Markovchick Vincent J., Pons Peter T., Bakes Katherine M.(ed.) Emergency medicine secrets. 5th ed
Подождите немного. Документ загружается.

Chapter 65 ED EVALUATION OF CHILD ABUSE458
between preadolescent children fewer than 4 years apart in the absence of coercion, including
bribes or threats.
20. Should a normal physical examination decrease the suspicion of abuse?
No. A normal physical examination does not confirm or rule out sexual abuse. The vast
majority of children who report sexual abuse have normal physical examinations. Mechanisms
of child sexual abuse (e.g., fondling, oral-genital contact) often cause no physical trauma, but
the emotional trauma of such incidents may be significant.
21. Should child victims of sexual abuse be treated empirically for sexually
transmitted diseases (STDs)?
Prophylactic treatment of prepubertal children reporting sexual abuse is not usually indicated,
unless the perpetrator is known or presumed to be infected or sexual contact included genital
trauma or contact with bodily fluids. In cases of acute assault with high-risk exposure,
prophylactic antibiotics and emergency contraception may be offered as with an adult assault.
Consultation with a child abuse specialist/team may be helpful.
KEY POINTS: CHILD SEXUAL ABUSE
1. A normal physical examination does not rule out sexual abuse.
2. Most children do not require STD testing or prophylaxis after sexual abuse.
22. What are the long-term consequences for victims of childhood abuse?
Early identification of abuse and intervention in children’s lives is important and likely
increases the victim’s chances for a positive outcome. Prospective studies have shown lower
levels of educational achievement (42% of maltreated children finished high school, compared
to 66% of nonmaltreated children). Abused children are more likely to require special
education than nonabused children (24% vs. 14%). These associations remained after
adjustment for family and social differences. Not surprisingly, adult victims of childhood abuse
also held lower-skilled, lower-paying jobs as adults than did controls (62% vs. 45%).
Childhood abuse has significant consequences for childhood and adult mental health.
Abused children suffer from increased depression, anxiety, and behavior problems in
childhood. Depression in adulthood is more common among victims of childhood abuse; 25%
to 33% have major depression by their late twenties, based on Diagnostic and Statistical
Manual (DSM) criteria. They also have higher rates of post-traumatic stress disorder than
controls. Physical and sexual abuse are linked to twice the average risk for suicide attempt in
victims studied into their late twenties. Alcohol and possibly drug abuse are more common
among adult victims of childhood abuse.
Childhood abuse may ultimately affect adult physical health. Strong evidence suggests that
childhood physical abuse, sexual abuse, and neglect are linked to obesity in adulthood, even
adjusting for family and social factors. There may be increased rates of promiscuity, STDs,
teen pregnancy, and prostitution in adult victims of child sexual abuse. Chronic pain in
adulthood may be associated with childhood physical or sexual abuse, but further research is
needed. Clearly, childhood abuse has significant physical and emotional effects on survivors
and profound effects on society. More research is needed to study the effects of child neglect
(the most prevalent type of abuse) on adulthood.
23. What can we do to help childhood victims and prevent abuse?
Most physical injuries in young children heal well; outcome is determined, in large part, by the
social management of children in abusive homes. The primary responsibility of physicians
Chapter 65 ED EVALUATION OF CHILD ABUSE 459
suspecting abuse is to report it and to arrange for safe disposition. It is perfectly acceptable
(and in fact, imperative) to admit the child, if no safe disposition can be arranged in the
community.
ED providers have critical opportunities to educate families about infant behavior and
potentially prevent future child abuse. A provider who explains normal infant crying patterns
and coping strategies to the family of a colicky infant may protect that infant from abuse.
Giving families encouragement and reassurance that their child’s behavior is normal and age-
appropriate can help decrease caregivers’ frustration and improve their coping skills. Finally,
national and local campaigns to educate families about crying behavior in infants may help
decrease the chance that a frustrated caregiver will injure a child. Even in a busy ED, providers
can, in a short conversation with families, alter the life of a child by either preventing abuse or
recognizing it and responding accordingly.
BIBLIOGRAPHY
1. Gilbert R, Widom CS, Browne K, et al: Burden and consequences of child maltreatment in high-income
countries. Lancet 373:68–81, 2009.
2. Hansen KK, Prince JS, Nixon GW: Oblique chest views as a routine part of skeletal surveys performed for
possible physical abuse-is this practice worthwhile? Child Abuse Negl 32:155–159, 2008.
3. Ingram JD, Connell J, Hay TC, et al: Oblique radiographs of the chest in nonaccidental trauma. Emerg Radiol
7:42–46, 2000.
4. Jenny C, Hymel KP, Ritzen A, et al: Analysis of missed cases of abusive head trauma. JAMA 281(7):621–626,
1999.
5. Langlois NE, Gresham GA: The ageing of bruises: a review and study of the colour changes with time.
Forensic Sci Int 50(2):227–238, 1991.
6. Laskey AL, Holsti M, Runyan DK, et al: Occult head trauma in young suspected victims of physical abuse.
J Pediatr 144(6):719–722, 2004.
7. Maguire S, Mann MK, Sibert J, et al: Can you age bruises accurately in children? A systematic review. Arch
Dis Child 90(2):187–189, 2005.
8. Newton AW, Vandeven AM: Update on child maltreatment with a special focus on shaken baby syndrome.
Curr Opin Pediatr 17:246–251, 2005.
9. Sapp M, Vandeven A: Update on child sexual abuse. Curr Opin Pediatr 17:258–264, 2005.
10. U.S. Department of Health and Human Services, Administration on Children, Youth, and Families. Child
Maltreatment 2007. Washington, DC: U.S. Government Printing Office, 2009.
WEBSITE
http://www.childwelfare.gov/index.cfm
SUGGESTED REFERENCES FOR FURTHER READING
11. Christian CW, Block R, and the Committee on Child Abuse and Neglect: American Academy of Pediatrics
Policy Statement: Abusive Head Trauma in Infants and Children. Pediatrics 123:1409–1411, 2009.
12. Kellogg N and the Committee on Child Abuse and Neglect: American Academy of Pediatrics Policy Statement:
The Evaluation of Sexual Abuse in Children. Pediatrics 116: 506–512, 2005.
460
PROCEDURAL SEDATION AND ANALGESIA
OF THE PEDIATRIC PATIENT
CHAPTER 66
Joe E.Wathen, MD, and Guy Upshaw, MD
1. Why is it called procedural sedation and analgesia or (PSA)?
What used to be called conscious sedation is now more accurately referred to as PSA. This
is defined as using sedatives, dissociative agents, and analgesics alone or in combinations
to assist patients in tolerating unpleasant procedures, while maintaining cardiorespiratory
function. An analgesic treats pain, whereas a sedative or anxiolytic relieves fear and
anxiety. Some analgesics, particularly narcotics, have sedative and analgesic properties,
which make them useful in certain procedures. If a procedure is painful and frightening
(e.g., chest tube insertion, fracture reduction), the child would benefit from both sedation
and analgesia.
2. Do I need sedation and analgesia when performing procedures on children?
Children undergoing frightening or painful procedures would benefit from agents providing
sedation or analgesia. These procedures include reduction of fractures or dislocations,
laceration repair, incision and drainage of abscesses, burn care, examinations after sexual
assault, and diagnostic procedures such as lumbar puncture, computed tomography (CT), or
magnetic resonance imaging (MRI). Systemic sedatives or analgesics may not be needed in
some older children who can remain calm and where local anesthetics provide adequate pain
control. A comforting staff or family member may be the needed calming ingredient. Many
EDs have also employed child life advocates for this very purpose.
KEY POINTS: WHY PROVIDE PROCEDURAL SEDATION AND
ANALGESIA TO CHILDREN?
1. Relieve fear and anxiety.
2. Provide analgesia as needed.
3. Provide amnesia for an unpleasant procedure.
4. Facilitate optimal outcome of the procedure.
5. Provide a standard of care now expected and appreciated by most parents.
3. What is brutaine and should I use it?
Brutaine, or simply holding a child down without medications to perform a procedure,
although tempting as a fast approach, is not ideal. Using sedation and analgesia helps prevent
or reduce crying and thrashing. Not only does PSA allow the provider to have a better chance
of actually performing the procedure, but it also provides pain control, reduces anxiety, and in
some cases results in amnesia for the event. Continuous crying leaves the child, family, and
staff exhausted and appears to onlookers as torture. Sometimes, the addition of a sheet wrap
or papoose in combination with sedation is needed. The ability to provide PSA for children is
an accepted and expected part of emergency medicine.

Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT 461
4. What are the different levels of sedation?
n
Mild sedation or anxiolysis refers to very little to no depression of level of consciousness
(LOC). This is the ideal level for procedural sedation in the older child where anxiolysis
alone is needed.
n
Moderate sedation/analgesia, previously considered conscious sedation, is a drug-induced
depressed LOC where patients respond to verbal or tactile stimulation while protecting their
airway reflexes. The child is still awake but with droopy eyes and slurred speech. Only
minimally painful procedures will be tolerated with this level of sedation (i.e., suture repair).
n
Deep sedation/analgesia implies a depressed LOC from which the child is not easily
aroused and may need airway and ventilatory assistance. This level may be needed for
more painful procedures (i.e., fracture reduction).
n
General anesthesia represents the end of this continuum, which many sedatives can
achieve if given in sufficient doses. This is not desirable because of the risk of
cardiorespiratory depression, loss of airway reflexes, and aspiration.
5. List the ideal characteristics of an agent used for PSA?
n
Produces effective anxiolysis, even during painful procedures
n
Is safe; produces a predictable degree of sedation for a given dose and has minimal effects
on airway reflexes and cardiorespiratory status
n
Minimizes movement, facilitating an optimal procedure
n
Provides amnesia for the procedure
n
Produces no adverse interactions with other agents that may be used concurrently
n
Is reversible
n
Can be administered painlessly
n
Is titratable (advantage of intravenous [IV] administration)
n
Has rapid onset, short duration, and rapid recovery (most important)
6. What routes of administration are available for administrating a sedative?
There are several potential routes available for administration of PSA. The route can parallel
the depth of sedation needed and the type of procedure to be performed. Routes include
oral, transmucosal (i.e., nasal, oral mucosal, rectal), intramuscular (IM), intravascular, or
inhalational. IV and inhalational routes allow for the important quality of titrating to effect.
However, it may be difficult in some pediatric patients to obtain IV access. In those cases
where moderate or deep sedation is needed, the intramuscular route may be ideal (e.g., IM
ketamine). Likewise, if anxiolysis or mild sedation is needed, oral or nasal midazolam may
be sufficient.
7. What are the key items to ask in the medical history prior to PSA?
n
When was the last oral intake of liquids and solids? (aspiration risk)
n
Are there allergies to any sedative or analgesic agents?
n
What are the current medications? Will there be any interactions?
n
Have recent medications (e.g., narcotics) been given? (additive effect)
n
Any chronic medical problems (e.g., chronic lung disease or airway abnormalities)?
n
Prior complications if received prior sedatives/analgesics or general anesthesia?
8. Are there guidelines for presedation fasting?
There are official guidelines for elective procedures per the American Society of
Anesthesiologists (ASA) guidelines. However, adherence to these presedation fasting
guidelines has not been shown to alter the rate of adverse events. Regarding emergency
medicine practice, the majority of ED procedures with indications for PSA are urgent or
emergent with variable prearrival fasting times. The American College of Emergency
Physicians (ACEP) consensus committee has offered clinical practice guidelines for these
ED PSA patients. They suggest targeting the depth and length of PSA based on the nature
of oral intake 3 hours prior to the procedure, balancing the patient risk factors and the
urgency of the procedure.

Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT462
For truly emergent procedures, the ACEP consensus committee advisory “permits all
levels of procedural sedation and analgesia regardless of fasting status or underlying patient
risk factors.”
9. What physical examination findings are important to note prior to PSA?
n
Items to note are the presence of airway abnormalities such as large tonsils or adenoids,
congenital abnormalities that may have a floppy or anatomically susceptible airway (Down
syndrome, Pierre Robin syndrome, Treacher-Collins syndrome) or lower respiratory
findings such as wheezing and rales.
n
Obese children may have associated sleep apnea and be at increased risk of adverse
respiratory event.
n
A visual inspection of the open mouth will tell you what the upper airway looks like
(Mallampatti score) and will remind you to look for loose teeth or dental hardware (retainers).
n
A careful cardiac and neurologic exam should also be performed.
10. Are there any children who should not receive PSA?
Relative contraindications to procedural sedation in the ED relate to the risk of complications,
including aspiration and potential difficulty in managing the airway. Children who may be
better candidates for operating room procedures under more controlled conditions include:
n
Unstable patients (children with abnormal mental status or hemodynamic instability)
n
Infants younger than 6 months old
n
Children with craniofacial malformations, such as Pierre-Robin syndrome
n
Children with cerebral palsy (abnormal swallowing mechanisms)
n
Children with snoring, stridor, apnea, or abnormal breathing regulation
n
Children with seizure disorders
n
Children with vomiting or gastroesophageal reflux
n
Children with severe systemic disease
11. What is the monitoring that should occur with PSA?
The level of monitoring can parallel the degree of sedation. The best monitor is a skilled,
dedicated observer who is not involved in the procedure and who can observe the child’s level
of consciousness, response to verbal and physical stimulation, airway patency, respiratory
function, and perfusion. Sedated children should not be left unobserved.
Monitoring and resuscitation equipment may include: cardiorespiratory monitor, pulse
oximetry, capnography, blood pressure cuff, suctioning equipment, proper-sized bag-mask
ventilation connected to oxygen source, and proper-sized advance airway equipment
(i.e., endotracheal tubes and laryngoscope).
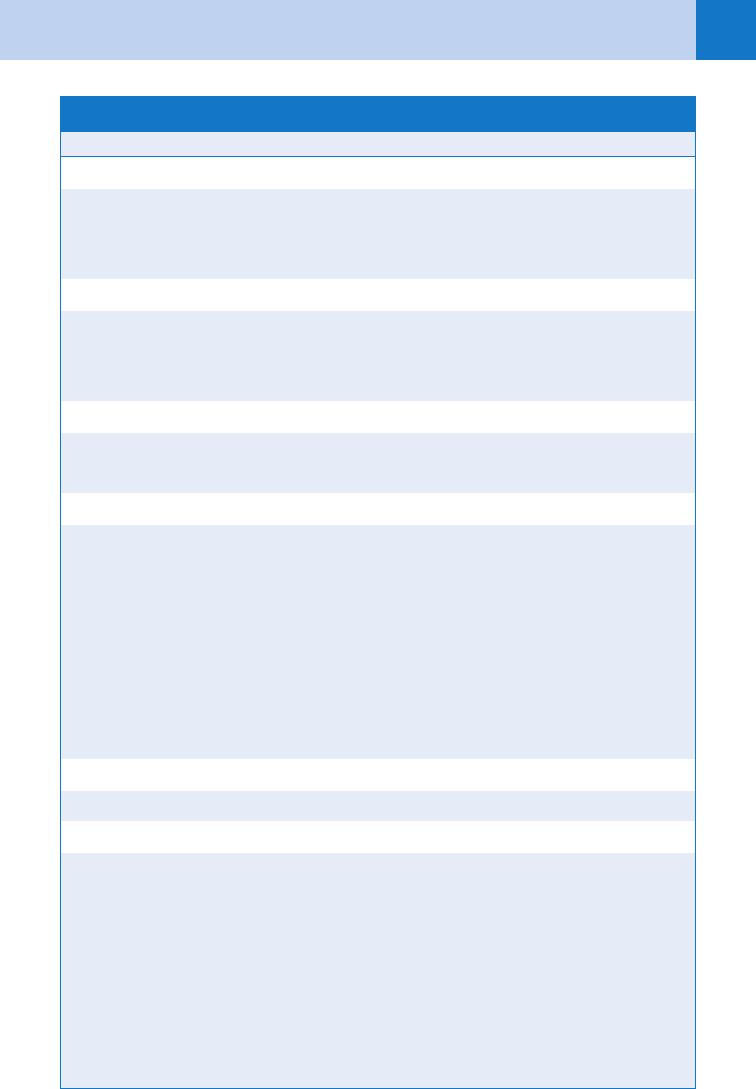
12. What are the agents used for pediatric PSA?
See Table 66-1.
13. What agents would you use if you needed to obtain a CT scan on a young
child?
Radiologic diagnostic procedures are common and may prove to be difficult to achieve
without adequate sedation. The newer CT scanners however, are faster diagnostic procedures
with the possibility of being performed without sedatives. If medications are needed, sedatives
alone are usually adequate. Potential agents include pentobarbital (Nembutal), midazolam,
methohexital, or etomidate. Pentobarbital has been shown to more effectively sedate a child
for radiologic imaging (97%) versus midazolam (19%).
14. Would the agents used for obtaining a CT scan work for an MRI?
MRIs are not particularly rapid events, so the child must remain motionless for a longer time
period. The ultrashort-acting sedatives would not be the best choice. Instead, agents that can
either be continuously infused (propofol) or have a longer duration of action (chloral hydrate)
would be preferred.
Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT 463
ETT, endotracheal tube; IM, intramuscularly; IN, intranasally; IV, intravenously; PO, by mouth; PR, per rectum.
*Can be given as a continuous infusion: 25–150 mg/kg/minute or in additional boluses of 0.5 mg/kg IV every
3 minutes as needed
Agent Dose Route Comment
Anxiolytics
Midazolam 0.1 mg/kg IV, IM Titrate to effect
0.3 mg/kg IN
0.5 mg/kg PO, PR 15 mg max
Sedative Analgesics
Fentanyl 1–3 mg/kg IV Avoid rapid or high-dose infusion
Morphine 0.1 mg/kg IV, IM
Meperidine 1.0 mg/kg IV, IM
Dissociative Agents
Ketamine 1–2 mg/kg IV Give intravenous dose over 1–2 min
2–4 mg/kg IM Longer recovery
Pure Sedatives
Pentobarbital 4–6 mg/kg IM
2–4 mg/kg IV
Etomidate 0.1–0.2 mg/kg IV Ultrashort
Propofol 0.5–1.0 mg/kg* IV Rapid onset and offset
Methohexital 1 mg/kg IV Ultrashort, limited studies
20–30 mg/kg PR
Chloral
Hydrate
50 mg/kg PO,PR Unpredictable effect, long duration,
avoid in newborns
Inhalational agents
Nitrous oxide 30%–50% NO
2
Inhalation Older children, able to hold mask
Reversal Agents
Naloxone 0.01 mg/kg fol-
lowed by 0.1
mg/kg if first
dose ineffective
IV, IM, ETT Can repeat every 5 min, 4 mg max
Flumazenil 0.01 mg/kg IV Titrate to max of 1.0 mg
TABLE 66-1. PROCEDURAL SEDATION AND ANALGESIA AGENTS

Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT464
15. What are the advantages and disadvantages of propofol for PSA?
Advantages Disadvantages
Sedative hypnotic qualities Risk of apnea
Rapid onset and offset Hypoxia-hypoventilation, 2% to 31%
High efficacy Dose-related hypotension
Amnesia Lipophilic suspension 5 pain at injection
Constant infusion for longer procedures Needs opiate for painful procedures
Contraindicated with egg or soy allergy
16. What medications would you use for a 2-year-old with a facial laceration?
For the majority of patients, local anesthetics such as topical lidocaine, epinephrine, tetracaine
(LET) or local injection with lidocaine is sufficient. The difficulty becomes reducing the child’s
anxiety. Effective sedation can be provided with midazolam, administered intravenously,
intranasal, or orally. When this does not provide adequate sedation and motion control for a
difficult repair (i.e., laceration crossing the vermillion border of the lip), an agent such as
ketamine either intravenously or intramuscularly works well.
17. What medications would you consider for a 6-year-old needing reduction of
an angulated forearm fracture?
Fracture reduction is associated with significant pain and anxiety. Both need to be treated.
Several options can be effective and include the following: fentanyl or morphine plus
midazolam, ketamine, propofol plus an opiate, or nitrous oxide with a hematoma block.
Ketamine has been shown to have fewer adverse respiratory events when compared to fentanyl
and midazolam.
18. What makes ketamine or kidamine useful as a PSA agent?
Ketamine, a dissociative agent causing a trancelike cataleptic state, has become a more
commonly used medication for pediatric PSA. It provides strong sedation, analgesia, and
amnesia while maintaining cardiovascular stability and protective airway reflexes. Ketamine
onset is within a couple of minutes intravenously and 5 to 10 minutes intramuscularly.
Because ketamine can increase salivation, coadministration with an antisialogogue such as
atropine was previously advised, however recent studies suggest this is unnecessary, with no
increase in adverse airway effects. Coadministration of midazolam has not been shown to
decrease recovery agitation or emergent phenomena (vivid dreams, hallucinations, delirium),
but can decrease recovery emesis, which occurs in 15% to 20%. Ondansetron has also been
shown to reduce recovery emesis associated with ketamine. Ketamine, although protective of
airway reflexes, may be associated with hypoxia in approximately 5%, and rarely
laryngospasm or apnea (,1%).
19. What are the contraindications for ketamine?
Glaucoma or globe injury, increased intracranial pressure (ICP) or central nervous system
(CNS) mass lesion, seizure disorder, hypertension, congestive heart failure, major psychiatric
disorder, porphyria, previous adverse reaction, procedures or conditions that can exacerbate
laryngospasm (pharyngeal procedures, endoscopy, upper respiratory infections), or age
younger than 3 months.
20. What complications are seen with PSA?
With oversedation, there is risk for:
n
Respiratory events: aspiration (from vomiting and loss of airway reflexes), hypoventilation,
hypoxia, laryngospasm, and apnea
n
Cardiovascular events: hypotension, bradycardia
n
Vomiting
Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT 465
During the postsedation recovery period, children may vomit, become agitated, ataxic,
dysphoric, or manifest other emergence reactions. In addition, the chance of respiratory
depression is increased when the painful stimulus of the procedure is complete. Close
observation and parental reassurance is essential. Because of the risks involved, at least
verbal informed consent should be obtained and documented.
*Respiratory events included hypoxia, laryngospasm, and apnea
†
OR represents odds ratio.
Sedation Drugs Respiratory Events* (%, OR
†
) Vomiting (%, OR
†
)
Ketamine alone 6%, 1 10%, 1
Ketamine/Midazolam 10%, 1.7 5%, 0.5
Fentanyl/Midazolam 19%, 3.7 2%, 0.2
Midazolam alone 6%, 0.9 0.8%, 0.07
TABLE 66-2. ADVERSE EVENTS BY DRUG TYPE
KEY POINTS: HOW TO AVOID ADVERSE EVENTS WITH
PEDIATRIC PROCEDURAL SEDATION AND ANALGESIA
1. Beware of infants, children with systemic disease processes, obstructive airway disease,
severe obesity, or active respiratory infections.
2. Become acquainted and comfortable with PSA drug regimens.
3. Verify the weight is in kilograms, not pounds prior to dosing.
4. Monitor carefully, both with equipment and a dedicated medical staff per American Academy
of Pediatrics or ACEP guidelines.
5. Be attentive to the end of the procedure when the painful stimulus is over and the child is
more prone to developing respiratory depression.
6. Prior to starting PSA, have advanced airway equipment ready including suction, oxygen,
and proper-sized bag-valve mask.
21. What are the complications associated with fentanyl?
Fentanyl is a commonly used narcotic in the ED because it provides analgesia and sedation
with a rapid onset and recovery. However, a few reminders about fentanyl are important.
When fentanyl is given rapidly or in high doses, it can cause the rigid-chest syndrome
(thoracic and abdominal wall rigidity). This muscular rigidity can be reversed by naloxone
(Narcan) or with neuromuscular blockade. In addition, fentanyl can cause apnea without the
usual concomitant decrease in mental status. Full monitoring is essential, including frequent
blood pressure checks.
22. Are some agents safer than others?
Using proper monitoring, most agents can be utilized and adverse events promptly treated;
reversal agents are seldom needed. Certain drug types used are associated with different
adverse event profiles. See Table 66-2.
Chapter 66 PROCEDURAL SEDATION AND ANALGESIA OF THE PEDIATRIC PATIENT466
23. What reversal agents are available for children?
For narcotics and benzodiazepines, specific reversing agents are available. Naloxone (0.01 mg/
kg-0.1 mg/kg intravenously, intramuscularly, or endotracheal, up to 4 mg per dose) reverses
narcotic effects, and flumazenil (0.01 mg/kg intravenously, up to 1.0 mg) reverses
benzodiazepine overdose.
General measures: Discontinue sedative or narcotic administration. Maintain the airway
and provide assisted ventilation, initially with bag-valve-mask ventilation, then with
endotracheal intubation if necessary. If poor perfusion or shock is present (e.g., capillary refill
time .2 seconds, cool extremities, weak pulses, poor tone), obtain vascular access and
initiate treatment with a bolus infusion of 20 mL/kg of crystalloid solution.
24. When can I discharge a child home after performing PSA?
The child should have normal vital signs, be reasonably alert, able to sit without assistance,
tolerate liquids by mouth, and respond to commands given in a normal voice.
WEBSITE
Agency for Healthcare Research and Quality. National guideline clearinghouse:
http://www.guideline.gov
BIBLIOGRAPHY
1. Agrawal D, Manzi SF, Gupta R, et al: Preprocedural fasting state and adverse events in children undergoing
procedural sedation and analgesia in a pediatric emergency department. Ann Emerg Med 42:636–646, 2003.
2. Bassett KE, Anderson JL, Pribble CG: Propofol for procedural sedation in children in the emergency
department. Ann of Emerg Med 42:773–782, 2003.
3. Brown L, Christian-Kopp S, Sherwin TS, et al: Adjunctive atropine is unnecessary during ketamine sedation in
children. Acad Emerg Med 15:314–318, 2008.
4. Green SM, Krauss B: Clinical guideline for emergency department ketamine dissociative sedation in children.
Ann Emerg Med 44:5, 2004.
5. Green SM, Roback MG, Miner JR, et al: Fasting and emergency department procedural sedation and
analgesia: a consensus-based clinical practice advisory. Ann Emerg Med 2007. 49:454–461.
6. Mace SE, Barata IA, Cravero JP, et al: Clinical policy: evidence-based approach to pharmacologic agents used
in pediatric sedation and analgesia in the emergency department. Ann Emerg Med 44:4, 2004.
7. Miner JR, Burton JH: Clinical practice advisory: emergency department procedural sedation with propofol.
Ann Emerg Med 50:182–187, 2007.
8. Moro-Sutherland DM, Algren JT, Louis PT: Comparison of intravenous midazolam with pentobarbital for
sedation for head computed tomography imaging. Acad Emerg Med 7:1370-1375, 2000.
9. Roback MG, Bajaj L, Wathen JE, et al: Preprocedural fasting and adverse events in procedural sedation and
analgesia in a pediatric emergency department: are they related? Ann Emerg Med 44:5:454–459, 2004.
10. Roback MG, Wathen JE, Bajaj L, et al: Adverse events associated with procedural sedation and analgesia in a
pediatric emergency department: a comparison of common parenteral drugs. Acad Emerg Med 12:6:508–513,
2005.
11. Sacchetti A, Carraccio C, Giardino A, et al: Sedation for pediatric CT scanning: is radiology becoming a drug-
free zone? Pediatr Emerg Care 21(5):295–297, 2005.
467
PEDIATRIC AND NEONATAL RESUSCITATION
CHAPTER 67
Katherine M. Bakes, MD
1. What is the pediatric assessment triangle?
The pediatric assessment triangle is a quick tool used to assess small children for end-organ
perfusion. The three points of the triangle are work of breathing, general appearance, and
circulation to the skin. This provides a rapid way to assess a child in less than a minute,
thereby enabling the provider to determine physiologic status with regard to oxygenation,
ventilation, perfusion, and brain function.
2. How do I prepare myself for a pediatric arrest coming to the ED?
n
Know your equipment. If you use it, review the Broselow tape frequently.
n
Be familiar with your difficult airway equipment for children and consider scenarios for use.
n
Keep a list of equipment that should be stocked and regularly checked in the event of a
pediatric arrest.
Finally, have scheduled mock pediatric resuscitations in your department so that you can
identify needed equipment, medications, and process impediments. Resuscitation of a child
requires a team effort, wherein everyone needs to be aware of the resources available and
specific age- and weight-based needs.
3. Is survival rate after cardiopulmonary arrest better in children or adults?
Due to inconsistencies in terminology, estimating exact survival after cardiac arrest in children
has been difficult. Investigators who have studied the two populations in parallel have shown
a slightly better predicated survival for adults after out-of-hospital cardiopulmonary arrest.
Survival to hospital discharge rates for pediatric arrests range from 2% to 12%, with
neurologically intact survival at approximately 2%. These poor outcomes can be explained by
the irreversible etiologies of pediatric arrests. Underlying causes of pediatric arrests can be
divided into age groups: leading causes of death in children younger than 1 year of age
include congenital anomalies, sudden infant death syndrome and sepsis; trauma and
respiratory infections leading to sepsis top the causes in children older than 1 year of age.
Although outcomes are poor, overall fewer children arrest.
4. What are predictors of outcome in pediatric arrest?
Predictors of mortality include:
n
Age younger than 1 year
n
Bradyasystolic rhythms
n
Need for epinephrine administration and greater than 15 minutes of cardiopulmonary
resuscitation (CPR)
A pediatric respiratory arrest with a pulse has an estimated 75% chance of survival, whereas a
pediatric patient in pulseless arrest has an estimated survival of 2% to 12%.
5. What are the fundamental differences between the pediatric versus the adult
airway?
The pediatric airway is relatively more anterior and cephalad, as well as more malleable due to
underdeveloped cartilage and supporting structures. These features make the pediatric airway
very susceptible to kinking with flexion and extension maneuvers, a feature the physician
should be aware of for proper airway positioning. The younger the child, the more submental