Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


482 Section VI • Liver
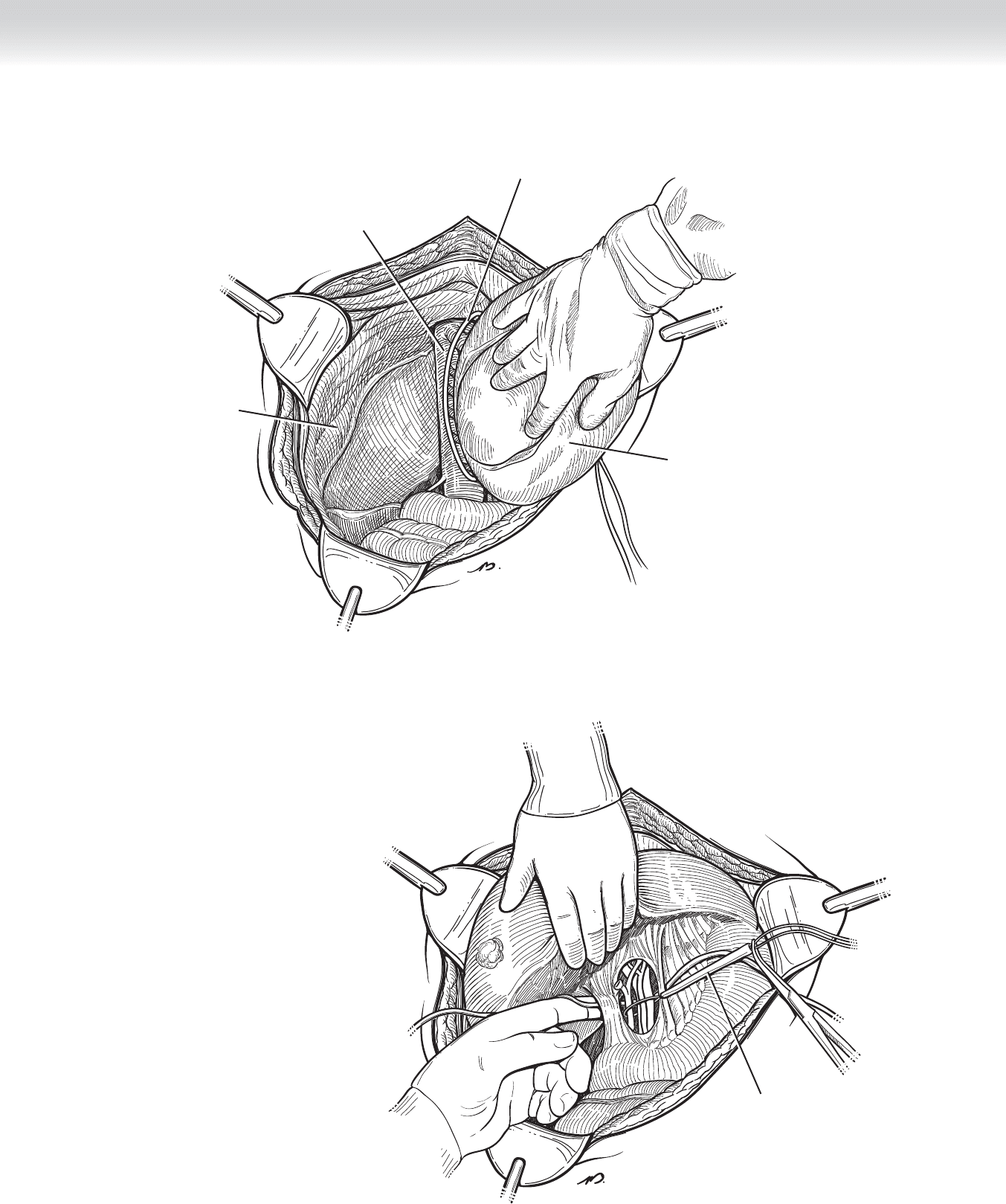
◆ Divide the anterior and posterior leafl ets of the right triangular ligament using electrocautery.
It is usually best to fi rst extend the incision of the anterior leafl et from the right lateral margin
to the midline. At this point, gentle blunt dissection will separate the diaphragmatic attach-
ments, better revealing the posterior leafl et and facilitating division of this structure. In this
fashion, the liver is mobilized to the midline, as well as in a caudal direction (Figure 45-6).
◆ At the most posterior and medial extent of this dissection, the vena cava is seen, and the
small tributaries between the posterior surface of the liver and the vena cava can be visual-
ized. We delay division of these vessels until we have fully dissected the hepatoduodenal
ligament. The umbilical tape is used as a tourniquet surrounding the liver parenchyma from
the posterior to the anterior surface in the anticipated line of resection. On occasion, this
maneuver may be useful to control parenchymal bleeding during division of the right liver
(see Figure 45-6).
◆ The right hepatic and middle hepatic veins will be visible at the superior extent of dissec-
tion in the midline. Dissect and place a vessel loop around the right hepatic vein at this
time for later division. Because the liver may be displaced either to the left or to the right
compared with classic orientation, one must confi rm that the vein encircled is in fact the
right hepatic vein (see Figure 45-5).
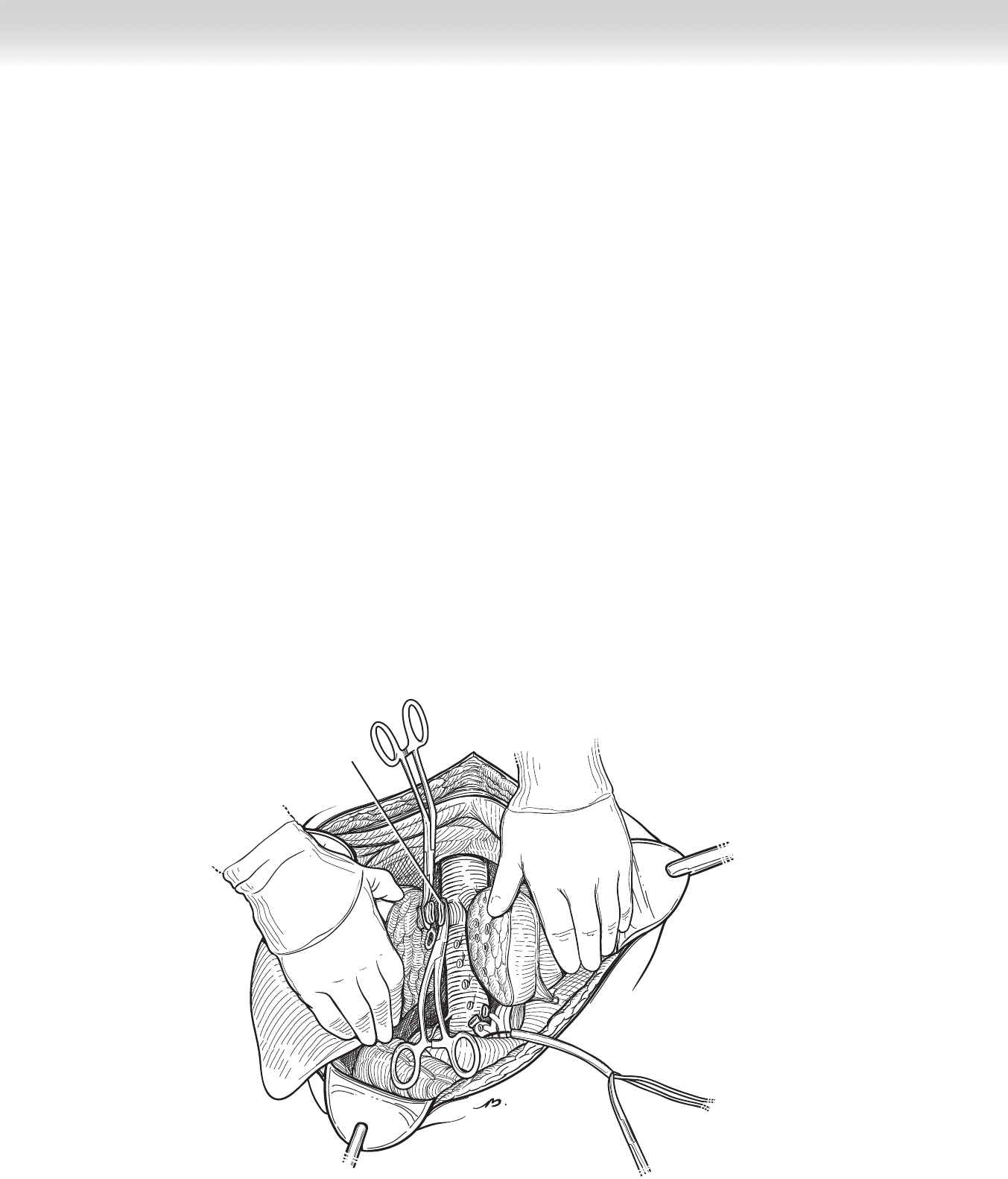
◆ Dissect the peritoneum overlying the hepatoduodenal ligament in a transverse direction.
After dividing the typically fi lmy gastrohepatic or lesser omentum medial to the ligament, it
should be possible to pass your fi nger or an instrument into the foramen of Winslow and
completely encircle the structures contained in the hepatoduodenal ligament (Figure 45-7).
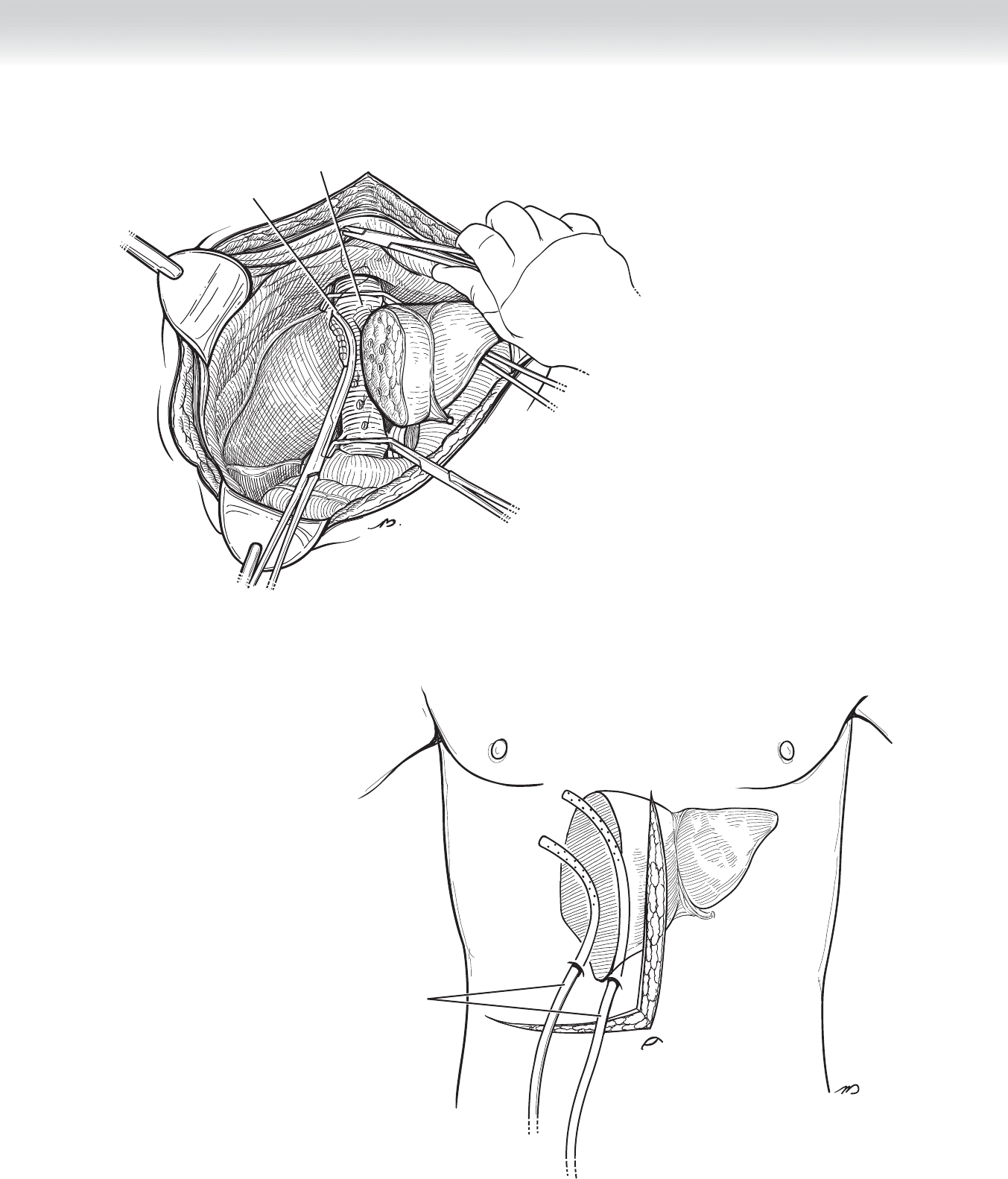
◆ Pass an umbilical tape around the ligament and, using the hooked instrument with a sec-
tion of rubber tubing, create a Rummel loop. This safety measure is performed to permit
complete infl ow occlusion, which may be necessary to control undue hemorrhage if
encountered during the procedure. Place a hemostat on the two loose ends of umbilical
tape (see Figure 45-7).
CHAPTER 45 • Right Hepatectomy 483
Rummel loop
FIGURE 45 –7
FIGURE 45 –6
Inferior
vena cava
Right lobe
reflected medially
Diaphragm
Tourniquet

484 Section VI • Liver
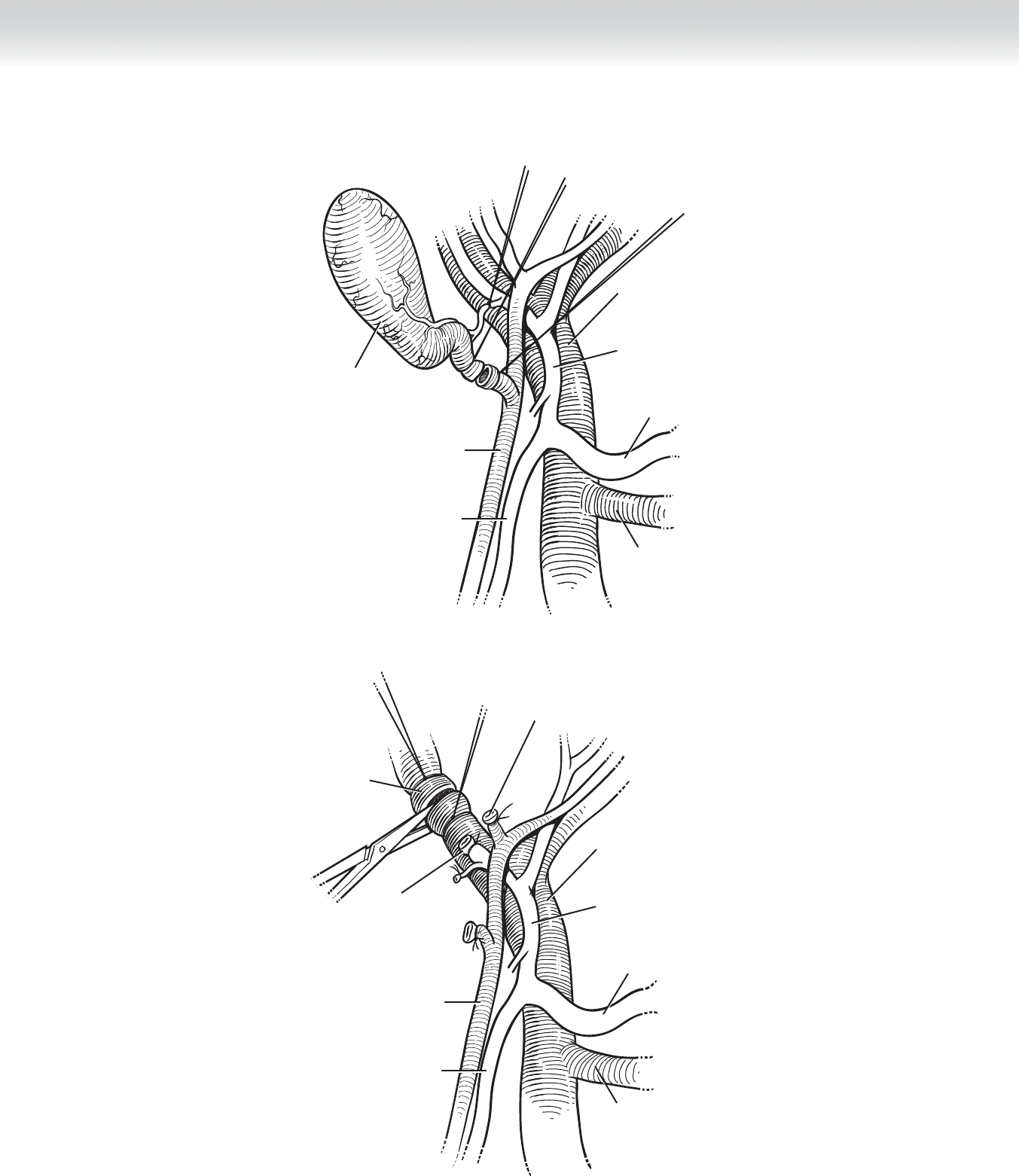
◆ Remove the gallbladder (Figure 45-8).
◆ At approximately the mid-portion of the hepatoduodenal ligament, dissect and isolate the
common bile duct laterally; the proper hepatic artery is located on the medial edge of the
ligament. Place a
1
⁄4-inch Penrose drain around the bile duct and a vessel loop around
the artery, and use traction laterally and medially on these two structures to reveal the por-
tal vein, positioned between and posterior to these two parallel structures. Gently tease the
fi lmy adhesions to isolate all three structures toward the hilum (Figure 45-9).
◆ Follow the common bile duct, hepatic artery, and portal vein toward the hilum of the liver,
and then isolate and encircle the right branch of each structure. Each of these will follow a
course directed toward the cystic plate, deep to the gallbladder bed (see Figure 45-9).
◆ By retracting the liver to the left, you expose the vena cava. Identify, ligate, and divide mul-
tiple small tributaries between the vena cava and the right lobe of the liver, permitting full
mobilization of the right liver.
◆ Interrupt vascular infl ow to the right liver by dividing the right hepatic artery between
clamps and suture ligating (see Figure 45-9).
◆ Divide the right branch of the portal vein between clamps. With the clamp in place, a contin-
uous running closure is performed with 5-0 Prolene, beginning at one corner. At the opposite
corner, lock the suture. Remove the clamp and place a second layer of continuous suture back
to the original corner and tie. Vascular staples may be substituted (see Figure 45-9).
◆ Divide and suture ligate the right branch of the hepatic duct using absorbable suture (see
Figure 45-9).
CHAPTER 45 • Right Hepatectomy 485
Common hepatic artery
Gallbladder removed
Common bile duct
Gastroduodenal artery
Portal vein
Splenic vein
Proper hepatic artery
Common hepatic artery
Common bile duct
Dividing right
portal vein
Right hepatic
duct divided
Right hepatic
artery divided
Gastroduodenal artery
Portal vein
Splenic vein
Proper hepatic artery
FIGURE 45 –8
FIGURE 45 –9
486 Section VI • Liver
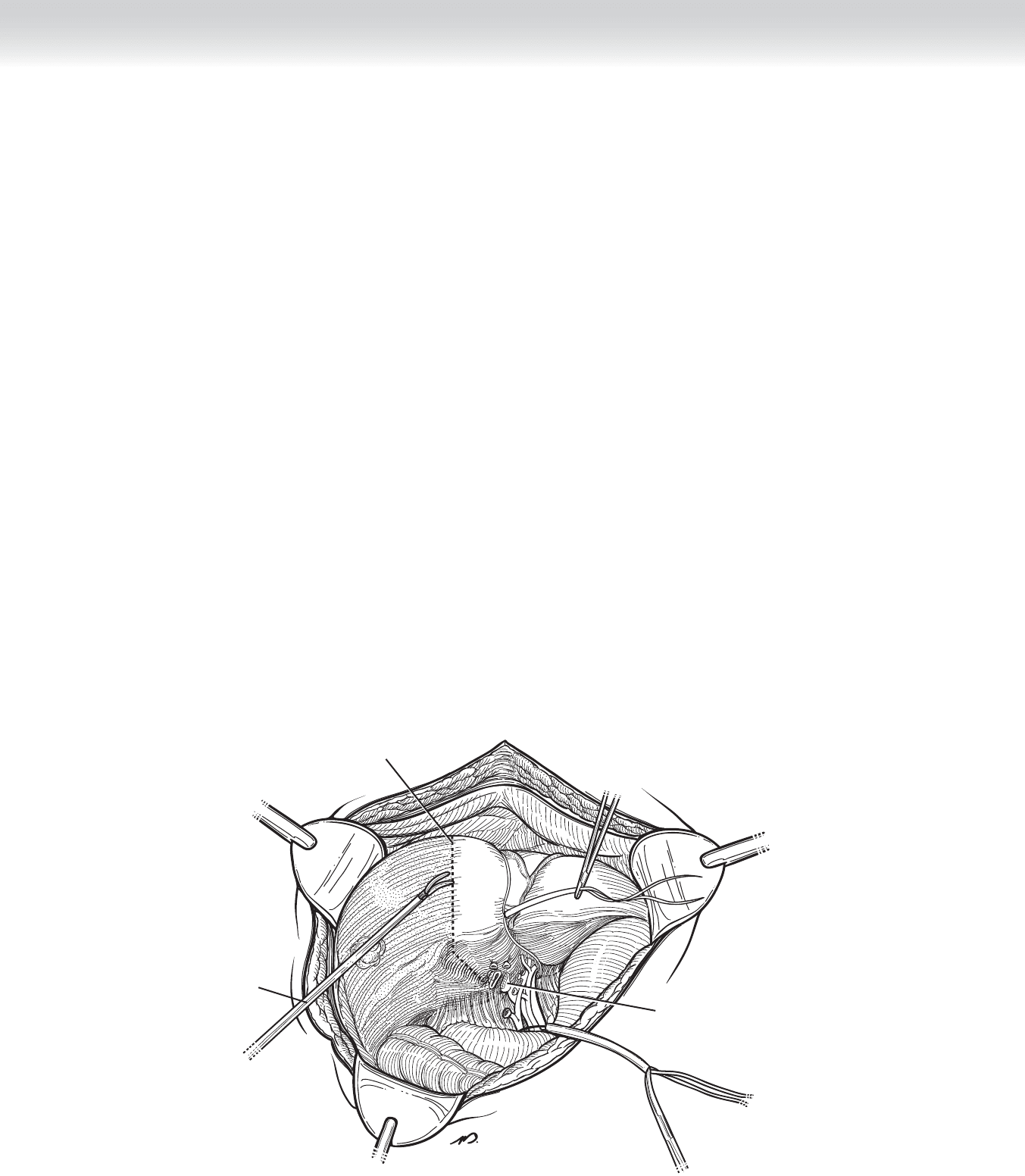
◆ Once the vascular infl ow is interrupted, the anatomic right liver assumes a dark purple hue,
giving it a clear demarcation for resection (Figure 45-10).
◆ Score the capsule of the liver along the line of demarcation using electrocautery.
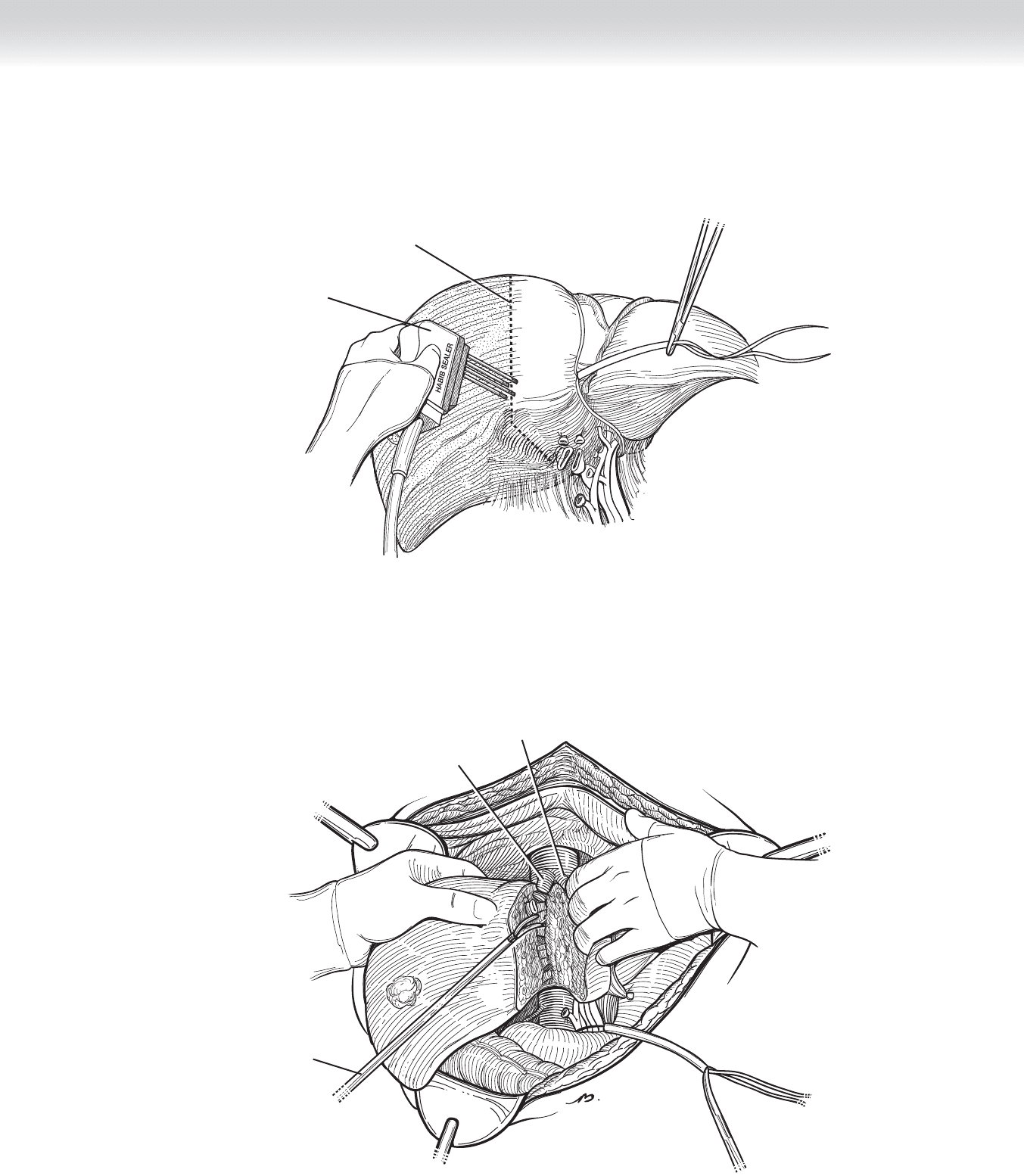
◆ Perform dissection through the parenchyma of the liver carefully and progressively using the
handheld harmonic dissector (see Figure 45-10). The recently available tissue-coagulating
instrument based on radio-frequency energy may be substituted for division of parenchyma
but should not be used near major vessels. The normal right lobe may be as deep in its ante-
rior to posterior dimensions as 20 cm. Patience must be exercised (Figure 45-11).
◆ Using visual inspection, and if necessary ultrasound guidance, identify major vascular tribu-
taries and branches, and then clamp, divide, and ligate. Biliary radicles, which must be
ligated individually, are most diffi cult to identify at the time of dissection. Failure to ligate
these structures results in postoperative bile leaks (Figure 45-12).
◆ Perform ultrasound examination intraoperatively to ensure adequate margin of resection in
the case of malignant tumor removal. A 1-cm margin is considered adequate, but in major
resections margins are not typically an issue.
◆ Extend division of the liver from the anterior to posterior capsule at the level of the vena cava.
Divided right portal vein
Harmonic
Demarcation line
FIGURE 45 –10
CHAPTER 45 • Right Hepatectomy 487
Habib sealer
Demarcation line
FIGURE 45 –11
Middle hepatic vein
Right hepatic vein
Harmonic
FIGURE 45 –12
488 Section VI • Liver
◆ Carry the dissection from the inferior edge of the liver to the superior edge, terminating at
the right hepatic vein. You might encounter tributaries within the parenchyma of the liver
before reaching the right hepatic vein. Throughout division of the parenchyma of the liver,
repeatedly reorient the specimen to be certain that dissection is not migrating toward the
left liver and more importantly toward the major vascular structures necessary for the left
liver’s viability (Figure 45-13, and see Figure 45-12).
◆ Double clamp the right hepatic vein on the vena cava side. Divide the right hepatic vein.
Close the stump of the right hepatic vein using running 5-0 Prolene suture in an identical
manner to that used on the portal vein (Figure 45-13 and Figure 45-14).
◆ Bring out two 10-mm Jackson-Pratt drains through separate stab wounds on the right side
of the abdomen and place along the divided edge of the liver. Some will advocate taking
omentum and placing it in the right upper quadrant to act as a biologic seal for the raw
edge of the liver parenchyma (Figure 45-15).
Right hepatic vein divided
FIGURE 45 –13
CHAPTER 45 • Right Hepatectomy 489
Middle hepatic vein
Right hepatic vein sewn
FIGURE 45 –14
Closed suction
drains
FIGURE 45 –15

490 Section VI • Liver
3. CLOSING
◆ Close the abdomen in a standard manner. We favor Smead-Jones closure with heavy-gauge
absorbable suture.
STEP 4: POSTOPERATIVE CARE
◆ In the fi rst 24 hours after surgery, the primary concern is hemorrhage and the related mea-
sure of coagulation status. These should be monitored by serial measurement of hemoglo-
bin and coagulation factors.
◆ In all major resections, particularly in patients with cirrhosis, one must be vigilant for any
signs of hepatic failure. A particularly ominous fi nding is the progressive rise in bilirubin
level with an enzyme pattern that supports neither obstruction nor parenchymal cell death,
such as transaminase elevations. The most ominous fi nding is a plummeting serum glucose
level, which refl ects the loss of glycogen stores in the liver and by inference the loss of via-
ble liver. Unfortunately, there is little one can do to reverse this pattern of failure. One pos-
sible cause is inadequate remaining liver after resection. This can resolve over time as the
liver regenerates, which it will do to some degree.
◆ One possible remediable cause of this progressive demise is thrombus formation in the por-
tal vein. This would seem to be unlikely, because coagulation is typically inadequate in
these patients, but we have seen this phenomenon. It is possible that lysis of this clot may
restore vital fl ow.
◆ Sepsis is particularly metabolically taxing to the liver. In the compromised postoperative
liver, sepsis can be catastrophic, and one should monitor and obtain cultures if necessary to
prevent infectious processes from progressing.
◆ Ascites may form, and one must be aware when this phenomenon has occurred and treat as
one would normally treat this entity with careful and judicious use of salt-containing intra-
venous fl uids and with diuresis.
◆ Remove drains if no bile is seen in the effl uent.
◆ One preoperative option, which was originally developed for cirrhotic patients with what
appeared to be inadequate functional reserve but later applied to all candidates, is emboli-
zation of the portal vein. In this manner some degree of the regeneration of lost liver takes
place before the stress of surgery is added.

CHAPTER 45 • Right Hepatectomy 491
STEP 5: PEARLS AND PITFALLS
◆ As with all major operative procedures, one must be extremely careful with patient selection.
◆ If hemorrhage occurs at any time during the procedure, the liver can be compressed into
the spine or into the right fl ank to gain control, and another capable surgeon can be called
for assistance.
◆ Before dividing any of the major vascular structures, stop and reconfi rm that the proper
structure is being divided.
◆ If ascites forms and the drains are still in place, excessive electrolyte and fl uid loss can occur
through actively draining liters of fl uid per day. In this setting, the drains (assuming they are
not bile tinged) should be removed, and the skin overlying the drain tract should be sutured.
SELECTED REFERENCES
1. Blumgart LH, Belghiti J: Liver resection for benign disease and for liver and biliary tumors. In
Blumgart LH (ed): Surgery of the Liver, Biliary Tract and Pancreas, 4th ed. Philadelphia, Saunders
Elsevier, 2007, pp 1341-1388.
2. Liu CL, Fan, ST, Cheung ST, et al: Anterior approach versus conventional approach right hepatic resection
for large hepatocellular carcinoma: A prospective randomized controlled study. Ann Surg 2006;244:
194-203.