Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 89 • Mesenteric Ischemia 981
SELECTED REFERENCES
1. Foley MI, Moneta GL, Abou-Zamzam AM, et al: Revascularization of the SMA alone for treatment of
intestinal ischemia. J Vasc Surg 2000;32:37-47.
2. Morasch MD, Ebaugh JL, Chiou AG, et al: Mesenteric venous thrombosis: A changing clinical entity.
J Vasc Surg 2001;34:680-684.
3. Wylie EJ, Stoney RJ, Ehrenfeld WK: Manual of Vascular Surgery. New York, Springer Verlag, 1980.

982
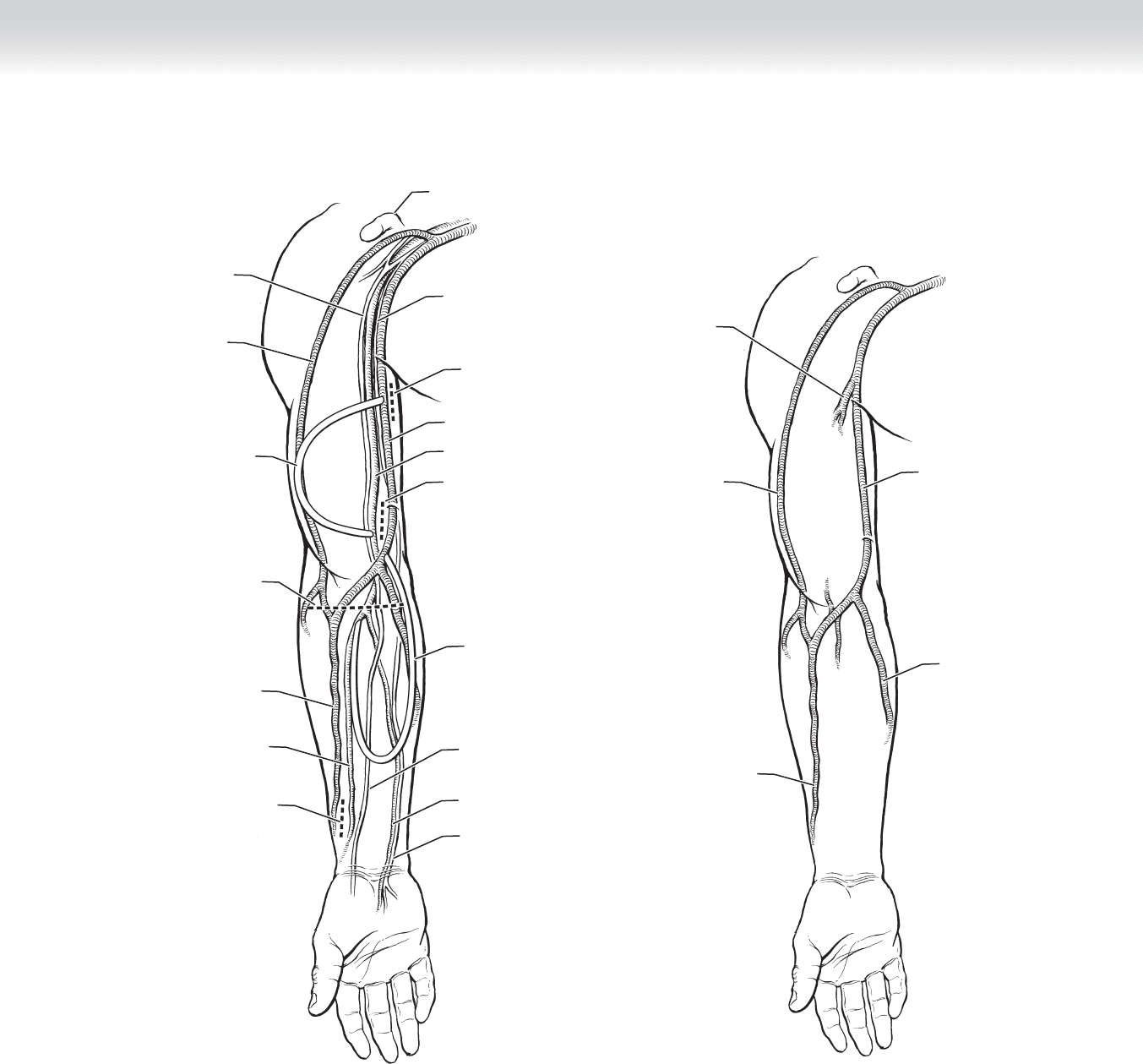
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of both the arterial infl ow and venous outfl ow of the arm
and forearm is critical to the successful placement and maintenance of hemodialysis access.
◆ Figure 90-1 demonstrates typical target sites for arterial and venous anastomoses.
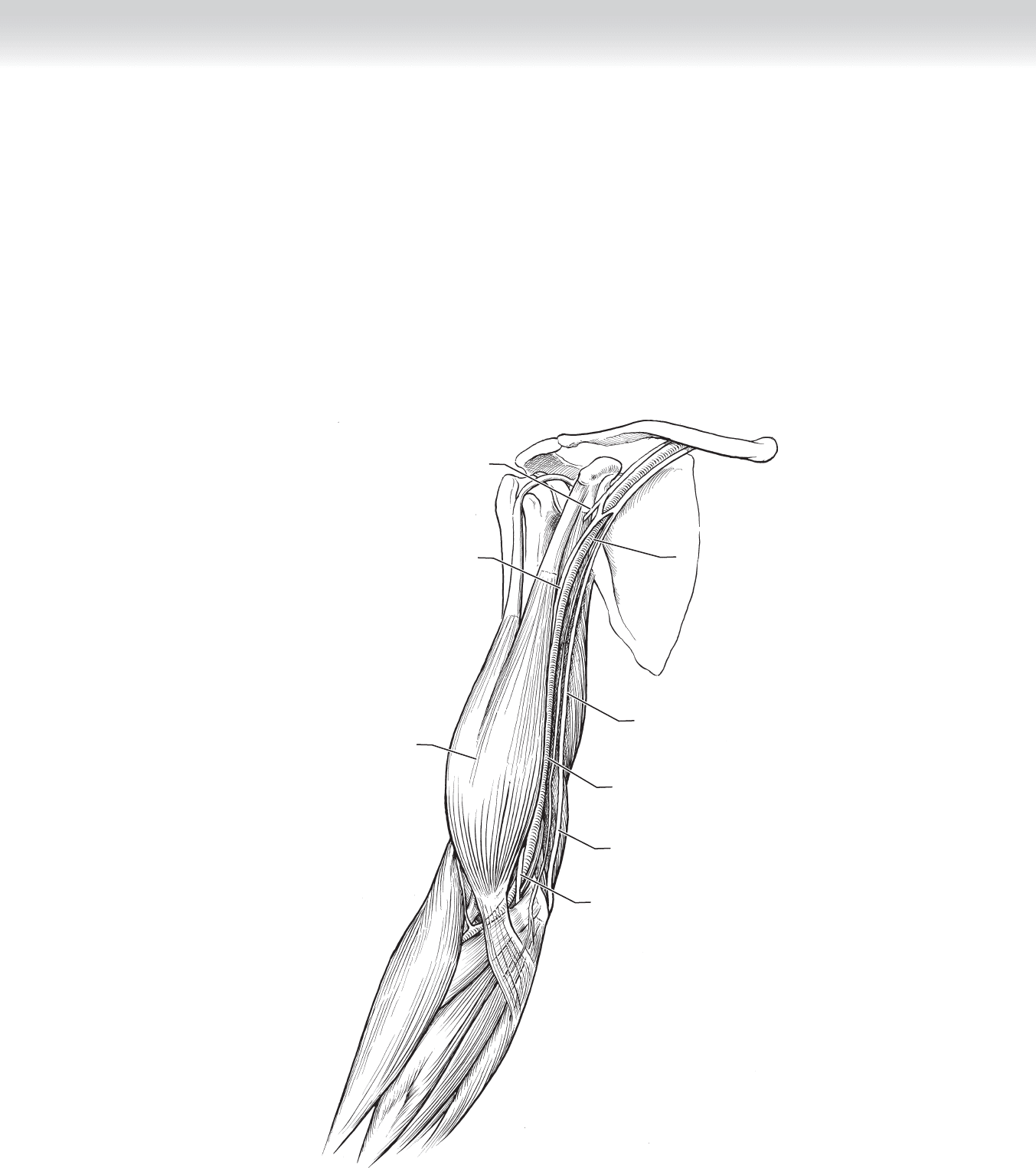
◆ Figures 90-2 through 90-4 demonstrate key anatomic relationships underlying operative
planning.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Placement of new access should be initiated several months before the anticipated need for
hemodialysis to allow time for fi stula maturation and troubleshooting, as well as to avoid
catheter placement and the associated risk of central vein stenosis.
◆ Physical examination for compressible veins in the forearm and arm should be performed,
as well as Allen’s test for palmar arch patency. Any history of congestive heart failure, diabe-
tes, intravenous drug use, or chemotherapy should be elicited.
◆ In most patients, preoperative vein mapping should be obtained to maximize the creation
of arteriovenous fi stulae over graft placement. Target veins should have a diameter larger
than 3 mm, although smaller distendable veins may be used.
◆ Access creation should occur in the nondominant forearm fi rst, starting at the most distal
site possible. Strategic placement of access is important to maximize the number of sites
available over the life of the patient.
◆ In patients with more subcutaneous fat, consider vein transposition to make the vein closer
to the skin surface and more accessible by the dialysis center.
CHAPTER
90
Hemodialysis Access Procedures
Kenneth J. Woodside
CHAPTER 90 • Hemodialysis Access Procedures 983
MC
Cephalic vein
Cephalic vein
Radial artery
Possible route
of graft
Possible route
of graft
Ulnar nerve
Median nerve
Coracoid
Median nerve
Basilic vein
Incision for Cimino
arteriovenous fistula
Incision for
basilic vein
Incision for
brachial artery
anastomosis
Incision for
arteriovenous fistula
Brachial artery
Ulnar artery
Ulnar nerve
FIGURE 90 –1
Cephalic vein
Cephalic vein
Brachial vein
(deep)
Basilic vein
Basilic vein
FIGURE 90 –2

984 Section XII • Vascular
Radial nerve
Brachioradialis
muscle
Superficial branch of
radial nerve
Biceps muscle
tendon
Pronator teres muscle
Brachialis
muscle
Ulnar nerve
Median nerve
Brachial artery
Radial artery
Median nerve
Flexor digitorum
superficialis muscle
Ulnar artery
Ulnar nerve
FIGURE 90 –3
◆ Steal syndrome, in which too much blood is shunted away from the hand, is more likely to
occur in patients with diabetes and in those with upper extremity atherosclerotic disease. In
addition, placement of the access above the elbow or use of synthetic conduit increases the
risk of steal symptoms.
◆ The axilla and shoulder must always be included in the surgical fi eld. Fistulograms, shunto-
grams, and central venograms are often required, so a suitable vascular bed and arm board
should be used. Preoperative antibiotics should be given at the appropriate time. Regional
anesthesia may promote venous dilation and assist in successful fi stula creation.
CHAPTER 90 • Hemodialysis Access Procedures 985
Brachial artery
Axillary artery
Axillary artery
Axillary artery
Median nerve
Median nerve
Musculocutaneous
nerve
Ulnar nerve
Ulnar nerve
Biceps muscle
FIGURE 90 –4
986 Section XII • Vascular
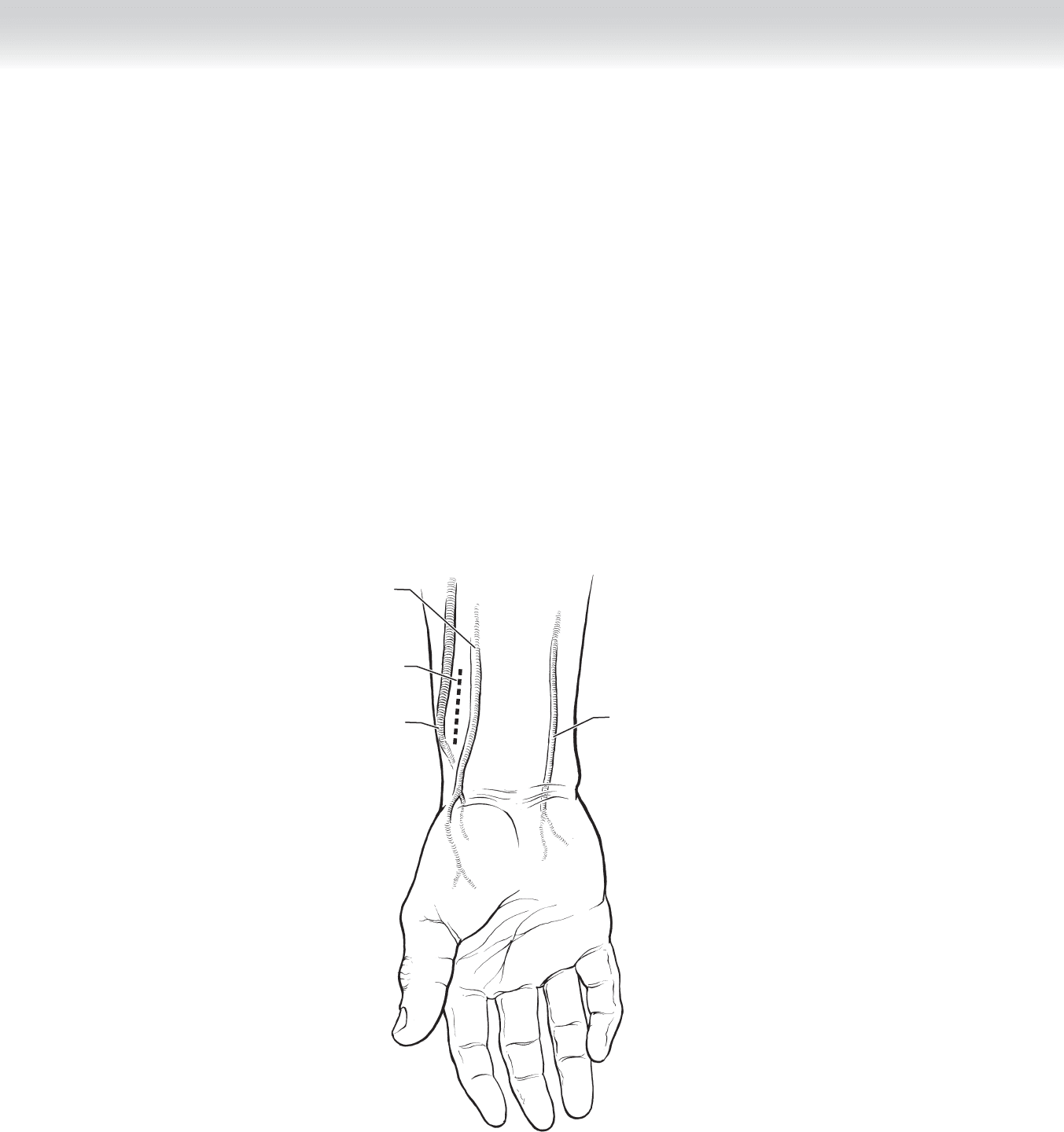
STEP 3: OPERATIVE STEPS—RADIOCEPHALIC ARTERIOVENOUS FISTULA
1. INCISION
◆ The patient is placed supine, with the arm placed on an arm board.
◆ The radial artery and the target cephalic vein are located. Intraoperative ultrasound can help
the surgeon localize the vein and reassess patency of the vessel.
◆ A longitudinal incision is made between the target vein and the radial artery (Figure 90-5).
Radial artery
Incision for
atreriovenous
anastomosis
Cephalic vein
Ulnar artery
FIGURE 90 –5
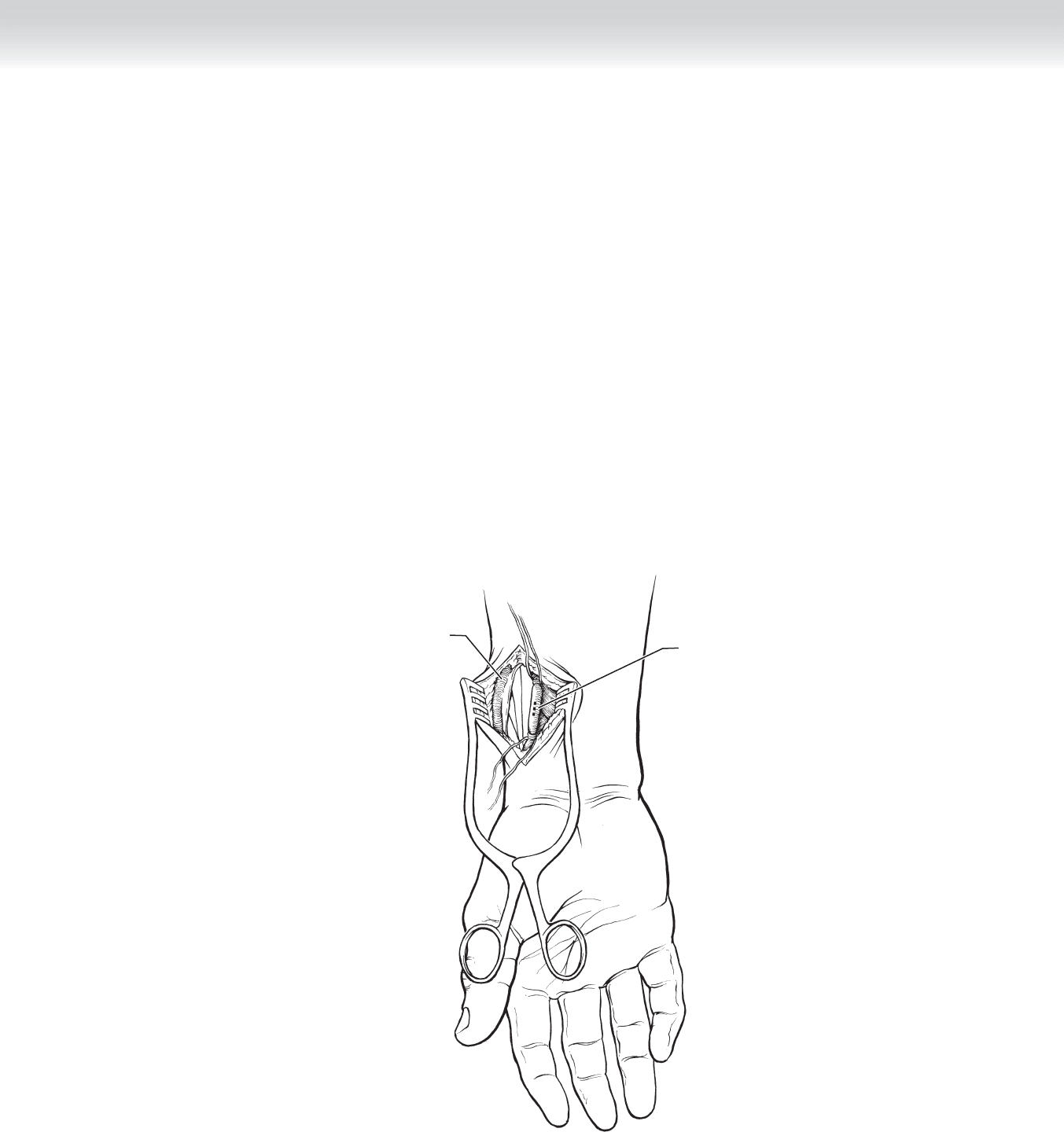
CHAPTER 90 • Hemodialysis Access Procedures 987
Cephalic vein
Incision for
arteriotomy in
radial artery
FIGURE 90 –6
2. DISSECTION
◆ A small fl ap is made to allow mobilization of the cephalic vein. The vein is mobilized for a
short distance and assessed for adequacy.
◆ The fascia over the radial artery is incised, and proximal and distal control of the vessel is
obtained (Figure 90-6).
◆ The cephalic vein is divided as distally as possible, fl ushed with heparinized saline, and
dilated manually.
◆ The patient is heparinized, and proximal and distal arterial clamps are placed.
988 Section XII • Vascular
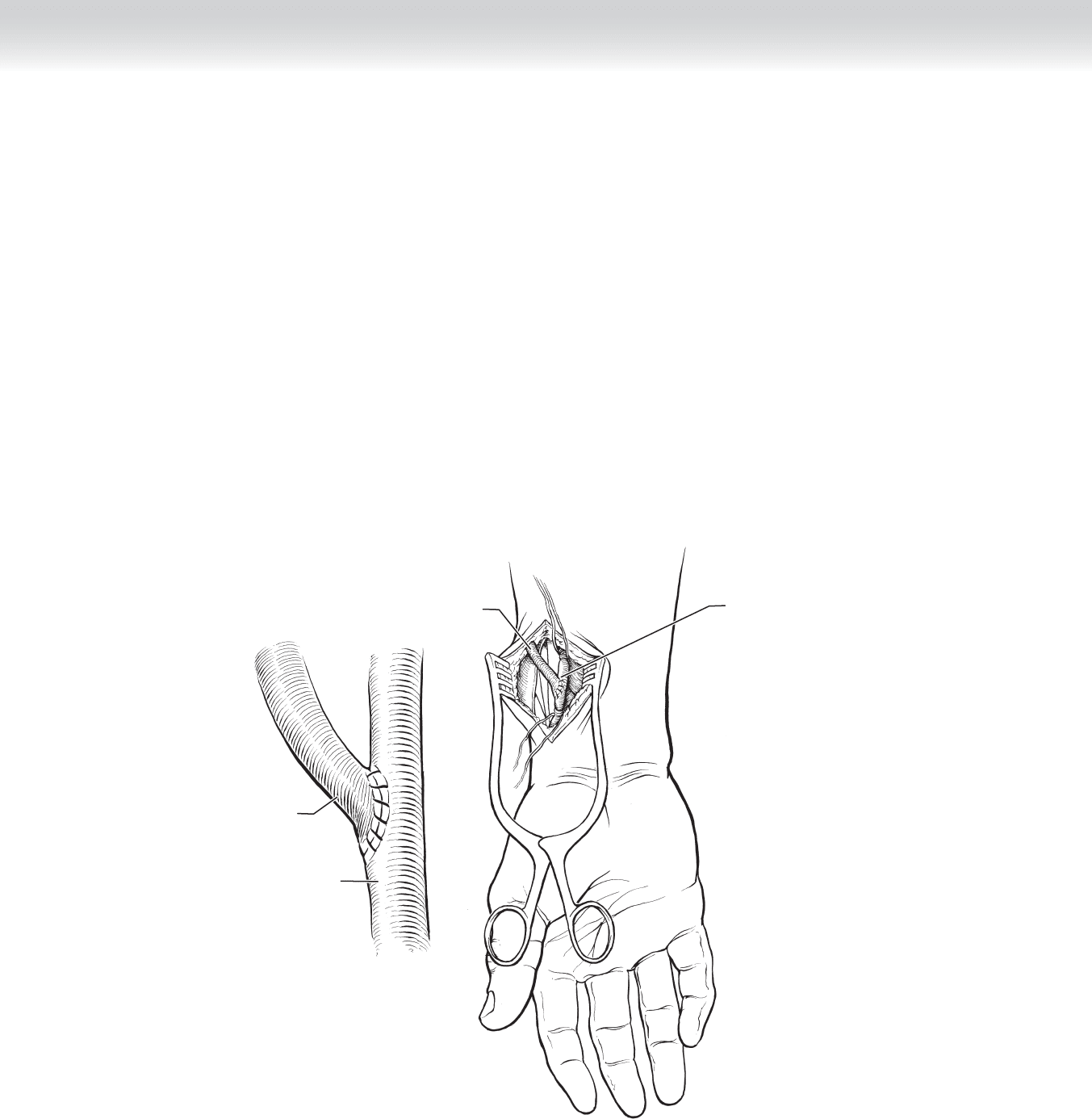
◆ An end-to-side anastomosis is performed with 6-0 Prolene suture (Figure 90-7).
◆ The clamps are removed, with the distal arterial clamp removed last. The cephalic vein is
palpated for a thrill. Revision may be necessary if a thrill is not readily palpable. If the
fi stula is pulsatile without a thrill, a distal obstruction may be present. If the obstruction is
not from inadequate vein mobilization, a venogram may need to be performed.
3. CLOSURE
◆ The wound is closed in two layers with interrupted 3-0 Vicryl subcutaneous sutures and a
running 4-0 Monocryl subcuticular layer.
Cephalic vein
Arteriovenous
end-to-side
anastomosis
Radial artery
Cephalic vein
FIGURE 90 –7
CHAPTER 90 • Hemodialysis Access Procedures 989
STEP 3: OPERATIVE STEPS—ANTECUBITAL ARTERIOVENOUS FISTULA
1. INCISION
◆ The patient is placed supine, with the arm placed on an arm board.
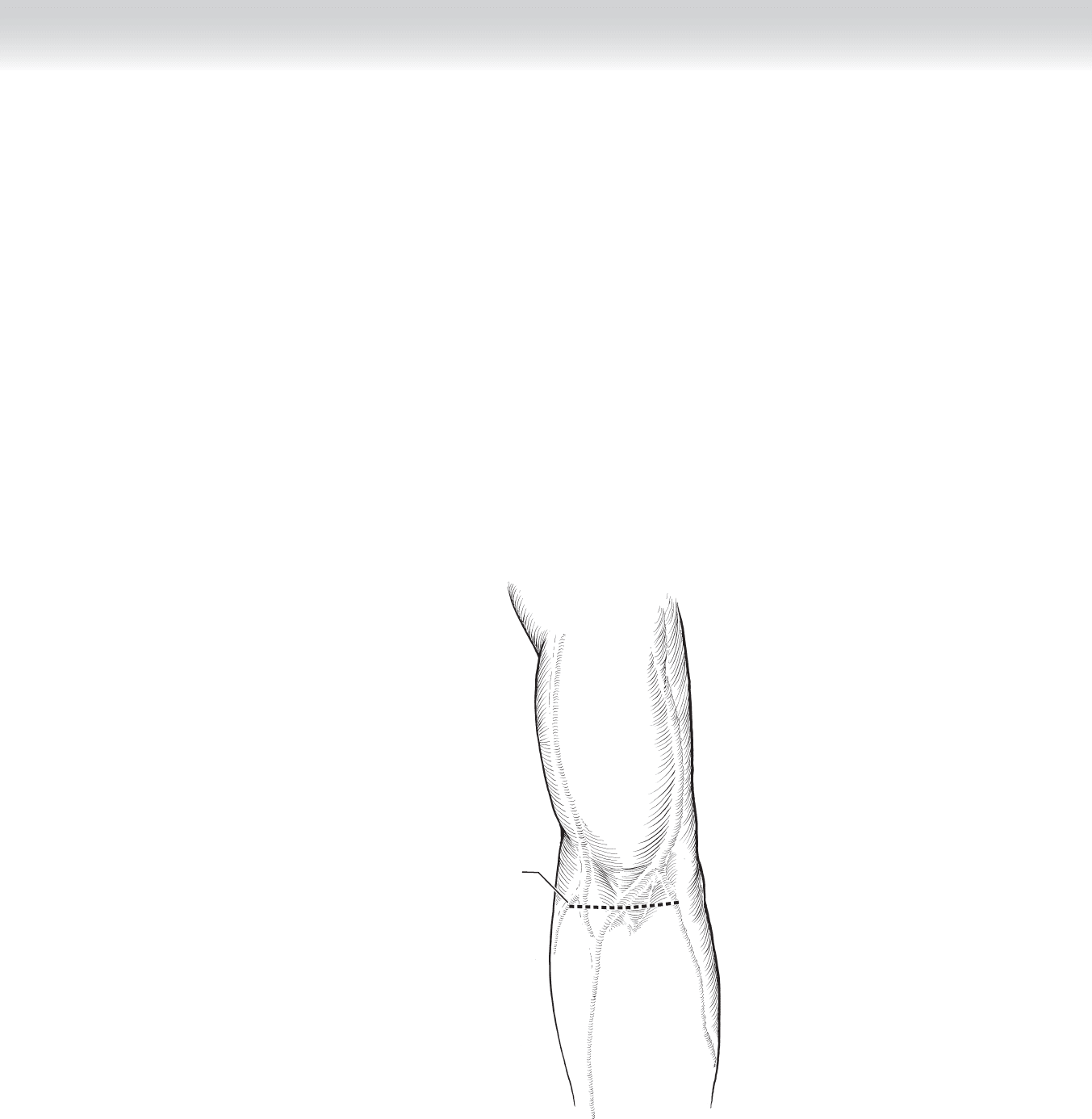
◆ Approximately 1 cm below the antecubital crease, a horizontal incision is made, with care
taken to preserve the subcutaneous veins (Figure 90-8).
Incision for
arteriovenous
fistula
FIGURE 90 –8

990 Section XII • Vascular
2. DISSECTION
◆ A suitable antecubital vein is identifi ed and mobilized. The basilic, cephalic, or antecubital
bridging veins are typically used. Strategically, fl ow through the cephalic vein will be easier
to access at the dialysis center (Figure 90-9).
◆ The brachial arterial pulse is identifi ed just proximal to the elbow. The bicipital aponeurosis
is divided, exposing the artery. Proximal and distal control is obtained. Communicating
veins overlaying the artery may need to be divided to allow adequate control. Care must be
taken to avoid damage to the nearby median nerve (Figure 90-10).
◆ The vein is divided as distally as possible, fl ushed with heparinized saline, and dilated
manually.
◆ The patient is heparinized, and proximal and distal arterial clamps are placed.