Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

bronchial smooth muscle constriction in the airways
of the lung (bronchospasm) and increased vascular
permeability in the skin, which may be manifested
as swelling or hives and produces itching by affecting
nerve endings. Stimulation of H
2
receptors in the
stomach results in increased acid secretion, which
can produce indigestion or peptic ulcer disease. The
H
3
receptor stimulus–response coupling is presently
unknown. The H
3
receptors were initially described
in presynaptic nerve endings and on nerve bodies of
histaminergic neurons in the brain, where they func-
tion as autoreceptors to regulate the synthesis and
release of histamine. H
3
receptors have also been
located in the airways and gastrointestinal tract.
0004 These histamine receptors and their responses can be
antagonized by specific compounds. For the H
1
recep-
tor, classical antihistamines such as diphenhydramine
and chlorpheniramine act as competitive antagonists
for the receptor. The H
2
receptor is antagonized by the
compounds, cimetidine and ranitidine, whereas the H
3
receptor can be antagonized by thioperamide.
Role in Allergic Reactions
0005 Allergic reactions are among the most commonly
recognized effects of histamine. Specific immuno-
globulin E (IgE) antibodies (the class associated with
allergic reactions), which may be directed at various
allergens, including inhalants such as pollens, molds
and animal dander, foods, drugs, or insect venoms,
are bound to the surface of mast cells and basophils
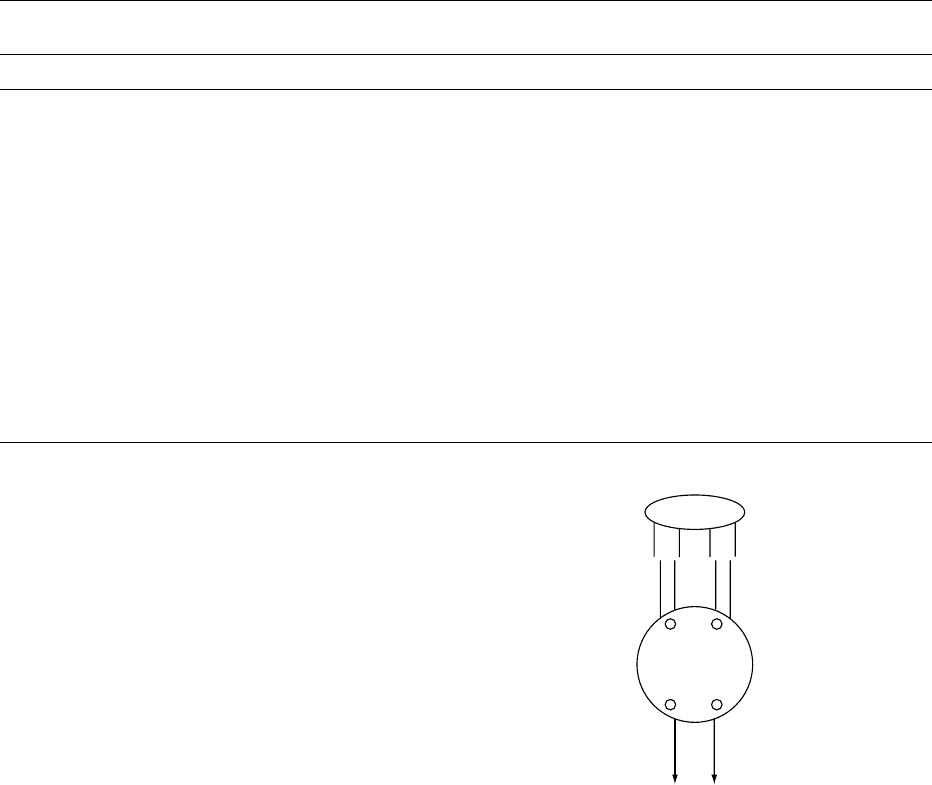
(Figure 2). When the allergen cross-links two IgE
molecules attached to the mast cell or basophil sur-
face, histamine release occurs. Histamine then inter-
acts with tissue histamine receptors (predominantly
H
1
), which can produce local reactions such as
sneezing, nasal and ocular pruritus (itching), rhinor-
rhea (nasal discharge), and nasal congestion. In asth-
matics, histamine release may cause cough, wheezing,
and dyspnea (shortage of breath) owing to bronchial
smooth muscle constriction. More generalized sys-
temic symptoms can occur as a result of the ingestion
of foods and drugs, insect stings, or parenteral ad-
ministration of various medications. These reactions,
whether immunological or nonimmunological in
nature, result in a release of histamine leading to a
prompt and sharp rise in plasma histamine levels.
The severity of the reactions is proportional to the
magnitude of this rise. Mild reactions are associated
with low histamine levels, approximately 1 mmol.
Elevation beyond this level can produce generalized
reactions with urticaria (itchy skin rash), gastrointest-
inal disturbance, cardiac arrhythmias, and hypoten-
sion (low blood pressure). At levels in excess of
tbl0001 Table 1 Characteristics of histamine receptor subtypes
H
1
receptor H
2
receptor H
3
receptor
Effects of stimulation Bronchial smooth
muscle constriction
Increased gastric
acid secretion
Regulate synthesis and release
of histamine from
histaminergic nervesIncreased vascular
permeability
Increased pepsin secretion
Gut smooth muscle
constriction
Decreased IgE-mediated
basophil histamine
releaseVasodilation Inhibits endogenous norepinephrine
release from sympathetic nerves
Pruritus Increased cyclic adenosine
monophosphate levels
Increased cyclic guanosine
monophosphate levels
Decreased lymphocyte-
mediated cytotoxicity
Stimulus–response
coupling
Linked to phosphoinositide
breakdown
Linked to adenylate cyclase ?
Increased calcium mobilization
Antagonists Chlorpheniramine, diphenhydramine,
loratidine, cetirizine, fexofenadine
Cimetidine, ranitidine,
famotidine, nizatadine
Thioperamide, clobenpropit
Allergen
Mast
cell
or
Basophil
Histamine
Non immunological
Immunological
IgE-allergen interaction
Complement fragments
(C
3a
, C
5a
)
Cytokines
(histamine-releasing
factors)
Calcium-ionophore
Basic compounds
(48/80)
Opiates
Enzymes (trypsin)
Drugs (radiographic
contrast agents)
Detergents
Physical stimuli (cold)
Chemical
(hyperosmolality)
Hypoxia
fig0002Figure 2 Human mast cell or basophil stimulated to release
preformed histamine by a variety of immunological and non-
immunological mechanisms.
HISTAMINE 3109

12 mmol, life-threatening responses such as severe
hypotension, bronchoconstriction, and ventricular
fibrillation can occur. (See Food Intolerance: Types;
Food Allergies.)
Cardiovascular Effects
0006 Histamine causes vasodilation and increased vascular
permeability. This can result in flushing and decreased
peripheral vascular resistance with subsequent lower-
ing of the blood pressure. Extravasation of fluid results
in angioneurotic edema (swelling of the skin on the
eyes, lips and extremities). These effects are primarily
mediated through H
1
receptor stimulation. Stimulation
of the H
1
and H
2
cardiac receptors can lead to a variety
of rhythm disturbances.
Bronchial Smooth Muscle Effects
0007 Stimulation of the H
1
receptors in bronchial smooth
muscles causes constriction, producing narrowing of
the airways. This results in breathing difficulties and
wheezing. Stimulation of H
2
receptors may lead to
relaxation of airway smooth muscle, although this
effect is minimal.
Effect on Gastric Secretion
0008 Gastric mucosal mast cells release histamine, which
causes an increase in gastric acid secretion by gastric
parietal cells through H
2
receptors. Histamine interacts
with acetylcholaine and gastrin to control acid output
in the stomach. H
2
receptor antagonists (cimetidine,
ranitidine) are widely used to treat peptic ulcer disease
because of their ability to decrease acid secretion.
Central Nervous System Effects
0009 Two major sources of histamine in the brain are mast
cells and histaminergic neurons. Mast cells are lo-
cated near blood vessels and may affect local blood
flow. Histaminergic neurons (nerve cells whose prin-
cipal neurotransmitter is histamine) are limited in
number, but their axons branch into long ascending
fiber networks that ultimately innervate much of the
brain. Their role is not clear, but the central effects
of histamine include antidiuresis (fluid retention)
through the release of vasopressin, induction of
adrenocorticotrophic-releasing hormone and prolac-
tin secretion, increase in blood pressure and heart
rate, temperature regulation, and control of arousal
mechanisms. The sedative affects of the first gener-
ation antihistamines (e.g., chlorpheniramine, diphen-
hydramine), which block H
1
receptors functions are
well known. In contrast, second-generation H
1
blockers (loratidine, fexofenadine, cetirizine) that do
not readily cross the blood–brain are less likely to
induce sedation.
Effect on the Immune System
0010Histamine may have a more general effect on the
immune system than its role in allergic reactions.
Stimulation of H
2
receptors suppresses lymphocyte
proliferation, T-cell-mediated cytotoxicity, lympho-
kine production, natural killer cell cytotoxicity,
and antibody production by B-lymphocytes. Histamine
in certain dose ranges is chemotactic for eosinophils,
which are the principal effector cells in killing of para-
sites such as schistosomes. Parasites that invade body
tissues generate profound IgE antibody responses.
Interaction of parasite antigens with specific IgE
antibodies on the surface of mast cells causes histamine
release and the subsequent attraction of eosinophils to
the area. Eosinophils can degranulate, releasing their
granular proteins, which are potent toxins to parasitic
organisms. (See Immunology of Food.)
Role of Cellular Proliferation
0011Another physiological role for histamine appears to
be in wound healing, since proliferating tissues syn-
thesize histamine at a higher rate than normal tissue.
The contribution to wound healing is still not com-
pletely understood, however.
Histamine Poisoning
0012Histamine is present in measurable quantities in certain
foods, including cheese, meat, wine, yeast products,
and some vegetables such as spinach and tomatoes
(Table 2). The ingestion of large quantities of histamine
can result in clinical symptoms indistinguishable from
those of an allergic reaction. These include flushing,
throbbing or severe headaches, palpitations of the
heart, abdominal cramps, and diarrhea. Dizziness,
burning of the mouth or throat, nausea, hives, and
angioneurotic edema can occur. Cough, wheezing,
and severe respiratory distress may appear in patients
who have an underlying allergic background, particu-
larly in those with asthma. Symptoms generally begin
30–60 min after ingestion of foods containing high
concentrations of histamine. (See Migraine and Diet.)
Measurement of Histamine in Food
0015A number of analytical methods for measuring the
histamine content of foods have been developed
including fluorometric methods, thin-layer chroma-
tography, oxygen-sensor-based methods, and biologic
methods. In addition, a number of commercially
available enzyme-linked immunoassay test kits are
marketed in the United States and Europe.
3110 HISTAMINE
Scombroid Fish Poisoning
0013 Scombroid fish poisoning results from eating spoiled
fish of the Scombridae and Scomberessocidae fam-
ilies, and produces headache, itching, diarrhea, flush-
ing, and palpatations immediately afer ingestion.
These fishes include tuna, mackerel, skipjack, and
bonito. However, nonscombroid fishes, such as
mahi-mahi, blue fish, amberjack, marlin, herrings,
sardines, and anchovies, have also been implicated in
scombroid-toxin-like illness. Scombroid fish poison-
ing is the most common cause of ichthyotoxicosis
worldwide. In addition to ingestion of fish, histamine
poisoning can occur occasionally through ingestion
of cheese such as Swiss, Cheddar and Gouda. (See
Fish: Spoilage of Seafood.)
001 4 There has been some debate as to whether histamine
is the sole cause of scombroid poisoning, but histamine
is the most likely causative agent of scombroid fish
poisoning. As clinical proof of the role of histamine, a
definitive study involved three patients who were ex-
posedtomarlin,andlaterdevelopedtheclassicalsymp-
toms of scombroid fish poisoning. Urinary excretion of
histamine and its metabolite, N-methylhistamine, was
measured.Urinesamplescollected1–4h afteringestion
of fish show that the histamine and the N-methylhista-
mine levels were respectively nine to 20 times and
15–20 times more than the normal mean, a likely indi-
cation of exposure to high histamine levels. During the
subsequent 24h, the levels fell to four to 15 times and
four to 11 times the normal values, respectively, and
had returned to normal by 14 days. There was no
evidence of mast cell activation as measured by the
principal urinary metabolite of prostaglandin D
2
.In
addition,ingestionofahighconcentrationofhistamine
has been demonstrated to produce symptoms of scom-
broid poisoning. These symptoms are generally self-
limiting, lasting a few hours, and can be quickly treated
with systemic antihistamine administration. Elevated
histamine levels in fish tissue have been associated with
poor refrigeration, which results in bacterial spoilage
and histamine formation. Bacteria possessing histidine
decarboxylase can contaminate the gastrointestinal
tract, skin, and gills of fish. In the case of cheese, the
entry point to contamination by the histamine-produ-
cingbacteriais raw milk.Refrigerationofraw milk and
fish, good hygiene during food preparation,and careful
control of fermentations will therefore avoid the prob-
lem. Cooking, however, will not destroy histamine.
Seealso: Fish:SpoilageofSeafood; Food Intolerance:
Types;FoodAllergies; Immunology of Food; Migraine
and Diet
Further Reading
Chrush C, Sharma S, Unruh H et al. (1999) Histamine H
3
receptor blockade improves cardiac function in canine
anaphylaxis. American Journal of Respiratory and
Critical Care Medicine 160: 1142–1149.
Douglas WW (1985) Histamine and S-hydroxytryptamine
(serotonin) and their antagonists. In: Goodman LS and
Gillman AG (eds) The Pharmacological Basis of Thera-
peutics, 7th edn, pp. 605–615. New York: Macmillan.
Helrich K (ed.) (1990) Histamine in seafood: fluorometric
method. In: Official Methods of Analysis of the Associ-
ation of Analytical Chemists,15thedn.Arlington,VA:
Association of Official Analytical Chemists, pp. 876–877.
Lehane L and Olley J (2000) Histamine fish poisoning
revisited. International Journal of Food Microbiology.
58: 1–37.
Marquardt D (1983) Histamine. Clinical Reviews in
Allergy 1: 343–351.
Marrow JD, Marolies GR, Rowland J and Roberts LJ II
(1991) Evidence that histamine is the cause of scom-
broid-fish poisoning. New England Journal of Medicine
324: 716–720.
Pierce FL (1991) Biological effects of histamine: an over-
view. Agents and Actions 33: 4–7.
Price RJ (1999) Compendium of fish and fishery products:
processes, hazards and controls. University of Califor-
nia–Davis. National Seafood HACCP Alliance for
Training and Education. Available at http://www-
seafood.ucdavis.edu
Rafferty P and Holgate ST (1989) Histamine and its antag-
onists in asthma. Journal of Allergy and Clinical Immun-
ology 84: 144–151.
Simon FER (1996) Histamine and H
1
-receptor Antagonists
in Allergic Disease. New York: Marcel Dekker.
tbl0002 Table 2 Foods with high histamine content
Food Histamine content (mgg
1
)
Fish
Tuna, mackerel, bonito,
mahi-mahi, bluefish
ND–9000
Sardine, herring, anchovy ND–2000
Cheeses
Swiss ND–2500
Roquerfort and blue Trace–4090
Cheddar ND–1080
Gouda Trace–200
Mozzarella ND–50
Wines
American red 0.2–15.5
American white 0.2–11.4
European red ND–30
European white ND–20
Dry sausages Trace–650
Sauerkraut <5.0–200
Soya sauce ND–2740
ND, not detectable.
Modified from Stratton JH, Hutkins RW and Taylor SL (1991) Biogenic
amines in cheese and other fermented foods: a review. Journal of Food
Protection 54: 460–470, with permission, and Diel E, Bayas N, Stibbe A et al.
(1997) Histamine containing food: Establishment of a German Food
Intolerance Databank (NFID). Inflamm Res 46(1): S87–S88.
HISTAMINE 3111

HIV DISEASE AND NUTRITION
C Baldwin, Chelsea and Westminster Hospital,
London, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 The acquired immunodeficiency syndrome (AIDS) is
a disorder characterized by progressive and profound
immunodeficiency that renders the infected individ-
ual highly susceptible to life-threatening opportunis-
tic infections and tumors. It is caused by infection
with the human immunodeficiency virus (HIV). The
first cases of AIDS were reported in June 1981. At the
end of December 1999 the World Health Organiza-
tion reported that there were 47 million cases of HIV
infection worldwide, of which more than 40 000 were
in the UK. AIDS is the now the fourth leading cause
of mortality.
0002 In the early days of HIV infection survival was
limited by the occurrence of lethal opportunistic in-
fections such as Pneumocystis carinii pneumonia and
Mycobacterium avium complex and the lack of anti-
retroviral therapies. As understanding of the natural
history of the disease improved and effective prophy-
laxis against the common opportunistic infections
became available, the associated morbidity and mor-
tality improved. Initial treatment approaches were
limited to the use of nucleoside analog monotherapy,
such as with zidovudine (AZT), which provided only
transient clinical and immunological benefits. Over
1995 and 1996, availability of a new diagnostic test,
viral load measurement, and new drug classes such as
protease inhibitors and nonnucleoside reverse tran-
scriptase inhibitors heralded a new approach to HIV
management. The era of highly active antiretroviral
therapy (HAART), in which suppression of plasma
viral replication to below viral load assay limits (cur-
rently < 50 HIV RNA copies ml
1
) is achieved in a
substantial proportion of individuals, has changed
the clinical management, prognosis, and survival of
people with HIV. The immunologic benefits gained
through virus control with ‘cocktails’ consisting of
three or more drugs have led to dramatic reductions
in the incidence of the major opportunistic infections
and mortality. As the clinical management of HIV
infection has altered, so has its nutritional manage-
ment, although the indications for nutritional support
remain less clearly defined. However, concern that
many therapy combinations or individual compon-
ents of therapy may lead to metabolic perturbations
in individuals with HIV has led to a new era of
nutritional evaluation and investigation in persons
with HIV. This article reviews what is known about
the nutritional status of people with HIV infection,
the nutritional problems specific to this infection
and its treatments, and the objectives of nutritional
support.
Nutritional Status of People with HIV
Infection
0003Before the introduction of HAART, profound weight
loss and wasting were amongst the most common
observations in people with HIV infection. In 1987
the Centers for Disease Control (CDC) included
HIV wasting (> 10% loss of baseline body weight þ
pathogen-negative diarrhea or persistent night
sweats), which could not be explained by the presence
of concurrent infection, in the list of AIDS-defining
illnesses. Two-thirds of men with AIDS were reported
to weigh less than 90% of their usual body weight.
Since 1995 effective combination therapy has been
associated with significant weight gain in the majority
of people. Indeed, some patients report gaining exces-
sive amounts of weight on therapy. This may be due
to a modest reduction in resting energy expenditure
(REE) and improvement in gut function and nutrient
absorption, and additionally, the resolution or pre-
vention of minor infections which may contribute to
bouts of weight loss. Weight loss and wasting are less
common in people receiving HAART but still occur
in some people who have an excellent antiviral/
immunological response, in some cases as a result of
side-effects of therapy. Additionally, not all patients
respond or respond durably to HAART.
0004Weight loss in HIV infection is often multifactorial
in its causation, even within individual patients. The
management of weight loss is dependent on an under-
standing of the underlying pathophysiology.
0005Two major mechanisms dominate the pattern of
tissue loss in HIV-related weight loss:
1.
0006Protein-energy malnutrition (PEM) is a condition
synonymous with starvation, resulting when the
body’s needs for protein, energy, or both cannot be
met by diet. In HIV infection this could result from
inadequate intake or nutrient malabsorption.
2.
0007Cachexia is a clinical syndrome characterized by
a mixture of metabolic abnormalities that lead
to weight loss through accelerated wasting of
host tissue mass, and failure of adequate nutrient
intake, absorption, and utilization. This is
3112 HIV DISEASE AND NUTRITION
different from malnutrition in that there is a
marked and rapid depletion of muscle rather
than fat.
The major difference between PEM and cachexia is
that the nutritional effects ofstarvation can be reversed
by the provision of appropriate feeding whilst the
nutritional changes associated with cachexia cannot.
0008 Malnutrition is associated with important clinical
consequences independent of the underlying disease.
Chronic undernutrition leads to deficiencies in work
capacity, immune function, wound healing, organ
function, mental state, and growth in children. When
secondary malnutrition occurs as a result of disease it
is associated with additional problems: reduced qual-
ity of life, disease complications, poor clinical out-
comes, and increased costs of management. In a study
of men with AIDS wasting (mean weight loss 15%),
the extent of muscle wasting was highly predictive
of the strength and functional capacity of the leg
muscles, demonstrating the important relationship
between loss of lean body mass and functional
capacity. Additionally, in people with HIV infection,
weight loss has profound prognostic implications,
predicting shortened survival, increased risk of hospi-
talization, and increased risk of being diagnosed with
an opportunistic infection. The effects of weight loss
are independent of immune function (as measured by
CD4 lymphocyte counts). Recently published obser-
vations have quantified the impact of weight loss in
HIV infection, demonstrating that a weight loss trend
over a 4-month period of even as little as 0–3% was
predictive of increased subsequent mortality. Weight
loss of more than 5% was associated with a relative
risk of 1.88 (P < 0.001) of developing an opportunis-
tic infection in the follow-up period.
Characteristics of Malnutrition
0009 Early studies of weight loss and body composition
conducted in a group of men with AIDS-related
weight loss, compared with an HIV-negative control
group, demonstrated that weight loss in this group
was associated with a profound depletion of body cell
mass that was greater than that expected for the body
weight reduction, whereas fat mass was largely pre-
served. These studies were performed before the first
antiretroviral drugs became available and therefore
represent untreated HIV infection.
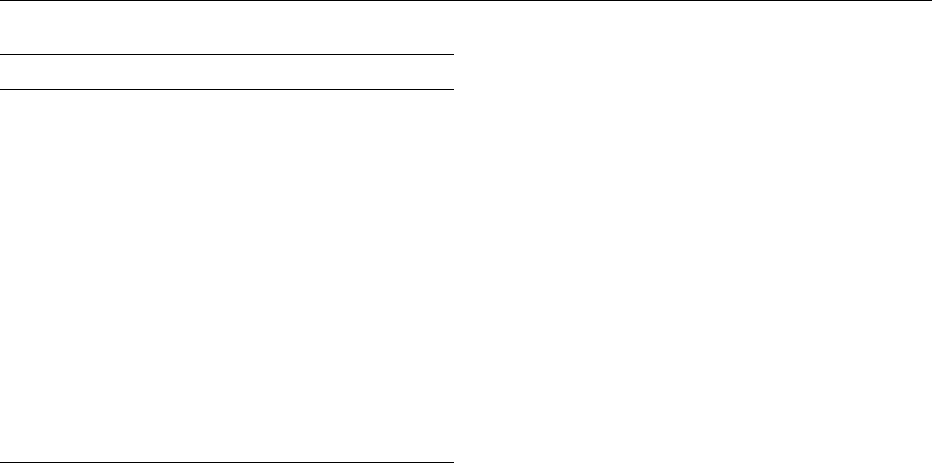
0010 A 1993 study examined patterns of weight change
in 30 individuals with HIV over a period of 9–49
months. Two typical patterns of weight change were
described – acute and chronic weight loss. Acute
weight loss (Figure 1) was usually rapid, occurring
at a rate of 4 kg per month or greater, and was
associated with opportunistic infections, mainly
nongastrointestinal. Recovery to usual or preillness
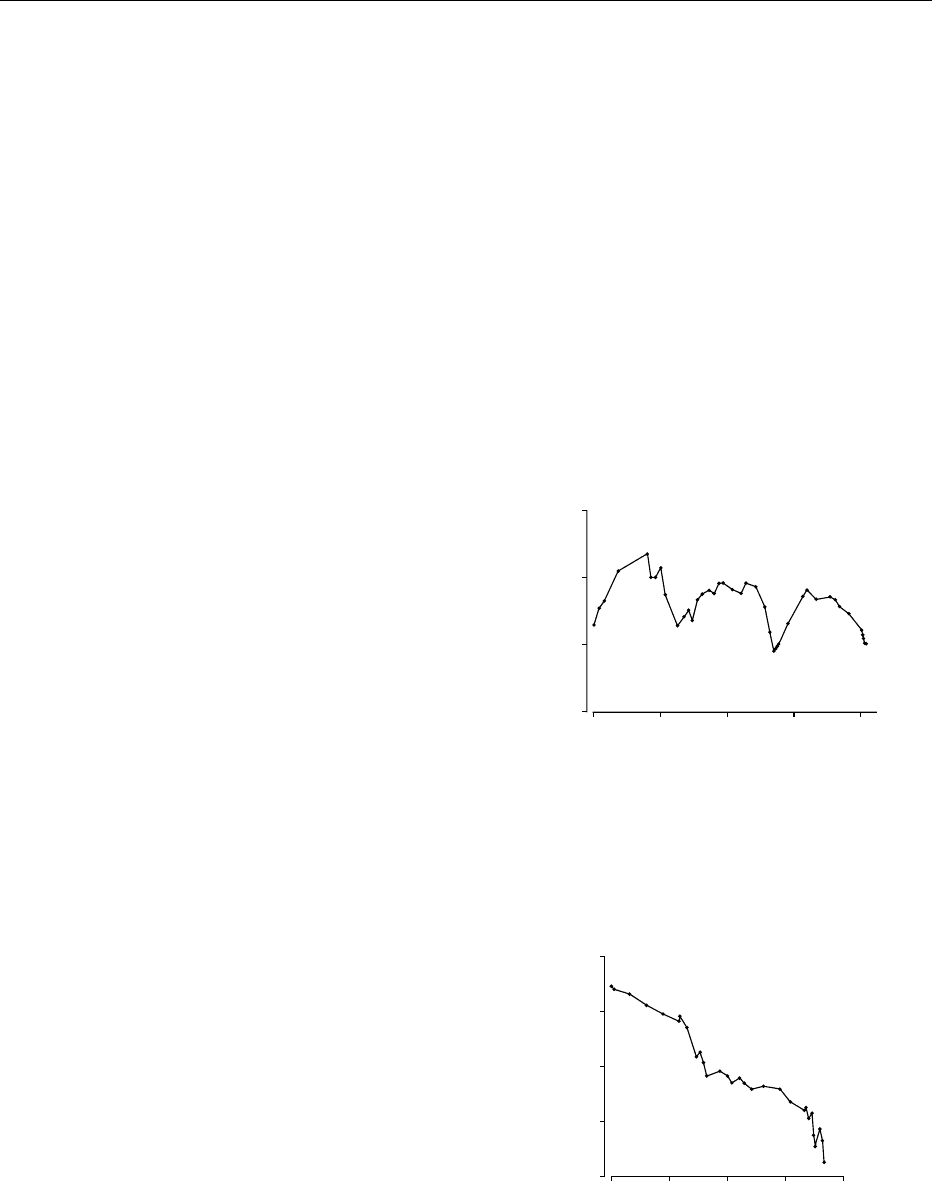
weight was common. Chronic weight loss (Figure 2),
in contrast, occurred at a slower rate of less than 4 kg
per month, was progressive, and was associated
mainly with gastrointestinal disease. These observa-
tions have a number of important implications for the
nutritional management of people with HIV. First,
they demonstrated that HIV infection was not associ-
ated with unremitting weight loss. Treatment of the
underlying infection leads to the ability to regain
weight, often back to preillness weight, and therefore
HIV does not prevent an appropriate anabolic re-
sponse. Second, weight loss may precede specific
signs and symptoms of infection and, therefore, is of
significant diagnostic value. This potential diagnostic
role prompted the recommendation that weight
0
50
60
70
80
200 400 600 800
Weight (kg)
Da
y
s
fig0001Figure 1 Example of acute weight loss episodes (time 0 ¼stage
IV diagnosis). Reproduced with permission from; Macallan DC,
Noble C, Baldwin C et al. (1993) Prospective analysis of patterns
of weight change in stage IV human immunodeficiency virus
infection. AmericanJournalofClinicalNutrition 58: 417–424.
0 200 400 600 800
40
50
60
70
80
Weight (kg)
Days
fig0002Figure 2 Example of chronic weight loss (time 0 ¼ stage IV
diagnosis). Reproduced with permission from; Macallan DC,
Noble C, Baldwin C et al. (1993) Prospective analysis of patterns
of weight change in stage IV human immunodeficiency virus
infection. AmericanJournalofClinicalNutrition 58: 417–424.
HIV DISEASE AND NUTRITION 3113

change be recorded in all patients and be represented
graphically in patient notes. Third, weight gain
achieved following recovery from weight loss epi-
sodes usually occurs without the use of invasive nu-
tritional support and, therefore, could be seen to
represent the natural history of weight change in
HIV infection.
Body Composition and Effective Antiviral Therapy
0011 Advances in the management of HIV infection have
had a significant impact on the incidence of weight
loss and wasting but nutritional status has not
returned to normal. In 1998 the first reports appeared
of altered body composition in people with HIV in-
fection. A syndrome of fat redistribution and associ-
ated metabolic abnormalities has been described
which has become known as lipodystrophy. The syn-
drome(s) consists of accumulations of fat (lipohyper-
trophy) in the abdominal area (intraabdominal in
men, breast enlargement in women), posterior neck
(‘buffalo hump’), and fat loss (lipoatrophy) in the face
(particularly the temporalis, nasolabial, and buccal
fat pad), arms and legs (leading to vein prominence).
Metabolic changes, including hypercholesterolemia,
hypertriglyceridemia, hyperglycemia, and insulin
resistance, are also reported in association with the
syndrome. There is so far no accepted definition for
the syndrome of fat redistribution or any accepted
set of standardized diagnostic criteria. However, the
clinical presentation is characteristic and highly stig-
matizing. Reports of the prevalence of the fat redistri-
bution syndrome vary widely, depending in part on
definition, from as low as 2% up to 84%. Initially the
syndrome was thought to be associated solely with
protease inhibitors, but more recently it has been
reported in people receiving all classes of antiretro-
viral therapy. Several authors have proposed mechan-
isms to explain the development of the syndrome but
the causes remain unknown. Identified risk factors
include duration of antiretroviral therapy, older age,
and white race. The use of protease inhibitors may
accelerate time to syndrome onset.
0012 An accurate assessment of body composition in
people with fat redistribution is difficult. Bioelectric
impedance analysis will not accurately measure body
composition in this syndrome as it is unable to detect
regional distribution or assess any changes that may
occur. Dual X-ray absorptiometry (DEXA) scanning
can determine regional fat compartments and may be
useful in assessing people with fat redistribution, al-
though the absence of data on normal body compos-
ition as well as regional body composition may limit
its usefulness in diagnosing the syndrome. Computer-
assisted tomography and magnetic resonance imaging
can quantify body fat and therefore may be of most
use in assessing body composition in this syndrome,
although they are not always practical.
Deficiencies of Individual Nutrients
0013A number of studies have attempted to measure vita-
min and mineral levels in HIV-positive subjects com-
pared with a control group. Overall, results suggest
that specific nutrient deficiencies are common in HIV
infection and especially in the advanced stages of
disease. The actual extent of overt and marginal defi-
ciency and their significance is unclear. More infor-
mation is needed on factors that might influence
nutrient status measures, such as nutrient intake,
drug–nutrient interactions, the influence of disease,
and the presence or absence of infection; improve-
ments in methods of nutrient assessment are also
needed.
0014There is extensive literature on the relationship of
nutrient deficiencies to immune function. Nutritional
deficiencies can impair immunity and so influence a
person’s susceptibility to infections. It has been sug-
gested that dietary manipulations might diminish or
reverse the immune defects caused by HIV infection
and enhance resistance to opportunistic infections. At
present there is insufficient evidence to support the
use of particular nutrient supplements to modulate
immune function. The use of vitamin and mineral
supplements containing 100% of the recommended
daily allowance for all micronutrients has been pro-
posed in the USA by the Task Force on Nutrition
Support in AIDS to insure sufficiency. Although
some authors have suggested supplementary levels
of some vitamins and minerals in people with HIV
in an attempt to achieve normal plasma levels, the
benefits of this approach in the short and long term
are unclear.
0015There is no evidence that megadoses of any vitamin
or mineral will alter the course of disease or improve
the nutritional status of people with HIV.
The Mechanisms of Malnutrition in HIV
Infection
0016There are a number of factors that may lead to the
development of malnutrition in HIV infection: altered
food intake, malabsorption of nutrients, and changes
in metabolism.
Reduced Food Intake
0017Food intake in an HIV-positive person may be
affected by many physical and emotional factors.
Anorexia is an accepted response to infection. Loss
of appetite is a problem in people with HIV infection
and may result from the associated opportunistic
3114 HIV DISEASE AND NUTRITION

infections, malignancies, gastrointestinal symptoms,
side-effects of medication, emotional issues, or a com-
bination of these.
Nutrient Malabsorption
0018 Malabsorption is common in HIV infection and may
result from intestinal pathogens and the side-effects
of medication.
Metabolic Alterations
0019 Hypermetabolism in association with febrile illness
is a familiar concept. A number of investigators
have measured REE in asymptomatic HIV infection
and demonstrated an increase of around 10%. The
presence of opportunistic infections is associated
with greater increases in REE of up to 34%. There
is still much to be learned about the mechanisms of
metabolic regulation that accompany weight loss
and wasting in HIV. It is not understood why an
increase in metabolic rate is not accompanied by an
increase in food intake. Cytokines such as tumor
necrosis factor (TNF) and interferons are respon-
sible for many aspects but there is now evidence
that they are not alone responsible for the wasting
process.
0020 If a person is to be in energy balance, then energy
intake must be equal to REE plus energy used in
activity (total energy expenditure (TEE)). A study
published in 1995 examined the relative contribu-
tions of changes in energy expenditure and intake to
the pathogenesis of HIV-related weight loss and has
provided important information on the underlying
causes of weight loss in HIV infection. It examined
energy balance in a group of 21 HIV-infected individ-
uals. TEE, REE, activity levels, and food intake were
measured during episodes of weight loss, weight gain,
and during periods of weight stability. It confirmed
that REE is raised in individuals with HIV infection
and that during periods of opportunistic infection
REE is elevated even further. During periods of
weight loss TEE was not elevated but reduced to be
almost equal to REE, accounted for by a reduction
in activity levels, and was raised during periods of
weight gain, therefore TEE could not account for the
changes in energy balance necessary to cause weight
changes. Measurement of energy intake confirmed
that reduced energy intake is the prime determinant
of weight change in HIV-associated weight loss. It has
been suggested that it is possible to predict the com-
position of tissue loss during periods of starvation
and that there is an inverse relationship between the
amount of body fat and the ratio of fat-free mass
(FFM) to total tissue lost during food restriction. In
the study mentioned above, the amount of FFM lost
during periods of weight loss was 58% of the total,
which is similar to that predicted using Forbes’ equa-
tion and is consistent with undernutrition as the
underlying mechanism of weight loss in this group
of people with HIV.
0021These findings suggest that an adequate supply of
nutrients could prevent weight loss or promote weight
gain in people with HIV-related weight loss but
simple deficiency of nutrients is not the only possible
cause of weight loss. Several other aspects of altered
metabolism have been described in people with HIV
infection, termed metabolic dysregulation, which
may account for relatively greater losses of lean
body mass relative to fat in some people (a predomin-
antly cachectic mechanism). First, reduced de novo
lipogenesis is a classic response to starvation in
healthy subjects. In AIDS wasting, de novo lipogen-
esis is increased in the majority of subjects. Second,
AIDS wasting is associated with hypertriglyceridemia
and low serum cholesterol levels compared with HIV-
negative controls, which may be indicative of futile
cycling of free fatty acids and triacylglycerols. Futile
cycling is thought to be mediated by TNF and is said
to occur when free fatty acids are released from fat
and returned to the liver, where they are reesterified in
triacylglycerols and secreted as very-low-density lipo-
proteins (VLDL), to return to the fat cell for break-
down and restorage as triacylglycerols. Third, AIDS
wasting is associated with serum testosterone levels in
the lowest quartile of the normal range. Low testos-
terone concentrations are observed in about 50% of
men with wasting and are usually associated with
advanced disease, weight loss, and hypogonadism,
suggesting that the low concentrations are stress- or
starvation-induced.
0022The above aspects of metabolic dysregulation do
not occur uniformly amongst people with HIV-
related weight loss and considerable heterogeneity
has been noted in this population. It has been sug-
gested that people with AIDS wasting fall into differ-
ent pathogenetic subsets and that it may be possible
to categorize people into those who have lost weight
as a result of ‘starvation’ and who may therefore
respond to provision of nutrients and differentiate
them from the subset of patients who are cachectic
and may not be able to respond appropriately to
nutrition.
Nutritional Problems for People with HIV
0023People who are HIV-positive are vulnerable to a wide
range of pathogens. A person’s ability to continue to
eat normally may be altered by the disease itself or by
the treatment (Table 1). The nutritional problems for
people with HIV fall into three main categories:
HIV DISEASE AND NUTRITION 3115
1.0024 Wasting and weight loss resulting from symptoms
that have an impact on food intake, such as dys-
phagia, taste changes, pain, nausea and vomiting,
and shortness of breath
2.
0025 Restrictions on food intake imposed by antiretro-
viral treatments
3.
0026 The side-effects of antiretroviral therapy, such as
nausea, vomiting and diarrhea and dsylipidemias,
impaired glucose tolerance, and body shape
changes
Dietetic management can be effective in managing
weight loss resulting from a range of symptoms.
Drug regimens may demand one of the following
adaptations:
1.
0027 Eating at the same time as taking the drug
2.
0028 Avoiding food for an hour or two after taking the
drug
3.
0029 Eating or avoiding certain types of food in order to
insure maximum absorption of medication
Dietary advice to accommodate antiretroviral ther-
apy is highly individualized and tailored to specific
circumstances and to specific combinations of drugs
and therefore will not be covered in any detail here.
0030The metabolic and body shape changes associated
with HIV represent a new challenge in the manage-
ment of HIV infection. The aim of the management of
fat redistribution is to replace lost fat and to reduce
accumulated fat deposits. So far, management has
tended to concentrate on changes to drug therapy
which involve switching away from drugs implicated
in the causation of the syndrome. A range of interven-
tions have been tried and modest benefits have been
reported, which may in part relate to the relaxation of
dietary restrictions associated with some medications
and to improved well-being. The use of recombinant
human growth hormone has been shown to have
some positive benefits, predominantly on reducing
accumulations of abdominal and dorsocervical fat,
in a few small studies. Diet and exercise remain
unevaluated as possible management strategies for
the fat redistribution syndrome.
0031The clinical significance of the metabolic compli-
cations associated with the fat redistribution syn-
drome are not known. A small number of reports
tbl0001 Table 1 Common manifestations of acquired immunodeficiency syndrome (AIDS) and potential nutritional problems
AIDS-relatedinfections andcancers Potentialnutritional problems
Opportunistic infections
Fungal
Candida
Oral Sore mouth, altered taste perception, anorexia, reduced saliva production
Esophageal Dysphagia
Cryptococcus
Meningitis Pyrexia, nausea, and vomiting
Protozoan
Toxoplasmosis Pyrexia, ethargy, confusion
Pneumocystis carinii pneumonia (PCP) Pyrexia, dyspnea, anorexia and weight loss, tiredness and lethargy
Bacterial
Mycobacterium avium intracellulare (MAI) Pyrexia, anorexia and weight loss, diarrhea and malabsorption
Viral
Cytomegalovirus (CMV) Pyrexia, diarrhea, and malabsorption
Herpes simplex (oral) Dysphagia
Human immunodeficiency virus (HIV) Pyrexia, diarrhea, and weight loss
Parasitic
Cryptosporidium Diarrhea and malabsorption, anorexia, weight loss, nausea and vomiting, pyrexia
Microsporidia
Cyclospora
Isospora
Cancers
Kaposi’s sarcoma (gastrointestinal) Dysphagia, sore mouth, anorexia, abdominal discomfort and obstruction, diarrhea, and
malabsorption
Non-Hodgkin’s lymphoma Anorexia, weight loss, dysphagia, diarrhea
Other
AIDS enteropathy Diarrhea and malabsorption, weight loss
AIDS encephalitis Confusion, dementia, lethargy
Side-effects of HAART Nausea, diarrhea, dyslipidemias
Coinfections e.g. hepatitis B and C, alcoholic liver disease
HAART, highly active antiretroviral therapy.
3116 HIV DISEASE AND NUTRITION

have been published of myocardial infarction in
people on HAART. Additionally, fatal pancreatitis
with hypertriglyceridemia has been reported. The
extent to which lipid disturbances and hyperglycemia
are associated with an increased risk of vascular
disease and increased survival is unknown and is the
subject of a 15 000-patient global study. Results are
not expected for another 2 years. Currently, manage-
ment of isolated hyperlipidemia is through conven-
tional dietary advice and lipid-lowering agents. As
some statins (human menopausal gonadotropin
coreductase inhibitors) may interact with protease
inhibitors, advice should be sought before introdu-
cing these agents.
0032 The effective treatment of the fat redistribution
syndrome will be most successful only once the mech-
anisms are understood. However, approaches which
in small, mostly cohort studies have yielded benefit in
some patients include exercise, growth hormone,
antiretroviral therapy modification, and metformin.
No uniformly effective management has been estab-
lished. The use of supplements such as acetyl-l-carni-
tine, coenzyme Q-10 (ubiquinone), and riboflavin to
support mitochondrial function in adipocytes has
been widely suggested but not evaluated.
Objectives of Nutritional Support
0033 The objectives of nutritional support in people with
HIV infection vary widely depending on the stage of
the disease and the presence or absence of symptoms
which have an impact on nutritional intake.
Asymptomatic HIV Infection
0034 When a person is diagnosed with HIV infection but
is symptom-free, he or she often considers dietary
change within a framework of lifestyle changes to
maintain health. Dietary information is available in
a variety of media, from the advice of friends and
family, to magazine articles, television programs, and
the internet. The rationale for making dietary changes
in people with asymptomatic infection is based on
avoiding nutrient deficiencies, which may have an
impact on immune function and maintaining an
ideal body weight. Advice is aimed at promoting a
regular balanced intake of a variety of foods. There is
no evidence for increased or decreased requirements
of any nutrient compared with the HIV-negative
population.
0035 Prior to the introduction of HAART, healthy-
eating guidelines designed to promote a reduced
intake of fat and sugar and an increase in fiber were
considered inappropriate in people with HIV. Since
the introduction of HAART and the associated
survival advantages and potential cardiovascular
side-effects, it may be pertinent to provide dietary
advice in line with healthy-eating guidelines. There
is no evidence base for such a recommendation,
however.
0036People with HIV infection are at greater risk of
contracting food- and waterborne infections since
they are immunosuppressed and often suffer from
coexisting disease or infections. It is generally recom-
mended that people with HIV are given advice on
food hygiene and water safety. Some local policies
specify that this happens once a defined level of
immunosuppression is reached. Cryptosporidiosis is
a waterborne protozoa which can cause chronic diar-
rhea in immunosuppressed individuals. There have
been reports of outbreaks of cryptosporidial infection
in people with HIV infection where tap water has
been implicated as the cause. The UK Department of
Health recommends that people with HIV with a low
CD4 lymphocyte count should boil all water (includ-
ing still, bottled water) used for drinking, brushing
teeth, and washing fruit and salad vegetables. This
practice has not been adopted throughout the UK and
will vary with local policies.
0037Unproven diet therapies There is currently no cure
for HIV/AIDS. Faced with this, many people seek to
take control of their own treatment and this often
involves the use of diet therapies, which claim to
prevent the progression of the disease, or to cure it.
There can be tremendous psychological benefit from
following a particular treatment, and people should
not be discouraged from following a regime of their
choice, but helped to evaluate and adjust their eating
habits in order to meet nutritional goals. It is import-
ant that eating remains an enjoyable experience and
that people do not subject their food choice to
unnecessarily rigid rules that may detract from
enjoyment.
0038The following considerations are helpful in evalu-
ating dietary options:
.
0039The diet should not contain substances in amounts
that may be physically harmful.
.
0040It should not completely replace health care that is
generally accepted as effective.
.
0041It should allow for an adequate energy and protein
intake along with a variety of foods.
.
0042It should not incur unnecessary expense or hard-
ship.
Symptomatic HIV Infection
0043Many of the manifestations of HIV infection affect a
person’s ability to eat normally and maintain body
weight, and therefore nutritional support is indicated.
HIV DISEASE AND NUTRITION 3117

The management of a person with weight loss should
involve a number of steps: first, diagnosis and treat-
ment of any underlying opportunistic infections,
second, control of any symptoms that may have an
impact on food intake; and third, dietary advice.
0044 In the first instance dietary advice should be to
maximize food intake by making alterations in the
type and timing of meals, including well-chosen
snacks between meals, and possibly modifying exist-
ing foods to increase their energy and protein content.
This approach is a basic tool of dietetics that has
received little research attention. A small uncon-
trolled study in 34 people with HIV demonstrated
that dietary advice was associated with significant
improvements in nutrient intake, weight, and anthro-
pometric indices. A recent randomized controlled
study of dietary counseling with or without oral nu-
tritional supplements showed that nutritional coun-
seling can achieve a substantial increase in nutrient
intake in 50% of malnourished people with HIV
which after 6 weeks was not associated with changes
in weight and nutritional status.
0045 A second line of dietary intervention is the use of
specialized proprietary food supplements in combin-
ation with a balanced food intake. These usually take
the form of prepacked drinks that are nutrient-dense
and nutritionally complete. Since the appearance of
these products 12–15 years ago, they have acquired
the reputation of being able to promote weight gain in
a person who is losing weight. A systematic review of
energy-dense supplements in illness-related malnutri-
tion has demonstrated significant benefits to weight
and nutritional status but the effects on morbidity
and mortality are less clear. A small number of studies
have looked at the use of oral nutritional supplements
in people with HIV and demonstrated short-term
benefits to nutritional intake, weight, and nutritional
status. More studies are needed to clarify the role of
nutritional intervention in HIV-related weight loss
and particularly the effects on morbidity, mortality,
and clinical outcome.
0046 If adequate nutrition cannot be achieved orally,
then enteral or parenteral nutrition should be con-
sidered. The major indication for nutritional support
in HIV is the failure to maintain body weight. The
main goals of nutritional support are to improve
survival morbidity by reducing the complication rate
associated with secondary infections and to improve
quality of life. There are a small number of studies
that have looked at the efficacy of nutritional support
in HIV. In general they have concentrated on the
safety and on the ability to replenish lean body
mass. Reports of rates of infection vary considerably
with enteral and parenteral feeding but the general
conclusions are that nutritional support can be
provided with safety in people with HIV infection
but should be undertaken with caution because of
the serious risk of infection. A small number of
studies have looked at the ability to replenish lean
body mass using enteral and parenteral nutrition.
The results suggest that nutritional support can effect-
ively maintain body composition and reverse the
depletion of fat and lean tissue in patients with weight
loss in the absence of concurrent infection or when
provided in conjunction with effective treatment of
an infection. In the stressed catabolic patient with
systemic infection, malnutrition is not restored
towards normal with nutritional support and weight
gains tend to be mainly fat and not lean body mass. It
is important to note that in some studies the provision
of artificial feeding led to prolonged survival with
improved functional capacity and resumption of
employment – benefits which should not be over-
looked when considering the initiation of nutritional
support.
0047The provision of nutritional support in the terminal
stages of disease is a controversial issue. One study
demonstrated benefits to quality of life associated
with the provision of parenteral feeding in the ter-
minal stages of illness. Recently, studies of the effects
on survival of enteral and parenteral feeding have
underscored the importance of starting feeding before
it is too late.
0048The area currently receiving the most interest in
relation to nutrition and HIV infection is the use of
growth hormone and anabolic steroids for their
ability to replenish lean body mass. Testosterone
and testosterone analogs and recombinant human
growth hormone have been demonstrated to replen-
ish lean body mass effectively in people with 5–15%
weight loss. Benefits have been demonstrated with
and without supervised exercise programs. This is a
relatively new area of nutrition and the potential role
of anabolic therapies in conjunction with the provi-
sion of nutritional support raises many questions:
.
0049Does increasing lean body mass change the prog-
nosis?
.
0050Is long-term anabolic steroid use safe?
.
0051Which patients are likely to benefit – those with
mild or advanced disease?
.
0052Should steroids be used intermittently or continu-
ously?
.
0053Which anabolic drug is most effective?
Advances in the understanding of the pathophysiol-
ogy of weight loss wasting have led to a greater
understanding of the role of nutrition in HIV infec-
tion. The primary determinant of weight loss is fre-
quently reduced food intake but this cannot alone
explain all aspects of HIV-associated wasting and
3118 HIV DISEASE AND NUTRITION