Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

514 Section VII • Pancreas
◆ Careful dissection of the retroperitoneum will permit mobilization between the kidney and
the adrenal glands posteriorly and the spleen and the tail of the pancreas anteriorly. After
this has been done, there is typically a vascular attachment at the inferior border of the pan-
creas between the spleen and the splenic fl exure of the colon. This should be divided
between clamps and tied using 3-0 or 2-0 silk ties. At the same time, the vascular attach-
ments between the greater curvature of the stomach at the fundus and the spleen, the short
gastric vessels, are divided between clamps and tied using 2-0 and 3-0 silk ties. Caution
should be taken not to place a tie on the wall of the stomach, because this may result in a
necrosis of the greater curvature. After this amount of mobilization, it should be possible to
separate completely the spleen and the tail of the pancreas from its retroperitoneal attach-
ments further toward the midline. Typically this dissection is carried until one has reached a
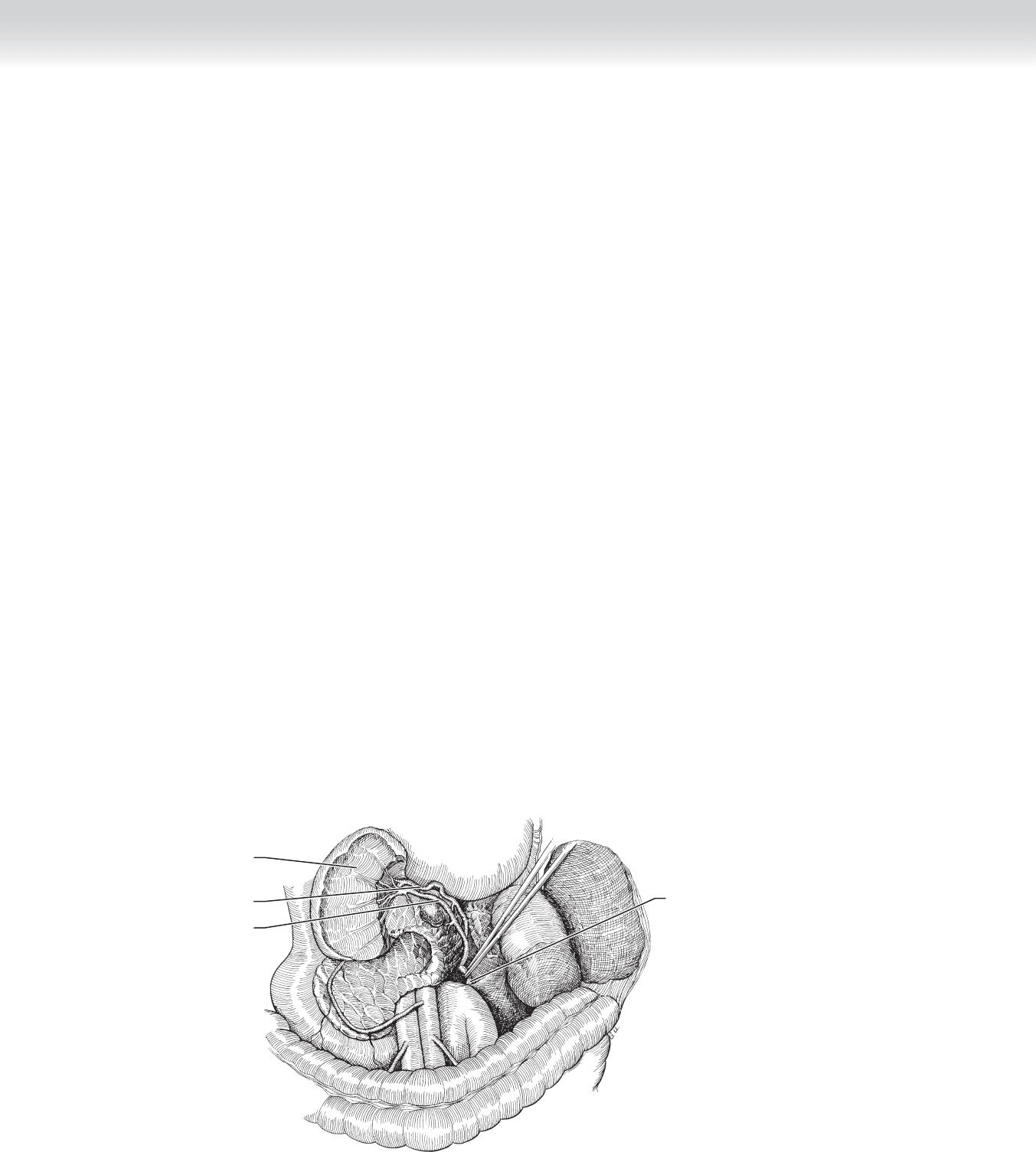
minimum of 3 cm medial to the mass that is anticipated for resection (Figure 47-5).
◆ At this point, the decision needs to be made regarding preservation of the spleen. If no
plans are made to preserve the spleen, it should be possible to separate and ligate the
splenic artery and the splenic vein. One must always divide the artery before dividing the
vein to prevent any engorgement and bleeding of the spleen that would result from dividing
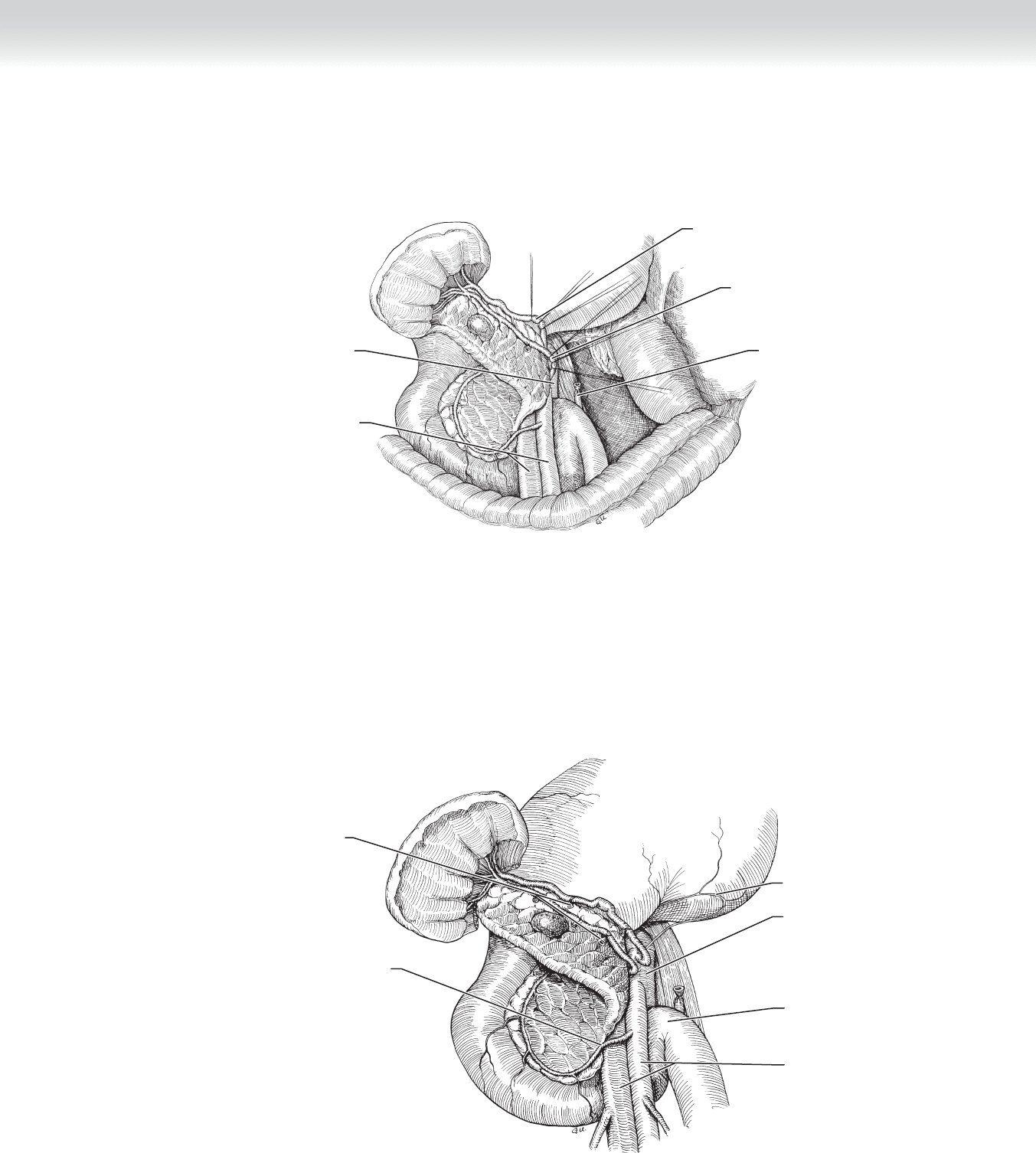
the vein fi rst (Figure 47-6).
◆ If one is planning on preserving the spleen, then the small vascular attachments between
the splenic artery and the tail of the pancreas and body of the pancreas and between the
splenic vein and the body and tail of the pancreas must be carefully divided and tied using
3-0 silk ties. It is during this dissection that one may conclude that a splenectomy is safer
than the hemorrhage that could at times result from this dissection in a patient who has
had a signifi cant history of pancreatitis (Figure 47-7).
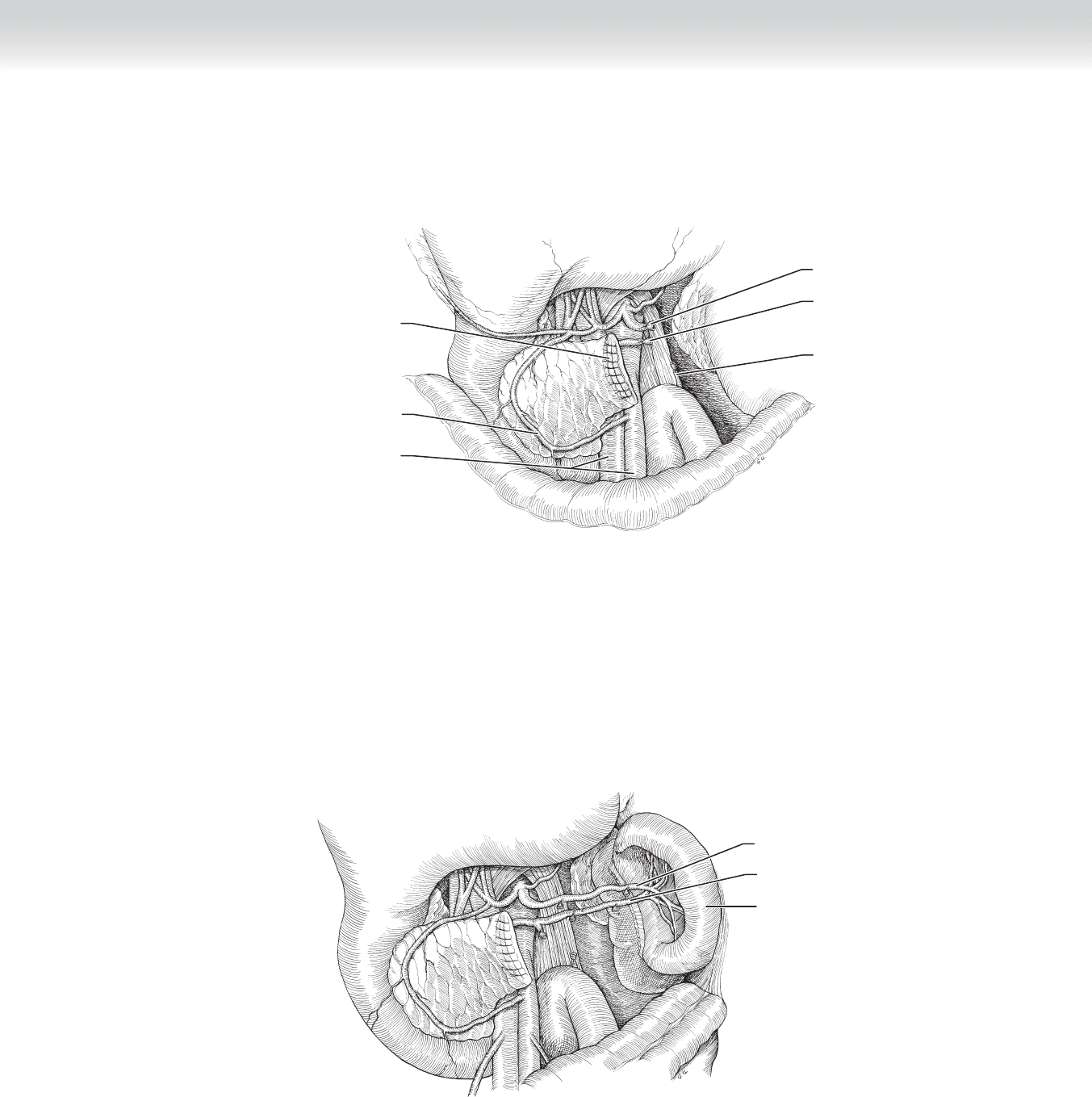
Inferior mesenteric vein
Spleen
Splenic artery
Splenic vein
FIGURE 47 –5
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 515
Aorta
Superior mesenteric
artery and vein
Splenic artery ligation with
double ties on proximal side
Splenic vein ligation with
double ties on proximal side
Inferior mesenteric vein
FIGURE 47 –6
Splenic artery branches and
vein tributaries ligated
Inferior pancreaticoduodenal artery
Left gastric artery
Duodenojejunal junction/
Ligament of Treitz
Aorta
Superior mesenteric
artery and vein
FIGURE 47 –7

516 Section VII • Pancreas
◆ At this point, one should have separated the tail of the pancreas from the splenic artery and
vein or should have divided the splenic artery and vein, and the only remaining attachments
should be the parenchyma of the pancreas. We prefer a fi sh mouth opening to the body of
the pancreas. This involves angling at approximately 45 degrees toward the head of the pan-
creas, along the anterior border of the body of the pancreas to approximately half the depth
of the body of the pancreas. We then go to 90 degrees in the opposite direction, again with a
45-degree angulation, and incise toward the tail of the pancreas. This permits apposing the
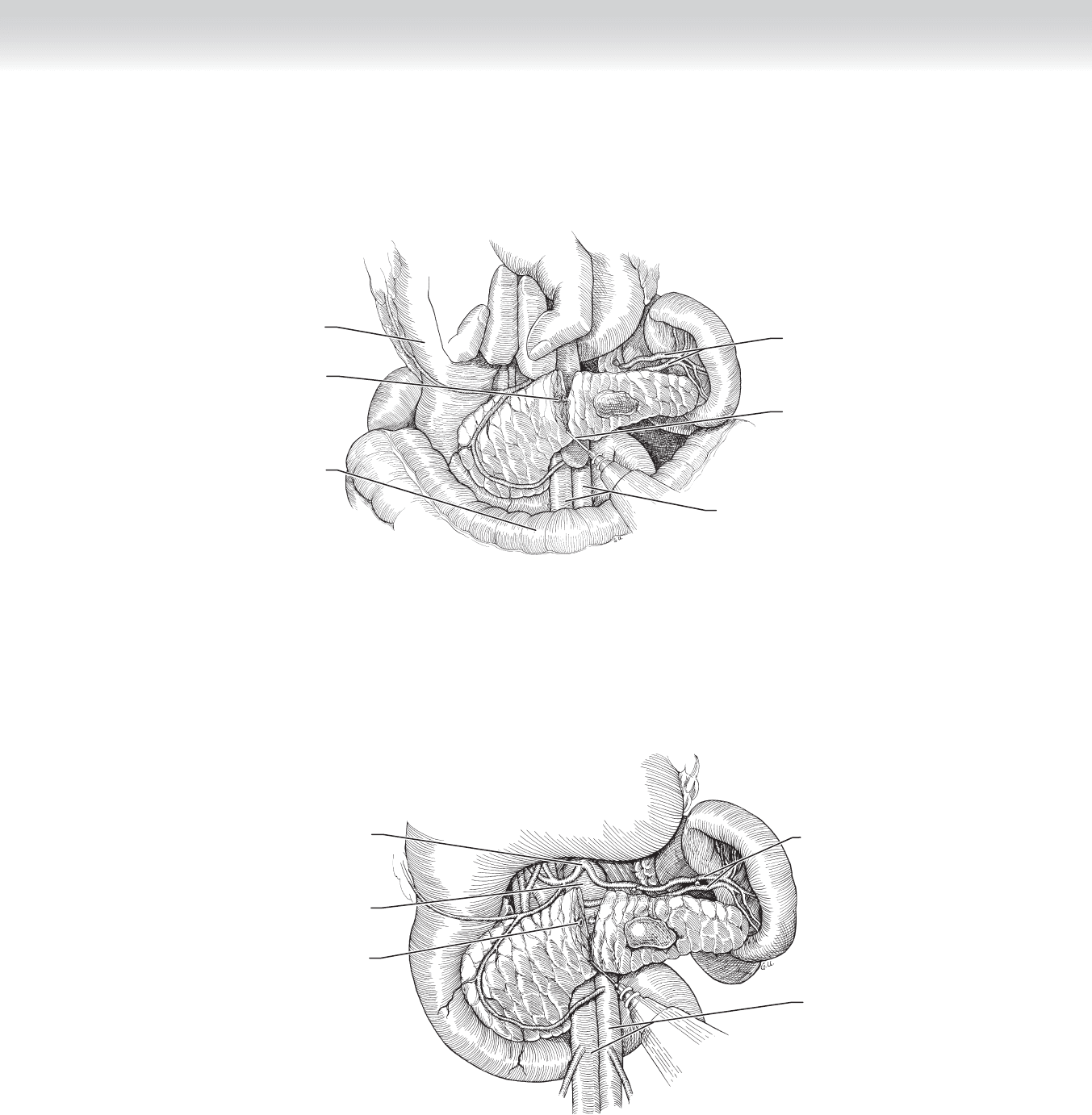
ends of the divided pancreas in the hopes of preventing a pancreatic fi stula (Figure 47-8).
◆ At this point, one must carefully identify the pancreatic duct. This may be accomplished by
gently massaging the body of the pancreas and expressing pancreatic juice through the pan-
creatic duct. In certain patients, particularly patients with a normal pancreas, the pancreatic
duct can be quite miniscule. The duct is ligated with a 4-0 Prolene stitch (Figure 47-9).
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 517
Electrocautery of pancreas
Stomach
Transverse colon
Pancreatic duct ligated
Splenic artery and vein ligated
Superior mesenteric artery and vein
FIGURE 47 –8
Splenic artery and vein
Superior mesenteric
artery and vein
Pancreatic duct ligated
Aorta
Celiac trunk
FIGURE 47 –9
518 Section VII • Pancreas
◆ After the pancreatic duct is ligated, the anterior and posterior portions of the fi sh mouth cre-
ated by dividing the body of the pancreas are reapproximated using interrupted 2-0 Prolene
sutures. After this is completed, the area is irrigated and two drains are placed in the retro-
peritoneum, just lateral of the divided body of the pancreas. This closure is identical for
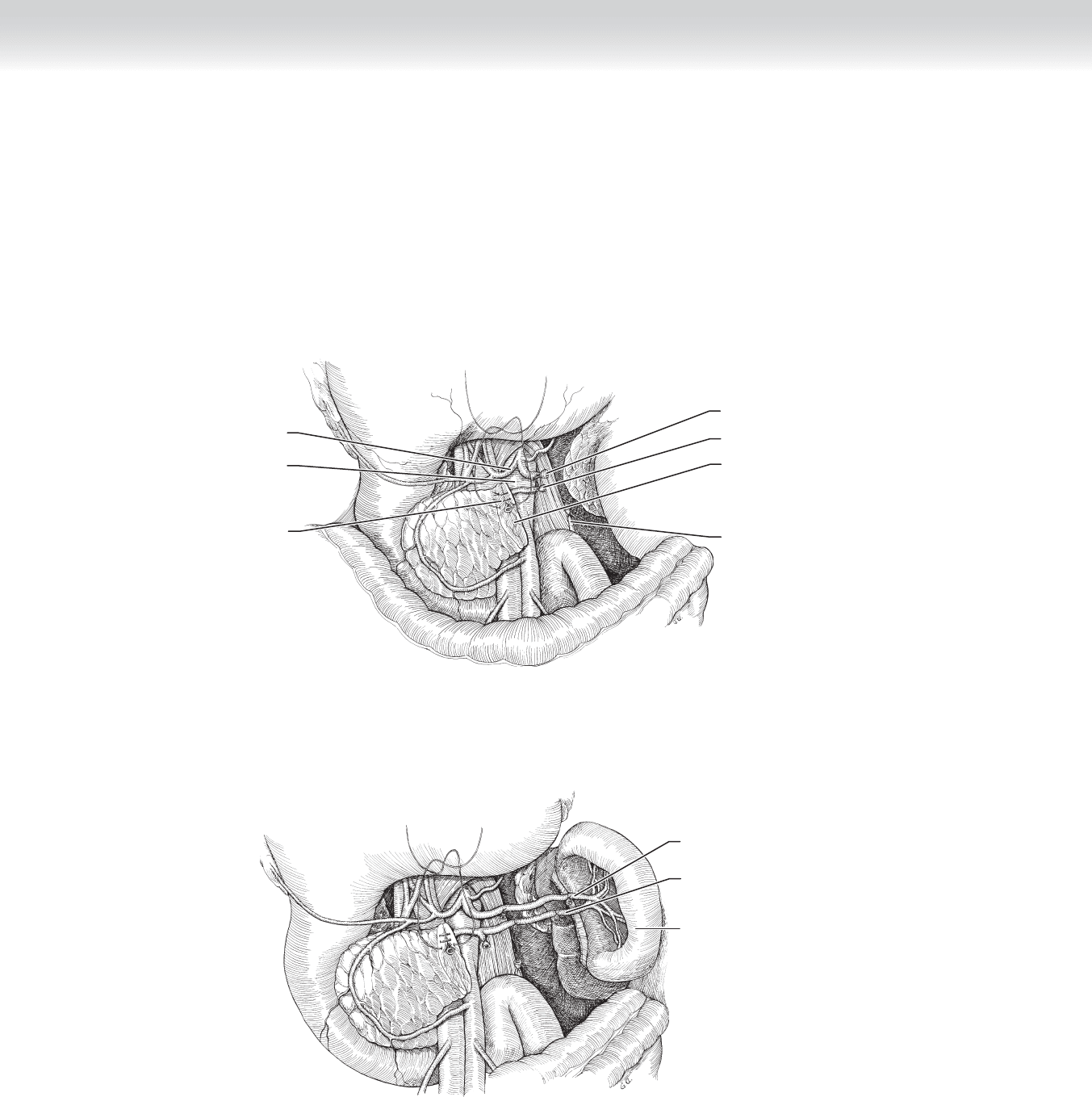
patients who have had splenectomy or splenic preservation (Figures 47-10 through 47-13).
Inferior mesenteric vein
“Fish mouth” division of the
body of pancreas
Splenic artery
Splenic vein
Aorta
Common hepatic artery
Interrupted sutures
FIGURE 47–10
Splenic vein
Spleen in situ
Splenic artery
FIGURE 47–11
CHAPTER 47 • Distal Pancreatectomy and Splenectomy 519
Splenic vein
Sutured closure of
pancreatic remnant
Inferior mesenteric vein
Superior mesenteric artery and vein
Splenic artery
Pancreaticoduodenal artery
FIGURE 47–12
Splenic vein
Splenic artery
Spleen in situ
FIGURE 47–13

520 Section VII • Pancreas
3. CLOSING
◆ The abdomen and skin are closed in the usual fashion. The drains are placed to closed bulb
suction.
STEP 4: POSTOPERATIVE CARE
◆ Monitor blood glucose and urine glucose.
◆ Monitor amylase and lipase levels to detect postoperative pancreatitis.
◆ Monitor platelet count to detect postoperative thrombocytosis.
◆ One may consider keeping a nasogastric tube in place after this procedure. There has tradi-
tionally been a concern that a dilated stomach may undermine the sutures along the short
gastric vessels. More recent practice has endorsed very brief use of such tubes.
◆ Monitor the drain outputs, and particularly examine them for amylase levels beginning on
day 4 or after a regular diet has been resumed to detect pancreatic fi stula.
STEP 5: PEARLS AND PITFALLS
◆ It is important to recognize that all signifi cant vascular infl ow to the spleen comes along the
splenic artery. For that reason, early isolation of the splenic artery may well maintain control
in the event that signifi cant hemorrhage occurs during the attempted resection. Particularly
with postinfl ammatory changes, the dissection along the spleen and the tail of the pancreas
may be fraught with potential hemorrhage, and much of this can be prevented by taking early
control of the splenic artery.
◆ Although we do not currently recommend additional measures preoperatively, one should be
prepared for the possibility of pancreatic fi stula, and we therefore take very seriously the liga-
tion of the divided main pancreatic duct in the pancreatic remnant. We particularly make an
effort to have good tissue apposition by the closure of our body of the pancreas. It is also
quite important to remove the drains after this operation only when one is certain that they
have been functioning and that they no longer have any signifi cant output. It is unfortunately
well known that one may remove a drain because he or she believes the drain outputs have
ceased when they have simply stopped because of drain failure. In this event, one may require
interventional radiology to help with proper drainage.

CHAPTER 47 • Distal Pancreatectomy and Splenectomy 521
SELECTED REFERENCES
1. Blumgart LH, Belghiti J: Liver resection for benign disease and for liver and biliary tumors. In Blumgart LH
(ed): Surgery of the Liver, Biliary Tract and Pancreas, 4th ed. Philadelphia: Saunders, 2007, pp 1341-1388.
2. Sugiyama M, Suzuki Y, Abe N, et al. Modifi ed liver hanging maneuver with extraparenchymal isolation of
the middle hepatic vein in left hepatectomy. J Hepatobiliary Pancreat Surg 2009;16:156-159.
3. Shirabe K, Shimada M, Gion T, et al. Postoperative liver failure after major hepatic resection for hepatocel-
lular carcinoma in the modern era with special reference to remnant liver volume. J Am Coll Surg
1999;188:304-309.

522
STEP 1: SURGICAL ANATOMY
◆ All pancreatic surgery requires an understanding of the anatomic relationships in the lesser
sac. After either an upper midline or a bilateral subcostal (chevron) incision, one enters the
lesser sac by dissecting along the avascular plane at the points of attachment of the gastro-
colic omentum to the transverse colon. The proper plane is between the anterior and poste-
rior leafl ets. This is my favored point of entry. The alternative entry is by dividing and ligat-
ing, in a transverse direction, the vascular structures embedded in the omentum while
preserving the gastroepiploic vessels located along the greater curvature of the stomach.
◆ Upon entering the lesser sac, one will encounter varying amounts of infl ammatory adhesions
between the posterior wall of the stomach and the anterior surface of the pancreas. Consid-
erable dense adhesions may be encountered in the background of chronic pancreatitis.
◆ The pancreas is essentially encased in a sandwich of major blood vessels. The vena cava and
aorta occupy the posterior surface in the midline. The splenic artery courses along the superior
surface from the aorta toward the tail. The splenic vein occupies the posterior superior surface
of the body and tail of the pancreas. It meets the superior mesenteric vein, which is oriented
vertically in the groove created by the uncinate process in the posterior aspect of the head of
the pancreas and the right lateral and anterior components of the head. The confl uence of
these two veins constitutes the portal vein, which traverses the uncinate groove encased by the
head of the pancreas and emerges to join the bile duct and the hepatic artery in the hepatoduo-
denal ligament.
◆ The superior mesenteric artery is located in a plane posterior and slightly medial to the supe-
rior mesenteric vein. The common hepatic artery, a branch of the celiac trunk (along with the
splenic artery and left gastric artery), courses along the superior border of the head of the pan-
creas to join the hepatoduodenal ligament. Its fi rst branch is the typically miniscule right gas-
tric artery. Just distal is the more substantial gastroduodenal artery, which emerges at a right
angle to the hepatic artery from its inferior surface and courses beneath the pylorus, and after
sending the right gastroepiploic artery in the plane between the inferior aspect of the pylorus
and the superior surface of the head of the pancreas, the gastroduodenal artery pierces the head
of the pancreas.
◆ The anterior superior and the posterior superior pancreaticoduodenal arteries also arise from
branches of the gastroduodenal artery. These arteries form an arch medial to the C-loop of
the duodenum, and they collateralize with branches of the anterior and posterior inferior
CHAPTER
48
Beger and Frey Procedures
William H. Nealon

CHAPTER 48 • Beger and Frey Procedures 523
pancreaticoduodenal arteries, which are branches of the superior mesenteric artery. Small
branches from these arteries provide blood supply to the duodenum. Both the Beger and
Frey procedures include division of these anterior vessels. Preservation of the posterior
arcade ensures viability of the duodenum.
◆ Key anatomic features in pancreatic head resections and in the Beger and Frey procedures
are the network of tributaries projecting between the superior mesenteric vein/portal vein
confl uence and the uncinate process. These tributaries are located at the right lateral aspect
of the veins. These tiny veins exit the pancreas at the mid-portion of the groove in which
the major veins reside.
◆ The pancreas is entirely retroperitoneal, and therefore operative procedures will require mobi-
lization of the pancreas from its retroperitoneal position. The plane lateral to the C-loop of the
duodenum is incised in nearly all procedures; this plane is avascular, and its mobilization is
termed the Kocher maneuver. This exposes the vena cava and aorta, and it permits “bimanual
palpation” of the head of the pancreas. The dissection may be easily extended to the fourth
portion of the duodenum and the ligament of Treitz (see Figure 48-3).
◆ The inferior border of the body of the pancreas is also avascular, although the inferior mes-
enteric vein may be encountered to the right of the spine.
◆ Peritoneum overlies the hepatoduodenal ligament. Dissection reveals the triad in gross ana-
tomic terms, which corresponds to the microscopic portal triad—with portal venous, hepatic
arterial, and biliary structures. The common bile duct is located in an anterior lateral posi-
tion, and the hepatic artery is anterior medial. The portal vein is positioned in the posterior
groove created by the apposition of these anterior structures (see Figure 48-5).
◆ On the inferior border of the pancreatic head, just where the duodenum dives beneath the
superior mesenteric vein and artery, one may dissect the peritoneum and visualize the supe-
rior mesenteric vein as it passes superiorly beneath the head of the pancreas.
◆ The main pancreatic duct originates in the tail of the pancreas and traverses the length of
the pancreas to exit in the duodenum through both main ampulla (Vater) and the accessory
ampulla, which is located more proximally in the duodenum. The main pancreatic duct
(Wirsung) and the minor or accessory duct (Santorini) fuse during fetal development at
what is termed the genu or “knee” of the duct.
INDICATIONS
◆ The indication for surgery in all patients with chronic pancreatitis is essentially the same.
The most common indication for surgery is chronic unremitting abdominal pain.
◆ A second indication for surgery in chronic pancreatitis is episodes of recurrent, acute exac-
erbations, either alone or combined with constant pain.