Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

502 Section VI • Liver
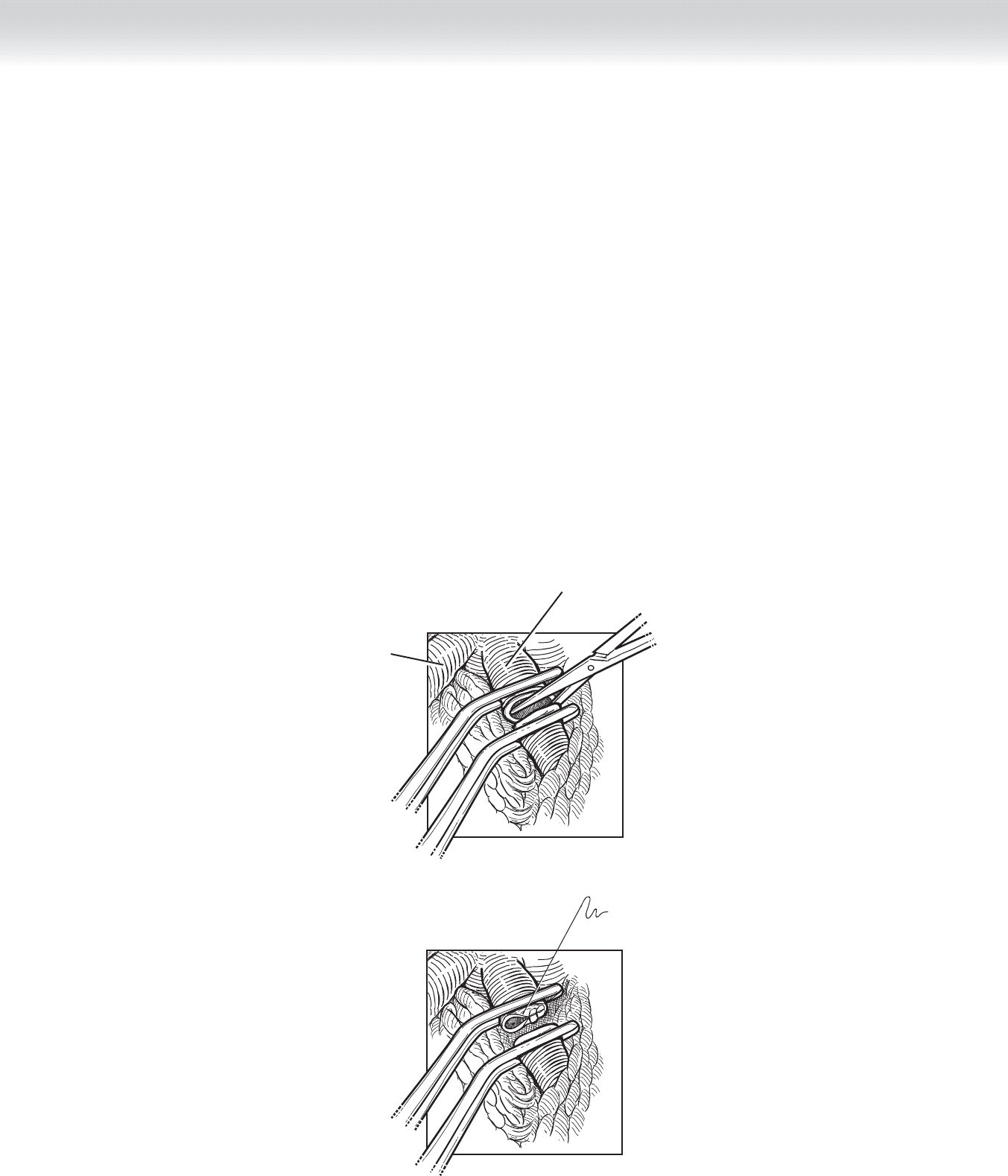
◆ Division of the left hepatic vein is performed in a manner similar to the division of the left
portal vein. Divide it between clamps. Close the open end of the divided vein with the run-
ning 4-0 Prolene suture (Figure 46-10).
◆ This step frees the specimen for removal. Perform ultrasound to confi rm that resection is
adequate and that the anticipated mass has been included in the specimen. The resulting
open space is now available for fi nal inspection (Figure 46-11).
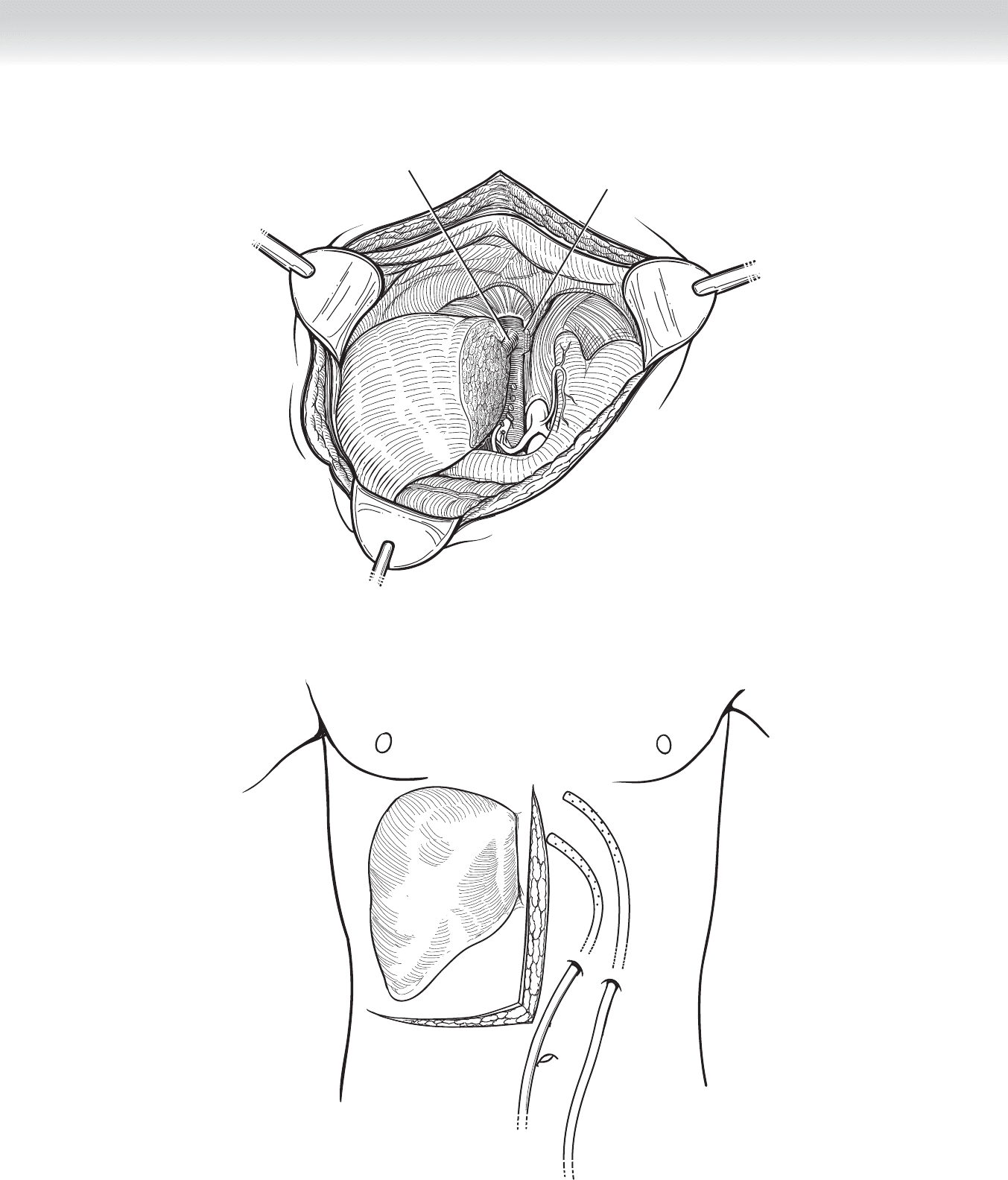
◆ Finally, address the large open surface of divided liver. Examine this surface for any large
blood vessels that may not have been adequately ligated. In particular, look for biliary
structures that must be ligated to prevent postoperative biliary leak. Drain the area with two
closed suction drains such as Jackson-Pratt or Blake drains. Place one drain more anteriorly
and the other more posteriorly. We prefer to place omentum in the space previously occu-
pied by the left liver (Figure 46-12).
Left hepatic vein
Middle hepatic vein
FIGURE 46 –10
CHAPTER 46 • Left Hepatic Lobectomy 503
Left hepatic vein
Middle hepatic vein
FIGURE 46 –11
FIGURE 46 –12

504 Section VI • Liver
3. CLOSING
◆ We close the fascia with an interrupted horizontal mattress suture (Smead-Jones) using
heavy-gauge absorbable suture. The skin is reapproximated in the standard fashion.
STEP 4: POSTOPERATIVE CARE
◆ In the fi rst 24 hours after surgery, the primary concern is hemorrhage and the related measure
of coagulation status. These should be monitored by means of serial measurement of hemo-
globin and coagulation factors.
◆ In all major resections, particularly in patients with cirrhosis, one must be vigilant for any
signs of hepatic failure. A particularly ominous fi nding is the progressive rise in bilirubin
level with an enzyme pattern that supports neither obstruction (alkaline phosphatase eleva-
tion) nor parenchymal cell death (transaminase elevations).
◆ The most ominous fi nding is a plummeting serum glucose level, which refl ects the loss of
glycogen stores in the liver and by inference the loss of viable liver. Unfortunately, there is
little one can do to reverse this pattern of failure.
◆ One possible cause of failure is inadequate liver remaining after resection. This can poten-
tially resolve over time as the liver regenerates, which it will do to some degree. Support of
the patient during this marginal period is vital.
◆ One possible remediable cause of this progressive demise is thrombus formation in the
portal vein. This would seem to be unlikely, because coagulation is typically inadequate in
these patients, but we have seen this phenomenon. It is possible that lysis of this clot may
restore vital fl ow.
◆ Sepsis is particularly metabolically taxing to the liver. In the compromised postoperative
liver, sepsis can be catastrophic. One should monitor and obtain cultures if necessary to
prevent infectious processes from progressing.
◆ Ascites may form, and one must be aware when this phenomenon has occurred and treat as
one would normally treat this entity with careful and judicious use of salt-containing intra-
venous fl uids and with diuresis.
◆ Remove drains if no bile is seen in the effl uent.

CHAPTER 46 • Left Hepatic Lobectomy 505
STEP 5: PEARLS AND PITFALLS
◆ As with all such major operative procedures, one must be extremely careful with patient
selection.
◆ If hemorrhage occurs during the procedure, one can compress the liver into the spine or
into the right fl ank to gain control, and always call for assistance from another capable
surgeon.
◆ Before dividing any of the major vascular structures, stop and reconfi rm that the proper
structure is being divided.
◆ If ascites forms and the drains are still in place, excessive electrolyte and fl uid loss may
occur from active draining of liters of fl uid per day. In this setting, one must remove the
drains (assuming they are not bile tinged) and suture the skin overlying the drain tract.
◆ In recent years, there has been some enthusiasm for preoperative embolization of the por-
tal vein on the side of the anticipated resection. This may offer some element of ischemia/
necrosis of the diseased liver and simultaneous regeneration of the opposite side.
SELECTED REFERENCES
1. Blumgart LH, Belghiti J: Liver resection for benign disease and for liver and biliary tumors. In Blumgart LH
(ed): Surgery of the Liver, Biliary Tract and Pancreas, 4th ed. Philadelphia, Saunders, 2007, pp 1341-1388.
2. Sugiyama M, Suzuki Y, Abe N, et al: Modifi ed hanging maneuver with extraparenchymal isolation of the
middle hepatic vein in left hepatectomy. J Hepatobiliary Pancreat Surg 2009;16:156-159.
3. Shirabe K, Shimada M, Gion T, et al: Postoperative liver failure after major hepatic resection for hepatocel-
lular carcinoma in the modern era with special reference to remnant liver volume. J Am Coll Surg
1999;188:304-309.

508
STEP 1: SURGICAL ANATOMY
◆ The term distal pancreatectomy and splenectomy typically refers to any resection begin-
ning at approximately the level of the spine and moving toward the tail of the pancreas
and the spleen. The associated anatomy includes the tail of the pancreas. This structure
traverses the left lateral boundaries of the retroperitoneum and extends superiorly, fi nally
ending toward the left hemidiaphragm. The tail fi ts into the concave area formed by the
medial aspect of the spleen. The blood supply to the tail of the pancreas is provided by
the splenic artery and vein.
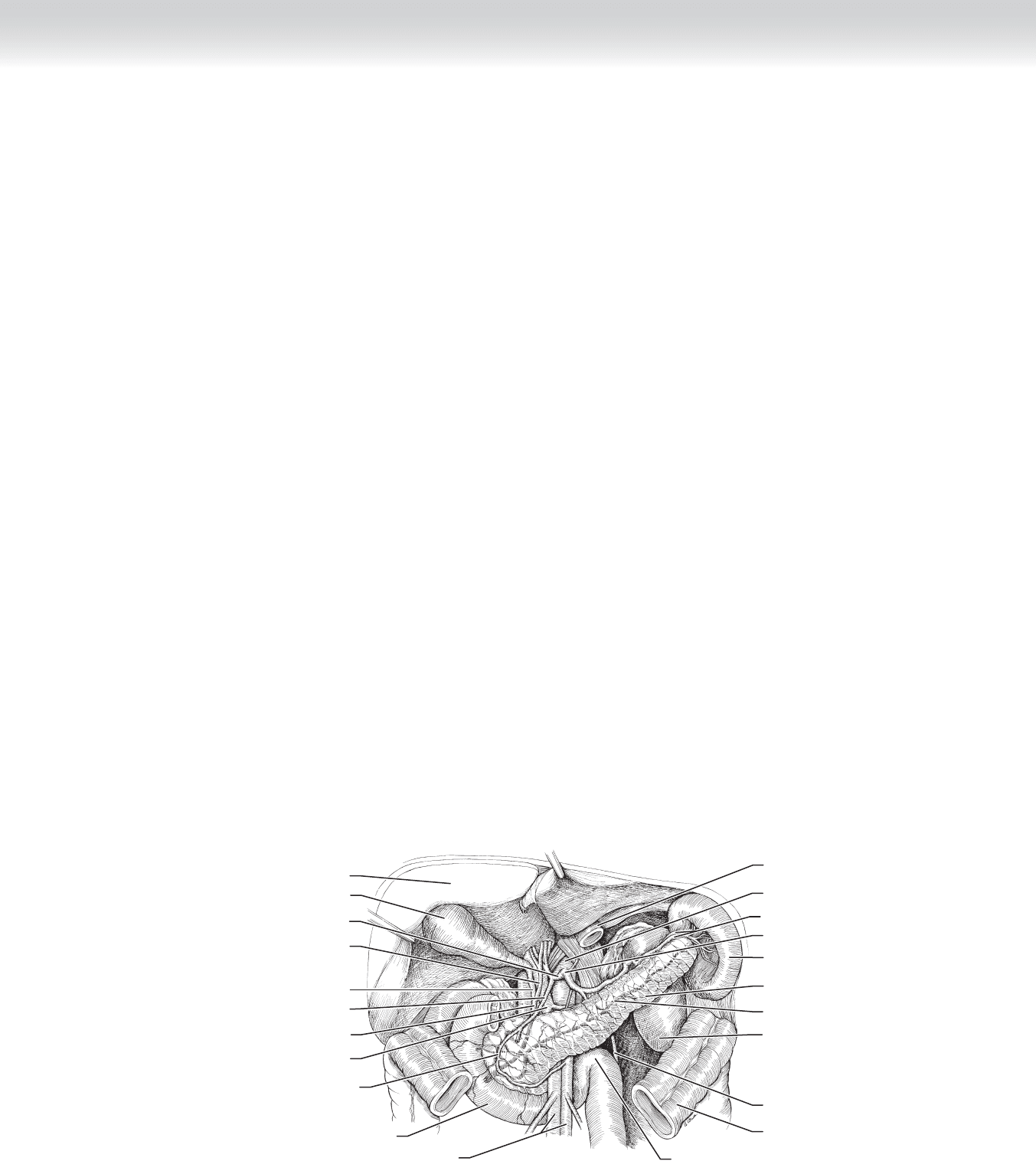
◆ The splenic artery (Figure 47-1) traverses the superior border of the body and tail of
the pancreas. There are many small branches between the artery and the body and tail
of the pancreas, which must be addressed should one choose to preserve the spleen after
distal pancreatectomy.
◆ The splenic vein is located on the posterior surface of the pancreas, and as it runs medially,
it joins the superior mesenteric vein to form the portal vein. From the body of the pancreas
out toward the tail, the splenic vein can be anticipated to maintain its position behind the
body of the pancreas until it reaches the hilum of the spleen. Once again, very small tribu-
taries will likely be encountered between the body and tail of the pancreas and splenic
vein—these must be addressed should one choose to preserve the spleen during a distal
pancreatectomy.
◆ The spleen is attached on its lateral and superior borders to the retroperitoneum, connecting
the peritoneal serosa to the visceral serosa. Posterior to the spleen and the tail of the pan-
creas is the left kidney and the left adrenal gland. These may be encountered during dissec-
tion. The stomach is situated anterior to the body and tail of the pancreas, and there are vas-
cular branches between the fundus of the stomach and the spleen. These vessels are termed
“short gastric vessels.” The transverse colon and, in particular, the transverse mesocolon may
be apposed to these tissues, and the dissections of these structures away from the spleen and
the body and tail of the pancreas are necessary to complete the resection. The splenic fl exure
of the colon typically will be mobilized during this dissection (see Figure 47-1).
CHAPTER
47
Distal Pancreatectomy and
Splenectomy
William H. Nealon
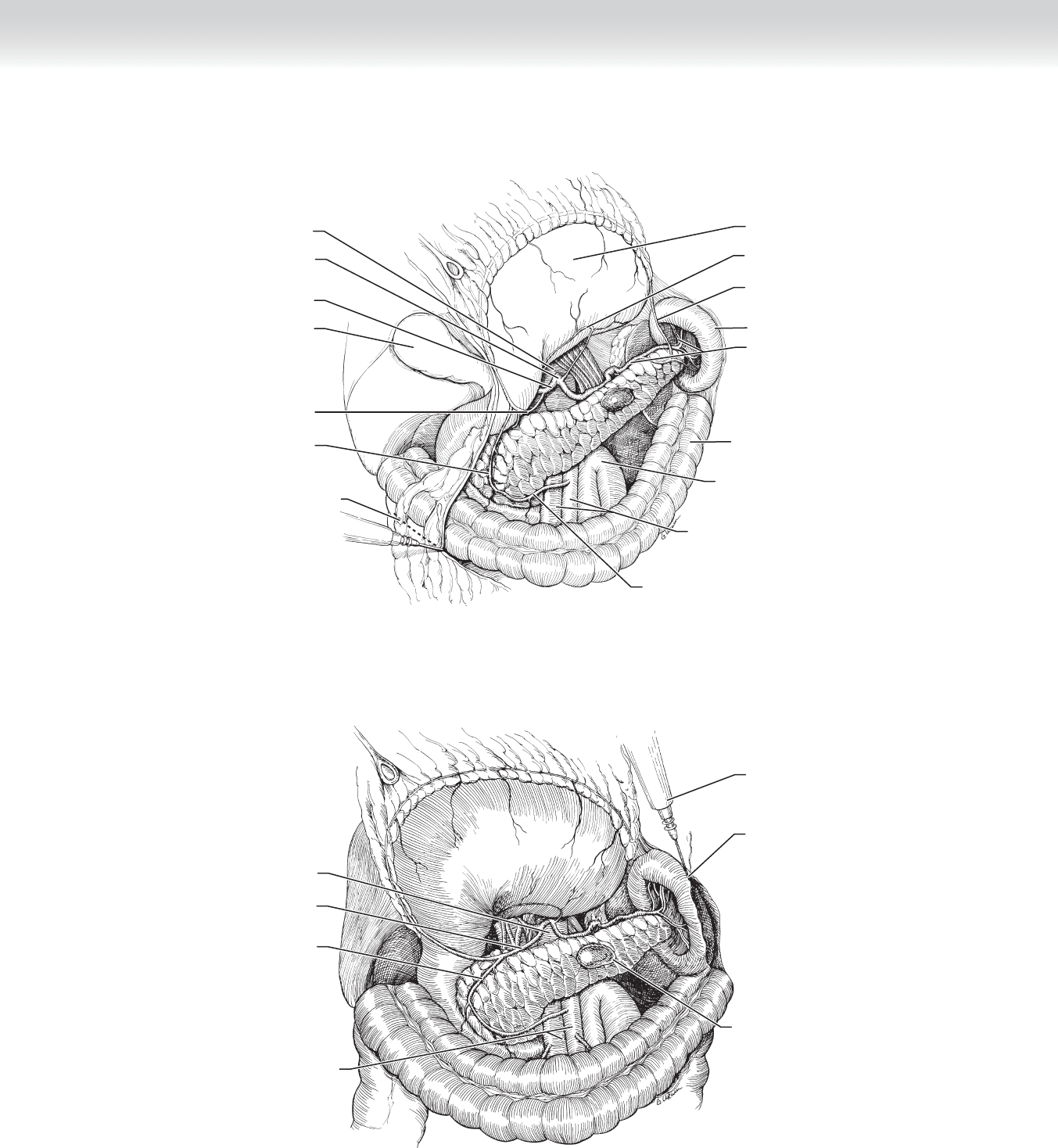
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 509
Spleen
Duodenojejunal flexure
and jejunum
Liver
Duodenum
Superior mesenteric artery and vein
Gallbladder
Cystic duct
Portal vein
Anterior, superior
pancreaticoduodenal artery
Gastroduodenal artery
Common bile duct
Splenic artery and vein
Pancreatic duct
Left kidney
Inferior mesenteric vein
Transverse colon (cut)
Pancreas
Stomach (cut)
Aorta
Celiac trunk
Common hepatic artery
Common hepatic duct
FIGURE 47 –1
INDICATIONS
◆ Distal pancreatectomy with or without splenectomy may be used for treatment of benign
and malignant lesions. Benign lesions may include an infl ammatory mass or infected
pseudocyst. Distal pancreatectomy may be required for individuals who have sustained
what has been termed “disconnected duct syndrome,” with a complete separation of the
ductal system in the tail of the pancreas from the head and body of the pancreas. This
may be found after episodes of necrotizing pancreatitis, as well as after trauma in which
typically the injury to the pancreatic duct is where the body of the pancreas traverses the
spine. Distal pancreatectomy may be used for premalignant lesions, such as intraductal
papillary mucinous neoplasms (IPMN). Similarly, mucinous cystic neoplasms are typically
located in the tail of the pancreas and are also considered to be premalignant lesions.
These are also candidates for resection. Patients may have neuroendocrine tumors, which
are not clearly malignant. These may include insulinoma or vasoactive intestinal peptide
(VIP)oma, and at times resection of the tail of the pancreas is performed to remove these.
Malignant lesions, such as primary carcinoma of the pancreas and metastatic tumors to
the pancreas, most notably renal cell carcinoma, may require distal pancreatectomy.
Among lesions in this category are primary adenocarcinoma of the pancreas, malignant
mucinous cysts, malignant neuroendocrine tumors, and metastic lesions in the tail of
the pancreas.
◆ The question of preserving the spleen is always mentioned when discussing distal pancre-
atectomy, although often the decision for including a splenectomy is made at the time of
the operation, depending on the anatomy encountered and the amount of distortion of
planes created by the underlying disease. There is general agreement that malignancies be
uniformly accompanied by splenectomy to ensure adequate margins. For benign disease,
particularly for lesions such as IPMN, in which the pancreas is essentially normal, it should
be possible to safely resect the tail of the pancreas without including the spleen.

510 Section VII • Pancreas
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ As with all major abdominal surgery, one needs to consider the patient’s American Society
of Anesthesiologists (ASA) status and relative risk of operation. Specifi c to this operation
are a number of features. First, because the density of beta cells may be far greater in the
tail of the pancreas than in the body and the head, there is a heightened risk of insulin de-
pendence after distal pancreatectomy. Surprising to some, the risk of insulin dependency is
greater after distal pancreatectomy than it is after a resection of the head of the pancreas. It
is important to advise the patient of this risk preoperatively. If the patient has an associated
diagnosis of chronic pancreatitis or borderline diabetes, certainly the risk of developing
insulin dependence is higher.
◆ The second issue is the possibility of a splenectomy and the need to address the issue of post-
splenectomy sepsis. This entity is now relatively easily managed by obtaining vaccines for the
encapsulated organisms that are responsible for postsplenectomy sepsis. These are pneumo-
coccus, meningococcus, and Haemophilus infl uenzae. There are two choices for administering
these vaccines. The fi rst is to administer them a minimum of 2 weeks before the operative
procedure. The strategy is that the immune status will be suffi cient to mount an antibody
response to the antigens before surgery. If the decision to administer vaccines is delayed until
it is clear that the patient has had a splenectomy, then the vaccines may need to be adminis-
tered postoperatively. Because of the proven changes in immune capabilities early after major
surgery, the recommendation is to wait a minimum of 4 weeks after surgery to administer the
vaccines. These vaccines should be administered at 5-year intervals for life, and the patient
should be advised of this issue before surgery. It is well known that a patient with a splenec-
tomy may also develop thrombocytosis after surgery, and this should be monitored carefully.
◆ Finally, particularly in patients with a normal pancreas, there is a chance that postoperative
pancreatitis may develop, and enzymes should be followed for evidence of acute infl amma-
tion in the early postoperative period. It is possible to assume some of these changes are
simply related to the stress of operation. One must exercise a high level of suspicion in this
regard.
◆ Perhaps the most nettlesome postoperative issue in these patients is the frequency of pan-
creatic fi stula after resection of the tail of the pancreas. There are those who have suggested
routinely using preoperatively placed pancreatic ductal stents to prevent this. This is cer-
tainly not practiced widely. In any event, it is important to advise patients that this eventu-
ality is seen in as many as 25% of patients who have undergone resection of the tail of the
pancreas. This compares poorly with the 15% risk of pancreatic fi stula after pancreaticodu-
odenectomy.
STEP 3: OPERATIVE STEPS
◆ Preoperative bowel prep and intravenous antibiotics at the time of the incision are both rec-
ommended. The characteristic bowel preparation is bowel cleansing combined with oral
neomycin and erythromycin for three doses before the surgery. Intravenous antibiotics are
generally second-generation cephalosporins or something similar.
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 511
1. INCISION
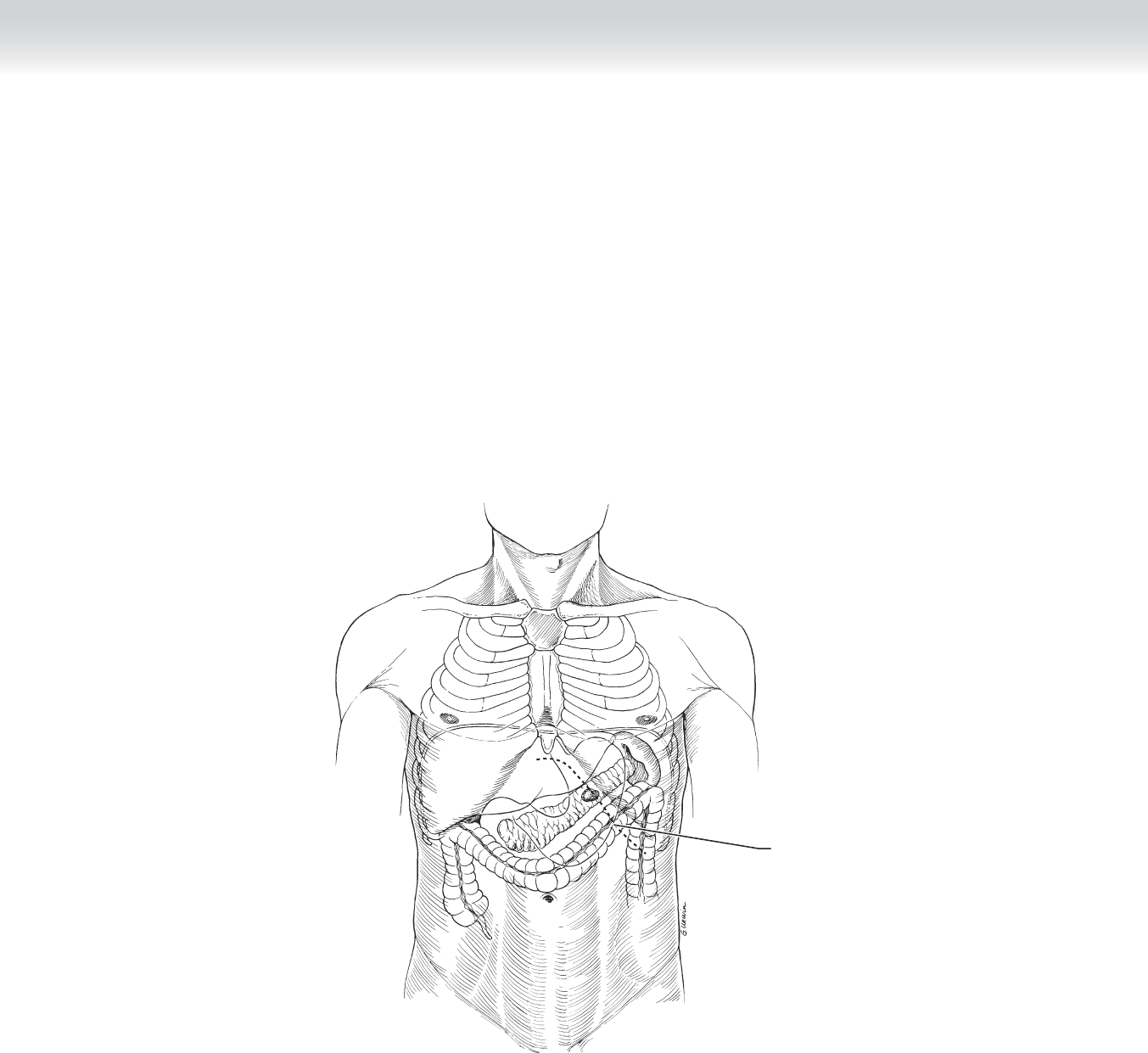
◆ We use the left subcostal incision with a horizontal shaping of the subcostal incision at
the midline to facilitate extending to the right subcostal if necessary. We similarly create a
horizontal direction to the incision as we pass beneath the costal margin laterally, again to
facilitate extending an incision if necessary. In general, with the exception of markedly
obese patients, one can perform this operation safely with the relatively minimal incision
in the left subcostal region (Figure 47-2).
Subcostal incision
FIGURE 47 –2

512 Section VII • Pancreas
2. DISSECTION
◆ Upon entering the abdomen, the general evaluation of the abdomen may be necessary, par-
ticularly if malignancy is being treated. Specifi cally, one should look for evidence of perito-
neal seeding or any evidence of hepatic metastasis. It is also usually possible to palpate the
lesion whether benign or malignant through the omentum in the left upper quadrant.
◆ The lesser sac is entered by grasping the gastrocolic omentum and refl ecting superiorly
and anteriorly. This reveals the posterior surface of the omentum as it attaches to the trans-
verse mesocolon. Using electrocautery and beginning well to the left of the spine, it is pos-
sible to dissect the attachments between the omentum and the transverse colon. There is
characteristically some amount of adhesion between the appendices epiploicae and the
transverse mesocolon, and these must be carefully separated until the lesser sect can be
entered (Figure 47-3). At times in patients who have had previous signifi cant pancreatitis,
this plane may be impossible to traverse. As the omentum is mobilized along the trans-
verse colon, the necessary window into the lesser sac will depend on the size of the patient
and the size of the lesion. It is certainly possible to extend the dissection well over to the
right of the midline if necessary to establish a wider entry into the lesser sac. Upon enter-
ing the lesser sac in this fashion, it is possible to refl ect the stomach superiorly and anteri-
orly, revealing the anterior surface of the body of the pancreas. The omentum dissection
can be carried to the left, mobilizing the splenic fl exure of the colon in this fashion. It may
be helpful to refl ect the splenic fl exure of the colon inferiorly to delineate the inferior bor-
der of the spleen and the inferior border of the tail of the pancreas. After this amount of
dissection, it is hoped that one should have fully visualized the lesion and determined ex-
actly what amount of body of the pancreas may need to be removed for adequate excision.
If it is not possible to fully identify the lesion at this point, it may be necessary to use an
ultrasound probe to facilitate identifi cation. This is commonly needed when exploring for
benign neuroendocrine tumors, such as insulinoma or gastrinoma (see Figure 47-3).
◆ At this point, an option is available for defi ning and dissecting the splenic artery on the
superior border of the pancreas. This maneuver may facilitate control of hemorrhage if one
anticipates encountering signifi cant hemorrhage during the dissection of the spleen and
the tail of the pancreas. This can simply be done with an atraumatic vascular clamp if one
is not certain that the spleen will need to be removed and serves as a control for hemor-
rhage (see Figure 47-3).
◆ Next, attention is directed to the left hemidiaphragm in the left upper quadrant of the ab-
domen. The peritoneal attachments, lateral to the spleen, are incised using electrocautery,
and this permits beginning of the mobilization of the spleen and the tail of the pancreas
toward the midline. One may continue medially along the superior border of the spleen.
As one turns the dissection in an inferior direction on the medial (hilar) aspect of the
spleen, one encounters the short gastric vessels (Figure 47-4).
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 513
Left gastric artery
Duodenojejunal junction/
Ligament of Treitz
Superior mesenteric artery and vein
Stomach reflected cephalad
Splenic artery and vein
Spleen
Left gastroepiploic artery
Transverse colon
Inferior pancreaticoduodenal artery
Aorta
Celiac trunk
Common hepatic artery
Gastroduodenal artery
Cautery of greater omentum
Gallbladder
Pancreaticoduodenal artery
Aorta
Pancreaticoduodenal artery
Gastroduodenal artery
Superior mesenteric artery
and vein
Cauterize lateral peritoneal
attachments to the spleen
Carefully dissect the
retroperitoneal attachments
and mobilize the spleen
to midline
Pancreatic lesion
FIGURE 47 –3
FIGURE 47 –4