Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 28 • Total Gastrectomy 309
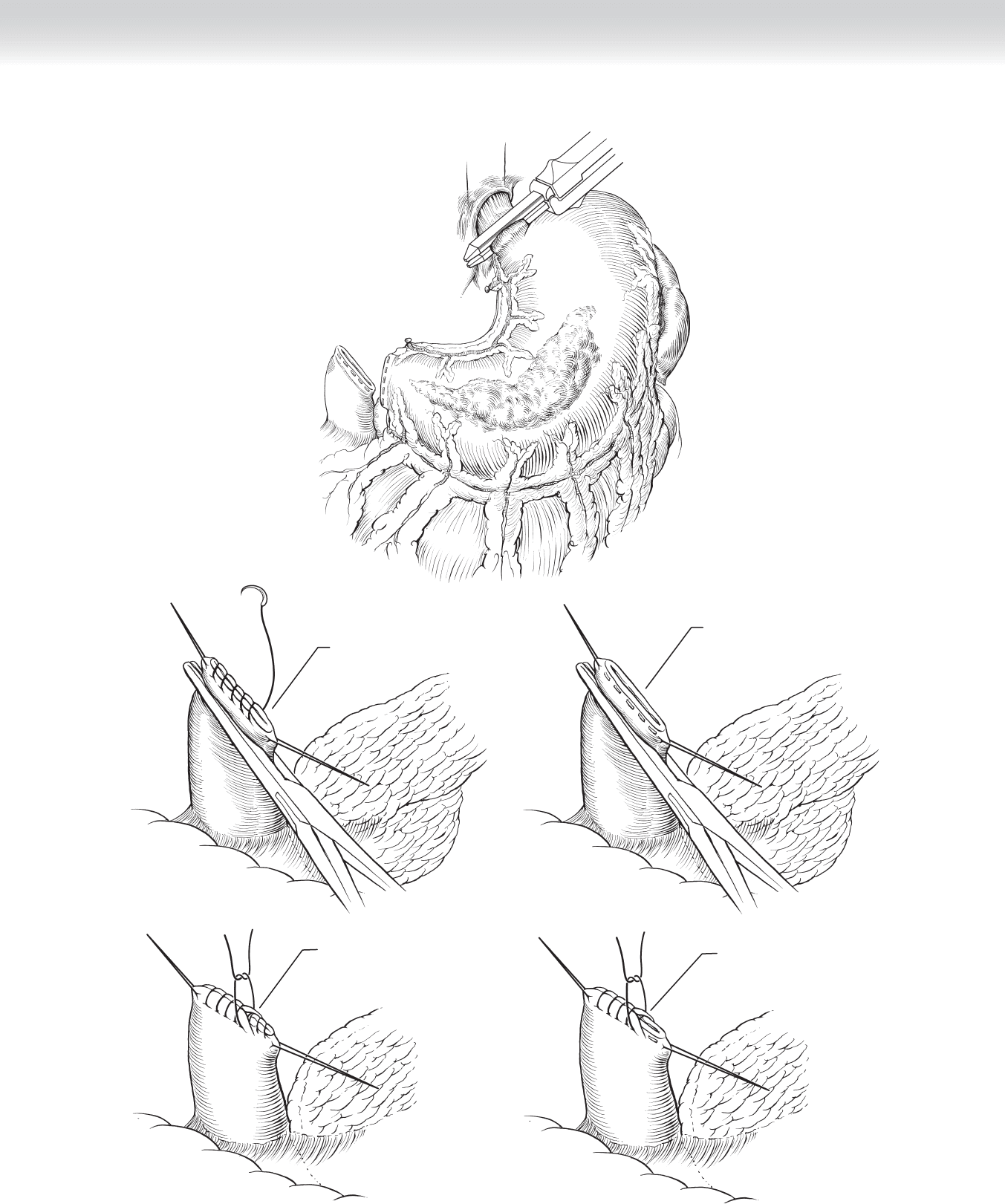
A
Suture closure
B
Staple closure
C
E
Interrupted suture
over stapled closure
D
Interrupted suture
over first row of
running sutures
FIGURE 28–8
310 Section IV • The Abdomen
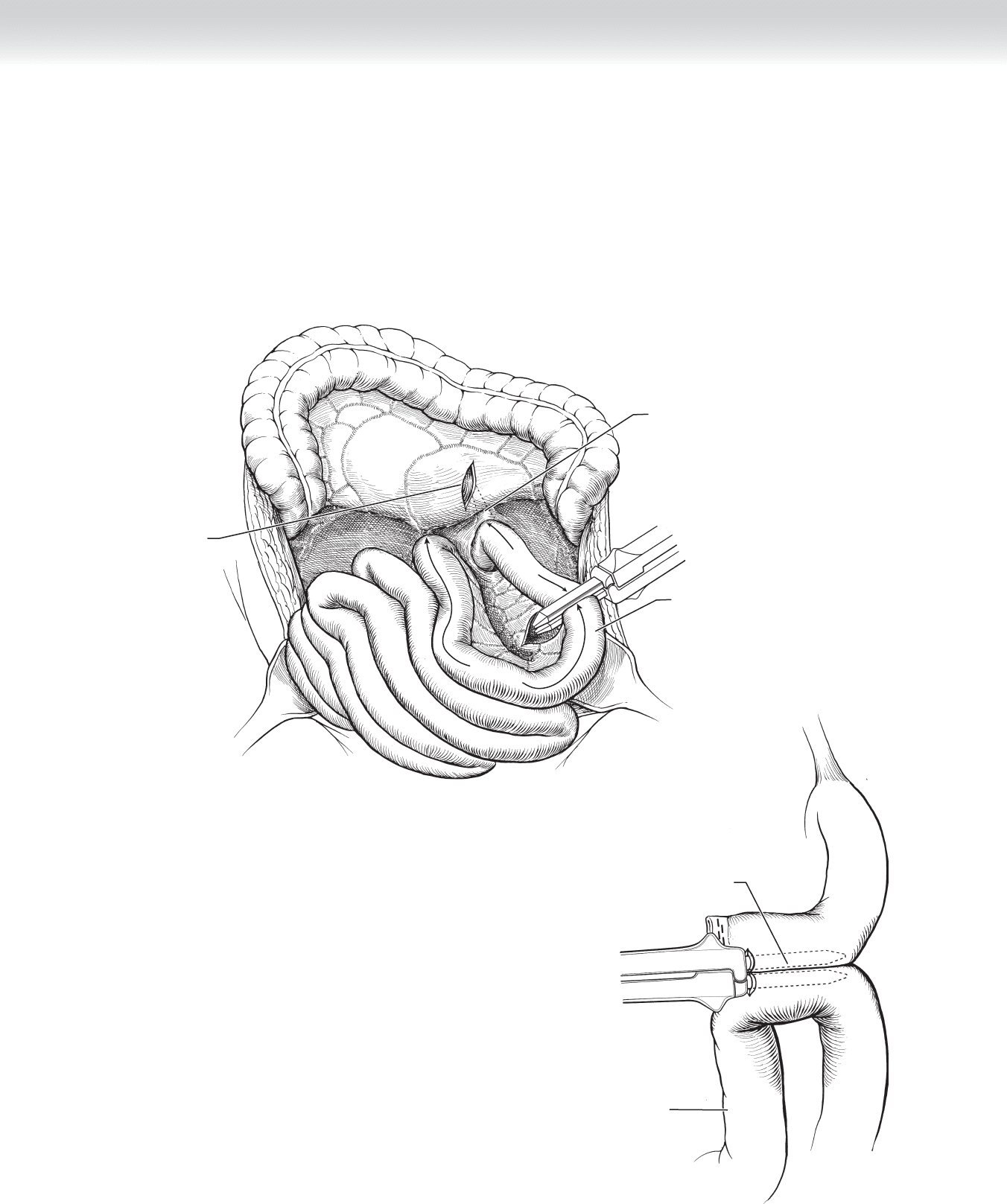
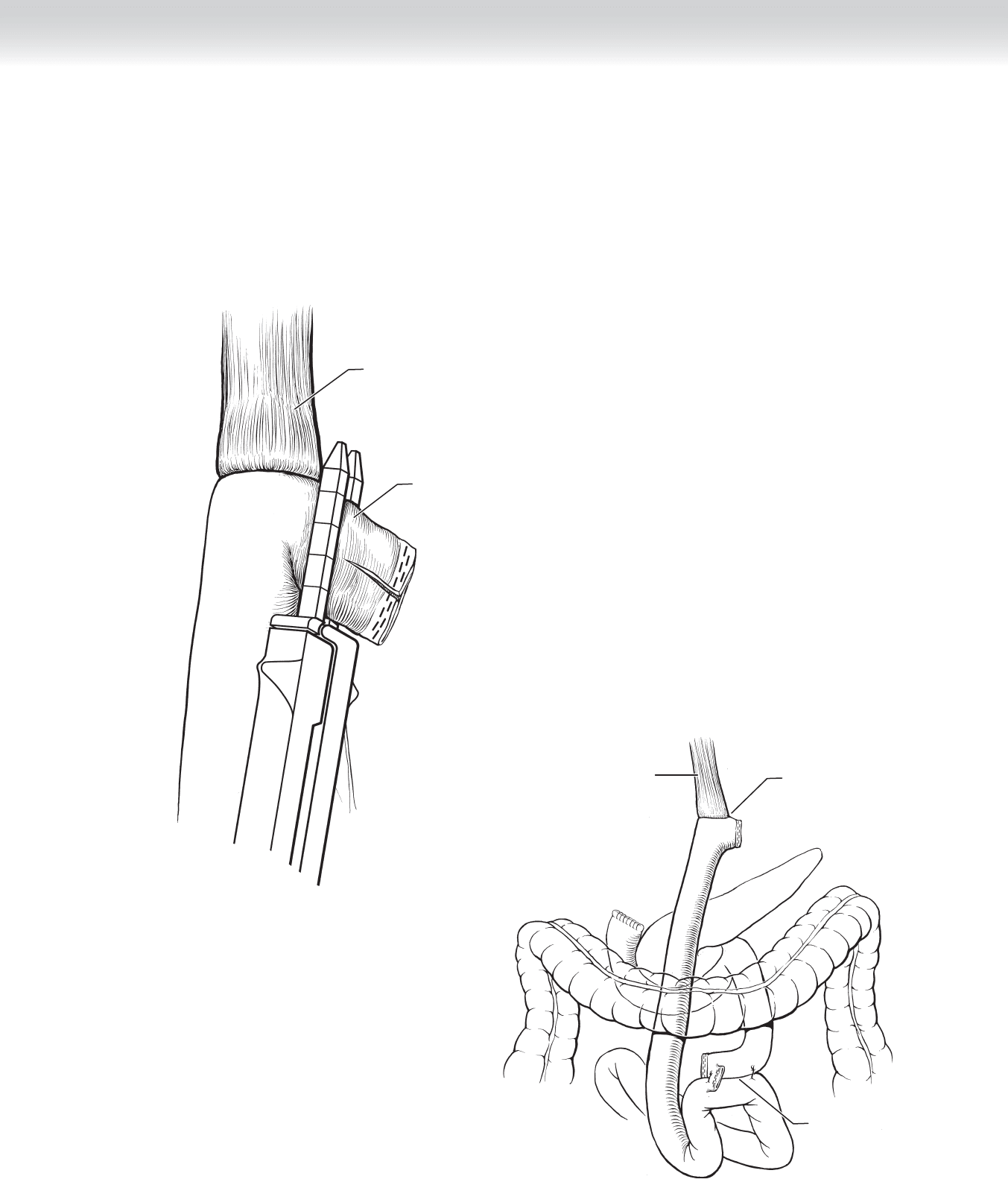
◆ An opening is made in the mesocolon, taking care to not damage any vessels running in
the mesocolon. The jejunum is then divided approximately 30 cm from the ligament of
Treitz using the GIA device, and a Roux limb of approximately 40 to 50 cm is created
(Figure 28-9).
◆ Figure 28-10 demonstrates creation of the jejunojejunal anastomosis using the GIA device.
Roux limb
Creating a
jejunojejunostomy
anastomosis
FIGURE 28–10
FIGURE 28–9
Opening created
in mesocolon
Roux limb
Ligament of Treitz
3
0
c
m
4
0
-
5
0
c
m
CHAPTER 28 • Total Gastrectomy 311
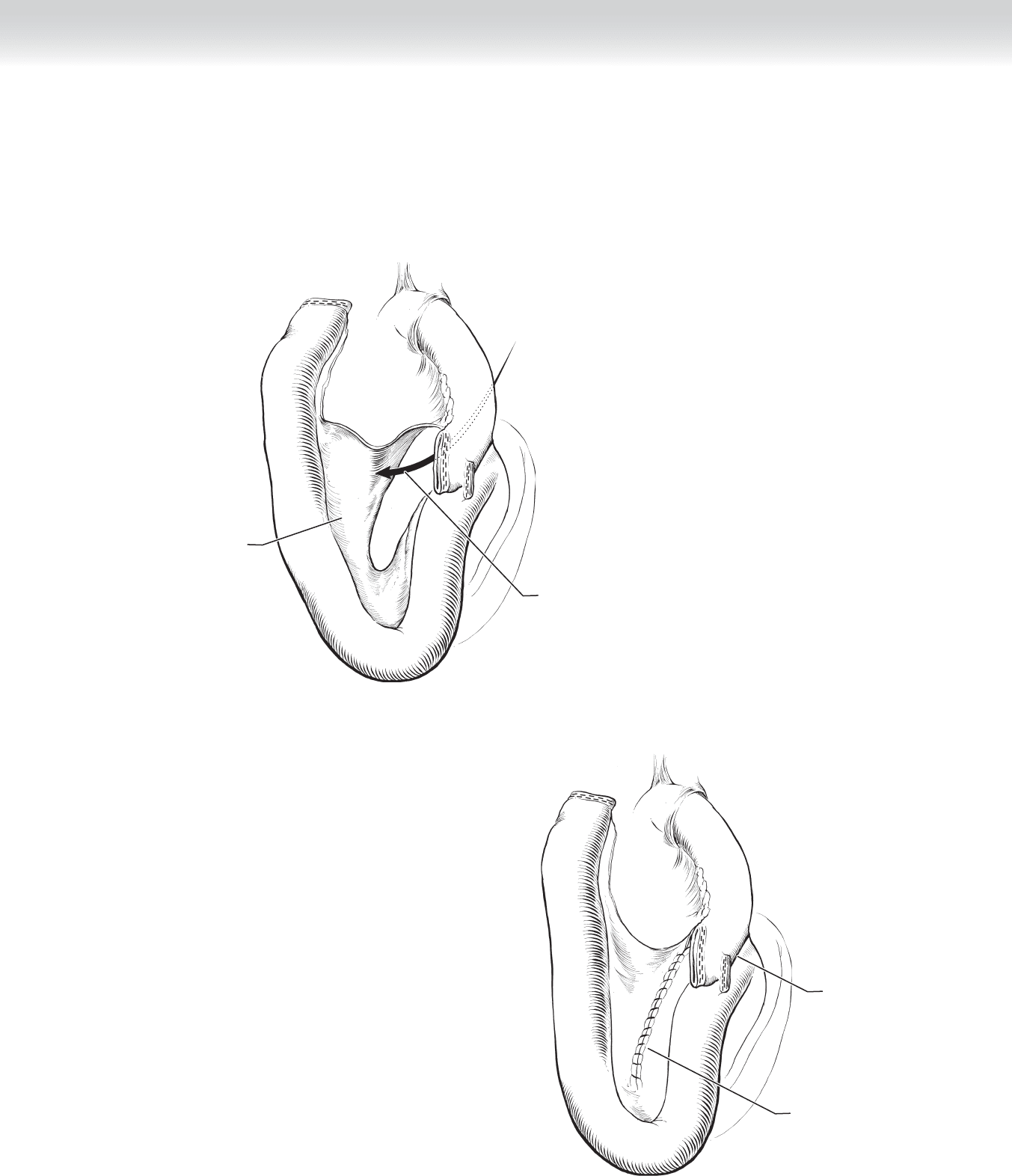
◆ The mesenteric rent that was created is now closed using a running (Figure 28-11, A) or
interrupted suture (Figure 28-11, B).
Arrow going through
mesenteric defect
Mesentery
to be closed
∗
∗
A
B
B
Closure of
mesenteric defect
Anastomosis
complete
∗
∗
FIGURE 28–11
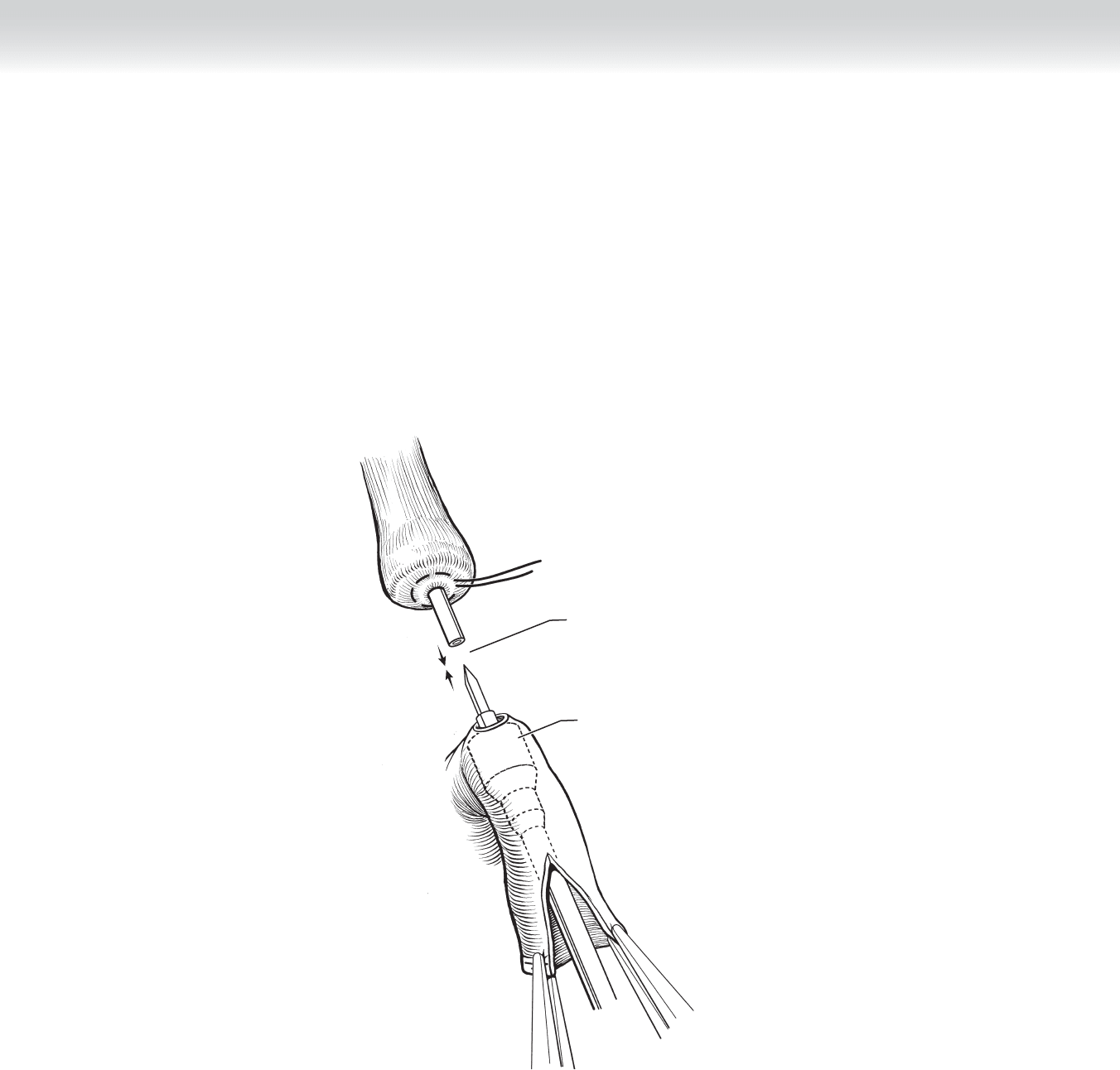
◆ Stay sutures are placed on the free end of the jejunum and the jejunum is opened adjacent
to the staple line. The end-to-end anastomosis (EEA) stapling device (without the anvil) is
placed into the lumen of the free end of the jejunum. A point is selected approximately 4 to
5 cm from the free margin. The post on the EEA stapling device is extended and brought
through the wall of the jejunum. Stay sutures are also placed on the distal esophagus,
which is then opened and the anvil placed into the distal esophagus. A purse-string suture
is then used to secure the anvil. The anvil is then placed into the post of the circular stapler
and the tissue is approximated. Firing of the EEA stapler places a circular double ring of
staples and extends a circular knife that excises the rings of the jejunum and esophagus
inside the circle of staples (Figure 28-12).
Mating together
circular stapler
and anvil
Circular stapler
FIGURE 28–12
Section IV • The Abdomen312
◆ The redundant section of jejunum is then excised using a GIA stapling device. This converts
the anastomosis functionally into an end-to-end esophagojejunostomy (Figure 28-13).
◆ Figure 28-14 demonstrates the completed esophagojejunal anastomosis with the Roux limb
positioned in a retrocolic fashion.
Cutting away
jejunal excess
Esophagus
FIGURE 28–13
Esophagojejunal
anastomosis
Jejunojejunum
anastomosis
Esophagus
Retrocolic
FIGURE 28–14
CHAPTER 28 • Total Gastrectomy 313

314 Section IV • The Abdomen
3. CLOSING
◆ The midline or bilateral subcostal incisions are closed in the usual fashion.
STEP 4: POSTOPERATIVE CARE
◆ A nasogastric tube is positioned in the esophagus just proximal to the anastomosis. Once
bowel function has resumed, oral feedings can be instituted when there is assurance that no
anastomotic leak has occurred. Some surgeons prefer to perform a contrast study using
water-soluble dye to ensure no leakage.
◆ Postgastrectomy patients require frequent small feedings. Adequate calorie intake may be
problematic in the initial postoperative period.
◆ In addition, supplemental vitamin B
12
is required at routine intervals.
STEP 5: PEARLS AND PITFALLS
◆ The use of the EEA stapling device has greatly simplifi ed performing the esophagojejunal
anastomosis.
◆ A Roux limb of 40 to 50 cm should be used to prevent complications of refl ux into the
Roux limb affecting the esophagojejunal anastomosis.
SELECTED REFERENCES
1. Mercer DW, Robinson EK: Stomach. In Townsend CM Jr (ed): Sabiston Textbook of Surgery: The Biological
Basis of Modern Surgical Practice, 18th ed. Philadelphia, Saunders, 2008, pp 1223-1277.
2. Thompson JC: Total gastrectomy. In Thompson JC (ed): Atlas of Surgery of the Stomach, Duodenum and
Small Bowel. St Louis, Mosby-Year Book, 1992, pp 153-165.
315
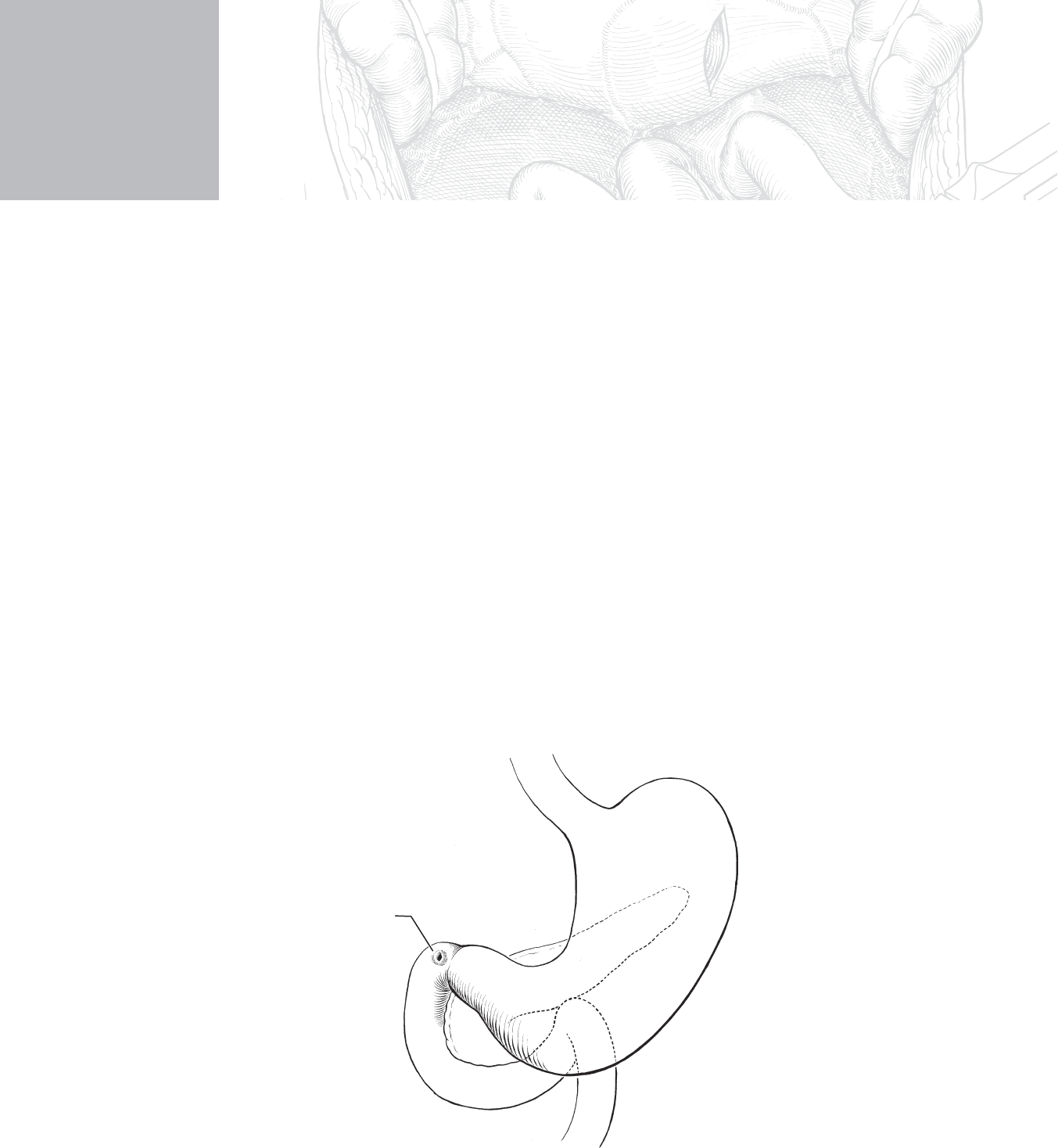
STEP 1: SURGICAL ANATOMY
◆ The usual site for a perforated peptic ulcer is anterior in the fi rst portion of the duodenum
just distal to the pylorus (Figure 29-1).
◆ Patients with perforated peptic ulcers can be approached by either the standard open tech-
nique or laparoscopically.
CHAPTER
29
Open and Laparoscopic Closure
of Perforated Peptic Ulcer
B. Mark Evers
MC
Peptic ulcer
FIGURE 29–1

STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The patient should be adequately hydrated before operation, and broad-spectrum antibiot-
ics should be initiated in the preoperative period.
◆ Consideration should be given as to whether to perform simple closure of the perforation
or to perform a more defi nitive operation if the patient has a history of chronic duodenal
ulcer disease.
◆ However, with current medical regimens including drugs to eradicate Helicobacter pylori,
the need to perform a more defi nitive ulcer operation at the time of closure of the perfora-
tion has greatly diminished.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ If an open repair of a perforated ulcer is to be performed, this can be accomplished via an
upper middle incision, which can be extended inferior to the umbilicus if necessary.
2. DISSECTION
Open:
◆ Upon entering the abdomen, the surgeon should locate the perforation. As stated previ-
ously, perforated peptic ulcers are routinely located anteriorly in the fi rst portion of the
duodenum (Figure 29-2, A).
◆ The abdomen should be copiously irrigated with warm saline, and, for a standard Graham
closure, interrupted 3-0 silk sutures are placed in Lembert fashion across the ulcer
(Figure 29-2, B).
Section IV • The Abdomen316
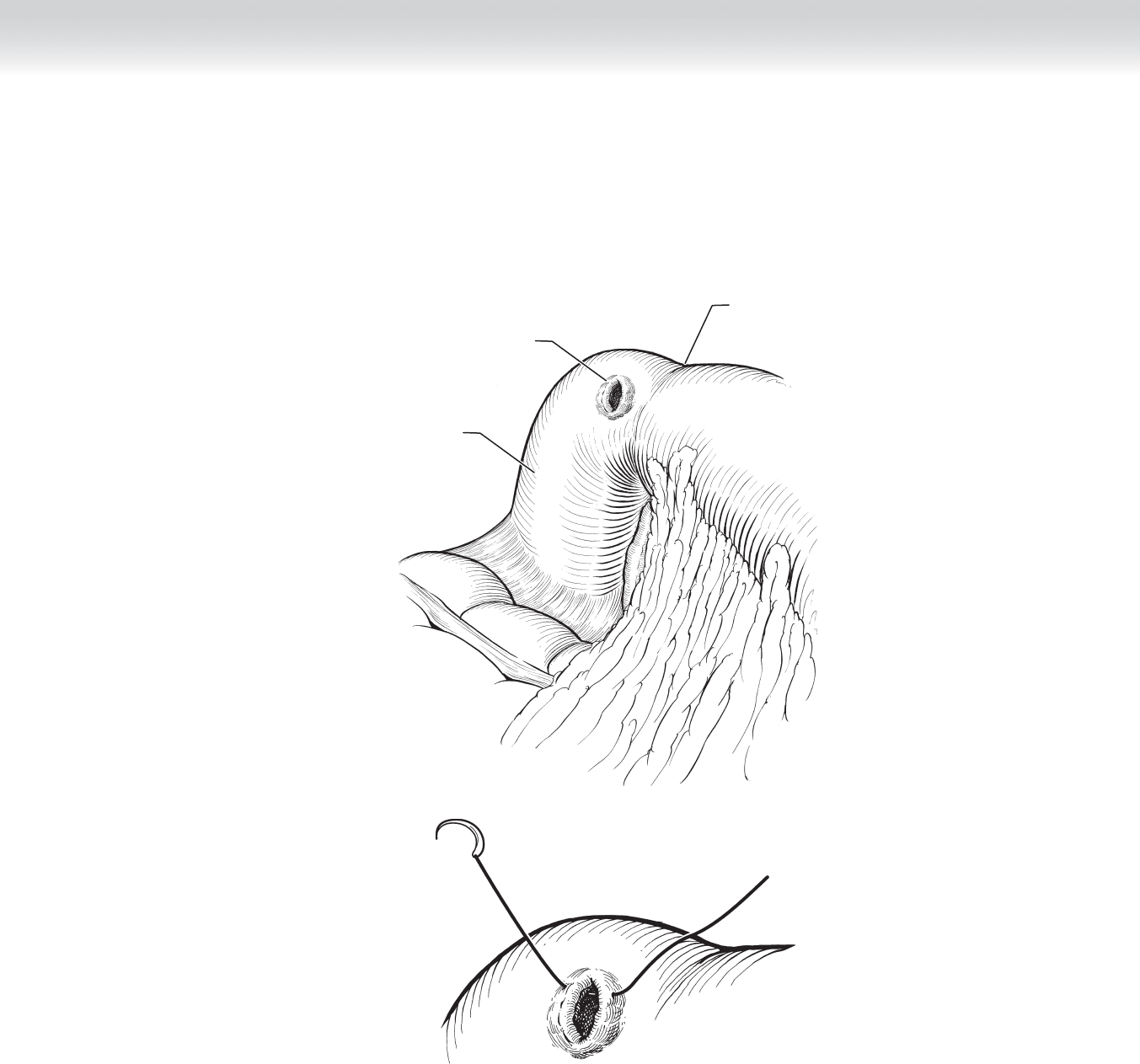
Pylorus
Peptic ulcer
Duodenum
A
B
FIGURE 29–2
CHAPTER 29 • Open and Laparoscopic Closure of Perforated Peptic Ulcer 317
318 Section IV • The Abdomen
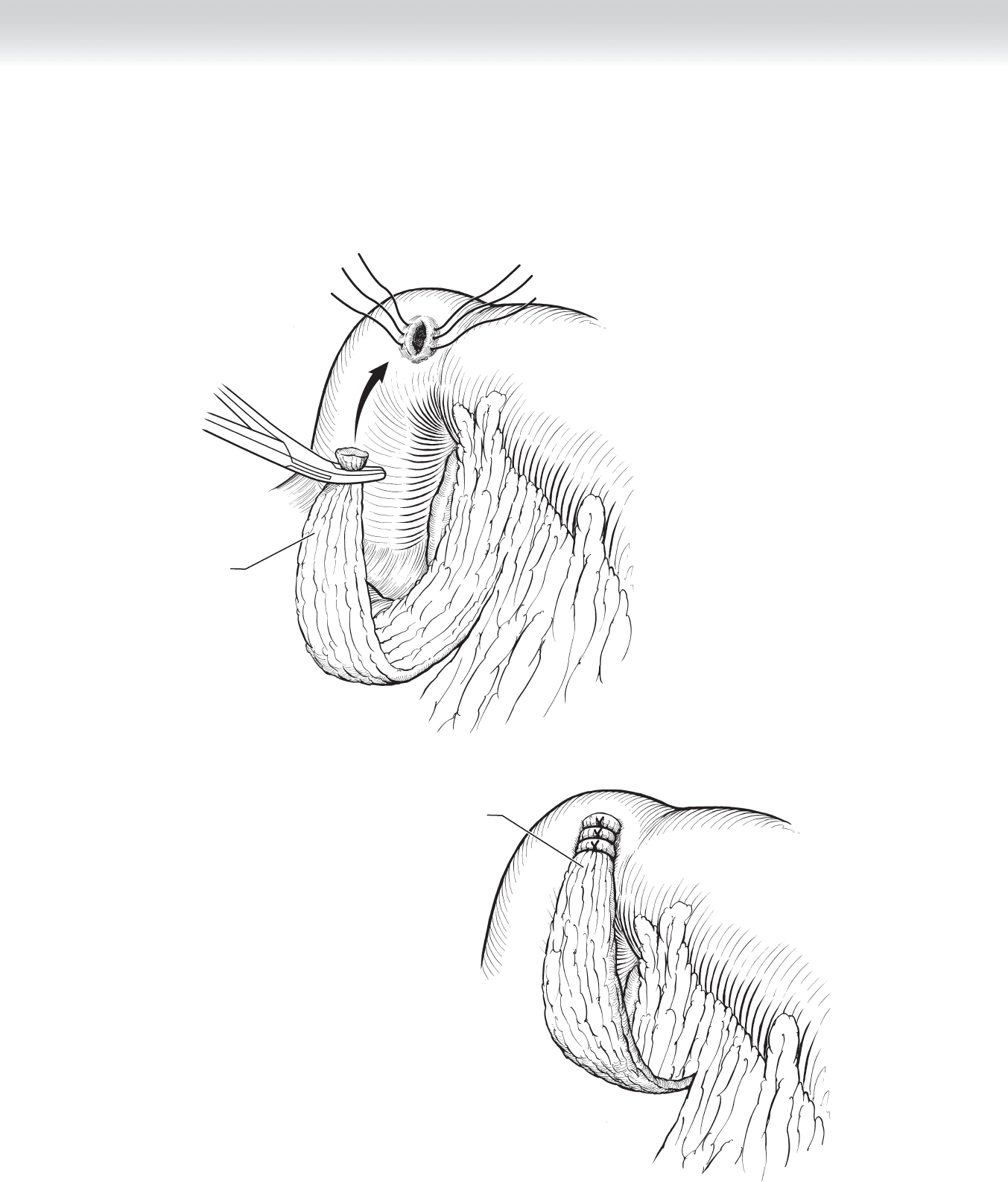
◆ Once the sutures are in place, a pedicle of omentum is placed across the base of the ulcer
(Figure 29-3). The sutures are then tied over the omental pedicle, thus sealing the perfora-
tion (Figure 29-4).
Omentum to be used
to plug inside of
perforated ulcer
FIGURE 29–3
Omentum secured
over ulcer
FIGURE 29–4