Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 32 • Gastrojejunostomy 339
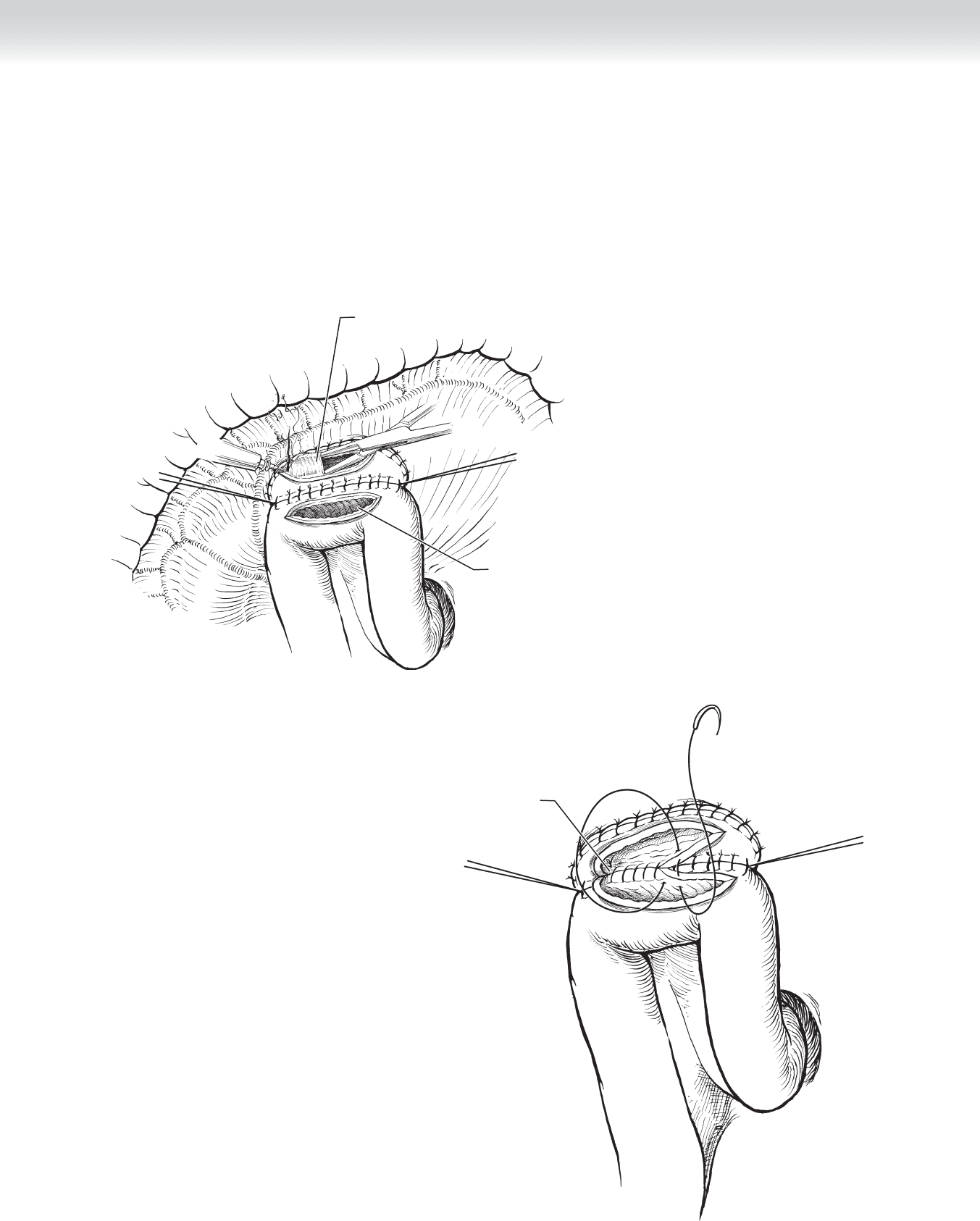
◆ Interrupted 3-0 silk sutures, placed in Lembert fashion, complete the anterior portion of
the two-layer gastrojejunostomy (Figure 32-8).
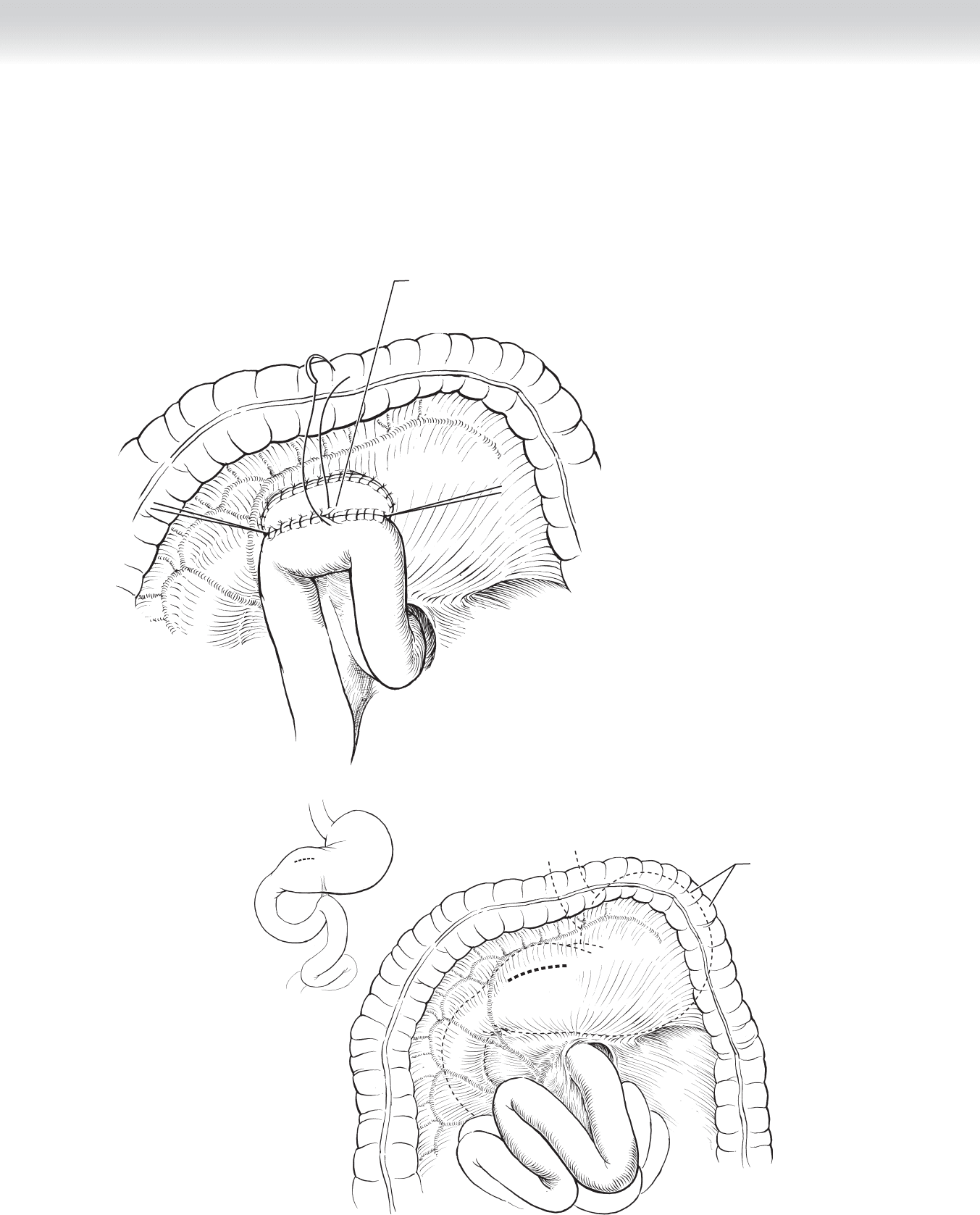
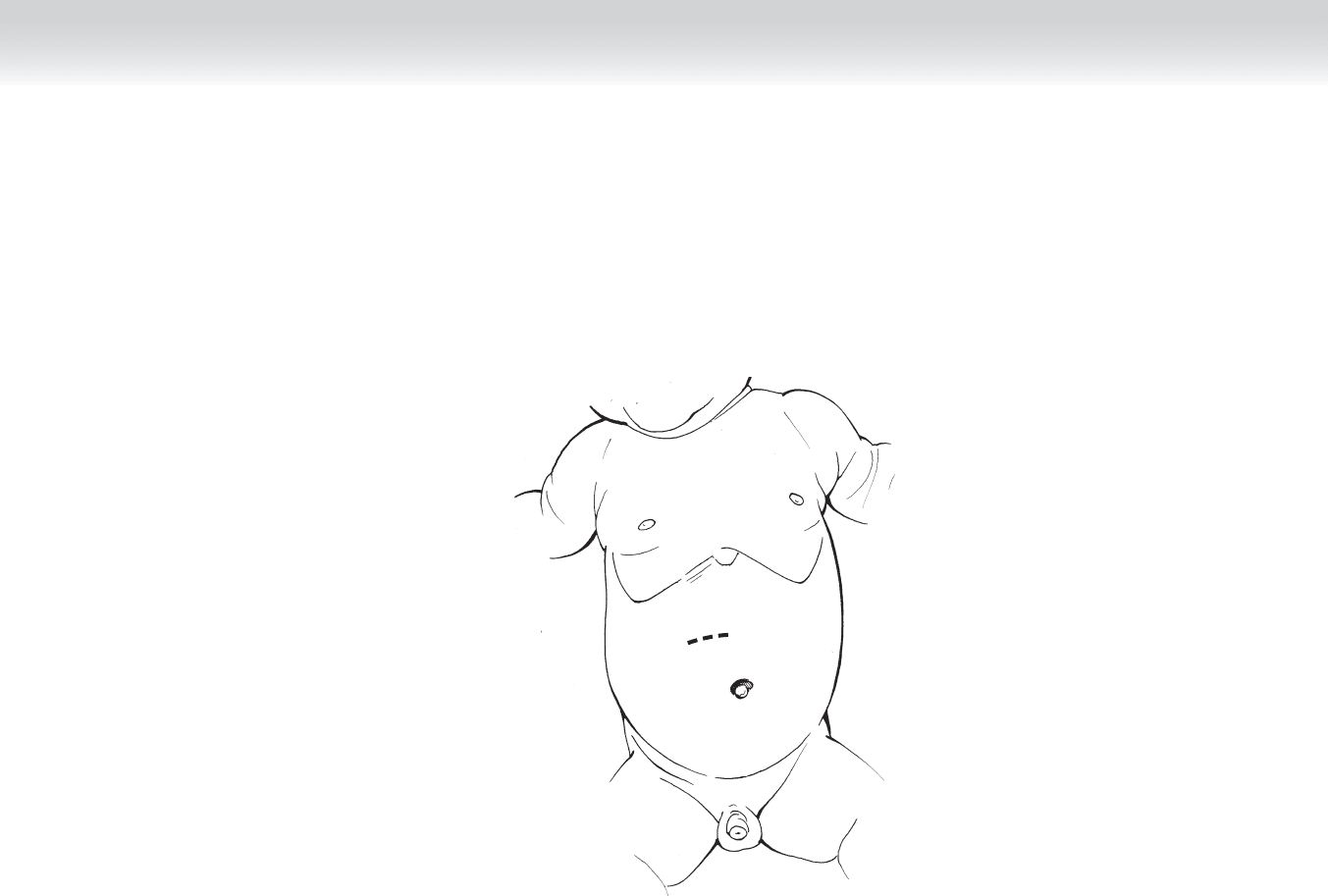
◆ If a retrocolic gastrojejunostomy is thought to be necessary, sites for anastomosis to the
stomach and jejunum are identifi ed as shown in the dashed lines in Figure 32-9. The
transverse colon is then lifted cephalad to visualize the mesentery and identify an avascular
area in which to bring the jejunal loop, as noted by the dashed lines.
Complete antecolic
gastrojejunostomy
FIGURE 32 –8
Transverse colon, and
stomach mobilized
cephalad
Sites for
anastomosis
FIGURE 32 –9
340 Section IV • The Abdomen
◆ A handsewn anastomosis is performed in the fashion already described using a two-layer
anastomosis with a posterior row of 3-0 silk interrupted sutures. The jejunal and gastric
stomas are then created using electrocautery (Figure 32-10).
◆ The inner layer of the anastomosis is accomplished using a running full-thickness absorb-
able suture (Figure 32-11).
Running closure
of posterior
mucosal layer
FIGURE 32 –11
Creating a gastric stoma
Jejunal stoma
FIGURE 32 –10
CHAPTER 32 • Gastrojejunostomy 341
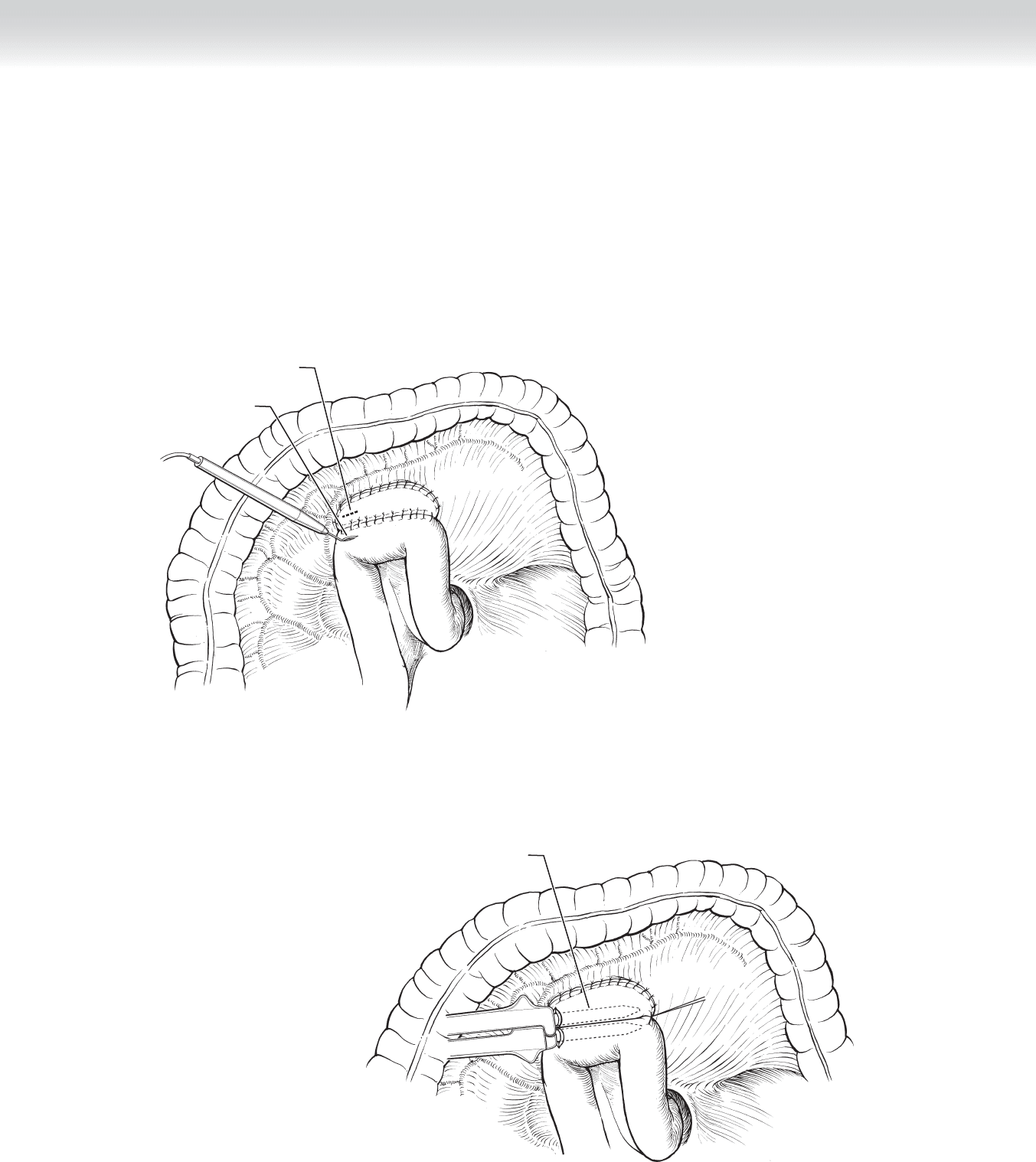
◆ The retrocolic gastrojejunostomy is then completed using interrupted 3-0 silk seromuscular
sutures placed anteriorly (Figure 32-12).
◆ Similar techniques are used to perform a stapled anastomosis (Figure 32-13).
Completing retrocolic
gastrojejunostomy
FIGURE 32 –12
Transverse colon, and
stomach mobilized
cephalad
Site for
anastomosis
MC
FIGURE 32 –13
342 Section IV • The Abdomen
◆ The jejunal and gastric stomas are created using electrocautery. The opening should be large
enough to allow entry of the stapling device (Figure 32-14).
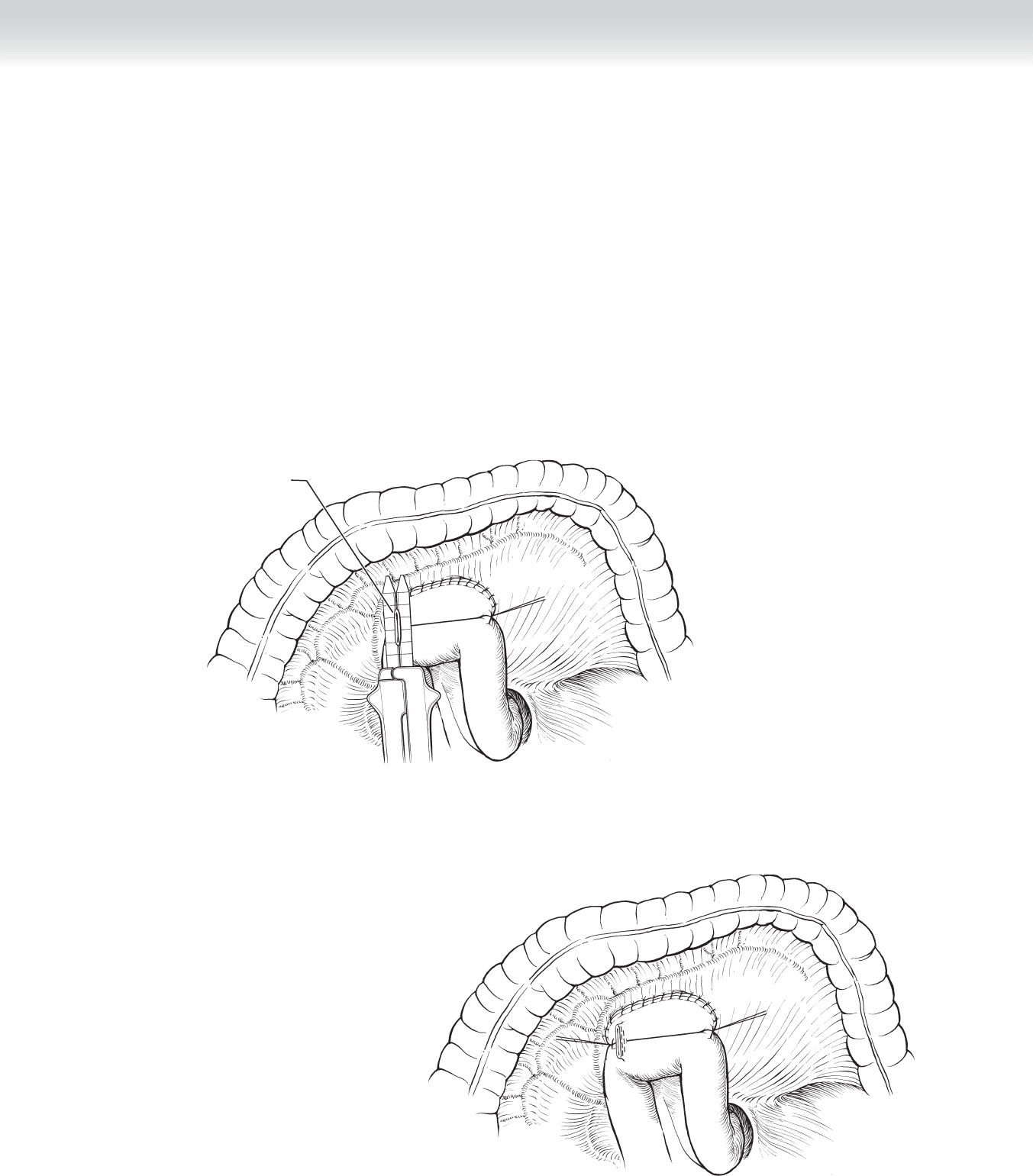
◆ The retrocolic gastrojejunostomy is then completed using the GIA stapler (Figure 32-15).
Site of gastric stoma
Creating a jejunal stoma
FIGURE 32 –14
Completing retrocolic
gastrojejunostomy
with stapler
FIGURE 32 –15
CHAPTER 32 • Gastrojejunostomy 343
◆ The openings created in the stomach and jejunum are closed together using a GIA or a TA
stapler (Figure 32-16).
◆ Figure 32-17 demonstrates the completed retrocolic anastomosis.
3. CLOSING
◆ The midline incision is closed in the usual fashion.
Removing excess
gastrojejunal tissue
FIGURE 32 –16
FIGURE 32 –17

344 Section IV • The Abdomen
STEP 4: POSTOPERATIVE CARE
◆ Postoperative care is achieved as previously noted for other gastric procedures. A nasogas-
tric tube is usually maintained postoperatively on suction, and once bowel function returns,
the tube is removed and a diet initiated.
STEP 5: PEARLS AND PITFALLS
◆ If the retrocolic approach is used, most surgeons loosely suture the edges of the mesenteric
rent to the jejunum, to minimize risk of herniation of a bowel loop.
◆ Care should be taken to clearly identify the proximal jejunum in which to make the gastro-
jejunostomy. A rare but tragic error is to mistakenly perform the anastomosis between the
stomach and ileum.
SELECTED REFERENCES
1. Mercer DW, Robinson EK: Stomach. In Townsend CM Jr (ed): Sabiston Textbook of Surgery: The Biological
Basis of Modern Surgical Practice, 18th ed. Philadelphia, Saunders, 2008, pp 1223-1277.
2. Thompson JC: Gastrojejunostomy. In Thompson JC (ed): Atlas of Surgery of the Stomach, Duodenum and
Small Bowel. St Louis, Mosby-Year Book, 1992, pp 77-81.

345
STEP 1: SURGICAL ANATOMY
◆ The pylorus sits at the distal end of the stomach. It is marked by thickening of the circular
smooth muscle layer, thus forming the pyloric sphincter, which acts as a valve between
the stomach and the duodenum and regulates gastric emptying. The pylorus does not have
independent blood supply; rather, it gets its blood supply from the vessels that perfuse the
distal stomach and proximal duodenum. Innervation of the pylorus is through the terminal
branches of the right and left vagus nerves. Any injury to these nerves or denervation of the
pylorus will result in pylorospasm and delayed gastric emptying.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The diagnosis is confi rmed when, in an infant or child with a history of postprandial, non-
bilious vomiting, the pyloric “olive” can be palpated. If this is not possible, hypertrophic
pyloric stenosis can be confi rmed by sonography when the pyloric muscle width is greater
than 4 mm.
◆ These infants often present with hypochloremic metabolic alkalosis and dehydration. Intra-
venous hydration, correction of metabolic disturbances, and establishment of adequate
urine output are imperative before pyloromyotomy.
◆ The operation is performed with the patient under general endotracheal anesthesia. Gastric
contents are suctioned thoroughly. Rapid sequence induction is used to prevent aspiration
of gastric contents.
◆ The patient is placed supine on the operating table. A folded towel under the thoracic
vertebrae facilitates exposure to the pylorus. The abdomen is painted with iodine solution.
CHAPTER
33
Pyloromyotomy
Carlos A. Angel

STEP 3: OPERATIVE STEPS
1. INCISION
◆ A transverse incision 2 to 3 cm long is made in the right upper quadrant. This incision
can be made midway between the xiphoid and umbilicus, just off the midline to the right
side. The anterior rectus fascia is opened in the direction of the incision, the rectus muscle
is divided transversely using electrocautery, and the posterior rectus fascia and peritoneum
are opened in the direction of the incision. If necessary, on the lateral side, the incision
may be extended by division (for a short distance) of the internal oblique and transversus
abdominis muscles to facilitate the delivery of the pyloric olive from the abdominal cavity
(Figure 33-1). Alternatively, a transumbilical approach may be performed by making a
semicircular incision superior to the umbilicus with a small cephalad extension (like a
Mercedes Benz star). The skin is undermined, and the rectus fascia is opened in the mid-
line for a distance of approximately 2.5 cm. The peritoneum is opened, and the pyloric
tumor is delivered into the operating fi eld by gentle traction on the antrum. After the
pyloromyotomy, closure is performed with running 5-0 polyglactin sutures for the fascia,
the most cephalad portion of the skin is reapproximated to the umbilicus, excess skin is
trimmed on both the right and left sides, and skin closure is completed with 6-0 polyglac-
tin sutures leaving a very well-hidden small semi-circular supraumbilical scar. Since there
is more extensive dissection and undermining of the skin with this incision, I routinely
administer a pre-operative dose and two post-operative doses of intravenous cefazolin to
these patients.
Section IV • The Abdomen346
CHAPTER 33 • Pyloromyotomy 347
FIGURE 33–1
348 Section IV • The Abdomen
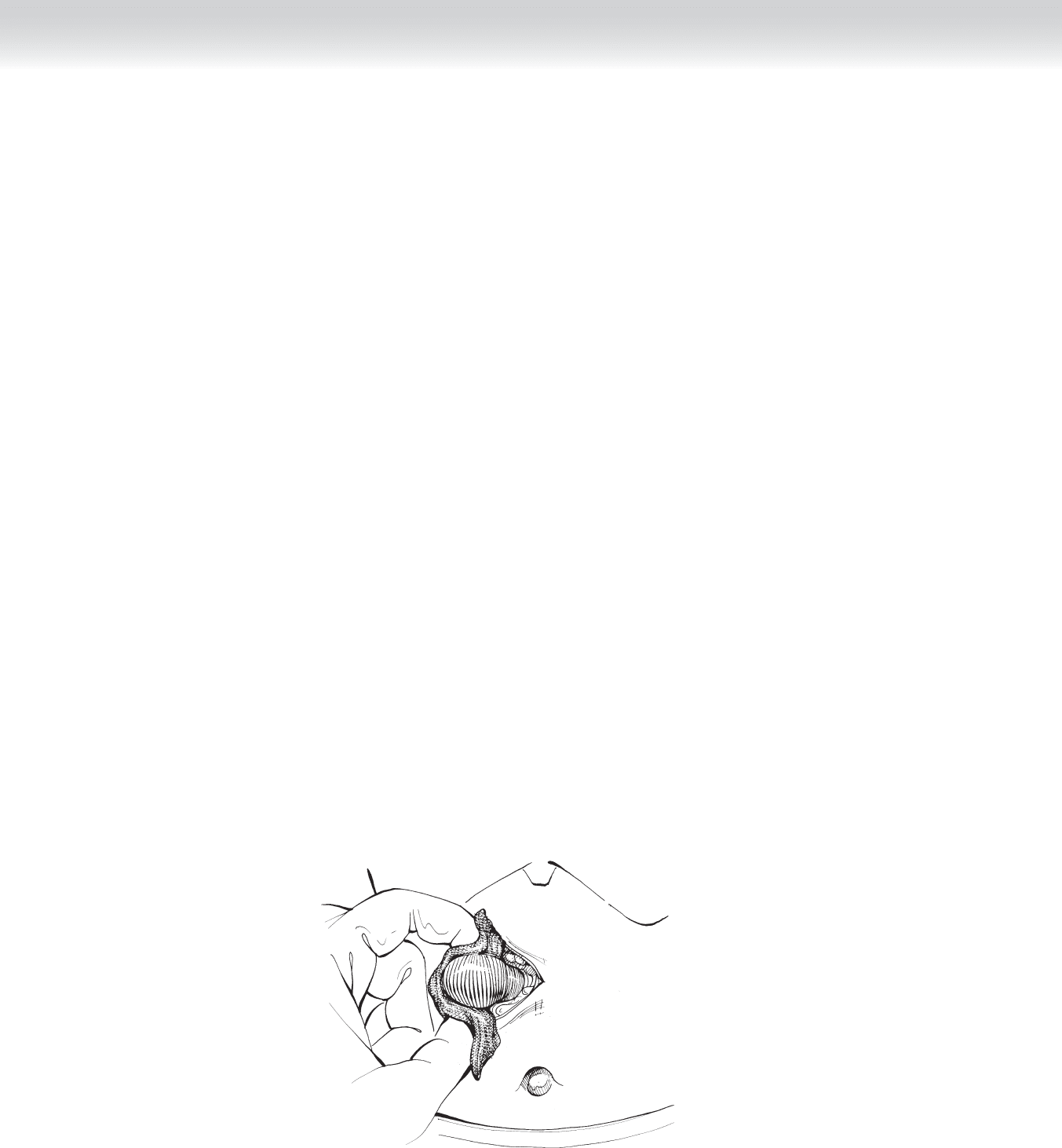
2. DISSECTION
◆ Upon entering the abdomen, the surgeon uses a small, malleable retractor over a moist gauze
to retract the liver and the falciform ligament cephalad and to the right side of the patient.
This maneuver usually exposes the greater curvature of the stomach. If the stomach is not
exposed, gentle caudal traction on the transverse colon will expose the greater curvature of
the stomach. Any attempts to grasp the pyloric tumor directly must be avoided because the
tumor is friable and will easily tear and bleed. With the stomach fi rmly grasped (a sponge
will help, because the stomach is slippery), the surgeon applies gentle to-and-fro rocking
traction to deliver the pylorus out of the incision (Figure 33-2). Palpation of the tumor will
allow precise identifi cation of the pyloroduodenal junction, because the tumor feels fi rm and
the duodenum is very soft. There is a relative avascular plane on the anterior surface of the
pylorus. A superfi cial serosal incision is made over this avascular plane, extending it distally
just proximal to the pyloroduodenal junction and proximally to the junction of the antrum
and pylorus; the length of this incision is 2 to 3 cm (Figure 33-3). There is a critical zone of
folded duodena mucosa in a very superfi cial position at the pyloroduodenal junction. This is
the area where perforations more commonly occur. Using a knife handle or another blunt
instrument, the surgeon splits the brittle pyloric muscle in the middle of the pyloromyotomy
down to the submucosa by gently pushing over the incision while supporting the pylorus
with the other hand. No attempts are made to split the muscle toward the duodenal side.
Using a pyloric spreader or a hemostat (ensuring that the tips are well above the mucosa),
the surgeon spreads the muscle beginning in the middle of the incision and then proceeding
distally and proximally (Figure 33-4). Hemostasis is performed with a fi ne-tipped cautery at
low setting; touching the mucosa with the cautery must be avoided. Completeness of the
pyloromyotomy is confi rmed when the two halves of the muscle move independently from
each other (Figure 33-5). Now the pylorus is placed back in the abdomen and a clean gauze
is placed on top of the pyloromyotomy for 2 minutes and subsequently inspected for the
presence of bile, gastric juice, or excessive bleeding. Closure is performed in layers with run-
ning 5-0 or 6-0 polyglactin sutures. The skin is closed with a running 6-0 polyglactin subcu-
ticular sutures after infi ltration with 0.25% bupivacaine and is dressed with Steri-Strips.
FIGURE 33–2