Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 88 • Renal Revascularization 961
Right renal vein
retracted cephalad
Dividing
right renal artery
E
Saphenous vein graft
Proximal anastomosis
Completing distal
anastomosis
Saphenous vein graft
F
Completed hepatorenal
bypass
G
FIGURE 88 –6, cont’d

962 Section XII • Vascular
3. CLOSING
◆ Both of the inner two layers of the right and left subcostal incisions are closed in a similar
fashion with running absorbable suture (2-0 Vicryl), and the outer layers (external oblique
and anterior rectus fascia) are closed with running monofi lament (2-0 PDS or Maxon)
suture.
STEP 4: POSTOPERATIVE CARE
◆ The patient is returned to the ICU with arterial line and Swan-Ganz pulmonary artery
catheter in place. IV fl uids are administered to control fl uid volume and blood pressure.
Nicardipine or sodium nitroprusside is used to control blood pressure. Beta blockade begun
in the preoperative period is continued to control heart rate and blood pressure. Urine out-
put is carefully monitored, and IV fl uid administration is adjusted accordingly.
◆ There are often signifi cant fl uid shifts in the immediate postoperative period. A combina-
tion of fl uid administration, vasopressors, and antihypertensive medications may be
required to ensure adequate perfusion pressures and to prevent hypertensive crises.
STEP 5: PEARLS AND PITFALLS
◆ The renal artery should be carefully palpated to determine the distal extent of the plaque
before an aortorenal bypass or endarterectomy is performed. This maneuver is especially
important if endarterectomy is contemplated if diffi culties with the end point are to be
avoided.
◆ Each renal anastomosis should be completed in 15 to 20 minutes. If prolonged renal ische-
mic times are anticipated, cold electrolyte solution can be infused into the renal artery and
the kidney packed in ice.
◆ Immediate evaluation of the patency of the repair with duplex ultrasound or renal isotope
fl ow studies is indicated if anuria develops in the postoperative period. Prompt return to
the operating room is indicated if the vessels are occluded.
◆ Atheroembolism is an uncommon but serious complication of renal revascularization. Care-
ful preoperative assessment of the aorta to determine the presence and location of athero-
matous debris or thrombus on a CT scan and the correct sequential application and
removal of clamps is imperative if this complication is to be avoided. Oliguria or anuria that
does not resolve, eosinophilia, and cholesterol crystalluria are clues to the diagnosis.
◆ In patients with oliguric acute renal failure dialysis, enteral or parenteral nutrition should
be undertaken early to avoid the rapid loss of muscle mass encountered in these patients.

CHAPTER 88 • Renal Revascularization 963
SELECTED REFERENCES
1. Hansen KJ, Tribble RW, Reavis SW, et al: Renal duplex sonography: Evaluation of clinical utility.
J Vasc Surg 1990;12:227-236.
2. Wylie EJ, Perloff DL, Stoney RJ: Autogenous tissue revascularization techniques in surgery for renovascu-
lar hypertension. Ann Surg 1969;170:416-428.
3. Moncure AC, Brewster DC, Darling RC, et al: Use of the splenic and hepatic arteries for renal revascular-
ization. J Vasc Surg 1986;3:196-203.
4. Benjamin ME, Dean RH: Techniques in renal artery reconstruction: Part I. Ann Vasc Surg 1996;10:
306-314.
5. Benjamin ME, Dean RH: Techniques in renal artery reconstruction: Part II. Ann Vasc Surg 1996;10:
409-414.

964
INTRODUCTION
◆ Despite recent advances in the diagnosis and treatment of mesenteric ischemia, the mortal-
ity rate remains between 59% and 93%. The low incidence of mesenteric ischemia, as well
as the diffi culties and delays encountered in establishing the diagnosis, contributes to
the high morbidity and mortality rates. Acute mesenteric ischemia may either be caused
by thromboembolic occlusive disease (80%) or result from nonocclusive ischemia (20%).
The thromboembolic causes of mesenteric ischemia include mesenteric embolism (50%),
thrombosis of a pre-existing atherosclerotic orifi cial stenosis (20%), and mesenteric venous
thrombosis (10%). Nonocclusive mesenteric ischemia occurs in the absence of anatomic
arterial or venous obstruction and is the result of hypoperfusion-induced vasoconstriction
throughout the entire mesenteric circulation. Chronic mesenteric ischemia is due to athero-
sclerotic occlusive disease in most patients. Less common causes include aortic coarctation,
aortic dissection, mid-aortic stenosis, vasculitides, fi bromuscular dysplasia, neurofi bro-
matosis, and celiac artery compression syndrome.
STEP 1: SURGICAL ANATOMY
◆ The blood supply to the abdominal viscera arises from the celiac, superior mesenteric, infe-
rior mesenteric, and hypogastric arteries. The celiac artery arises from the aorta at the level
of the T12 and L1 vertebral bodies and is 1.5 to 2.0 cm in length. The artery divides into
the left gastric, splenic, and common hepatic arteries. At its origin, the artery is surrounded
by the ganglia and fi bers of the celiac autonomic nerve plexus.
◆ The superior mesenteric artery (SMA) arises 1 cm below the celiac trunk at the L1-L2 inter-
vertebral disc. It lies posterior to the splenic vein and pancreas and is separated from the
aorta by the left renal vein.
◆ The inferior mesenteric artery (IMA), the smaller of the three vessels, arises from the ante-
rior lateral aspect of the aorta at the level of the third lumbar vertebra, approximately 3 to
4 cm above the aortic bifurcation.
◆ The abdominal viscera have a rich collateral blood supply formed by the interconnections
between the three major vessels: the celiac artery and SMA communicate via the superior
and inferior pancreaticoduodenal arteries and the SMA and IMA communicate via the arc of
CHAPTER
89
Mesenteric Ischemia
Glenn C. Hunter

CHAPTER 89 • Mesenteric Ischemia 965
Riolan (middle and left colic arteries). The marginal artery of Drummond formed by anasto-
moses between the main trunks and the arcades arising from the ileocolic, right colic, mid-
dle colic, left colic, and sigmoid arteries, augmented by the superior, middle, and inferior
rectal arteries—branches of the hypogastric arteries.
STEP 2: PREOPERATIVE CONSIDERATIONS
EVALUATION
◆ The modes of presentation of patients with acute mesenteric ischemia are quite varied. The
acute onset of severe abdominal pain, nausea, and vomiting in a patient with cardiac
arrhythmias suggests mesenteric embolism. The exacerbation of symptoms in a patient with
the symptom triad of abdominal pain, fear of eating, and severe weight loss is suggestive of
thrombotic occlusion of a high-grade celiac artery or SMA stenosis. The symptom complex
of diffuse abdominal pain, hypotension, and severe lactic acidosis in the setting of cardio-
genic, septicemic, or hypovolemic shock is suggestive of nonocclusive mesenteric ischemia.
The clinical presentation of mesenteric venous thrombosis is often more insidious and the
physical fi ndings more subtle than those of acute arterial ischemia. However, severe abdom-
inal pain out of proportion to the physical fi ndings is present in more than 80% of patients.
◆ A history of pre-existing congestive heart failure, use of digoxin or ␣-adrenergic agents,
cardiac arrhythmias, valvular heart disease, recent myocardial infarction, cardiopulmonary
bypass, hypercoagulable states, vasculitides, and malignancy should be elicited.
◆ In patients with chronic mesenteric ischemia, severe abdominal pain, fear of food, and
weight loss in patients with atherosclerotic peripheral vascular disease (PVD) or underlying
thrombotic or coagulation disorders should be elicited.
PHYSICAL EXAMINATION
◆ Careful assessment of the abdomen for the presence of distention, tenderness, signs of peri-
toneal irritation, bruits, and presence or absence of femoral pulses should be undertaken.
◆ In the early phases, signs of peritoneal irritation such as guarding and rebound tenderness
are usually absent. As the bowel becomes more ischemic, abdominal distention, absent
bowel sounds, excruciating tenderness, feculent vomiting, and occult bleeding become
evident.
DIAGNOSTIC TESTS
◆ An electrocardiogram should be performed in all patients and an echocardiogram in
selected patients with poor cardiac output. A complete blood count and routine laboratory
chemistries for electrolytes, blood urea nitrogen, creatinine, troponin levels, liver function
tests, and arterial blood gases should be performed. In patients with suspected

966 Section XII • Vascular
hypercoagulable states, blood should be drawn for the prothrombotic work-up before the
administration of heparin. Blood and blood products are typed and crossmatched.
◆ In patients suspected of having acute mesenteric ischemia, a plain abdominal radiograph
may demonstrate “thumbprinting,” ileus, or pneumatosis. A contrast-enhanced computed
tomography (CT) scan with CT angiography provides the defi nitive diagnosis but does not
allow treatment with intra-arterial vasodilators.
◆ Angiography with anterior posterior and lateral views of the aorta is indicated in patients
with acute and chronic mesenteric ischemia and in whom diagnostic uncertainty exists. If
nonocclusive mesenteric ischemia is present, the angiographic catheter is left in place for
the infusion of vasodilators, such as papaverine, nitroglycerin, tolazoline, or verapamil. In
patients with exacerbation or recent onset of symptoms (less than 3 hours) found to have a
high-grade celiac artery or SMA stenosis, angioplasty and stenting should be considered.
◆ Resuscitation with intravenous fl uid is begun while the investigation is ongoing. Broad-
spectrum antibiotics are administered, and any potential underlying mechanism such as
arrhythmias or congestive heart failure is corrected. A heparin infusion is begun to prevent
extension of thrombus into the microvessels.
STEP 3: OPERATIVE STEPS
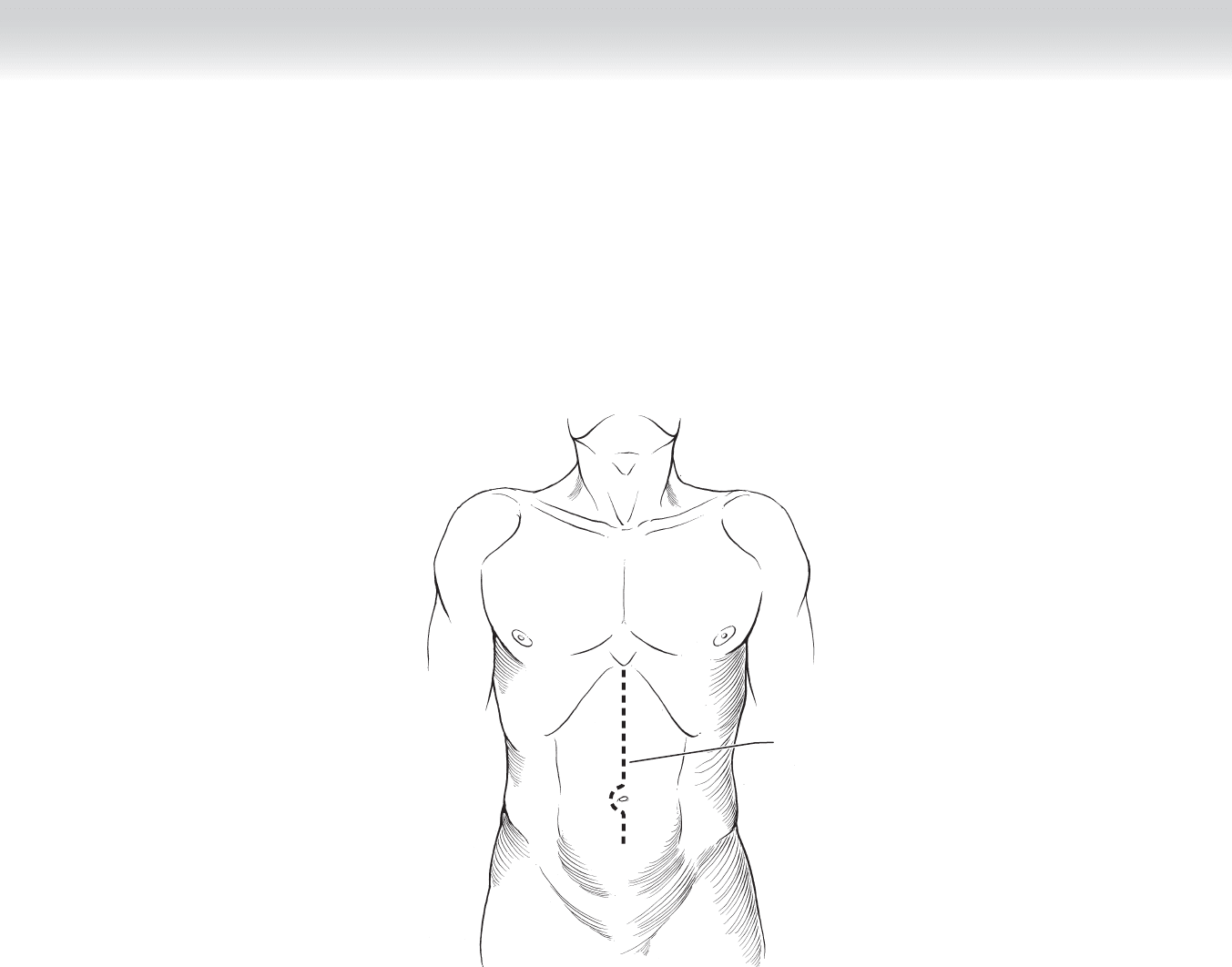
1. INCISION
◆ The abdomen is opened via an upper midline incision, and the extent of the ischemia is
assessed (Figure 89-1). Perfusion of the proximal 10 to 15 cm of jejunum is indicative of
embolic occlusion, whereas bowel ischemia including this segment suggests arterial throm-
bosis. Both the small and large bowel appears dusky if nonocclusive mesenteric ischemia is
present. Segmental ischemic changes with edema of the adjacent mesentery are indicative of
mesenteric venous thrombosis. If the entire bowel is necrotic, the abdomen should be
closed and comfort measures instituted.
CHAPTER 89 • Mesenteric Ischemia 967
MC
Midline incision
FIGURE 89 –1
968 Section XII • Vascular
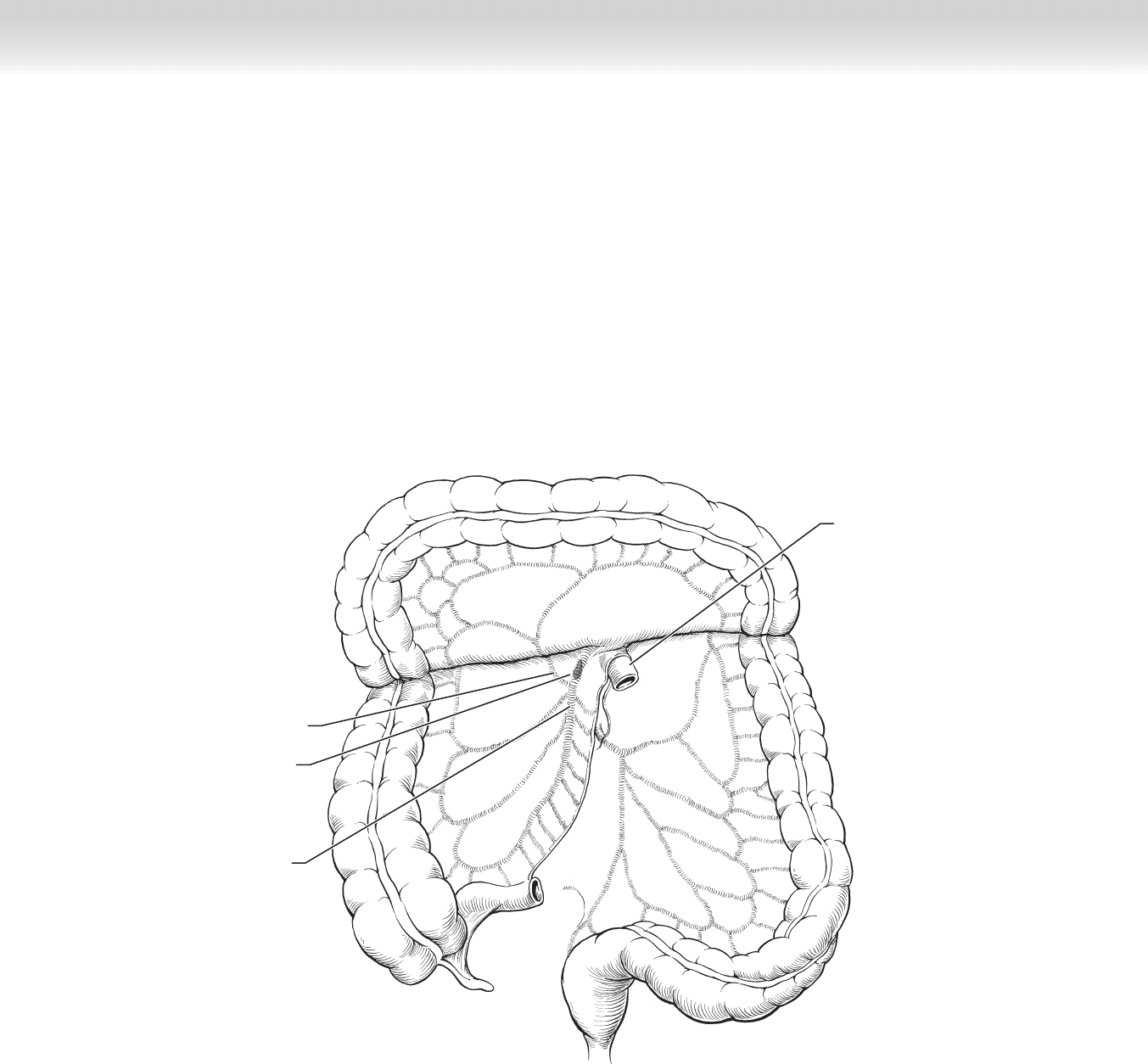
2. DISSECTION
Mesenteric Embolism
◆ The transverse colon is elevated superiorly, and the fourth part of the duodenum is mobi-
lized. The small bowel is retracted to the right, and a self-retaining retractor is placed. The
SMA is isolated at the root of the mesentery and mobilized, taking care to preserve all its
branches (Figure 89-2).
Middle colic
artery
Embolus
Superior
mesenteric
artery
Jejunum
FIGURE 89 –2
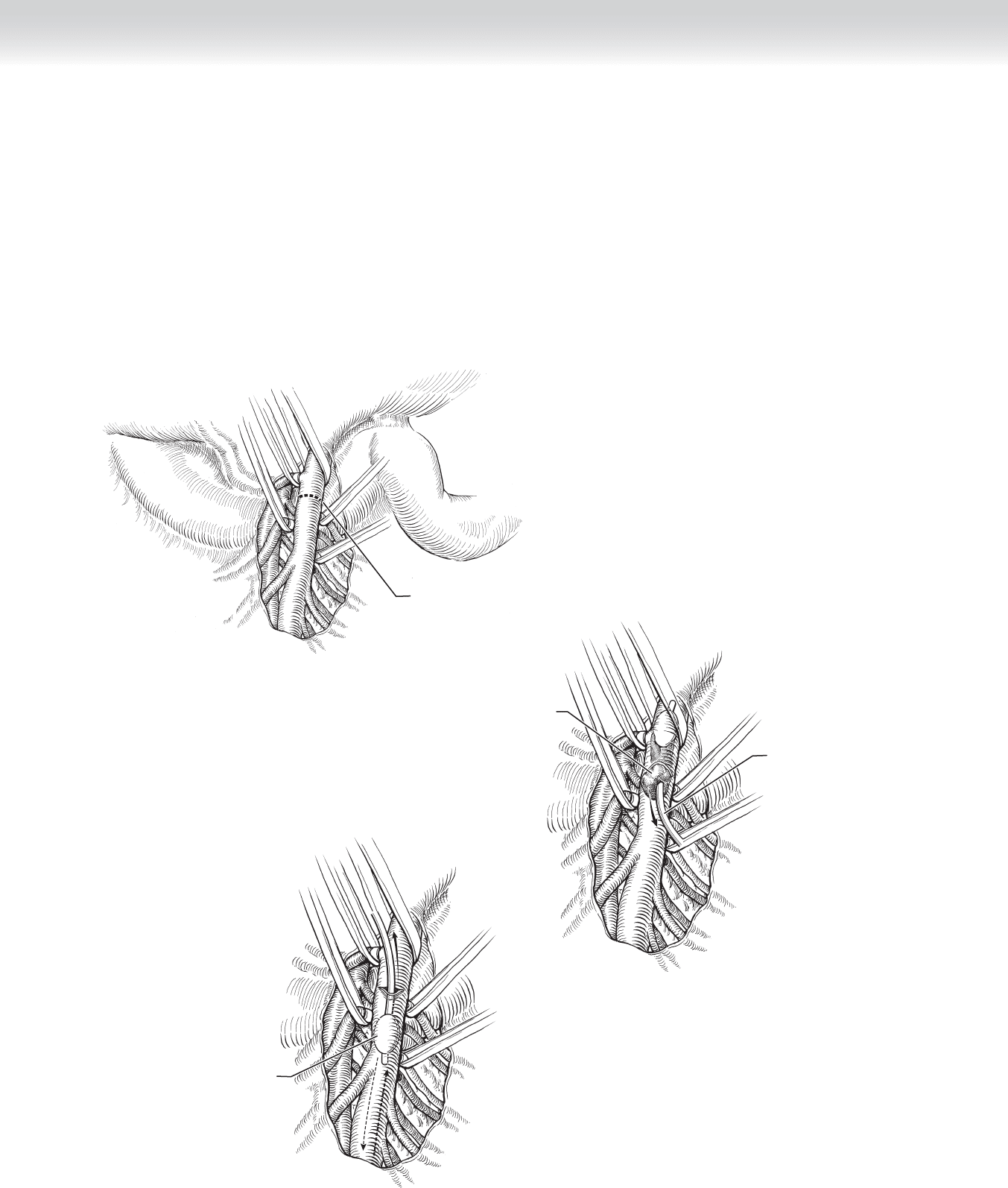
CHAPTER 89 • Mesenteric Ischemia 969
Embolus
Catheter removing
embolus from proximal
superior mesenteric artery
B
A
Transverse arteriotomy
in superior mesenteric
artery
C
Catheter removing embolus from
distal superior mesenteric artery
FIGURE 89 –3
◆ An ACT is drawn and additional heparin is administered to ensure adequate heparinization
(ACT >250). The SMA and its jejunal branches are occluded, and a transverse arteriotomy
is made (Figure 89-3, A).
◆ A balloon catheter is then passed proximally toward the origin of the SMA, the embolus is
extracted, and the proximal SMA is occluded once adequate infl ow has been restored
(Figure 89-3, B). The balloon catheter is also passed distally to ensure no thrombotic mate-
rial remains (Figure 89-3, C). The clamps are temporarily removed, and the vessel is
fl ushed proximally and distally.
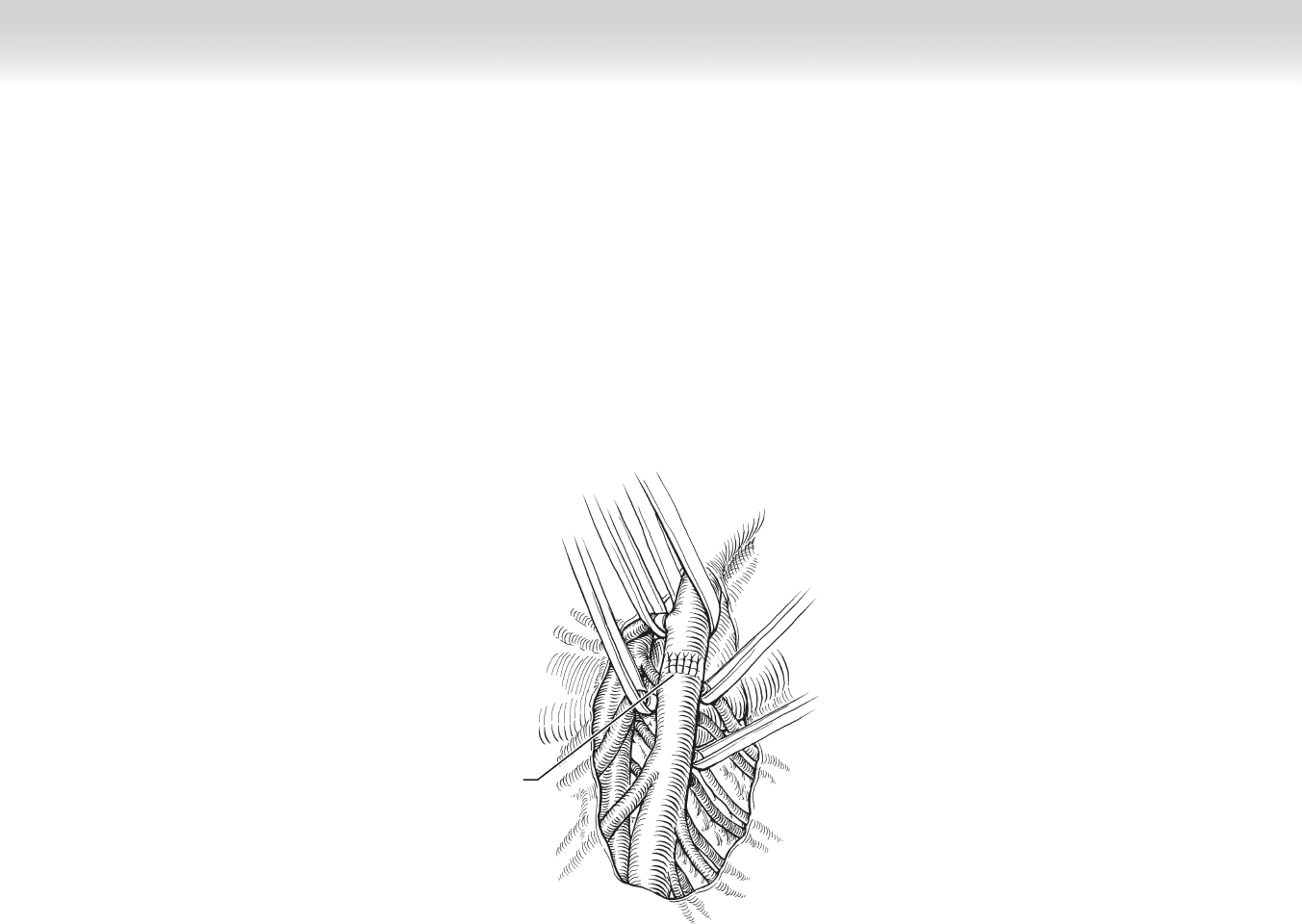
970 Section XII • Vascular
◆ The lumen of the SMA is irrigated with heparinized saline, and the arteriotomy is approxi-
mated with interrupted 6-0 polypropylene suture (Figure 89-3, D).
◆ The bowel is inspected, and mesenteric vessels are interrogated with Doppler ultrasound to
ensure adequate perfusion. Nonviable segments of bowel should be resected.
D
Interrupted
sutures to
close arteriotomy
FIGURE 89 –3, cont’d