Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

Molds See Mycotoxins: Classifications; Occurrence and Determination; Toxicology; Spoilage: Chemical and
Enzymatic Spoilage; Bacterial Spoilage; Fungi in Food – An Overview; Molds in Spoilage; Yeasts in Spoilage
Molluscs See Shellfish: Characteristics of Crustacea; Commercially Important Crustacea; Characteristics of
Molluscs; Commercially Important Molluscs; Contamination and Spoilage of Molluscs and Crustaceans;
Aquaculture of Commercially Important Molluscs and Crustaceans
Monosodium Glutamate See Taste Enhancers
MULTIPLE SCLEROSIS – NUTRITIONAL
MANAGEMENT
R Cichon and L Wadolowska, Warmia and Masuria
University in Olsztyn, Olsztyn, Poland
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Multiple sclerosis (MS) belongs to the demyelinating
diseases, which comprise a group of neurologic dis-
orders. Demyelinating diseases have in common the
pathologic feature of local or patchy destruction of
myelin sheaths in the central nervous system accom-
panied by an inflammatory response. Destruction of
the myelin sheaths leads to dysfunction of the central
nervous system (CNS) in transmission of electrical
nerve impulses.
0002 The term ‘sclerosis’ is applied to the hardening of
the CNS and is called ‘multiple,’ because multiple
areas of optic nerves, brain and spinal cord undergo
sclerosis, whereby myelin is replaced with sclera and/
or scar tissue. The disease was first described by
Cruveilhier in 1835 under the name ‘sclerose en
plaque,’ in that the disease is marked by the appear-
ance of hard patches throughout the brain and spinal
cord. Its outstanding symptoms are weakness,
muscular incoordination, jerky movements of the
eyeballs, paralysis, and a curious, deliberate way of
speaking, known commonly as ‘scanning speech.’
The condition has periodic remissions and on the
whole tends to become worse, but is seldom an im-
mediate threat to life. The disease most commonly
strikes between the ages of 20 and 40 years, and
females account for 60–70% of cases. The average
age of onset of the first clinical episode of MS is in the
third and fourth decades. It is rare for the disease to
begin in childhood or beyond the sixth decade, but it
is not unknown.
Features of Multiple Sclerosis
0003MS is pleomorphic in its presentation. The clinical
picture is determined by the location of foci of
demyelination within CNS. Classic features include
impaired vision, nystagmus, dysarthria, decreased
perception of vibration and position, ataxia and in-
tension tremor, weakness or paralysis of one or more
limbs, spasticity, and bladder problems. Diagnosis is
based on the clinical presentation, neurological tests
and magnetic resonance imaging (MRI, to reveal the
presence of plaques). There are two main forms and
two subtypes of the disease: relapsing-remitting
MS (RRMS), chronic progressive MS (CPMS), and
secondary progressive and benign MS. In RRMS,
periods of acute worsening of symptoms are followed
by spontaneous improvement. In CPMS, there are no
clear-cut attacks, and the symptoms become steadily
worse. This form of MS might progress rapidly,
4034 MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT

causing severe disability and even premature death
within a few years. Secondary progressive MS is
described when RRMS becomes progressive, and
benign MS when an initial attack is never followed
by another. The criteria for the diagnosis of clinically
definite MS include a reliable history of at least two
episodes of neurologic deficit and objective clinical
signs of lesions at more than one site within the CNS.
Clinically probable MS is defined as either two
attacks with clinical evidence of one lession or one
attack with clinical evidence of two lesions. However,
classifications of MS are based on clinical phenomen-
ology, and the definitions of relapse, remission, and
progression are still imprecise.
0004 MS usually presents in the form of recurring
attacks of focal or multifocal neurologic disfunction,
reflecting lesions within the CNS. The disease begins
most commonly in early adult life. The frequency of
flare-ups is greatest during the first 3–4 years of the
disease, but a first attack may be so mild as to escape
medical attention, for example, blurred or double
vision. Once the initial symptoms disappear, they
may never recur, and a period of months or years
may pass before other symptoms appear, such as
weakness of certain muscles, unusual tiring of a
limb, minor interference with walking, muscle stiff-
ness, dizziness, loss of bladder control, and disturb-
ances in the senses of touch, pain, and heat. Each
symptom may appear and then disappear, only to
be followed by another. The disease continues to
progress, and eventually, the patient becomes
crippled and even bedridden. However, the progres-
sion and remission of MS are different for every indi-
vidual. Although occasional patients die within the
first few years of disease onset, most do not, and the
average survival from MS is more than 30 years after
the onset of disease.
Pathology
0005 In 1961, Swank proposed the hypothesis that a
dysfunction of the blood–brain barrier is a primary
damage defect in MS. Current opinion holds that
autoimmunity or viral infection is likely to be impli-
cated in their pathogenesis.
0006 Many scattered, discrete areas of demyelination,
termed plaques, are the pathologic hallmark of MS.
Plaques vary in size and may be found anywhere
in the white matter but typically occur in the para-
ventricular areas of the cerebrum and subpially,
and within the brainstem and spinal cord. The per-
ipheral nervous system is not affected. Many plaques
are clinically silent. In fact, some autopsy studies
indicate that 20% of MS cases are clinically silent
during life.
0007Active MS lesions feature T-lymphocyte and mono-
cyte–macrophage accumulations about venules and
at plaque margins is being destroyed. The invasion
of white matter by inflammatory cells is held respon-
sible for the myelin breakdown. They also function as
scavengers of myelin debris; fat-laden macrophages
may persist for months, perhaps years, after the acute
inflammatory response has subsided. Despite much
research, viral inclusions have not been detected.
Only limited regeneration of myelin occurs, and the
reason is unclear. There are probably several mechan-
isms responsible for recovery from an MS attack. The
pathologic features of MS fail to account for hour-to-
hour and day-to-day waxings and wanings in func-
tion so characteristic of the disease. Conduction of
impulses through demyelinated nerve is compromised
and is further altered by transient changes in the
internal milieu such as functuations in temperature
and electrolyte balance or by stress.
Etiology
0008The causes of MS remain unknown. A role for
immune-mediated or infectious factors has been pro-
posed, but data to support these postulates are incon-
clusive. Epidemiological studies have implicated an
interplay between genetic and environmental factors
in the etiology of MS. It has been suggested that
nutrition and food pattern, particularly high con-
sumption of animal fat and low intake of fish prod-
ucts may play a role in the etiology of MS. Recently,
studies have focused on long-chain polyunsaturated
fatty acids (LCPUFA) and vitamin D.
Epidemiology
0009Epidemiologic studies have established several facts
that ultimately will have to be incorporated into any
coherent theory of the disease. Neuroepidemiology
has played a fundamental role in the study of multiple
sclerosis by providing some etiologic clues, although
a definitive basis for the conclusive resolution of its
enigma is still lacking. Epidemiologic and genetic
studies have indicated that MS is probably caused
by multiple factors, both genetic and environmental,
none of which is individually sufficient, and appear to
act before adolescence – or possibly later – in genetic-
ally susceptible individuals. This unifying hypothesis
emphasizes the role of a genetic–racial susceptibility,
the importance of environmental factors, a possible
etiologic heterogeneity, and a lack of specificity of the
unknown endogenous and exogenous agents. Situ-
ations or events with biological plausibility, such
as childhood or adolescent infectious diseases, ex-
posures to geographic and sociocultural factors,
MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT 4035

nutritional habits, hypersensitivity, significant head
and spinal trauma, and other factors may contribute,
at different times, to the putative acquisition of MS,
trigger its onset, and modify its subsequent course.
0010 In general, the incidence in temperate climates
exceeds that in tropical zones, but variations within
regions with similar climates do exist; hence, the
effect is not simply one of latitude or temperature.
Geographically, MS describes three frequency zones.
High-frequency areas (characterized by a prevalence
of 30þ per 100 000) now comprise most of Europe,
Israel, Canada, northern USA, southeastern Australia,
New Zealand, and eastern Russia. Medium-frequency
areas include the southern USA, most of Australia,
South Africa, the southern Mediterranean basin,
Russia into Siberia, the Ukraine and parts of Latin
America. Prevalence rates of less than 5 per 100 000
are found in the rest of Asia, Africa, and northern
South America. The incidence of MS in northern
Europe, Canada, and the northern USA is approxi-
mately 10 new cases each year per 100 000 persons
between the ages of 20 and 50, two to three times
higher than that in Australia, New Zealand, and the
southern USA. MS is rare in Japan, elsewhere in the
Orient, and Africa. Some epidemiologic evidence also
suggests that persons emigrating from high- to low-
risk regions as children may be partially protected
from MS. Immigrants from high- to lower-risk areas
retain the MS risk of their birth place only if they are
at least 15 years old at the time of emigration. Those
from low- to high-risk areas increase their risk
even beyond that of the natives, with susceptibility
extending from about 11 to 45 years of age. MS
occurred in epidemic form in the North Atlantic
islands, particularly in the Faroe Islands, where the
first symptom onset was in 1943, heralding the first of
four successive epidemics at 13-year intervals. What
was transmitted is thought to be a specific, wide-
spread, persistent infection called primary multiple
sclerosis affection (PMSA), which only rarely leads
years later to clinical MS. The search for PMSA is best
attempted on the Faroes, where there are regions still
free of MS after 50 years. The data are consistent with
the existence of an environmental factor, possibly a
virus, and perhaps geographically restricted, that
influences the development of MS. Immunologic,
epidemiologic, and genetic data indicate that tissue
injury in MS results from an abnormal immune re-
sponse to one or more myelin antigens that develop in
genetically susceptible individuals after exposure to
an as-yet undefined causal agent.
0011 There is some evidence for genetic factors in mul-
tiple sclerosis. The evidence comes from epidemiolo-
gic studies, racial predilection, risk in family members
(sibs, half sibs, adoptees), and twin studies. MS is not
a Mendelian inherited disease; only the susceptibility
to the disease is inherited. MS seems to be an oligo-
or multigenic disorder with an apparently similar
phenotype for the different genes involved. A genetic
component in MS is indicated by an increased relative
risk to siblings compared with the general population
and an increased concordance rate in monozygotic
compared with dizygotic twins. Whole genome
screens conducted in different populations have
identified discrete chromosomal regions potentially
harboring MS-susceptibility genes.
Nutrition and Multiple Sclerosis
0012Specific nutritional therapy has been advocated for
a number of neurologic diseases of undetermined
etiology. In some of the disorders, improper or
inadequate nutrition is implicated. Therefore, dietary
manipulation constitutes the main therapeutic mode.
For instance, a low-fat diet has been recommended as
an effective means of reducing the incidence of
exacerbations in patients suffering from MS. How-
ever, objective evaluation of the efficacy of this treat-
ment modality has not yet been possible. In MS, a
combination of genetic and environmental factors,
including dietary factors, underlies the symptoms
and signs of neurologic dysfunction that can be ameli-
orated by changes in the diet and/or vitamin supple-
mentation.
0013Epidemiologic studies relating MS to nutritional
factors have revealed a possible link between the
incidence of the disease, total fat intake, and percent-
age of calories (of animal origin) consumed. A long-
term study carried out by Swank showed significantly
less deterioration and much lower death rates among
MS patients when they consumed less fat (20 g of fat
per day).
0014The results of prospective case-control studies
showed that some foods consumed at certain ‘critical’
ages could play a causal role in the oneset of MS. An
association was suggested between MS and high
consumption of bread and ‘pasta,’ butter and lard,
legume soup, horse flesh, coffee and tea in the period
from infancy to adolescence, and of eggs and wine
during adulthood. A possible autoimmune demyeli-
nating disease with lipid changes suggests a deficiency
of PUFA.
0015MS tends to be more prevalent in countries where
the use of animal fat is high. It has also been suggested
that the administration of unsaturated fatty acids,
such as linoleic or arachidonic acid, may reduce the
number and severity of MS attacks. This idea is based
on the observation that brain and spinal cord
obtained from patients who have died of MS is defi-
cient in unsaturated fatty acids and that linoleic and
4036 MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT

arachidonic acids tend to inhibit the lymphocyte–
antigen interaction, the cellular mechanism that may
enhance demyelination. Sensitized lymphocytes prob-
ably interact with myelin components in the affected
parts of the nervous system during an attack of MS.
That the ingestion of unsaturated fatty acids, such
as linoleic acid, affects the course of MS remains
unproved.
0016 Early epidemiological studies demonstrated a low
incidence of atheroslerotic, inflammatory, and auto-
immune diseases in Greenland Eskimos who con-
sumed diets high in marine-derived (n-3) PUFA.
Human studies have consistently demonstrated a de-
crease in production of pro-inflammatory cytokines
when moderate to high levels of marine-derived (n-3)
PUFA are taken orally. The decrease in production of
pro-inflammatory cytokines and eicosanoids contrib-
utes to the beneficial effect of fish oil in reducing the
pathogenesis of inflammatory and atherosclerotic dis-
eases. Essential fatty acids (EFA) are necessary for
normal immune function of humans and animals.
EFA deficiency impairs B- and T-cell-mediated re-
sponses. These impairments can be ameriorated by
the inclusion of EFA in the diet. The possibility that
polyunsaturated fatty acids have an immunosup-
pressant effect has led to the evaluation of
high-polyunsaturated fatty acids diets in MS, as neu-
rologic disorders of immune-inflammatory etiology
that affect CNS. a-Linolenic acid (C18:3 n-3) can be
converted to EPA (C20:5 n-3), which can replace
arachidonic acid in membrane phospholipids and
can be preferentially used by cyclooxygenase. This
results in the reduced production of prostaglandins
(PG) of the 2 series and leukotrienes of the 4 series.
Thus, the consumption of oils containing C18:3 n-3
might be associated with immunological changes.
This opinion is supported by many studies that have
shown immunological modulation following marine
oil consumption.
0017 Evidence on etiology in MS suggests that the preva-
lence depends on the interaction of two factors, diet
and exposure to visible sunlight. The dietary features
that may be beneficial include supplementation with
fish oils, avoidance of saturated fats, and the associ-
ated intake of antioxidants with unsaturated fatty
acids. Inhibition, by antioxidants, of the enzyme
lipoxygenase inhibits leukotriene synthesis, and the
presence of fish oils leads to the production of leuko-
trienes with less inflammatory properties. This is of
particular importance in the retina, where leuko-
trienes might be the underlying cause of retrobulbar
neuritis.
0018 A significant protective effect has been observed
with other nutrients, including vegetable protein,
dietary fiber, vitamin C, thiamin, riboflavin, calcium,
and potasium. With respect to specific foods (as op-
posed to nutrients), a higher intake of fruit juices was
inversely associated with risk. A protective effect was
also observed with cereal/bread intake; pork/hot dogs
and sweets/candy were positively associated with
risk. The study generally supports a protective role
for components commonly found in plants (fruit/
vegetable and grains) and increased risk with high-
energy and animal food intake.
0019An epidemiologic study on the relationship be-
tween mortality rates from MS for the period 1983–
1989 for 36 countries has shown that saturated fatty
acids, animal fat, animal minus fish fat, and latitude
correlated independently and positively with MS
mortality. The ratio of polyunsaturated fatty acids
to saturated fatty acids (P/S ratio) and the ratio of
unsaturated to saturated fatty acids (U/S ratio) correl-
ated independently and negatively with MS mortality.
The results support the data, at least partially, on an
association between certain dietary factors and MS.
0020For MS patients, good nutrition has the potential
to enhance the quality of life and reduce the risk of
lifestyle diseases and secondary conditions. Eating
patterns in patients with MS showed the need for
interventions to promote good nutrition among per-
sons with MS. Usually, nutritional intake for MS
patients is not optimal in many important areas.
0021Acute and chronic neurologic diseases of nonnutri-
tional origin that impair consciousness of motor func-
tions essential to adequate nutritional intake, such
as paralysis or weakness of the facial muscles, the
tongue, the pharynx, and the muscles of deglutition,
frequently require the temporary or permanent use of
a nasogastric tube or gastrostomy for the patient’s
well-being. These measures make possible proper
enteral nutrition and may, in fact, prove to be life-
saving. In most of these disorders, nutritional support
does not affect the basic pathogenesis of the disease.
The use of B-complex vitamin preparations for a
variety of acute and chronic neurologic diseases of
cryptic origin continues to be common medical prac-
tice. To date, however, there is no objective evidence
that this practice has any effect on the speed of recov-
ery of the afflicted nervous tissue.
0022Despite significant advances over previous decades
in the field of nutrition, large gaps remain in our
understanding of the role in the normal and abnormal
activity of the nervous system. More sensitive and
critical methods for the assessment of the nutritional
status of the nervous system and for the evaluation
of the dietary management of MS are essential for
more rational and effective therapeutic manipulation
(treatment).
0023Nutritional therapy consisting of vitamins and
other nutrients continues to be used in neurologic
MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT 4037

disorders of unknown cause, in spite of a total lack of
scientific rationale. The popularity of administering
large doses of vitamins (and other nutrients) as ther-
apy for chronic neurologic diseases of uncertain eti-
ology stems from the fact that experimentally induced
deficiencies of this nutrients in animals frequently
result in symptoms caused by reversible lesions of the
CNS. In most instances, the far-advanced lesions show
demyelination, a frequent finding in many human
neurologic diseases. However, considering the large
doses of vitamins consumed daily, for a variety of
reasons, by an ever–increasing number of people, vita-
min toxicity affecting the nervous system is relatively
rare. Of all the vitamins, only two – vitamin A and
pyridoxine – are known to produce adverse neurolo-
gic reactions when ingested in pharmacologic, rather
than recommended, nutritional doses.
0024 Patients who are being treated with drugs may
incur a significant degree of vitamin deficiency (D,
B
12
, and folic acid). The prolonged administration of
drugs may lead to a decrease in bone mineral content.
The drugs interact with the vitamin D and its active
forms, decreasing intestinal calcium absorption
and redistribution. The severity of demineralization
appears to be related to the dose of the drugs, a
deficiency of physical activity, and a lack of exposure
to sunlight. In general, the problem does not appear
to be of sufficient clinical importance to warrant the
routine vitamin D supplementation of patients with
MS drugs; however, the possibility should be borne in
mind, and vitamin D metabolites should be estimated
periodically in long-term patients with poor intake or
malabsorption.
0025 Studies with animals, tissue cultures, as well as
humans indicate that both the level and degree of
saturation of dietary fats influence inflammatory
and immunologic responses. Some of these immuno-
logic changes are associated with beneficial clinical
effects, for example, reduction in pro-inflammatory
cytokine by marine-derived (n-3) PUFA. Others might
not be desirable, for example, decreased T-cell-
mediated function by marine-derived (n-3) PUFA in
older people.
0026 Recommendations to increase PUFA intake should
be accompanied by appropiate recommendations for
an increase in antioxidant intake, in particular vita-
min E. Without adequate antioxidant protection, the
substitution of membrane fatty acids with highly oxi-
dizable (n-3) PUFA of fish oil, that is, EPA and DHA,
may potentiate the peroxidation of cellular mam-
branes. Foods high in polyunsaturates should contain
at least 0.6 mg of tocopherol equivalents per gram of
polyunsaturated fatty acids. Higher levels may be
necessary for fats rich in fatty acids containing more
than two double bonds.
0027In general, for MS patients, recommendations to
decrease dietary total fat intake, with the inclusion of
moderate amounts of (n-6 and n-3) PUFA with ad-
equate antioxidant nutrients should provide for a
competent immune response. The n-6 and n-3 fatty
acids have critical roles in the membrane structures
and as precursors of eicosanoids, which are potent
and highly reactive compounds. Various eicosanoids
have widely divergent, and often opposing, effects
on inflammatory processes and the immune system.
Since they compete for the same enzymes and have
different biological roles, the balance between the n-6
and n-3 fatty acids in the diet can be of considerable
importance. The ratio of linoleic to a-linolenic acid in
the diet should be between 5:1 and 10:1. Patients with
a ratio in excess of 10:1 should be encouraged to
consume more n-3 rich foods such as green leafy
vegetables, legumes, fish, and other seafood.
Dietary Management of Multiple Sclerosis
0028Although there have not been any valid clinical trials
supporting the efficacy of nutrition in delaying the
progression of MS, it is imperative that the dietitian
evaluates the nutritional health status and arranges a
patient’s diet. The nutritional management of patients
with MS is primarily concerned with ensuring that
their nutrient intake meets the requirements. The spe-
cific dietary modifications that are needed in some
patients, mostly because of drug therapy, are of
secondary importance. The principles of management
have to take in consideration the individual needs,
circumstances and difficulties. The current consensus
is that extreme dietary change should have no place in
the management of MS. Patients with MS should be
encouraged to follow a varied, well-balanced diet
based on good nutritional practice and principles for
the population in general. In order to achieve the
recommended dietary targets, considerable changes
in the dietary habits of the MS patient will be
required, usually necessitating:
.
0029increased intake of micronutrient-rich foods such
as fruits, vegetables, pulses, seeds, legumes, and
cereals. Leafy green vegetables may contribute
adequate amounts of antioxidative vitamins, e.g.,
vitamins E and C;
.
0030use of low-fat alternatives for full-fat milk and
dairy products;
.
0031replacing saturated fat spreads and cooking fats
with low-fat spreads and monounsaturated oils;
.
0032avoiding sugar-rich/fat-rich food group, such as
meat products, pastries, chips, snakes, cakes and
biscuits;
.
0033encouraging the consumption of all types of fish
and seafood; two portions of fish or seafood per
4038 MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT

week, including oily fish, are recommended to
secure a moderate increase intake of n-6 and n-3
fatty acids, in particular LCPUFA.
0034 An important consideration in the management of
all patients is their hydration status. The consumption
of at least six to eight glasses of fluid per day usually
meets the adequate fluid intake of a patient.
0035 Nutritional problems associated with MS vary
according to the symptoms of illness and the degree
of physical disability of patients. Dysphasia may
occur as the disease progresses, and the diet consist-
ency may need to be modified from solid to soft or
pure
´
ed foods and even thick liquids. Other problems
include impaired vision, dysarthria, and poor ambu-
lation, thus making eating less enjoyable because
meal preparation becomes a difficult task. In this
situation, single-serving or convenience foods often
permits independent preparation of meals. Given the
chronic nature of this disease, patients may require
enteral nutrition support.
0036 Neurogenic bladder is common, causing urinary
incontinence, urgency, and frequency. To minimize
these problems, it is helpful to distribute fluids evenly
throughout the waking hours and limit them before
bed. Some patients limit fluid intake severely to
decrease the frequency of urination, thus increasing
the risk of urinary tract infection.
0037 Neurogenic bowel can cause either constipation or
diarrhea, and the incidence of fecal impaction is
increased in MS. A diet that is high in fiber with
additional prunes and adequate fluid intake can mod-
erate these problems.
Supplement Usage
0038 Patients may be taking combinations of different
supplements in large doses, sometimes risking over-
dosage with fat-soluble vitamins. The types of supple-
ments likely to be used include evening primrose oil,
fish oil capsules, cod liver oil, and linseed oil. If a
well-balanced diet containing dietary sources of n-3
and n-6 fatty acids is consumed, additional supple-
ments of LC-PUFA sources, vitamins, and minerals
are unlikely to be necessary or beneficial. Patients
who wish to take supplements should be advised to
restrict these to one multiple multivitamin/mineral
preparation providing no more than the recom-
mended dietary allowance, rather than taking several
different types of supplement. In any case, it is best to
do this after consultation with the dietitian.
See also: Cholecalciferol: Properties and Determination;
Essential Fatty Acids; Fish Oils: Dietary Importance;
Vitamins: Overview
Further Reading
Antel JP and Arnason BGW (1987) Demyelinating diseases.
In: Braunwald E et al. (eds.) Harrison’s Principles of
Internal Medicine, 11th edn, pp. 1995–2000. New
York: McGraw-Hill.
Briony T (ed.) (2001) Manual of Dietetic Practice, 3rd edn.
Oxford: Blackwell Science.
FAO/WHO (1994) Fats and Oils in Human Nutrition. FAO
Food and Nutrition Paper 57. Rome: FAO/WHO.
Hamazaki T and Okuyama H (ed.) (2001) Fatty acids and
lipids – new findings. World Review of Nutrition and
Dietetics 88.
Kahana E (2000) Epidemiologic studies of multiple scler-
osis: A review. Biomedicine and Pharmacotherapy 54:
100–102.
Kurtzke JF (2000) Multiple sclerosis in time and space –
geographic clues to cause. Journal of Neurovirology
6(supplement 2S): 134–140.
Mahan LK and Escott-Stump S (eds) (2000) Krause’s Food,
Nutrition & Diet Therapy, 10th edn. Philadelphia, PA:
W.B. Saunders.
Oksenberg JR and Barcellos LF (2000) The complex genetic
aetiology of multiple sclerosis. Journal of Neurovirology
6(supplement 2S): 10–14.
Muscle See Exercise: Muscle; Metabolic Requirements
MULTIPLE SCLEROSIS – NUTRITIONAL MANAGEMENT 4039

MUSHROOMS AND TRUFFLES
Contents
Classification and Morphology
Use of Wild Mushrooms
Classification and Morphology
S Rajarathnam and M N Shashirekha, Central Food
Technological Research Institute, Mysore, India
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Mushrooms constitute a specialized group of fungi
and represent the fruiting bodies with a great diver-
sity in shape, size, color, and texture, bearing the
spores of sexual reproduction. In nature, they serve
the function of production, maturation, and dissem-
ination of spores, for the perpetuation of the species.
Thus, these mushrooms as a group of fungi, are
nonchlorophyllous organisms that cannot utilize
solar energy to manufacture their own food as do
green plants. However, mushrooms can produce a
wide range of enzymes that can degrade the complex
substrates on which they grow, following which they
absorb the soluble substances for their own nutri-
tion. This absorptive nutrition is a characteristic of
fungi. Mushrooms as macrofungi can be either epi-
geous, as in ‘morels’ or ‘field mushrooms,’ or hypo-
geous, as in ‘truffles,’ and large enough to be seen
with the naked eye and to be picked by hand. Mush-
rooms need not be aerial, or fleshy, or edible. Out of
69 000 described species of fungi, there are about
10 000 species of fleshy macrofungi, and only a
handful of these are lethal. There are no simple
ways of distinguishing between edible and poisonous
mushrooms. This will be dealt with in a later
section.
Classification
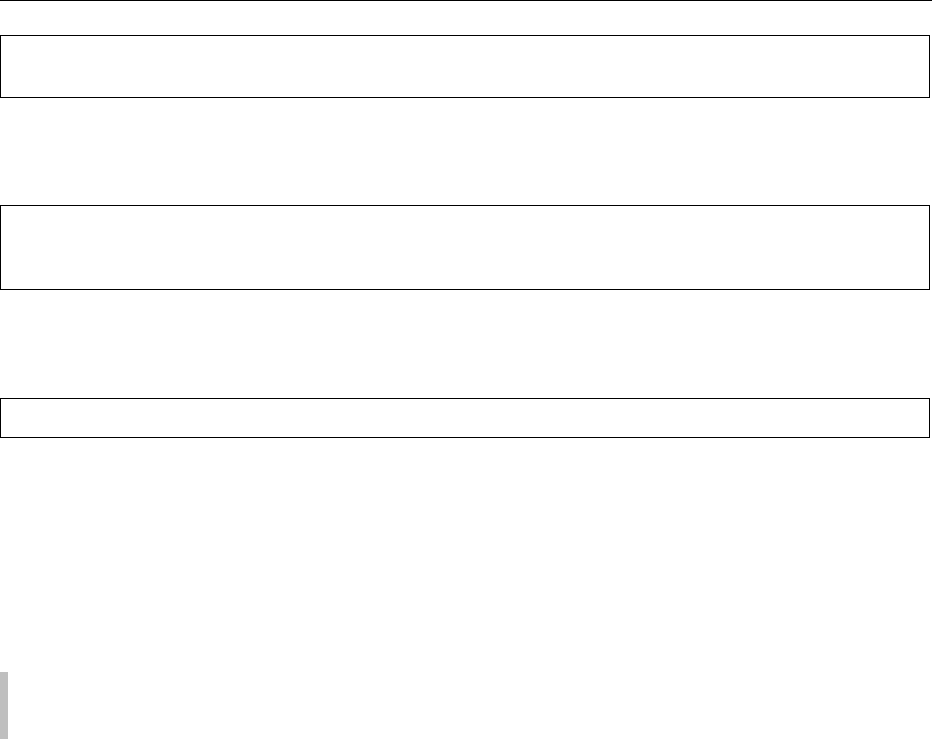
0002 Mushrooms and truffles fall under the class Basidio-
mycetes and a few orders of Euascomycetes, respect-
ively (Figure 1).
Euascomycetes
0003 Euascomycetes include morels (species of Morchella)
with epigeous fruiting bodies and truffles (species
of Tuber) with hypogeous fruiting bodies and are
characterized by the production of ascospores endogen-
ously inside special club-shaped structures called asci.
Basidiomycetes
0004Basidiomycetes are considered the most highly
evolved group of fungi and are characterized by the
exogenous production of basidiospores borne over
club-shaped structures called basidia.
Subclass: Hymenomycetes
0005This group includes all fungi composed of mem-
branes, fleshy, woody, or gelatinous, whether grow-
ing on the ground or on wood. The spore-bearing
surface, called the ‘hymenium,’ is external at an
early stage in the life cycle. The spores are borne on
basidia, and when the spores ripen, they fall to the
ground or are carried by the wind to a host that
presents all the conditions necessary for germination;
there, they produce the thread-like structures called
mycelia. Within these threads are small knots, which
in time develop into full-grown mushrooms.
0006The subclass Hymenomycetes is generally classi-
fied in one large order, the Agaricales, which in turn
is divided into six families:
1.
0007Agaricaceae–hymenium with gills;
2.
0008Polyporaceae–hymenium with pores;
3.
0009Hydnaceae–hymenium with spines;
4.
0010Thelephoraceae–hymenium horizontal and mostly
on the under surface;
5.
0011Clavariaceae–hymenium on a smooth club-shaped
surface;
6.
0012Tremellaceae–hymenium even and superior – gel-
atinous fungi.
Subclass: Gastromycetes
0013The word ‘Gastromycetes’ is derived from two Greek
words, ‘gaster’ (stomach) and ‘mycetes’ (fungus). The
hymenium is enclosed in the rind or peridium. The
word ‘peridium’ comes from ‘peridio’ (‘I wrap
around’), because the peridium entirely envelopes
the spore-bearing portion, which eventually sheds
the enclosed spores formed inside the basidia and
spicules. The cavity within the peridium consists of
two parts: a threaded part, called the capillitium,
4040 MUSHROOMS AND TRUFFLES/Classification and Morphology
which can be seen in any dried puff ball, and a cellular
part, called the gleba, which is the spore-bearing
tissue, composed of minute chambers lined with the
hymenium. The peridium breaks in various ways to
permit the spores to escape. When children pinch a
puff ball to ‘see the smoke,’ they are doing just what
the puff ball would have them do, scattering its seeds
to the winds.
0014 Gastromycetes has four orders:
A.
0015 Glebal chambers usually not separating from the
peridium or from each other;
B.
0016 Gleba powdery;
C.
0017 Hymenium present in early stages; spores mostly
light-colored, small – Lycoperdales;
0018 CC. Hymenium lacking or indistinct; spores mostly
dark, large – Sclerodermatales;
0019 BB. Gleba slimy and fetid; exposed on a receptacle –
Phallales;
0020 AA. Glebal chambers forming waxy peridioles, or
entire gleba separating as a unit from the peri-
dium – Nidulariales.
Distribution of Mushroom Species
0021Mushroom species are distributed throughout the
world, some very specific to certain geographic
areas, while others are universal and may occur in
different seasons in the same region. Temperature
plays a critical role in the distribution of mushroom
species, and so their distribution can be categorized
under tropical, subtropical, and temperate belts
(Table 1). The reason for specific distribution of
mushroom species in relation to temperature is to be
Class
Sub-class
Series Discomycetes Hymenomycetes
Agaricales
Gastromycetes
Lycoperdales
E.g. Lycoperdon
Pezizales
E.g. Morchella
Tuberales
E.g. Tuber
Sclerodermatales
E.g. Sclerodendron
Phallales
E.g. Phallus
Nidulariales
E.g. Cyathus
Family Agaricaceae
E.g. Agaricus
Polyporaceae
E.g. Polyporus
Hydnaceae
E.g. Hydnum
Thelephoraceae
E.g. Thelephora
Clavariaceae
E.g. Clavaria
Tremellaceae
E.g. Tremella
Order
Euascomycetes Basidiomycetes
Fungi
fig0001 Figure 1 Location of mushrooms and truffles in the classification of fungi.
tbl0001Table 1 Geographic distribution of various mushroom species
Climatic belt Mushroom species
Tropical Volvariella spp.
Subtropical Agaricus bitorquis
Pleurotus spp.
Temperate Agaricus bisporus
Boletus grevillei
Tricholoma saponaceum
Laccaria laccata
Polyporus squamosus
MUSHROOMS AND TRUFFLES/Classification and Morphology 4041
viewed to the specific enzymes secreted and factors
influencing these enzymes by the mushroom species
under study, in relation to the geographic conditions
of natural occurrence.
Morphology
Natural Habitat
0022 Mushroom species can be found growing on dead and
decaying plant material, humus soil, e.g., Agaricus,
as saprophytes on the dead trunks of live trees, e.g.,
Pleurotus, as parasites on the living trees, e.g., Armil-
laria, or characteristically in symbiotic association
with the roots of pine trees, e.g., Morchella. Species
of Termitomyces grow on the ant hills, again an
example of symbiosis. Tuber species grow under-
ground in certain European climates and their flavour
is often detectable by dogs.
Vegetative Phase
0023 Mushrooms have two phases in their life cycle: a
mycelium that is usually hidden and inconspicuous
with a longer growth phase followed by short-lived
fruiting bodies. The mycelium derives the nutrition
for its growth (which, after a period of establishment,
culminates in the production of fruiting bodies) under
certain defined favorable conditions. The conditions
for mycelial growth are not very specific, in contrast
to the very specific growth conditions required by the
fruiting bodies. The constraints and problems associ-
ated with the latter explain why several mushroom
species have yet not been able to be cultivated artifi-
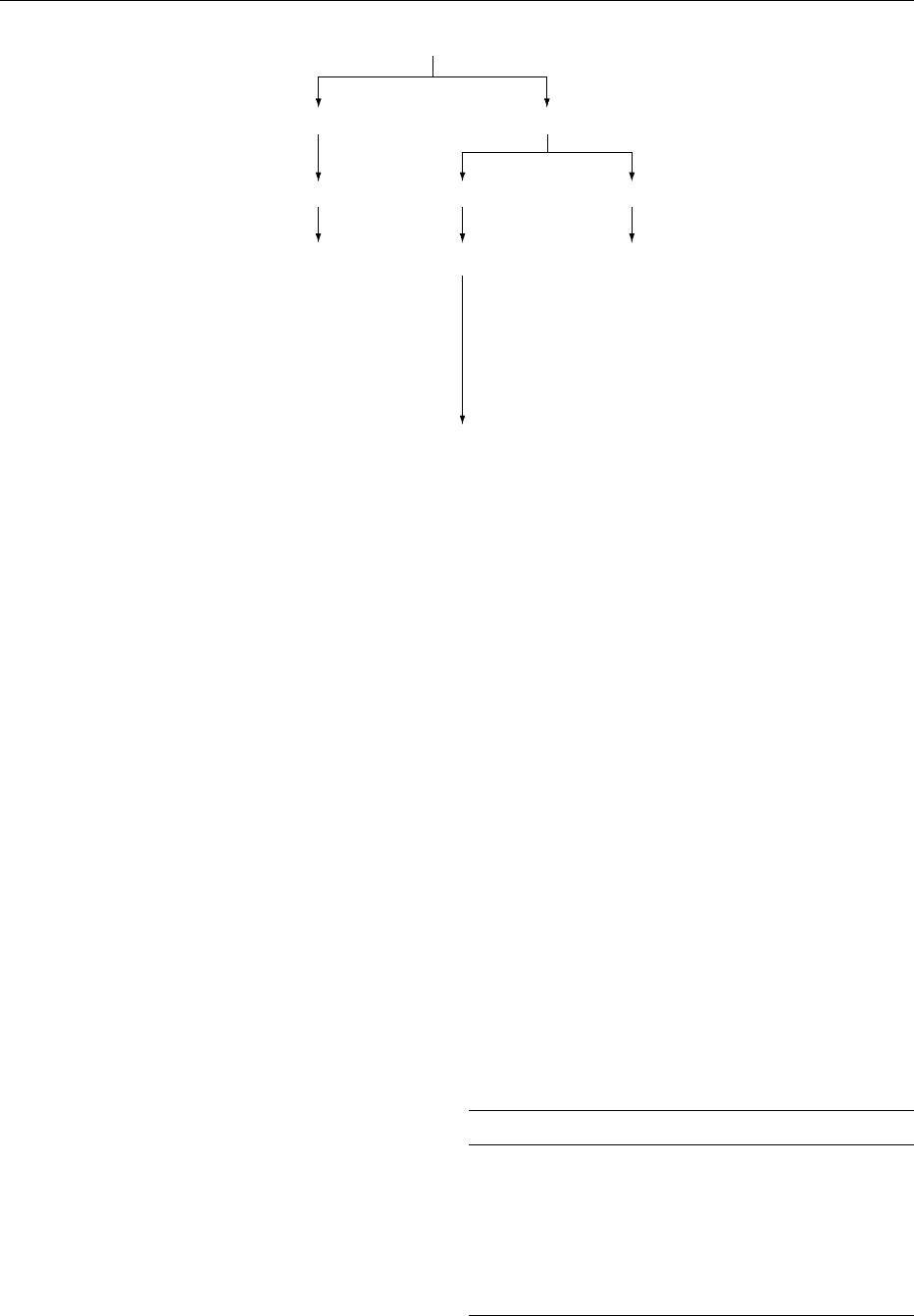
cially. Mycelia may be uninucleate (monokaryotic) or
binucleate (dikaryotic) (Figure 2), depending on the
species and stage in the life cycle. In nature, generally,
the spore germinates under favorable conditions to
produce the uninucleate mycelium.
Reproductive Phase
0024After a certain amount of vegetative growth depend-
ing on the availability of the compatible strain, the
uninucleate mycelium reaches the dikaryotic phase,
which in turn leads to the production of fruiting bodies,
bearing spores. For clarity, the typical life cycles of
three mushroom varieties are described below.
0025Primary homothallism Here, the basidiospore ger-
minates to produce the mycelium, which in turn is
self-fertile and ultimately can result in the production
of fruiting bodies, which bear gills, basidia terminat-
ing with four basidiospores (per basidium), as a prod-
uct of meiosis, e.g., Volvariella volvacea (Figure 3).
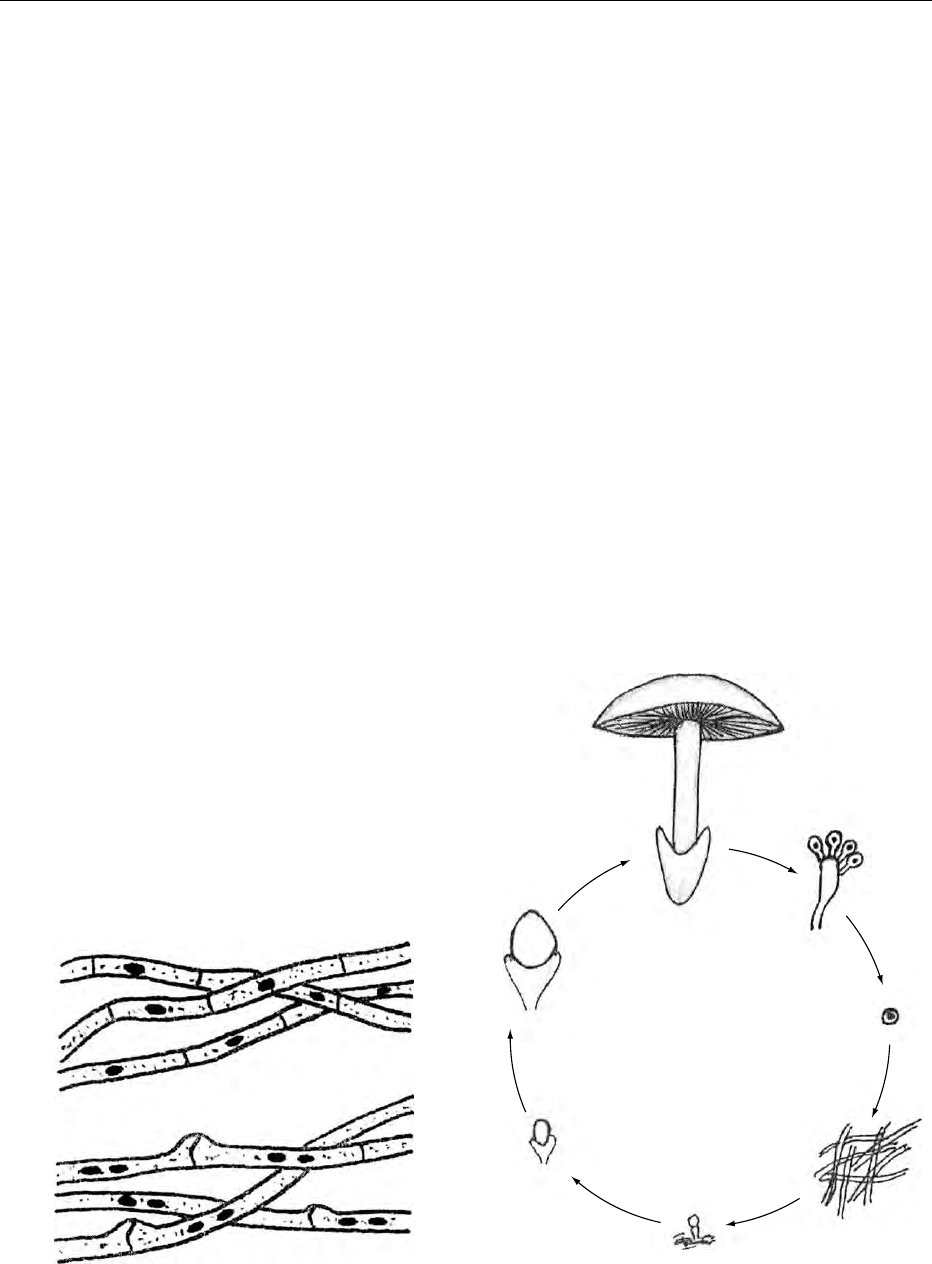
0026Secondary homothallism Agaricus bisporus is an
example of this phenomenon, wherein the basidium
by name itself bears only two spores, and each spore in
turn is binucleate, carrying both the compatible
factors in the same spore, so that the mycelium that
results from germination of the basidium finally yields
to the development of fruiting bodies (Figure 4).
a
b
fig0002 Figure 2 Mono- and dikaryotic mycelia. (a) septate without
clamp connections; (b) septate with clamp connections.
a
b
c
d
f
e
g
fig0003Figure 3 Primary homothallism in Volvariella volvacea. (a)
fruiting body; (b) basidium; (c) basidiospore; (d) mycelium; (e)
fruiting initial; (f and g) developing fruiting body.
4042 MUSHROOMS AND TRUFFLES/Classification and Morphology
0027 Heterothallism Species of Pleurotus are classic
examples of heterothallism, in which each basidium
bears four basidiospores, each genetically different
from the other, so that the degree of inbreeding is
reduced to 25%, with increased scope for outbreed-
ing of 75%. This represents possibly the most highly
evolved life-cycle system of the basidiomycetes and is
strengthened further by the operation of multiple
alleles at the two different loci (Figure 5).
Variations in Mushroom Morphology
0028 The fruiting body is the net result of a certain min-
imum amount of vegetative growth, followed by the
onset of conditions (physical, chemical, or biological)
favoring reproduction. The fruiting body that de-
velops typically has a stem/stalk called a ‘stipe,’ with
or without a basal cup, called a ‘volva,’ and a ring on
the stem known as an ‘annulus’ (Figure 6). The occur-
rence of an annulus/volva is dependent on the charac-
teristic nature of development or morphogenesis
of the fruiting body. The display of annulus and
volva also varies depending on the species (Table 2).
The stipe terminates with a cap, also called a ‘pileus’
varying in shape, size, texture, structure, and color,
and constituting one of the most beautiful objects of
nature on the earth. The great diversity in morph-
ology of the mushroom species is depicted in
Figure 7. The cap is variously colored, bright, or
dull. However, the toxicity of a mushroom bears no
relation to its coloration (Table 3). The cap consists of
a fertile layer called a ‘hymenium’ (Figure 8) compris-
ing gills, which in turn bear basidia with basidios-
pores at the distal end intercalated with sterile
cysitidia. The fruiting body may collapse as a result
of autodigestion, as in Coprinus (inky cap) or may
even have latex-containing tissues as in Lactarius
(milky mushroom).
0029Orientation of gills The morphology of gills con-
tributes to valuable taxonomic criterion in Agaricus,
when the gills are open from the genesis to the shed-
ding of basidiospores. Their attachment to the stipe/
stem varies and is specific to the species. Gills may be
free and detached from the stipe. A mushroom is
described as decurrent when the gills run down the
stem (the usual situation in many funnel-shaped
fruiting bodies), adnate when the gill is attached
along its entire width, adnexed when attachment is
along only a part of the total width, and sinuate when
there is a notch where the gill joins the stem. The
attachment of gills in the cap has a bearing on the
confluency of the cap, and this interrelation is
depicted in the Figure 9.
0030In Euascomycetes, ascospores are formed inside
the club-shaped structures called ‘asci,’ whereas in
a
b
c
d
e
f
fig0004 Figure 4 Secondary homothallism in Agaricus bisporus.
(a) fruiting body; (b) basidium with two basidiospores; (c) basi-
diospore; (d) mycelium; (e and f) developing fruiting body.
a
b
c
d
e
f
g
fig0005Figure 5 Heterothallic and tetrapolar life cycle in Pleurotus
sajor-caju. (a) fruiting body; (b) basidium with four genetically
different basidiospores; (c) basidiospores; (d) germinating
basidiospores; (e) monokaryotic mycelia; (f) dikaryotization;
(g) dikaryotic mycelia.
MUSHROOMS AND TRUFFLES/Classification and Morphology 4043