Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
369
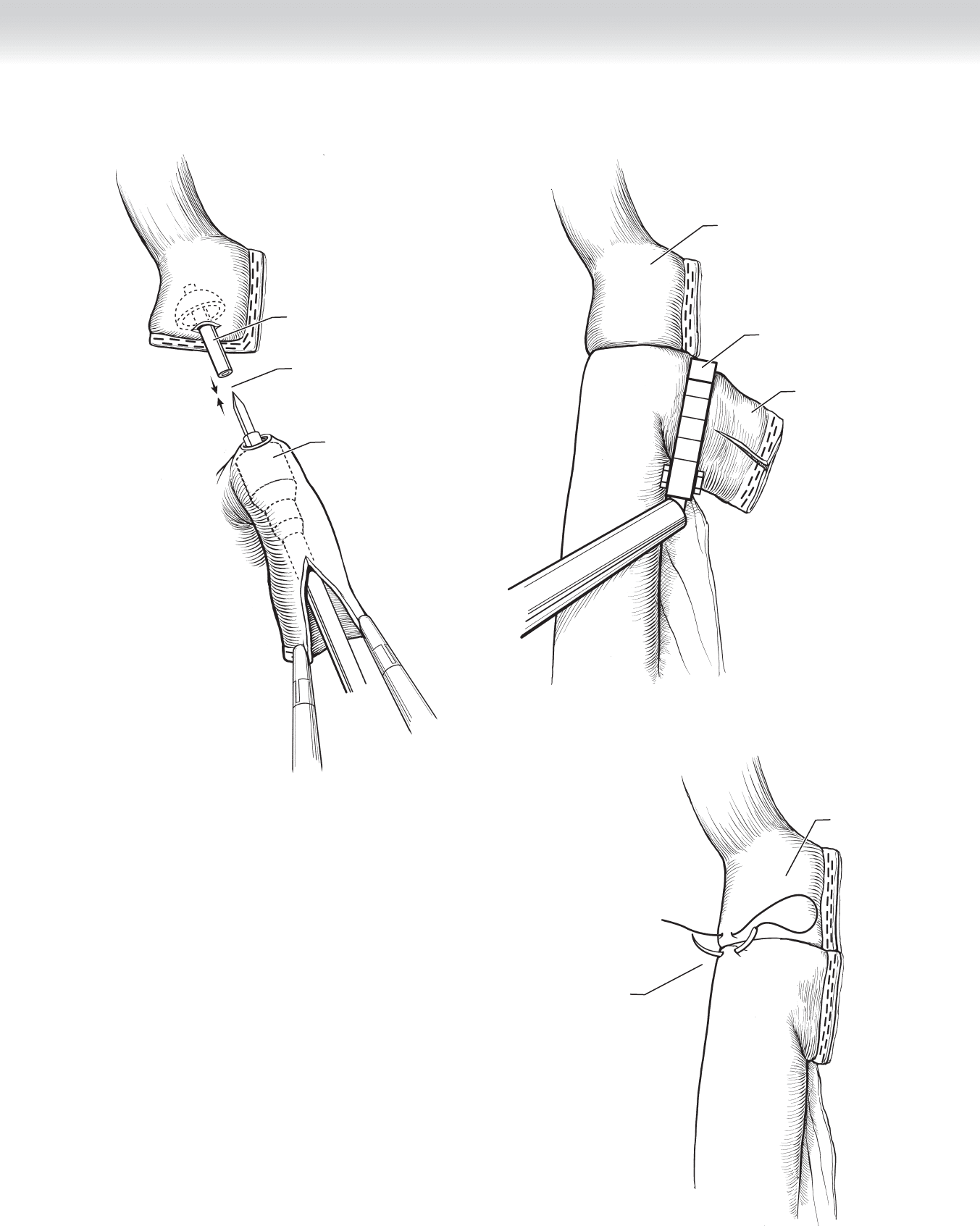
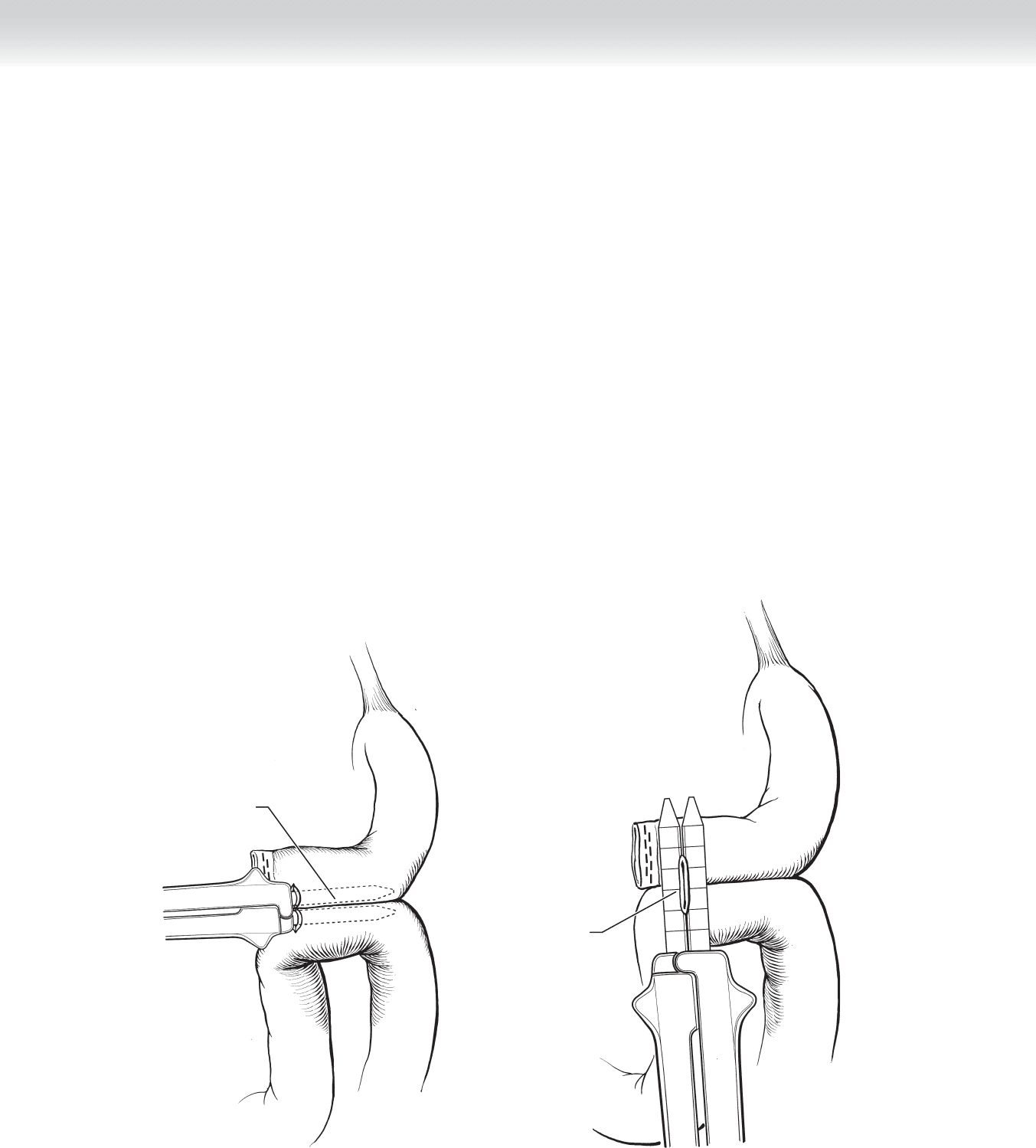
Mating together
circular stapler
and anvil
Circular stapler
Anvil
FIGURE 34–26
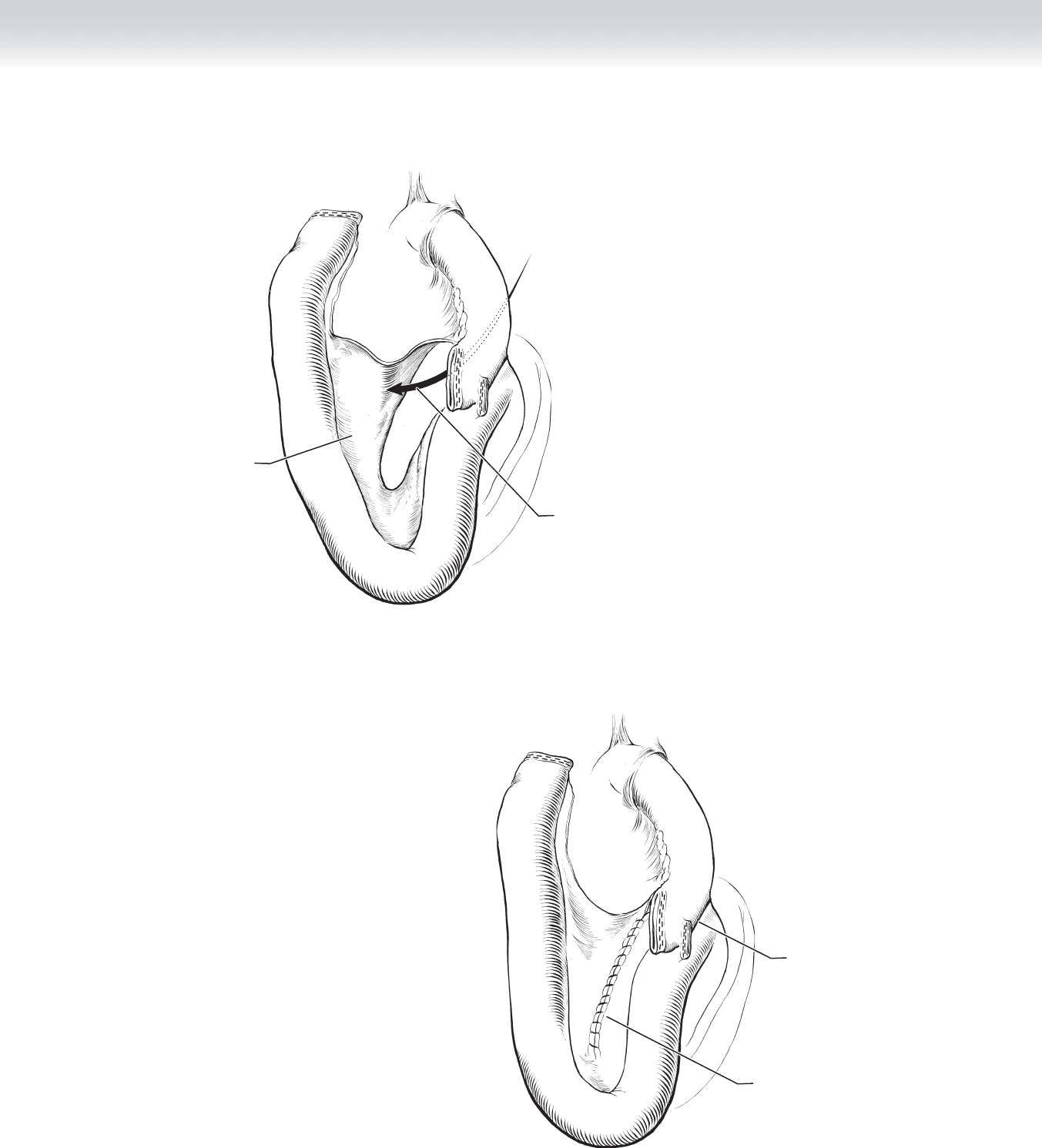
Jejunal Roux
end excess
Cutting away
jejunal excess
Stomach pouch
FIGURE 34–27
Pouch
One seromuscular
suture
FIGURE 34–28

370 Section IV • The Abdomen
3. CLOSURE
◆ The port site that had been dilated to 26 mm can be closed with two successive sutures of 0
Vicryl placed using the laparoscopic suture passer or fascial sutures through the open wound.
There is no need to close the 5- and 12-mm port sites when using bladeless trocars.
◆ The instruments and ports are removed under direct visualization as the pneumoperito-
neum escapes.
◆ The circular stapler site should be copiously irrigated before closure, because this site has
been contaminated by the circular stapler and removal of the trimmed tissue from the stom-
ach and small bowel.
◆ The skin incisions are closed with subcuticular sutures and either tissue adhesive or sterile
tapes.
OPEN
1. INCISION
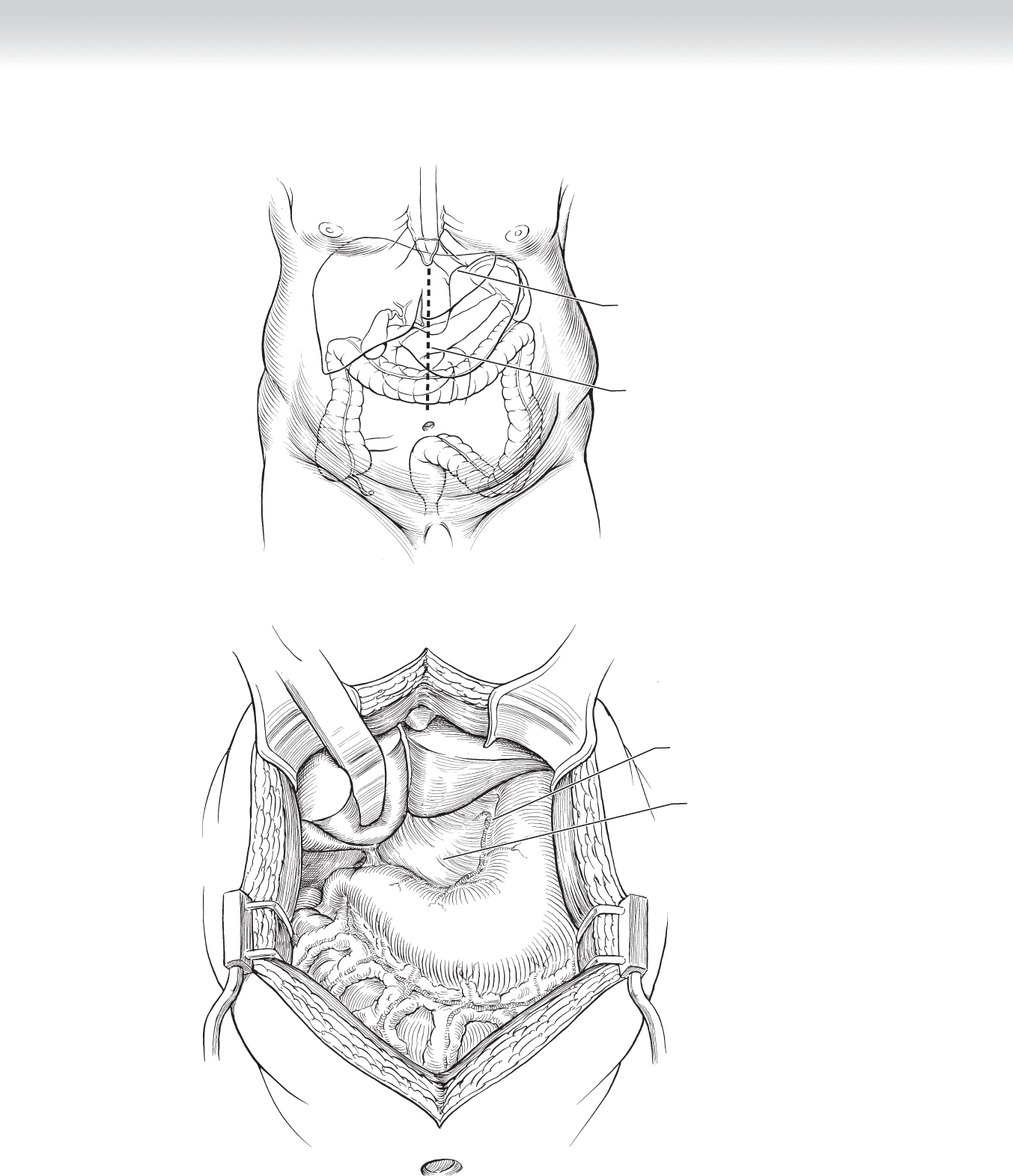
◆ A midline laparotomy from the xiphoid to near the umbilicus is preferred (Figures 34-29
and 34-30).
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
371
Esophagogastric junction
/
esophageal hiatus
Midline incision
MC
FIGURE 34–29
Stomach
Hepatogastric ligament
Left gastric artery
FIGURE 34–30
372 Section IV • The Abdomen
2. DISSECTION
◆ A table-mounted body wall retractor such as the Bookwalter model facilitates exposure.
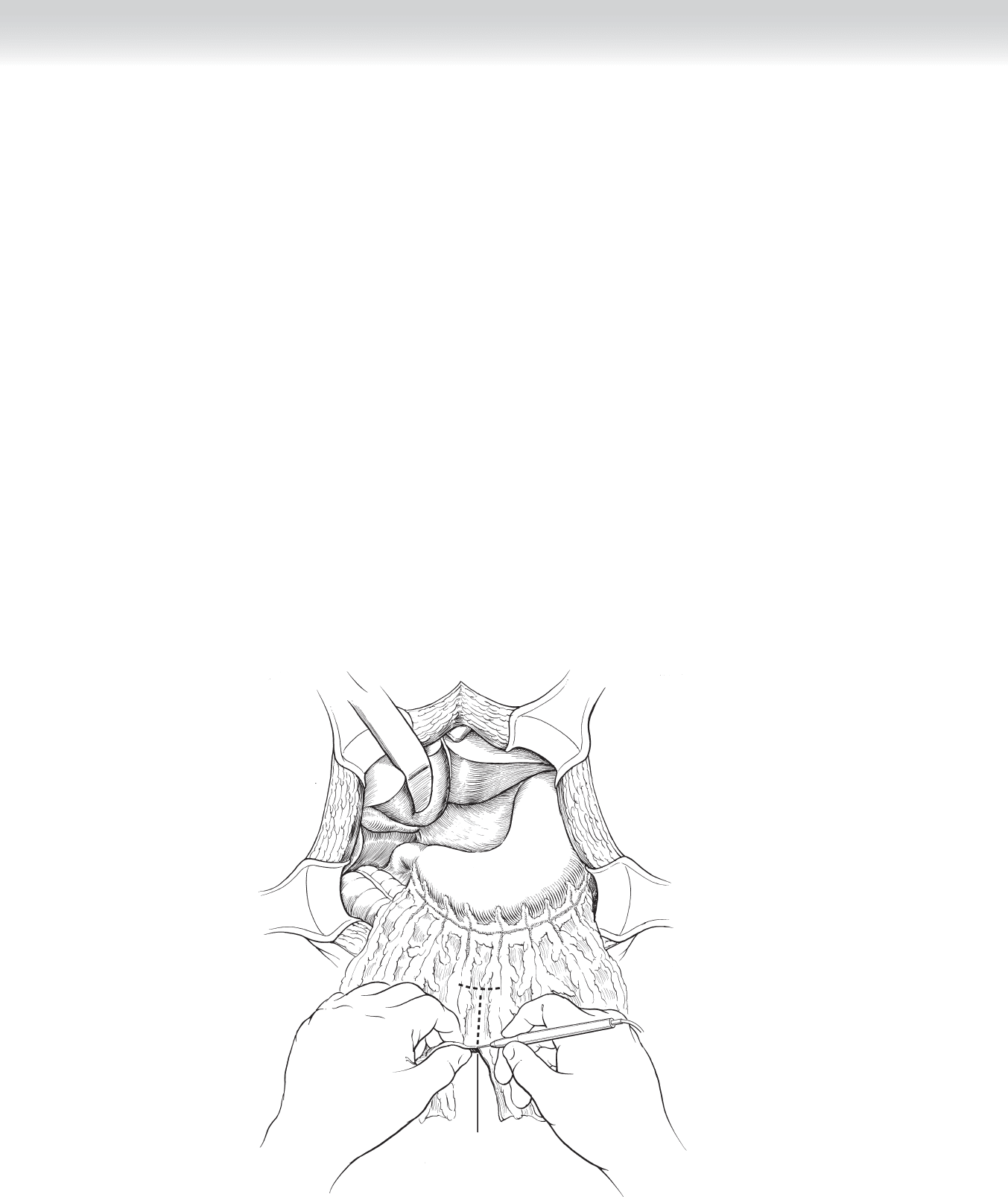
◆ The omentum is divided in the midline all the way to and for a short distance along the
transverse colon using the ultrasonic shears. This will allow placement of the Roux limb
anterior to the colon and stomach with less tension. Adhesions to the abdominal wall may
need to be divided fi rst (Figure 34-31).
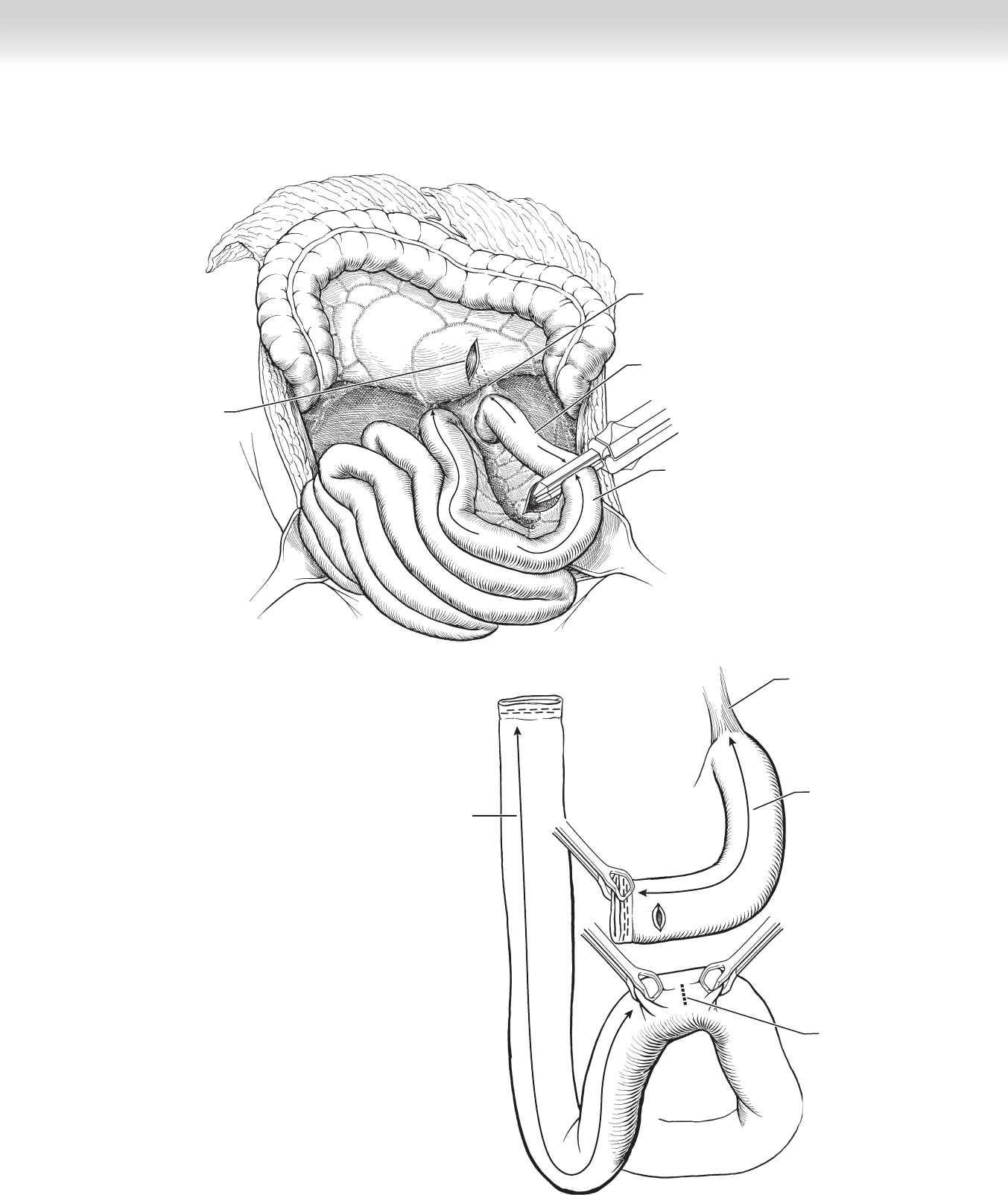
◆ The ligament of Treitz is identifi ed, and the jejunum is divided approximately 40 cm distal to it. An
opening is made in the transverse mesocolon if a retrocolic approach is favored (Figure 34-32).
◆ The mesentery of the distal aspect of the divided jejunum is incised next to the bowel wall
to provide additional mobility of the Roux limb. Any ischemia area created by this maneu-
ver will be trimmed during one of the fi nal steps.
◆ The jejunum is followed for approximately 100 cm for a standard-length gastric bypass. Here
a small enterotomy is made on the antimesenteric border. Another small enterotomy is made
at the antimesenteric corner of the proximal blind end of the jejunum. The enterotomies are
only large enough to accommodate the end of the stapler (Figure 34-33).
Creating
omental window
FIGURE 34–31
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
373
Opening created in
mesocolon
Biliopancreatic limb
Roux limb
Ligament of Treitz
3
0
c
m
1
0
0
c
m
FIGURE 34–32
Ligament of Treitz
Creating
enterotomies
30 cm
Roux limb 100 cm
from initial jejunal
transection
FIGURE 34–33
374 Section IV • The Abdomen
◆ With a jaw of the 2.5-mm stapler height linear cutter inserted though each of the enteroto-
mies, the stapler is fi red to create the anastomosis. Either one fi ring of the 60-mm stapler or
two successive fi rings of the 45-mm stapler is used here (Figure 34-34).
◆ The resulting enterotomy is closed with one fi ring of the 60-mm or two fi rings of the
45-mm linear stapler using the 2.5-mm stapler loads (Figure 34-35).
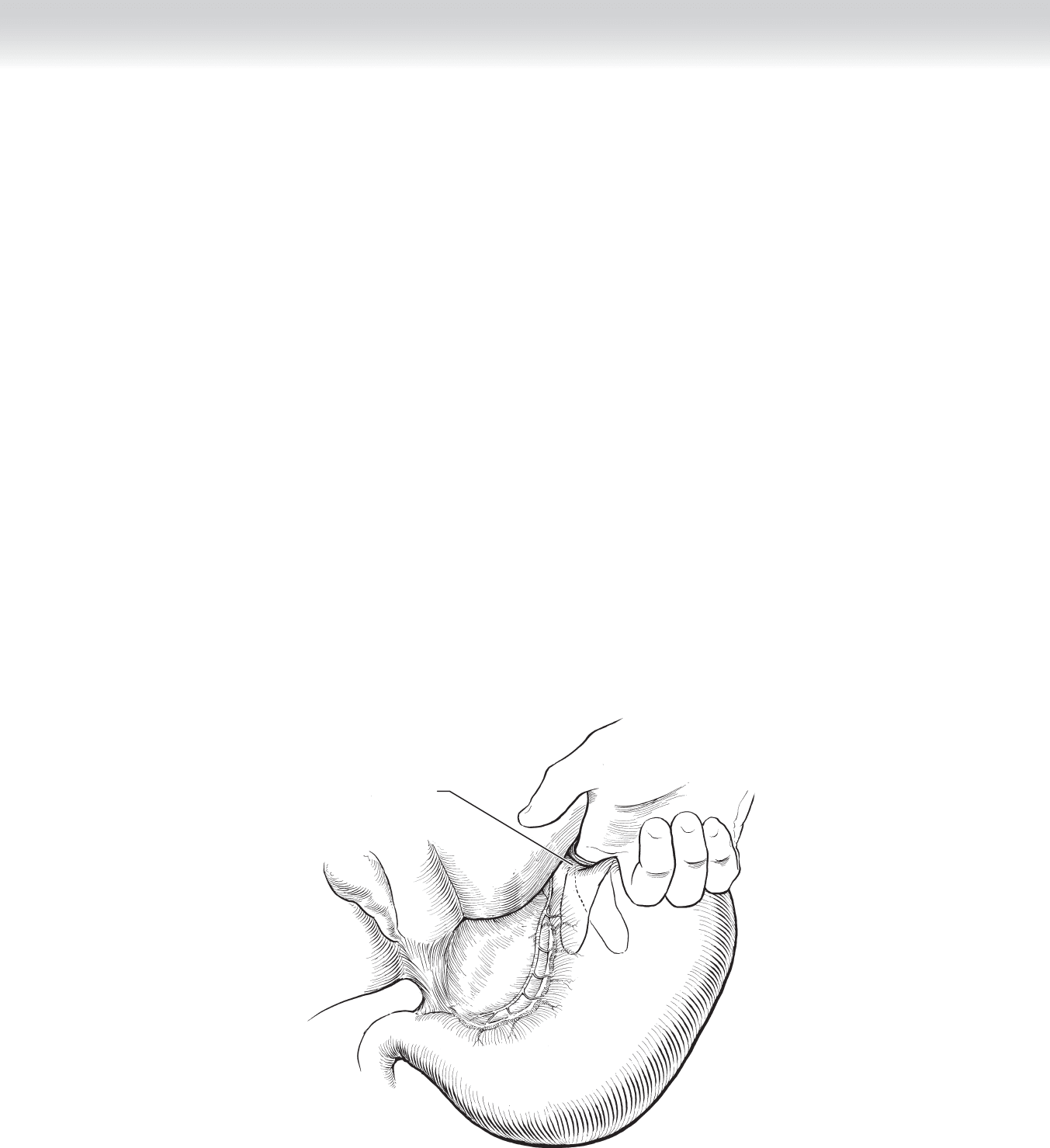
◆ A seromuscular stitch of 2-0 silk is placed at the left side of the anastomosis. The mesen-
teric defect is closed from the right side with a running 2-0 silk suture, starting at the base
of the defect and ending with a seromuscular bite of each portion of jejunum. This sero-
muscular bite is reported to decrease the risk of anastomotic obstruction (Figure 34-36).
◆ The jejunojejunostomy is inspected for adequacy of the lumen and hemostasis of the suture
and staple lines. The patient is turned to the reverse Trendelenburg position.
Creating a
jejunojejunal
anastomosis
FIGURE 34–34
Enterotomy
stapled closed
FIGURE 34–35
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
375
Arrow going through
mesentery defect
Mesentery
to be closed
A
∗
∗
B
B
Closure of
mesentery defect
Anastomosis
complete
∗
∗
FIGURE 34–36
376 Section IV • The Abdomen
◆ The peritoneum overlying the left crus of the diaphragm at the angle of His is disrupted
and spread open to expose the diaphragmatic muscle. Blunt dissection with a fi nger is used
to enlarge this space posterior to the stomach and along the crus. A thin veil of peritoneum
is left between the stomach and spleen (Figure 34-37).
◆ A balloon-tipped orogastric tube is placed in the stomach to size the pouch. The balloon is
infl ated to 20 mL and pulled back snuggly to the esophagogastric junction. Once the line of
transection is identifi ed, the balloon is defl ated and pulled back into the esophagus. One
must be continuously aware of the position of all tubes in the esophagus, because stapling
across the tubes requires a diffi cult and lengthy revision (Figure 34-38).
◆ The cautery or ultrasonic shears is used to carefully incise the peritoneum and underlying
fat of the gastrohepatic ligament to enter the lesser sac without injuring the wall of the
stomach, the vagus branches, or the vasculature of the pouch. There are a number of small
veins that, when not entirely sealed, can cause troublesome bleeding. Therefore this dissec-
tion should be performed slowly and meticulously, with a delicate combination of sweeping
and judicious use of energy sources (Figure 34-39).
Entering
phrenogastric ligament
at angle of His
FIGURE 34–37
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
377
Inflated balloon at
esophagogastric
junction
Line of
transection
FIGURE 34–38
Opening in
phrenogastric ligament
at angle of His
Entering
lesser sac
FIGURE 34–39
378 Section IV • The Abdomen
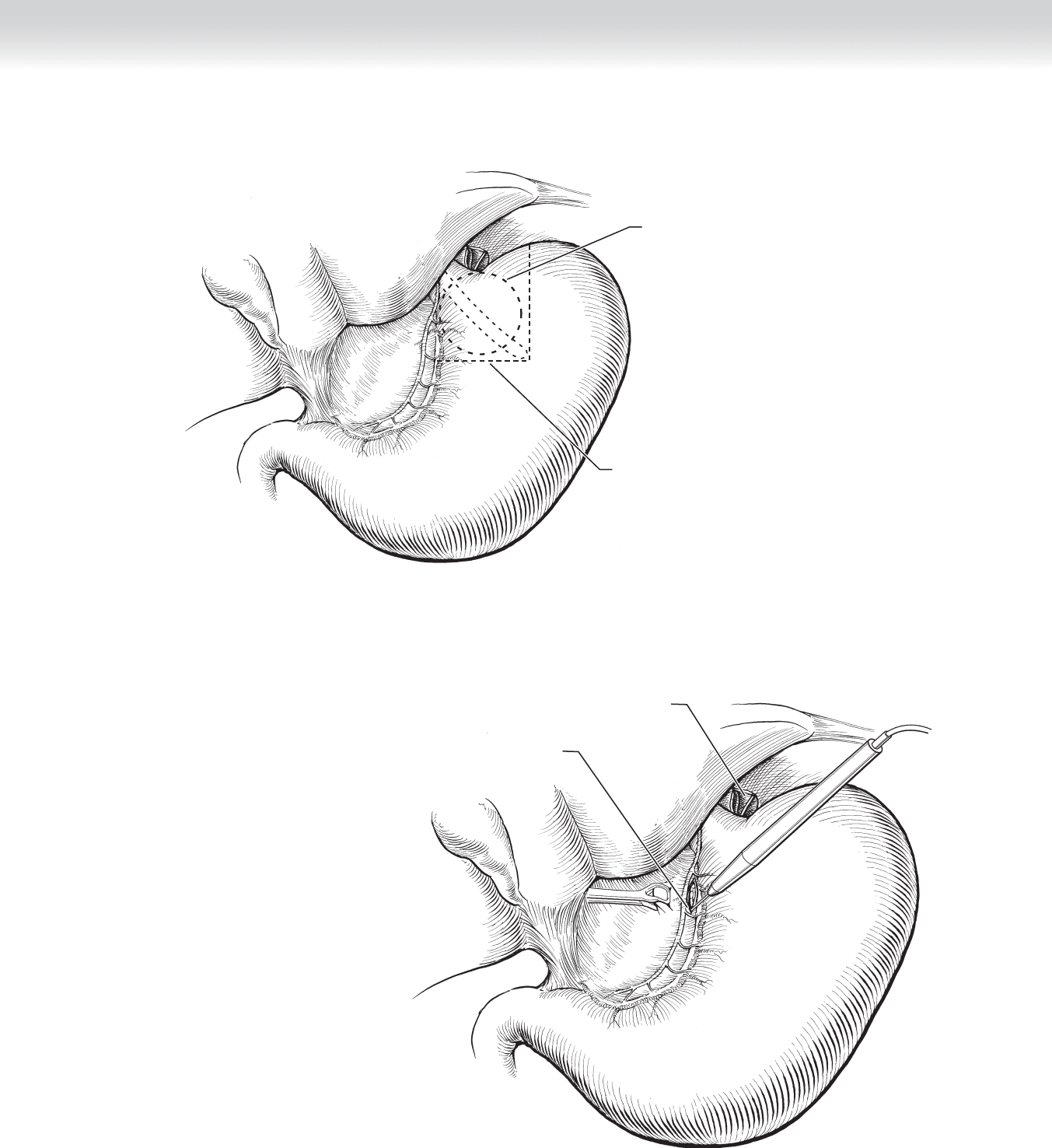
◆ An articulating 45-mm linear cutting stapler loaded with 3.5-mm staples is angled, placed, and
fi red transversely across the lesser curvature approximately 4 cm distal to the esophagogastric
junction at the site identifi ed by the balloon to begin creation of the pouch (Figure 34-40).
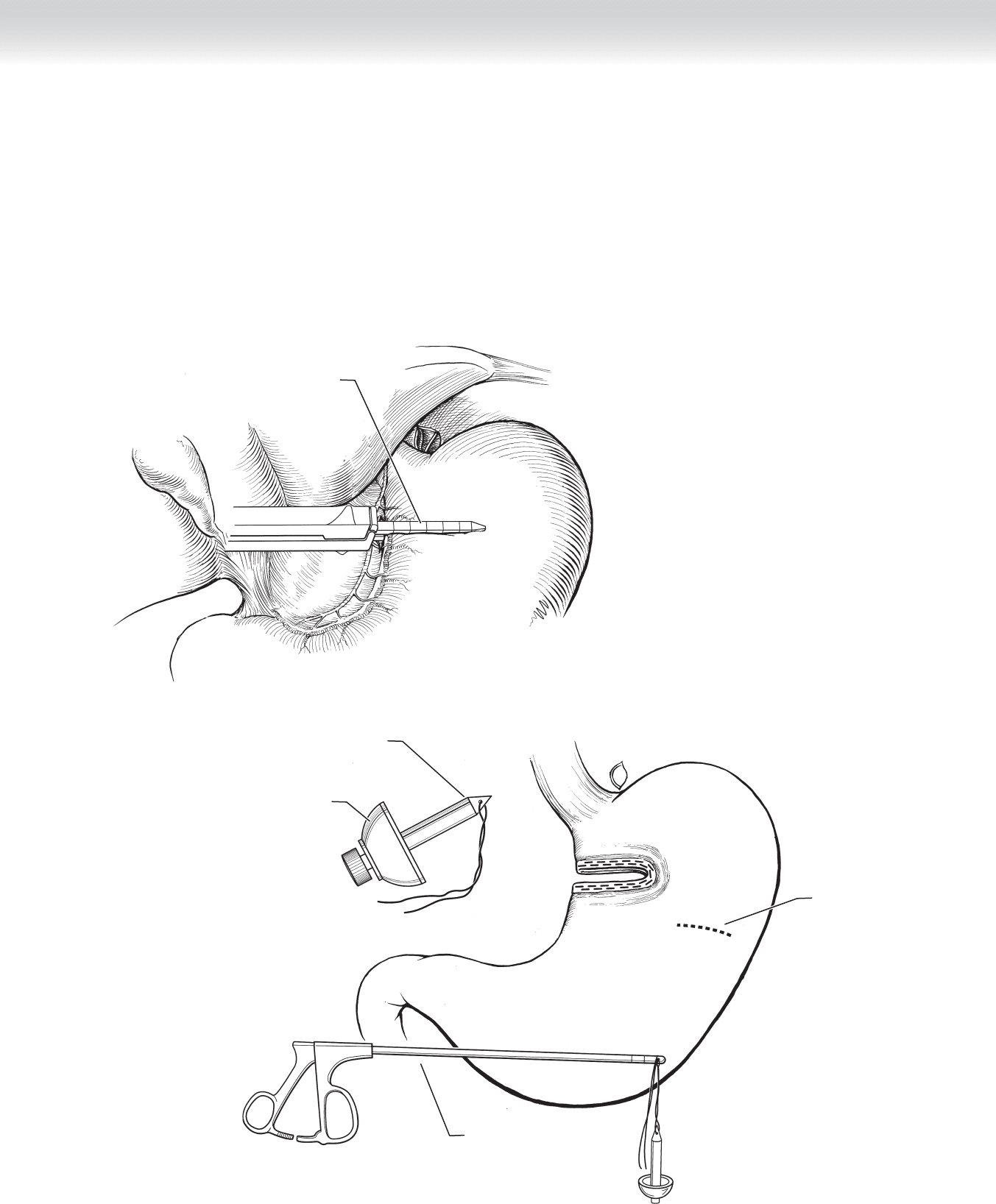
◆ A gastrotomy is made near the greater curvature of the stomach. The anvil of a 25-mm
end-to-end stapler is loaded with the spike that has a 2-0 polyester suture knotted through
its eye. The anvil is placed through the gastrotomy. The suture is threaded downward
through the eye of the 5-mm articulating dissector (Figure 34-41).
Stapling transversely
across lesser curvature
FIGURE 34–40
Trocar (spike) with
2-0 polyester suture
Circular staple anvil
Laparascopic
band passer
Gastrotomy
FIGURE 34–41