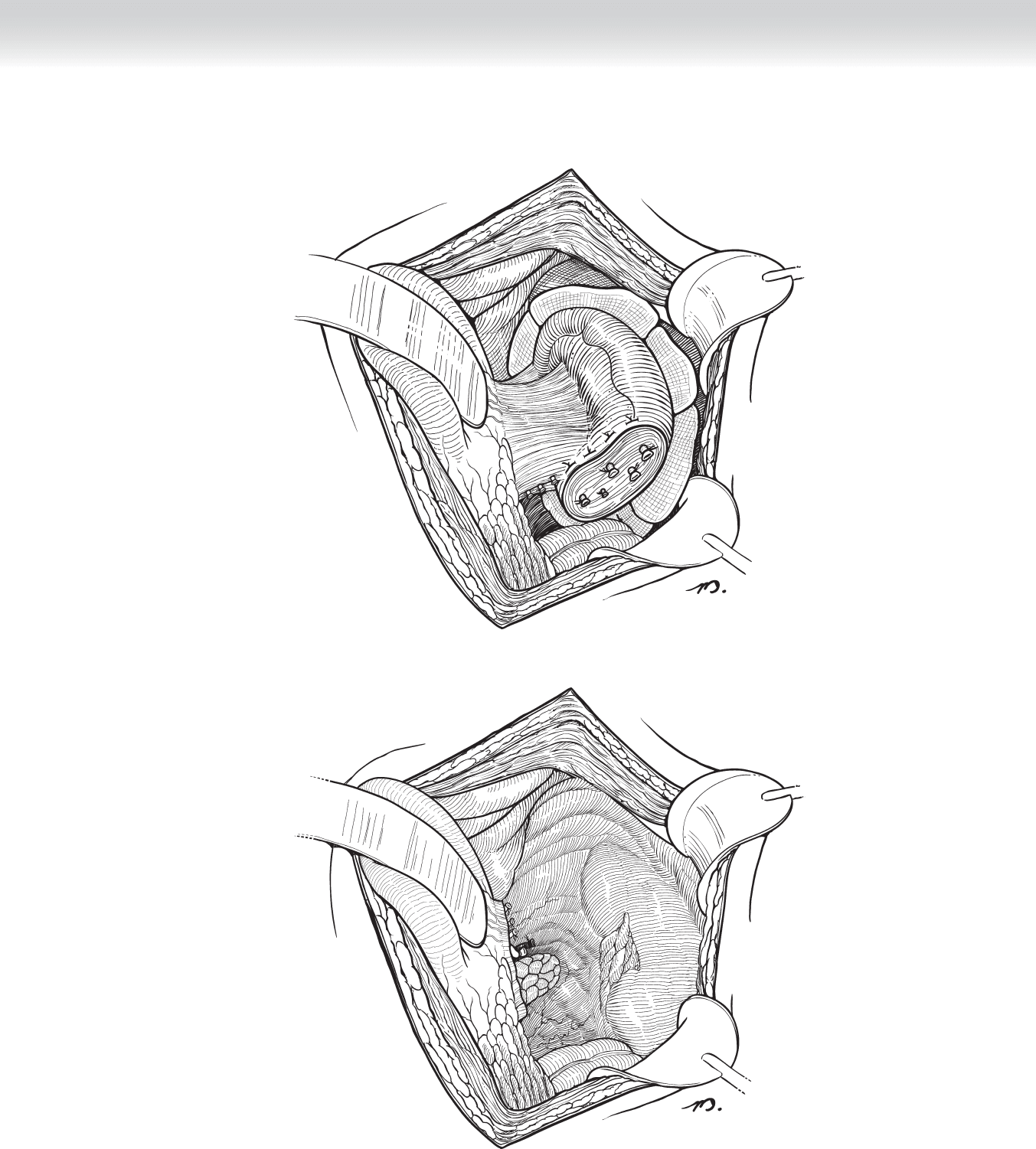
◆ In patients who respond to control of the bleeding and resuscitation, splenorrhaphy re-
mains an option. This can be accomplished with topical hemostatic agents, suture ligature
with or without pledgets, and in some cases, wrapping of the spleen in absorbable mesh
(Figure 52-6).
◆ The splenic fossa should be carefully examined for hemorrhage and possible injury to the
pancreas before closing. If there is evidence of or reasonable concern for possible injury to
the pancreas, a closed suction drain should be left in the splenic bed (Figure 52-7).
Splenic artery and
vein are ligated and
divided
FIGURE 52 –5
CHAPTER 52 • Splenectomy/Splenic Repair 607
FIGURE 52 –6
FIGURE 52 –7

608 Section VIII • Spleen
3. CLOSING
◆ Although nonoperative management is successful in more than 80% of patients with spleen
injuries, rapid emergent operative treatment may be required.
◆ It cannot be overemphasized that nonoperative treatment is applicable only when the patient
is hemodynamically stable. Patients who have evidence of signifi cant hemoperitoneum, in-
cluding signifi cant free fl uid surrounding loops of small intestine; those with contrast blush
on the CT scan; those taking anticoagulants (warfarin [Coumadin], clopidogrel [Plavix]);
those with portal hypertension; those with multiple injuries that may increase the risk from
hemorrhage or intracranial injury; and the elderly are at increased risk of ongoing hemorrhage
and failure of nonoperative treatment.
◆ When operative intervention is indicated, exposure and full mobilization of the spleen are
essential to either splenorrhaphy or splenectomy.
STEP 4: POSTOPERATIVE CARE
◆ A nasogastric tube is continued in place until evidence of effective gastric emptying is
clearly present. Incentive spirometry and pulmonary toilet are important to limit postopera-
tive atelectasis and pneumonia. Prophylaxis for deep venous thrombosis (DVT) with frac-
tionated heparin may begin on postoperative day 1. In the patients who undergo splenec-
tomy, immunization against pneumococcus, meningococcus, and Haemophilus infl uenzae
should be administered before discharge from the hospital.
STEP 5: PEARLS AND PITFALLS
◆ Pancreatic fi stula may occur following splenectomy as a result of pancreatic trauma or iatro-
genic injury. Careful inspection of the tail of the pancreas and taking care to avoid pancre-
atic injury while ligating the vasculature of the spleen are the best preventative measures. If
there is concern that the tail of the pancreas might be damaged at the time of surgery, a
closed suction drain should be left and effl uent assayed for amylase and lipase levels before
the drain is removed.
◆ Gastric fi stula following splenectomy is a recognized complication that can be avoided by
careful ligation of the short gastric vessels without including any of the gastric serosa, or if
necessary imbricating the short gastric ligatures.
◆ Overwhelming postsplenectomy sepsis may occur.

◆ The spleen contributes to immune competence in a variety of ways, including opsonization
and phagocytosis. Asplenic patients are at increased risk of overwhelming postsplenectomy
infection from encapsulated bacteria, such as Streptococcus pneumoniae, Neisseria meningit-
idis, and H. infl uenzae. Following splenectomy patients should be counseled regarding the
increased susceptibility to infections and vaccinated against these potential infections with
Prevnar, Menactra, and ActHIB before discharge from the hospital.
SELECTED REFERENCES
1. Starnes S, Klein P, Magagna L, Pomerantz R: Computed tomographic grading is useful in the selection of
patients for nonoperative management of blunt injury to the spleen. Am Surg 1998;64:743-648;748-749
[discussion].
2. Cocanour CS, Moore FA, Ware DN, et al: Delayed complications of nonoperative management of blunt
adult splenic trauma. Arch Surg 1998;133:619-624;624-625 [discussion].
3. Ochsner MG: Factors of failure for nonoperative management of blunt liver and splenic injuries. World
J Surg 2001;25:1393-1396.
CHAPTER 52 • Splenectomy/Splenic Repair 609
612
STEP 1: SURGICAL ANATOMY
◆ It is useful to review the anatomy of the abdominal musculature when planning a laparo-
scopic operation.
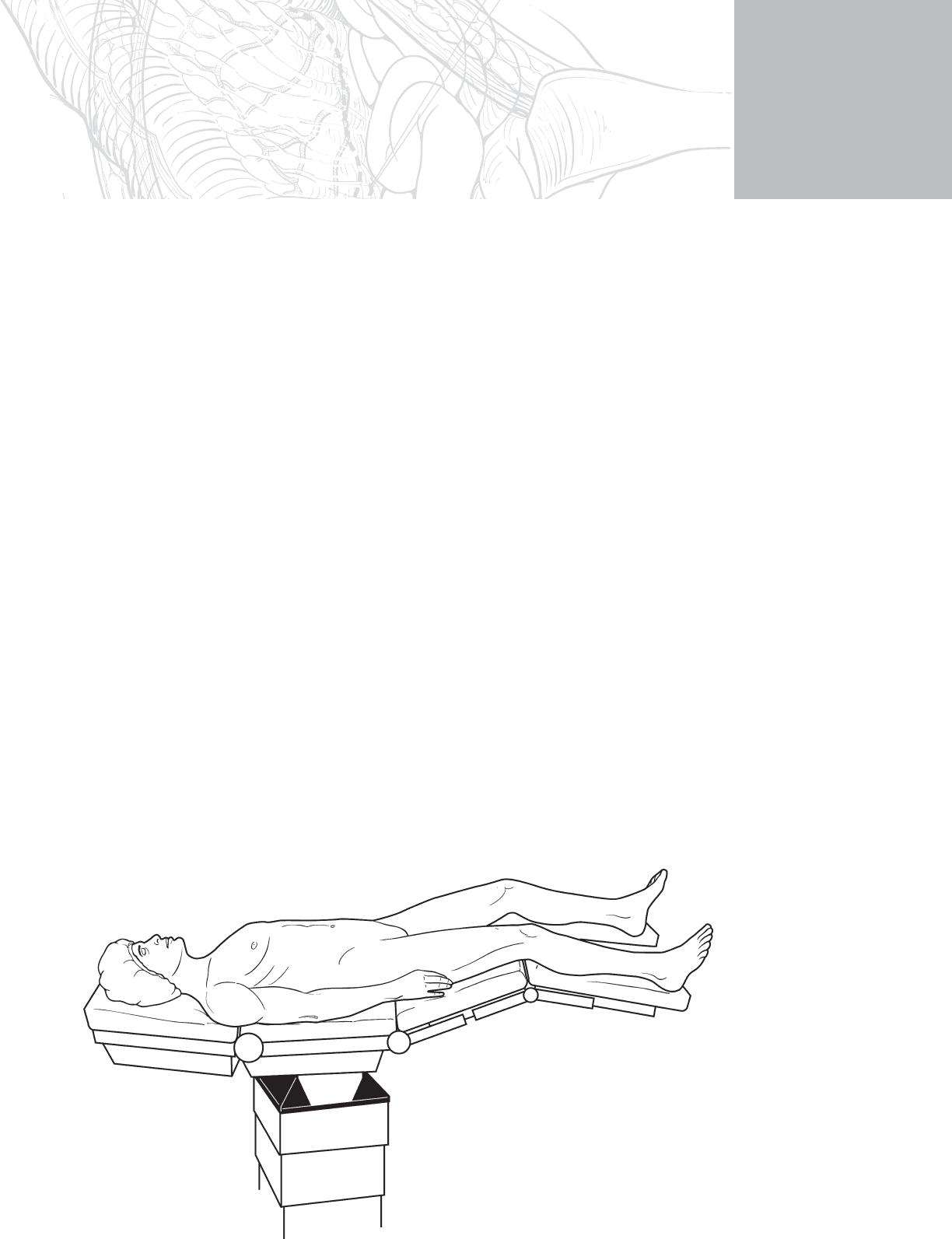
STEP 2: PREOPERATIVE CONSIDERATIONS
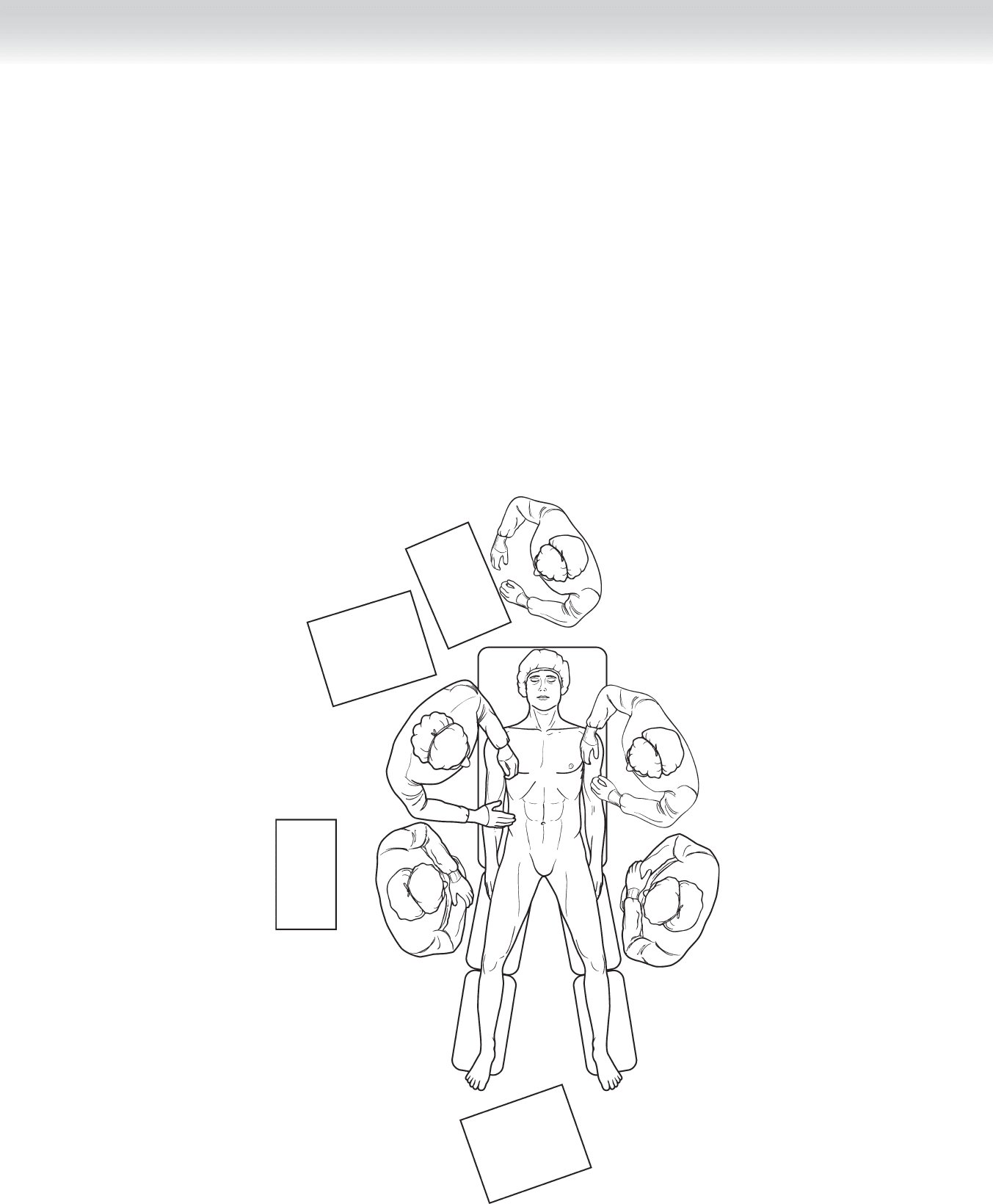
◆ Laparoscopic colonic surgery is usually performed with the patient in the modifi ed lithotomy
position. The lower extremities should not be fl exed so much as to interfere with movement
of the long laparoscopic instruments (Figure 53-1). When tucking the upper extremities,
protect the hand from entrapment in the movement of the bed surfaces.
CHAPTER
53
Port Placement for Colon
Operations
Michael D. Trahan
FIGURE 53 –1
CHAPTER 53 • Port Placement for Colon Operations 613
◆ The principle of triangulation of the operative target should be kept in mind as the plan for
port placement is developed. In general, the surgeon should position the operative target
between himself or herself and the monitor screen. For a sigmoid colectomy, the surgeon
stands at the patient’s right and the monitor is at the foot (Figure 53-2). The surgeon
should move from the patient’s right to the left or between the legs as needed to comfort-
ably reach the target.
◆ An optically guided bladeless trocar is the best selection for the initial port to be inserted.
The optical guidance is provided by an end-viewing laparoscope. This port is usually placed
at or near the umbilicus but may be placed elsewhere in patients who are expected to have
midline adhesions.
◆ The size, selection, and number of the remaining ports are subject to much variability depend-
ing on the planned procedure, size and type of anticipated instruments, patient’s body habitus,
and surgeon’s preference.
Monitor
Light source
Camera
Insufflator
Monitor
Video recorder
Irrigation
Electrosurgical
unit
Anesthetist
Second assistant
First assistant Surgical technician
Surgeon
FIGURE 53 –2

614 Section IX • Colon
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The site of each incision should be preemptively anesthetized with a local anesthetic injec-
tion to include the skin and peritoneum.
◆ The incisions should be just large enough to accommodate the trocar without tension on
the skin as the trocar is inserted.
2. DISSECTION
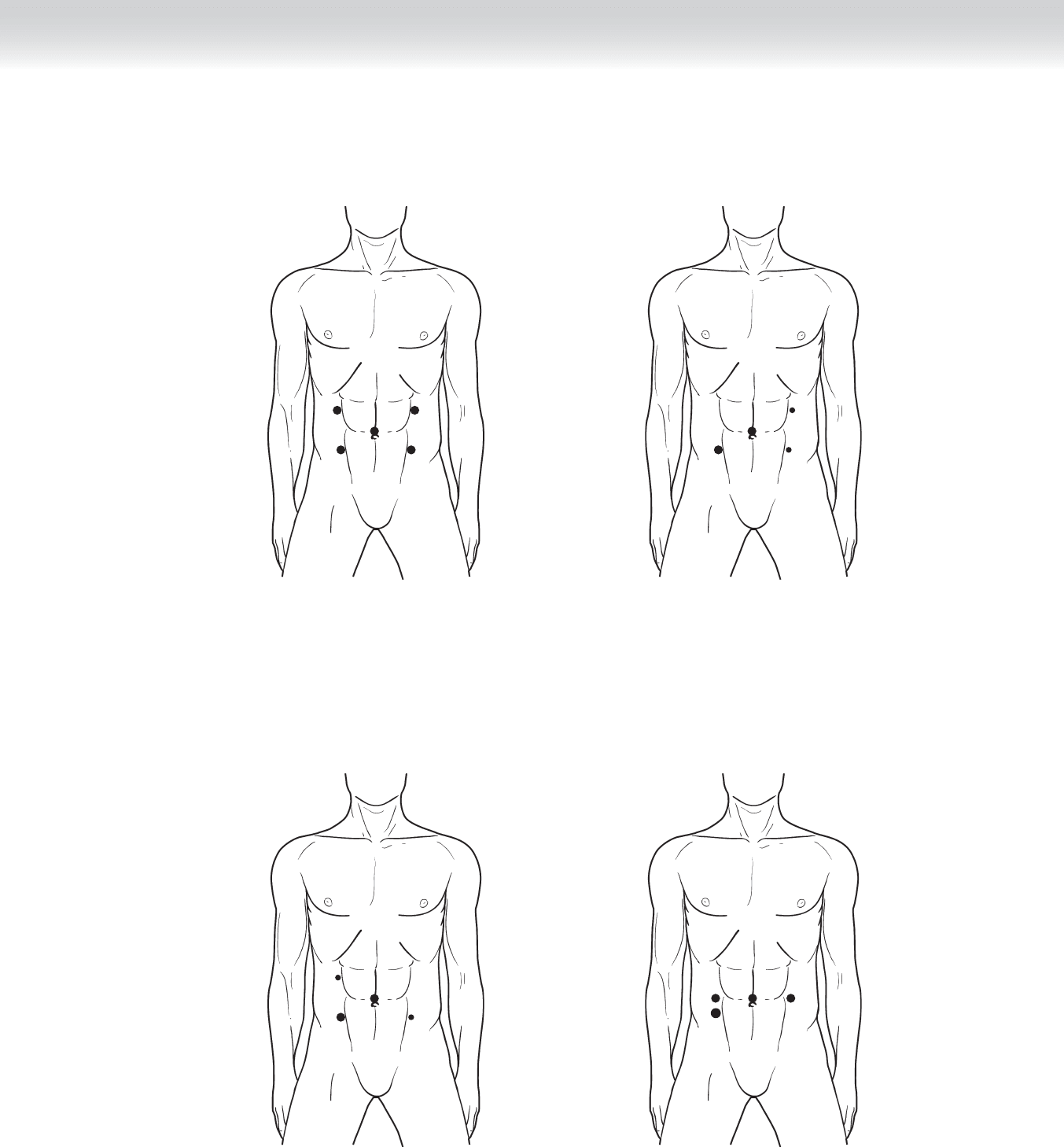
◆ Five 10- to 12-mm ports are used. One port is near the umbilicus. One port is in each of
the abdominal quadrants lateral to the rectus muscles (Figure 53-3).
◆ A 10- to 12-mm port is near the umbilicus. A 5- or 10-mm port is in the left lower quad-
rant. A 10- to 12-mm port is in right lower quadrant. A 5- or 10-mm port is in the left
upper quadrant (Figure 53-4).
◆ A 10- to 12-mm port is near the umbilicus. A 10- to 12-mm port is in the right lower
quadrant. A 5- or 10-mm port is in the right upper quadrant. A 5- or 10-mm port is in the
left lower quadrant (Figure 53-5).
◆ Four 10- to 12-mm ports are used. One port is near the umbilicus. One port is in each of
the mid-clavicular lines at the level of the umbilicus. One port is in the right mid-clavicular
line, 10 to 15 cm inferior to the other (Figure 53-6).
3. CLOSING
◆ Bladeless trocar port sites up to and including 12 mm do not typically need to be closed at
the fascial level.
◆ Transabdominal laparoscopic suture passers provide a quick and relatively simple way to
close small abdominal fascial incisions, especially through a deep abdominal pannus.
◆ If no suture passer is available, larger port site fascial defects should be closed with transab-
dominal suture externally after appropriate retraction of the skin and subcutaneous tissue.
CHAPTER 53 • Port Placement for Colon Operations 615
FIGURE 53 –3
FIGURE 53 –4
FIGURE 53 –5
FIGURE 53 –6

616 Section IX • Colon
STEP 4: POSTOPERATIVE CONSIDERATIONS
◆ Postoperative care is provided consistent with the primary disease process and extent of the
operation.
STEP 5: PEARLS AND PITFALLS
◆ The initial optical entry should be made away from sites expected to have adhesions. In a
patient with extensive prior surgical history, the open insertion technique may be preferred.
◆ Each subsequent trocar entry should be made with direct internal visualization, avoiding
the epigastric vessels and the large subcutaneous vessels identifi ed by transillumination.
◆ One should not hesitate to use additional trocars if needed to improve exposure and the
safety of the operation.
◆ Hand-assisted laparoscopic surgery (HALS) is the approach favored by many. The hand port
should be located at the proposed site of specimen extraction.
SELECTED REFERENCES
1. Ludwig KA, Lee WY: Laparoscopic partial colectomy. In Soper NJ, Swanstrom LL, Eubanks WS (eds):
Mastery of Endoscopic and Laparoscopic Surgery, 2nd ed. Philadelphia, Lippincott Williams & Wilkins,
2005, pp 436-448.
2. Baig MK, Wexner SD: Laparoscopic-assisted abdominoperineal resection. In Soper NJ, Swanstrom LL,
Eubanks WS (eds): Mastery of Endoscopic and Laparoscopic Surgery, 2nd ed. Philadelphia, Lippincott
Williams & Wilkins, 2005, pp 449-458.
3. Fowler DL, Sonoda TS, McGinty J: Laparoscopic subtotal and total colectomy. In Soper NJ, Swanstrom LL
and Eubanks WS (eds): Mastery of Endoscopic and Laparoscopic Surgery, 2nd ed. Philadelphia, Lippincott
Williams & Wilkins, 2005, pp 459-469.