Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 88 • Renal Revascularization 951
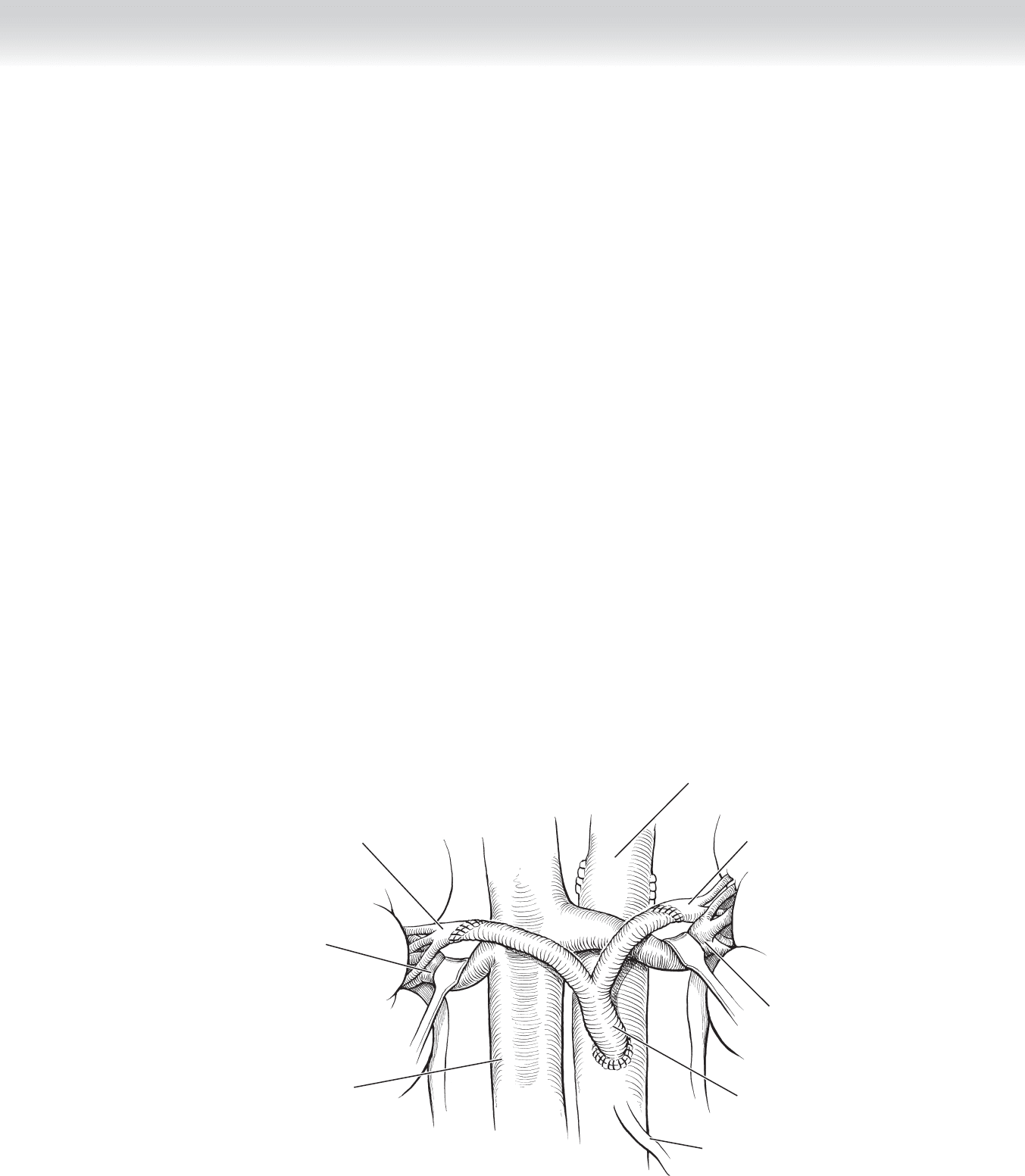
◆ If bilateral renal revascularization is required, a 14 ⫻ 7 or 12 ⫻ 6 Dacron or PTFE bifur-
cated graft is used (Figure 88-3). Saphenous vein or hypogastric artery can be used as
alternative conduits, especially in young adults and children with branch vessel disease. If
the infrarenal aorta is severely diseased, the infl ow of the bypass can originate from the
supraceliac aorta or common iliac arteries.
◆ After the renal anastomosis is completed, heparin is reversed with protamine sulfate
(1 mg/100 U heparin), and 40 mg furosemide is administered.
3. CLOSING
◆ The retroperitoneum is closed with 2-0 Vicryl, and the incision is closed with running
looped monofi lament 1-0 polydioxanone (PDS) or polypropylene suture.
◆ Dressings
◆ Cover the wound with saline-soaked gauze and a nonconstricting bandage.
Right renal artery
Right renal vein
Inferior
vena cava
Bifurcated
prosthetic graft
Left renal vein
Abdominal aorta
Left renal artery
Inferior
mesenteric artery
FIGURE 88 –3

952 Section XII • Vascular
STEP 3: OPERATIVE STEPS—AORTORENAL ENDARTERECTOMY
Endarterectomy is used in selected patients with bilateral focal orifi cial atherosclerotic RAS.
1. INCISION
◆ The aorta is approached through a midline or transverse incision.
2. DISSECTION
◆ The aorta is mobilized from the level of the celiac artery to the inferior mesentery artery.
This requires division of the diaphragmatic crural fi bers, and the dense neural tissue that
surrounds the origins of the celiac and superior mesenteric and renal arteries.
◆ This dissection should isolate a suffi cient segment of aorta to allow safe placement of the
proximal clamp above the renal or superior mesenteric arteries, if these vessels are so close
that a clamp cannot be safely placed between them. The lumbar arteries are occluded with
removable clips and clamps applied in sequence to the renal arteries, the superior mesen-
teric artery, and the infrarenal and suprarenal aorta.
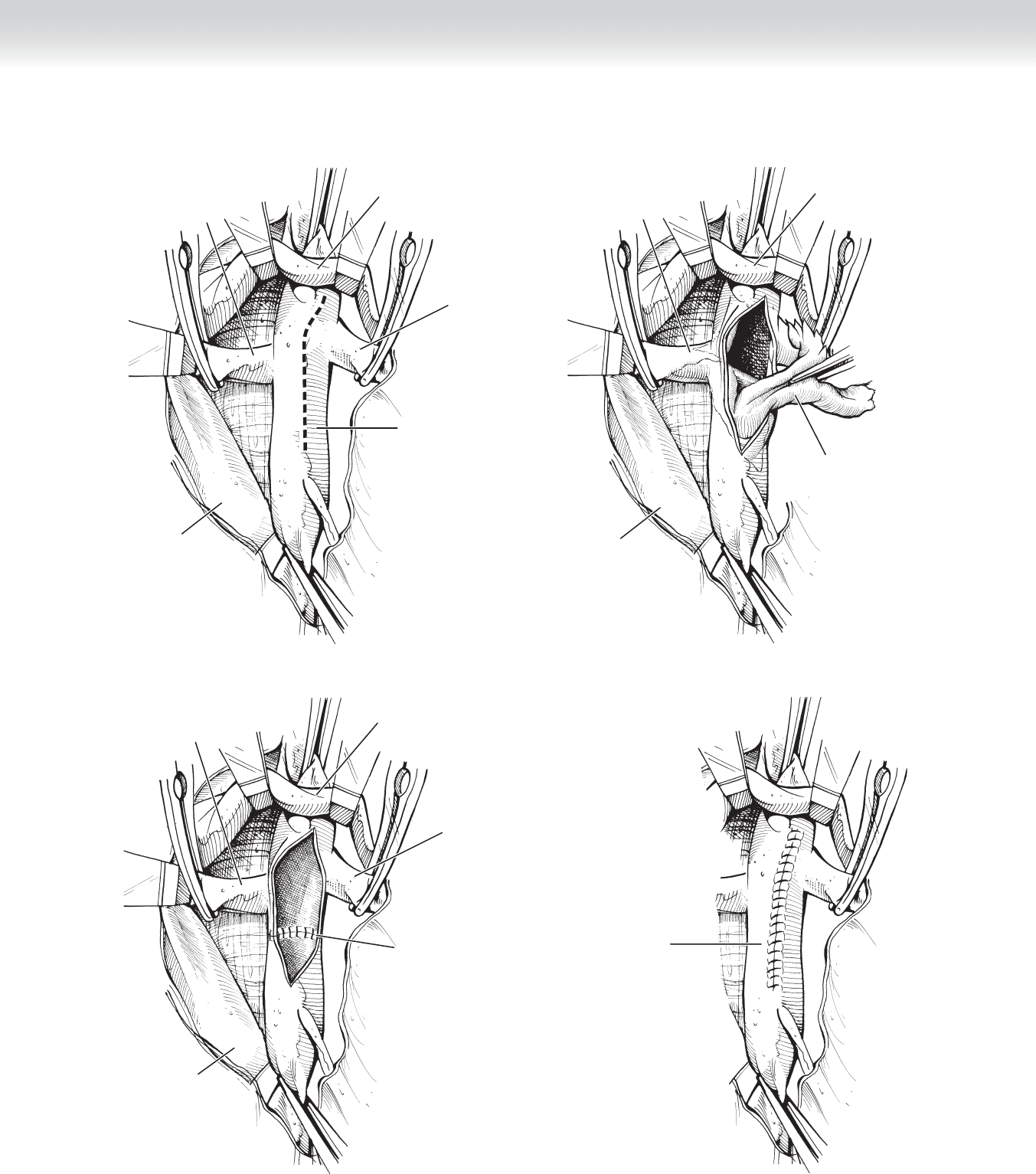
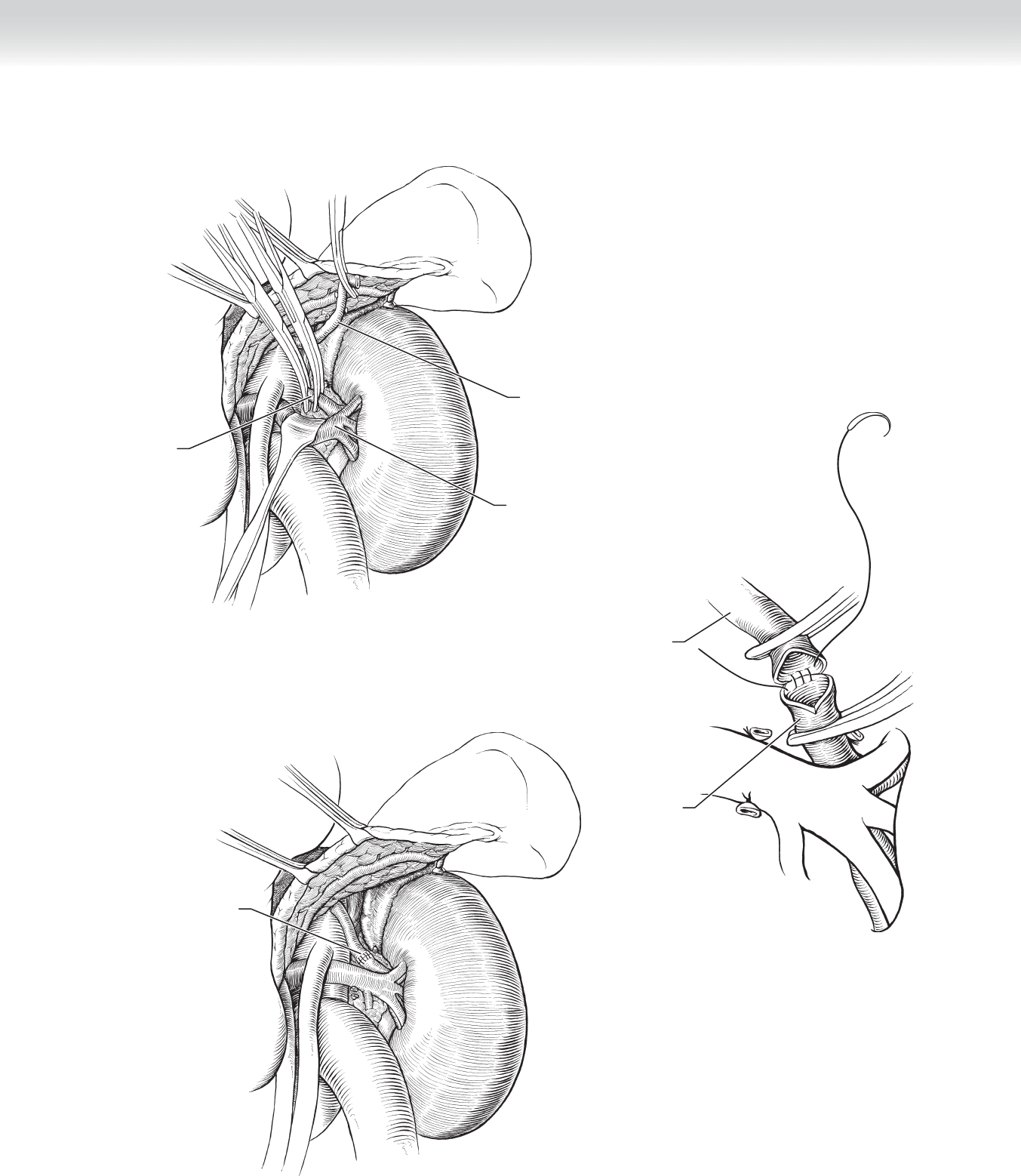
◆ A longitudinal arteriotomy is made extending from the left side of the superior mesentery
orifi ce to below the renal arteries (Figure 88-4, A). The technique involves removal of the
aortic intima in this section of the aorta. Once the aortic intima has been dissected proxi-
mally, each individual renal artery is approached. The aortic intima is grasped and gentle
traction is applied, pulling to the opposite side. The renal ostial lesion is then dissected
from the media by prolapsing the renal artery into the aorta (Figure 88-4, B).
◆ Gentle advancement of the renal artery toward its orifi ce by the assistant facilitates feather-
ing of the end point. The process is repeated on the contralateral side.
◆ The distal intima of the aorta is divided and secured with interrupted 6-0 polypropylene
tacking sutures (Figure 88-4, C). The arteries are fl ushed of atheromatous debris and air,
and the arteriotomy is closed with running 4-0 polypropylene suture (Figure 88-4, D). The
adequacy of the renal endarterectomy is evaluated by intraoperative duplex ultrasound. If
any residual plaque is detected, a transverse arteriotomy is made in the affected renal artery,
the plaque is extracted, and the distal end point is secured with tacking sutures. The arterio-
tomy is closed with interrupted 7-0 polypropylene sutures.
CHAPTER 88 • Renal Revascularization 953
Abdominal
aorta
A
Right
renal artery
Left
renal vein
Left
renal artery
Inferior
vena cava
B
Right
renal artery
Left
renal vein
Aortorenal plaque
Inferior
vena cava
C
Abdominal aorta;
Secured distal
end point
Right
renal artery
Left
renal vein
Left
renal artery
Inferior
vena cava
D
Completed
arteriotomy closure
FIGURE 88 –4

954 Section XII • Vascular
3. CLOSING
◆ The closure of the abdomen is similar for both aortorenal bypass and renal endarterectomy.
The retroperitoneum is closed with 2-0 Vicryl, and the incision is closed with running
looped monofi lament 1-0 PDS or polypropylene suture.
STEP 3: OPERATIVE STEPS—SPLENORENAL BYPASS
◆ Both aortorenal bypass and renal endarterectomy may be contraindicated in elderly patients
with severe aortoiliac occlusive or aneurysmal disease and multiple comorbidities. The pres-
ence of a dense fi brotic reaction from previous operations or renal angioplasty makes dis-
section diffi cult and increases the operative risk. The addition of an aortic bypass to renal
revascularization, which may be indicated in younger patients, is associated with increased
morbidity and mortality in older individuals. In these patients, alternative bypass proce-
dures, such as splenorenal bypass for high-grade left RAS and hepatorenal bypass for dis-
ease on the right, should be considered. The more ischemic kidney is repaired fi rst unless it
is atretic.
◆ Careful angiographic assessment of the hepatic and splenic arteries with anterior posterior
and lateral views is imperative before undertaking these alternative renal revascularization
procedures, because extensive plaque may be present in the donor vessels, which may not
be detected on standard anterior posterior angiographic views.
◆ For both splenorenal and hepatorenal bypass, the patient is positioned supine on the oper-
ating table with a sandbag elevating the affected side and prepped from nipple to knee.
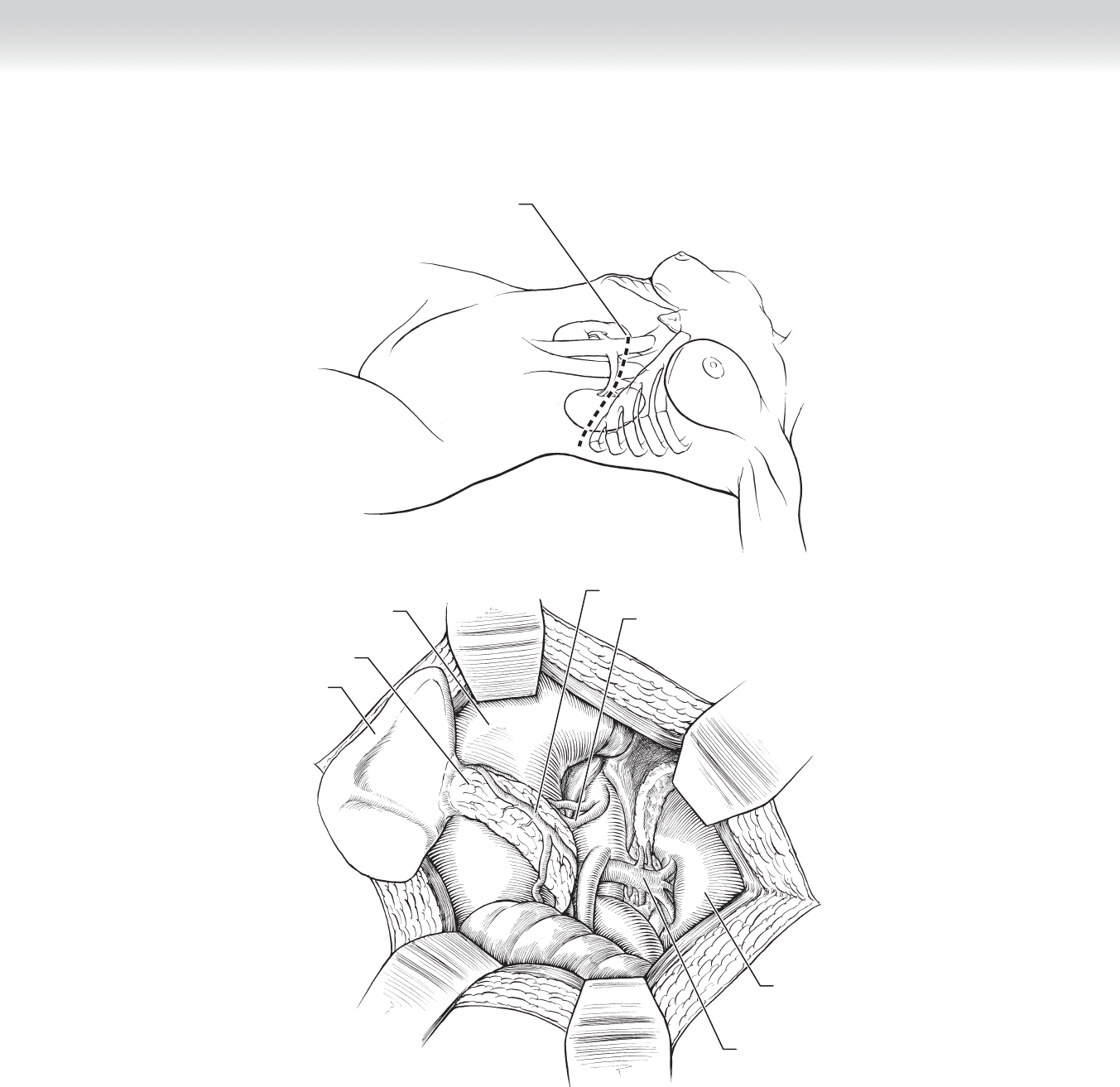
1. INCISION
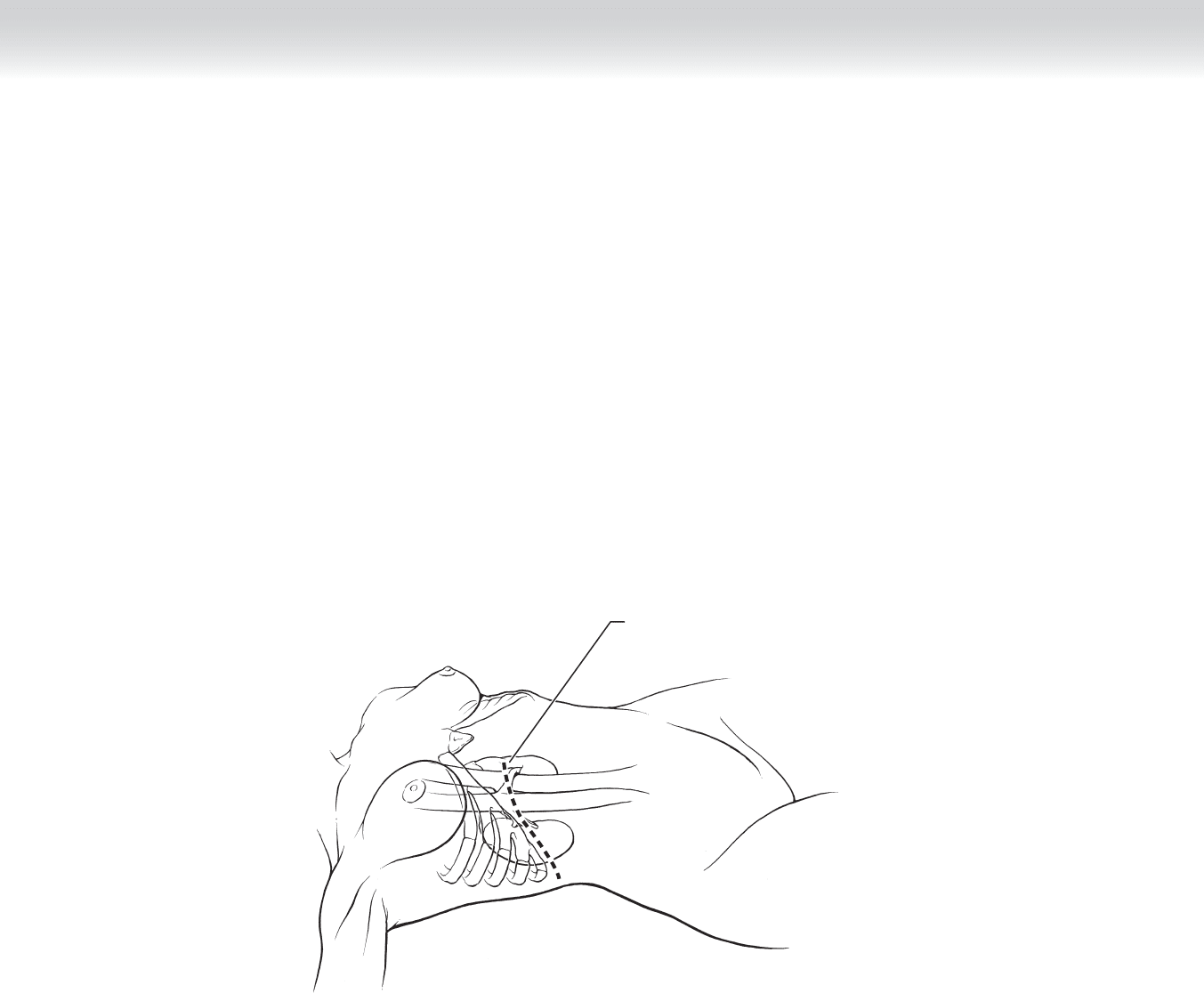
◆ The abdomen is entered via a left subcostal incision that can be extended medially and
laterally if necessary. The splenocolic ligament, spleen, and pancreas are refl ected medially,
and a self-retaining retractor is placed (Figure 88-5, A-B).
CHAPTER 88 • Renal Revascularization 955
MC
Left subcostal
incision
A
Pancreas
Left kidney
Left renal vein
Spleen
B
Splenic vein
Splenic artery
Stomach
FIGURE 88 –5
956 Section XII • Vascular
2. DISSECTION
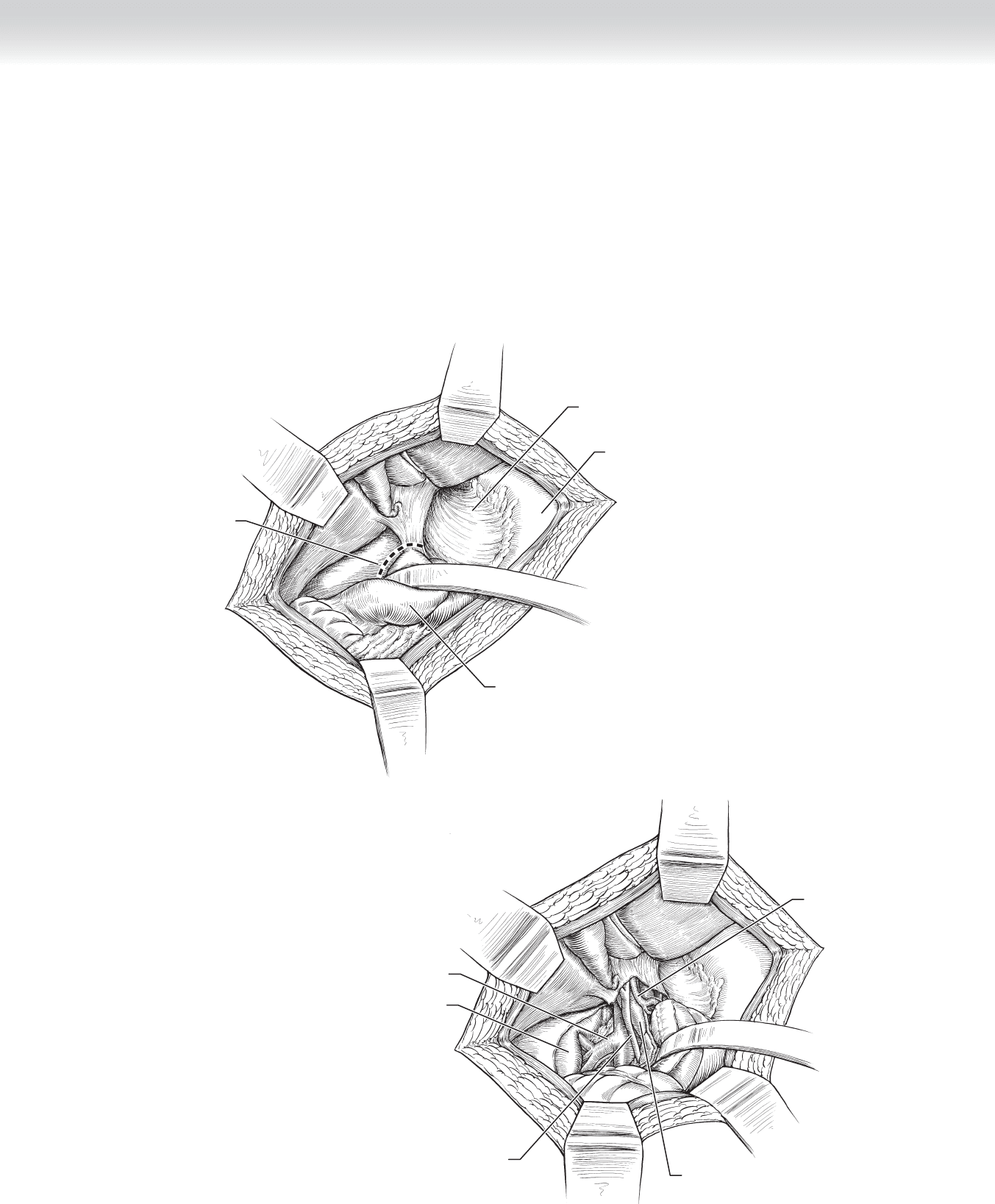
◆ The left renal vein is mobilized by dividing the lumbar and adrenal branches to expose the
renal artery. The pancreas is retracted cephalad to expose the splenic artery and vein. The
splenic arterial and venous branches to the pancreas are divided between 4-0 silk suture lig-
atures. A segment of splenic artery of suffi cient length close to its origin (where its diameter
is largest) is mobilized (Figure 88-5, C-D).
3. CLOSING
◆ After IV heparin is administered, the splenic artery is occluded and divided between
clamps, and the distal end of the vessel is oversewn with 5-0 polypropylene suture. The
renal artery is then mobilized, the proximal end is oversewn with 5-0 polypropylene suture,
the vessels are spatulated, and an end-to-end anastomosis is constructed between the
splenic and renal arteries using running (posterior wall) and interrupted 6-0 polypropylene
suture (Figure 88-5, E-G). The patency of the anastomosis is evaluated with duplex
ultrasound.
C
Dividing inferior suprarenal
vein and artery
Ligation and division
of splenic artery
branches
D
FIGURE 88 –5, cont’d
CHAPTER 88 • Renal Revascularization 957
Retracting
left renal vein
caudally
Divided
splenic artery
Dividing left
renal artery
E
F
Distal left
renal artery
Splenic artery
Completed splenorenal
anastomosis
G
FIGURE 88 –5, cont’d
958 Section XII • Vascular
STEP 3: OPERATIVE STEPS—HEPATORENAL BYPASS
◆ In patients with severe aortic atherosclerosis or aneurysmal degenerative disease and normal
liver function with a high-grade right RAS, hepatorenal bypass should be considered.
1. INCISION
◆ The abdomen is entered via a right subcostal incision (Figure 88-6, A).
MC
Right subcostal
incision
A
FIGURE 88 –6
CHAPTER 88 • Renal Revascularization 959
2. DISSECTION
◆ The hepatic fl exure is mobilized, a Kocher maneuver is performed to mobilize the duode-
num medially, and the Omni-Tract retractor is placed (Figure 88-6, B).
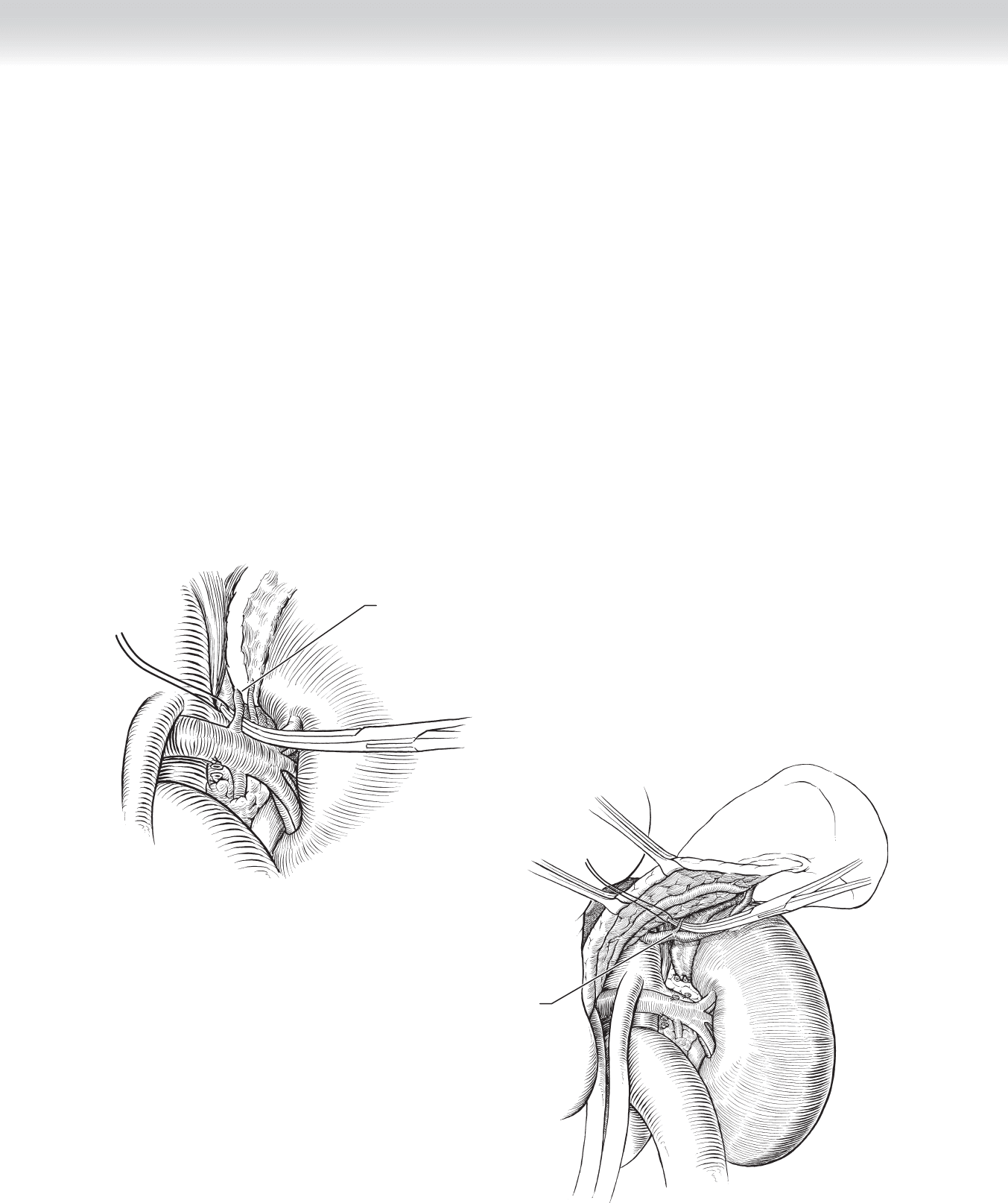
◆ The hepatic artery is exposed between the portal vein and common bile duct
(Figure 88-6, C).
Lesser omentum
Stomach
Incision of peritoneum
and hepatoduodenal
ligament
B
Retracting
duodenum
Hepatic artery
Portal vein
Right renal vein
Right kidney
Common bile duct
C
FIGURE 88 –6, cont’d
960 Section XII • Vascular
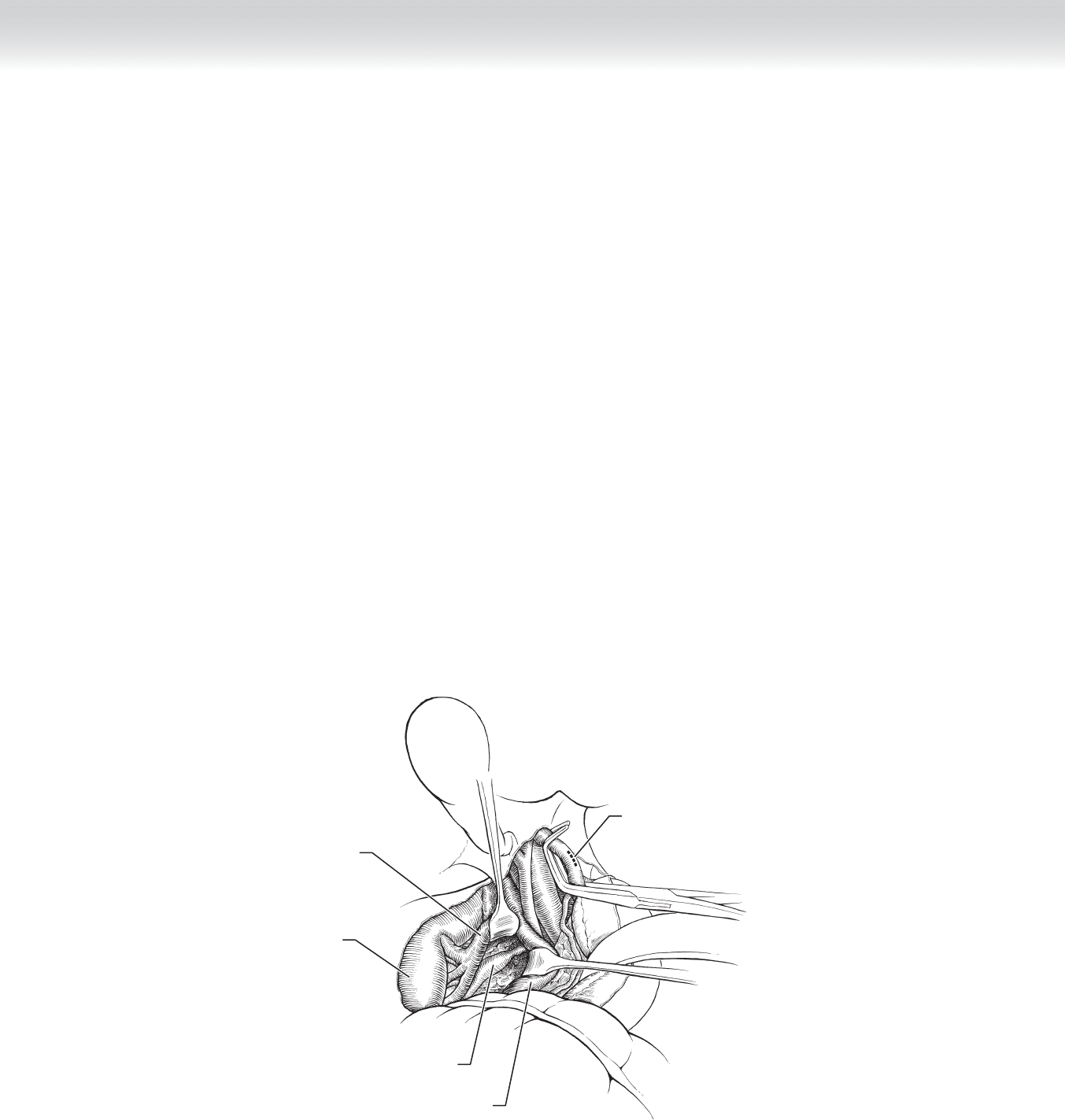
◆ The right renal artery is exposed posterior to the vena cava by retracting the right renal vein
cephalad and the vena cava to the left (Figure 88-6, D).
◆ A 10-cm segment of saphenous vein is harvested and gently distended with a papaverine
solution (see Figure 88-2, B). After systemic heparinization and the administration of man-
nitol, the hepatic artery is occluded between clamps and the saphenous vein graft is anasto-
mosed end-to-side to the hepatic artery distal to the takeoff of the gastroduodenal artery
with running 6-0 polypropylene suture (Figure 88-6, E).
◆ The renal artery is similarly divided close to its origin from the aorta, and the proximal end
is suture ligated with 5-0 polypropylene suture. An end-to-end spatulated anastomosis
between the saphenous vein graft and the distal end of the renal artery is constructed with
interrupted 6-0 polypropylene suture (Figure 88-6, F-G). The patency of the anastomosis
is evaluated with duplex ultrasound.
◆ After the renal anastomosis is completed, heparin is reversed with protamine sulfate
(1 mg/100 U heparin), and 40 mg furosemide is administered intravenously.
D
Inferior vena cava
retracted medially
Hepatic arteriotomy
Right renal vein
retracted cephalad
Right renal artery
Right kidney
FIGURE 88 –6, cont’d