Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 56 • Loop Colostomy 637
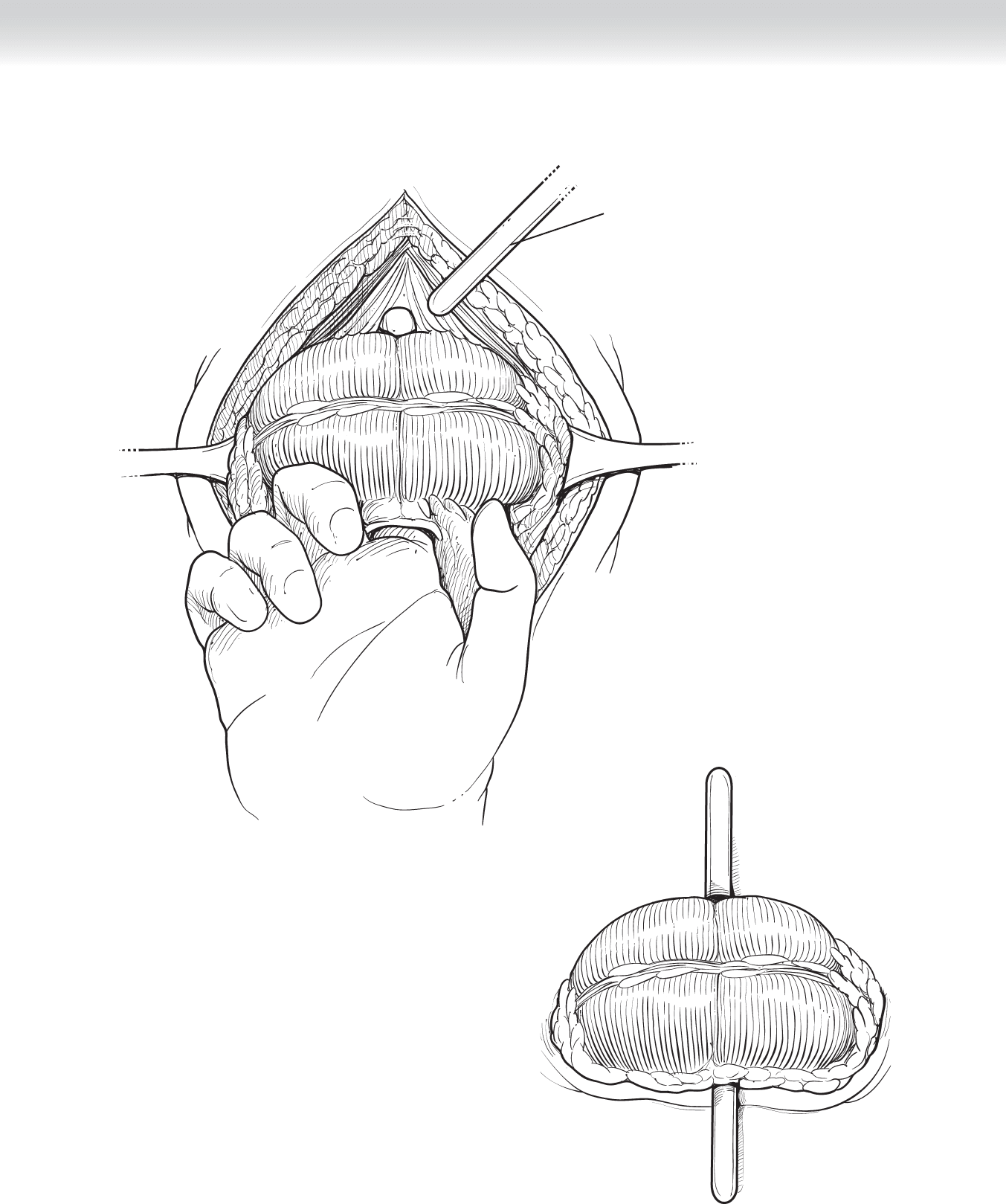
Glass or plastic rod
FIGURE 56 –2
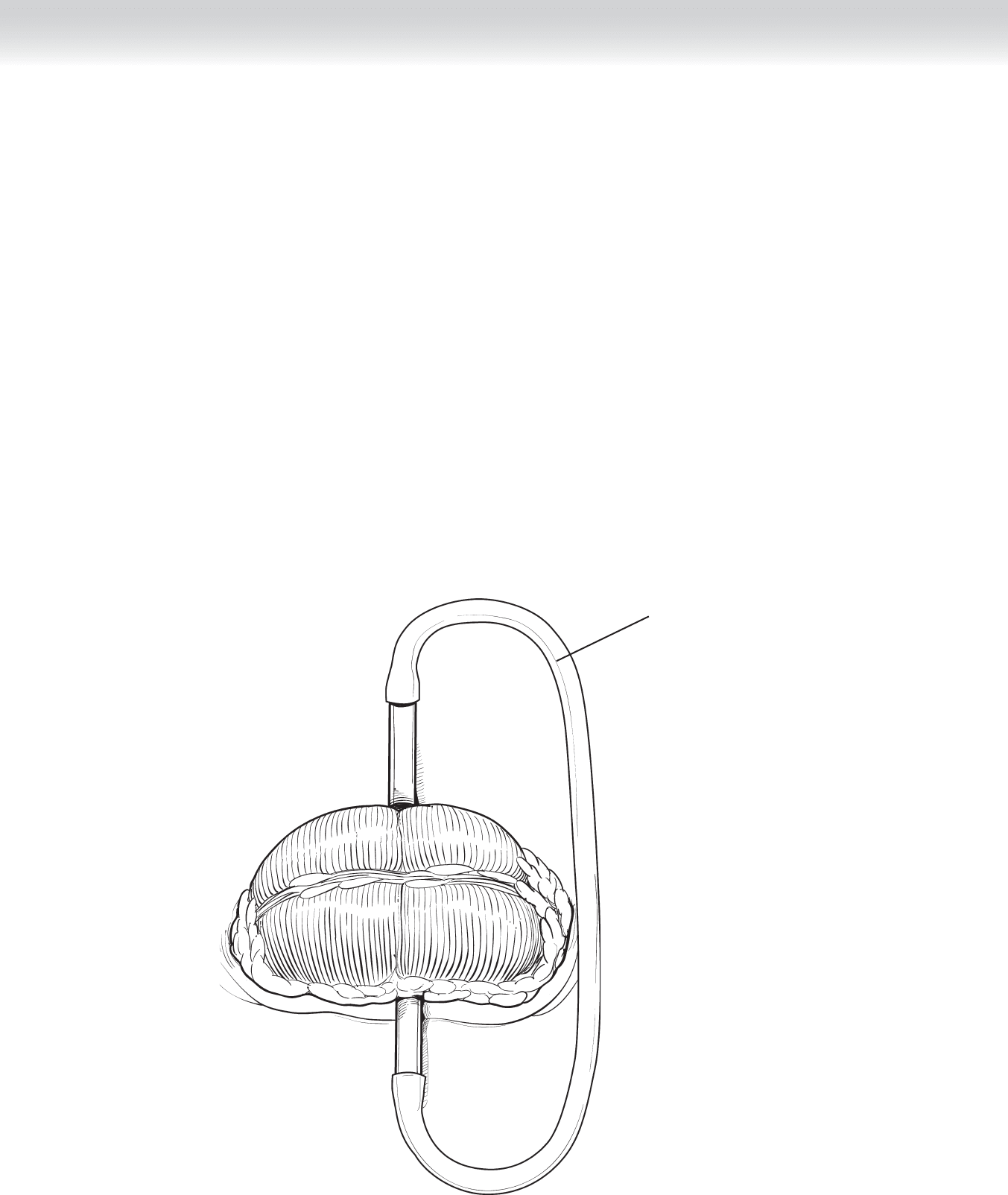
FIGURE 56 –3
638 Section IX • Colon
◆ Secure the rod in place by attaching tube catheter to each end of the rod circling over the
colon (Figure 59-4).
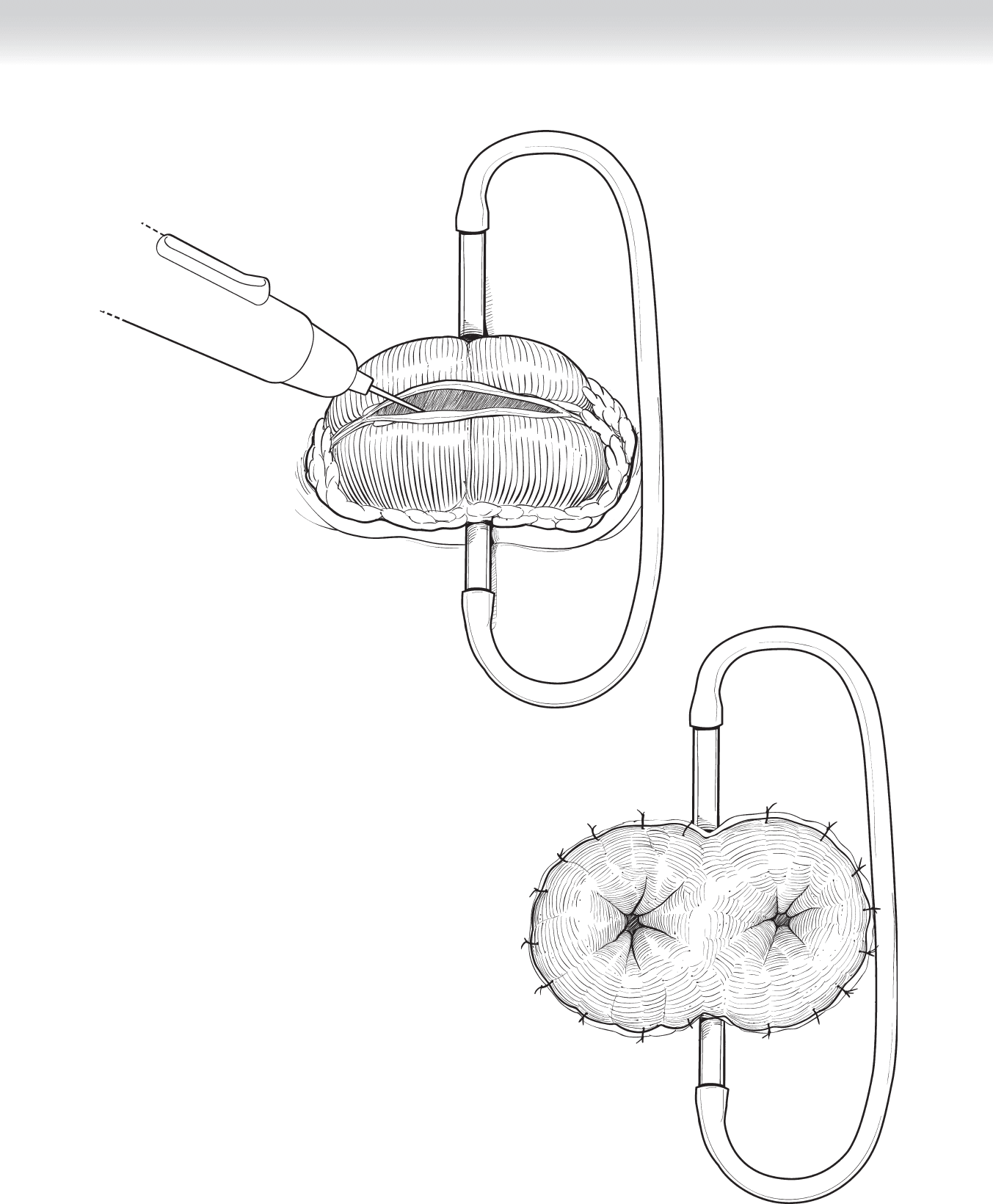
◆ The colotomy is performed with electrocautery along the taenia coli (Figure 56-5).
◆ Edges of the colotomy are secured to the edges of the incision with multiple 3-0 Vicryl
sutures (Figure 56-6).
Tube catheter
FIGURE 56 –4
CHAPTER 56 • Loop Colostomy 639
FIGURE 56 –6
FIGURE 56 –5

640 Section IX • Colon
3. CLOSING
◆ Routine
STEP 4: POSTOPERATIVE CARE
◆ Provide routine ostomy care.
◆ The plastic rod can be removed once the surgical site has healed, which is usually approxi-
mately 2 weeks.
STEP 5: PEARLS AND PITFALLS
◆ Omentum and pericolic fat precludes solid healing of the colostomy to the incision. It is
best to trim fat. However, use caution and vigilance in ensuring hemostasis on retracted
omentum and mesenteric fat.

641
STEP 1: SURGICAL ANATOMY
◆ The surgeon should be familiar with the anatomy of the double-barrel or looped stoma.
◆ Fascial closure of the abdominal wall after stoma takedown requires knowledge of the anat-
omy of the fascial relationship to the rectus abdominis muscle. Below the arcuate line, the
posterior wall of the rectus sheath is absent, and the rectus muscle lies on thin transversalis
fascia. Thus recognition and closure of the anterior rectus fascia is signifi cantly important in
preventing postoperative incisional hernia in patients with stomas below the umbilicus.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Reestablishment of intestinal continuity should take into consideration the original condi-
tion for which the diversion was created. Appropriate preoperative imaging and diagnostic
studies should be obtained to establish the safety of reversal.
◆ Wrapping the stoma with Seprafi lm, a sodium hyaluronate–based bioresorbable membrane
that prevents adhesions during the initial surgery, allows for easier takedown later, and a
midline incision should be avoided.
◆ Informed consent should include potential complications, such as anastomotic stricture or
leak, bowel obstruction, wound infection at the former stoma site, intra-abdominal wound
infection, hematoma, injury to adjacent bowel or mesentery, incisional hernia, and the need
for re-creation of the ostomy.
CHAPTER
57
Stoma Takedown: Takedown
of Loop Colostomy
or Ileostomy
Valerie P. Bauer
642 Section IX • Colon
◆ The type of bowel preparation is determined by the location of the stoma and the surgeon’s
preference.
◆ Loop ileostomy requires clear liquid the day before and a bottle of magnesium citrate the
night before surgery.
◆ Loop colostomy requires clear liquid the day before and Fleet enema before surgery.
Mechanical bowel preparation is no longer favored for this procedure.
◆ Appropriate preoperative parenteral antibiotics are administered within 1 hour before cut
time, according to the Physician Quality Reporting Initiative (PQRI) measures defi ned for
elective colorectal operations. We use ertapenem (Invanz) 1 g intravenously (IV) without re-
dosing, because it has 24-hour duration of action.
◆ Patients who have been taking steroids preoperatively should receive a stress dose of hydro-
cortisone 100 mg IV before the operation. This should be continued postoperatively and ta-
pered accordingly.
STEP 3: OPERATIVE STEPS
◆ The patient is placed supine on the operating table with arms outstretched on armboards.
◆ After general endotracheal anesthesia is administered, a Foley catheter is placed along with
sequential compression devices on the lower extremities.
◆ The ostomy appliance is removed and the abdomen is shaved as needed with clippers.
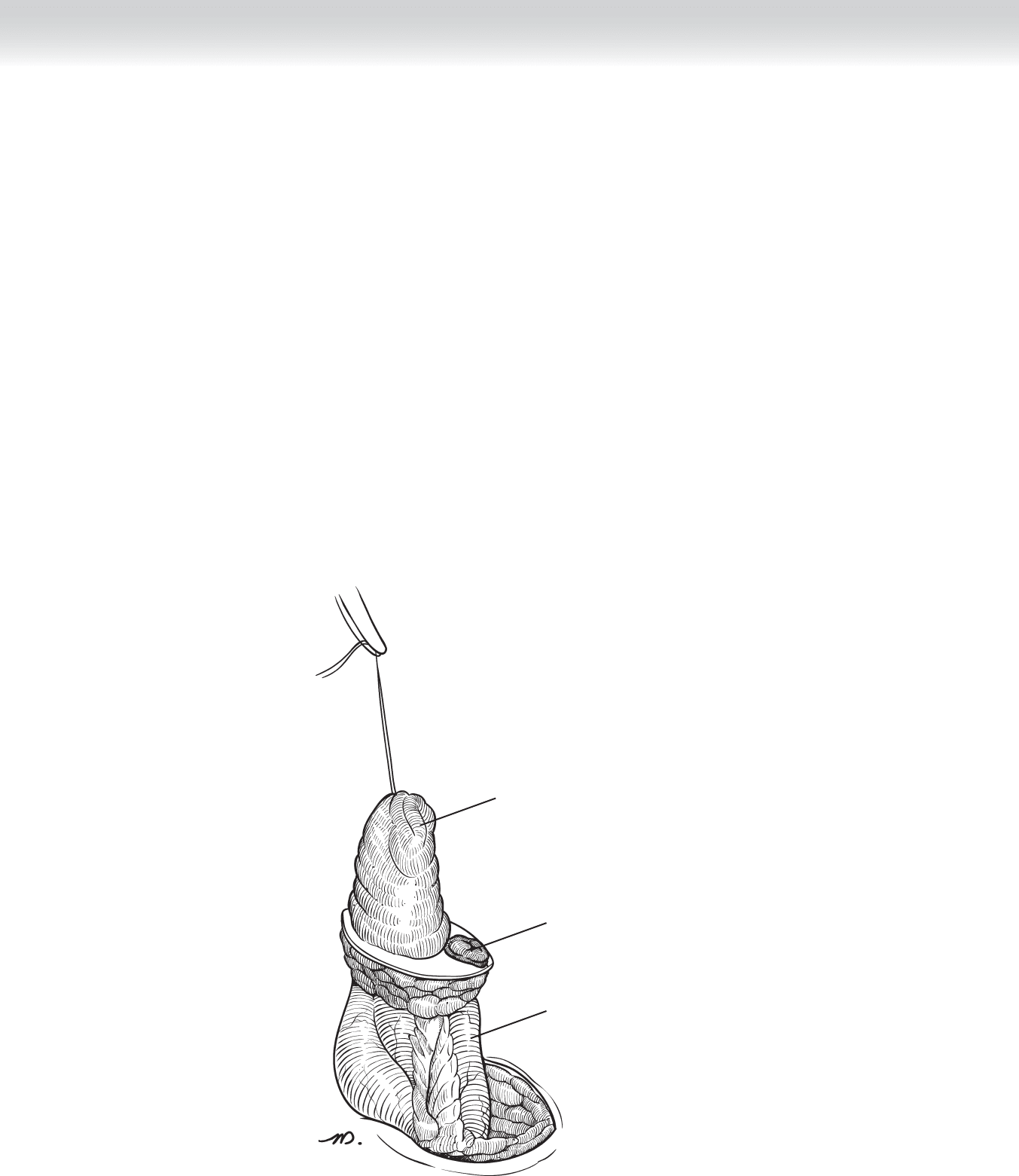
◆ The abdomen is prepped and draped, and a 2-0 Vicryl suture is used to close the proximal
loop of the stoma (Figure 57-1).
FIGURE 57 –1
CHAPTER 57 • Stoma Takedown: Takedown of Loop Colostomy or Ileostomy 643
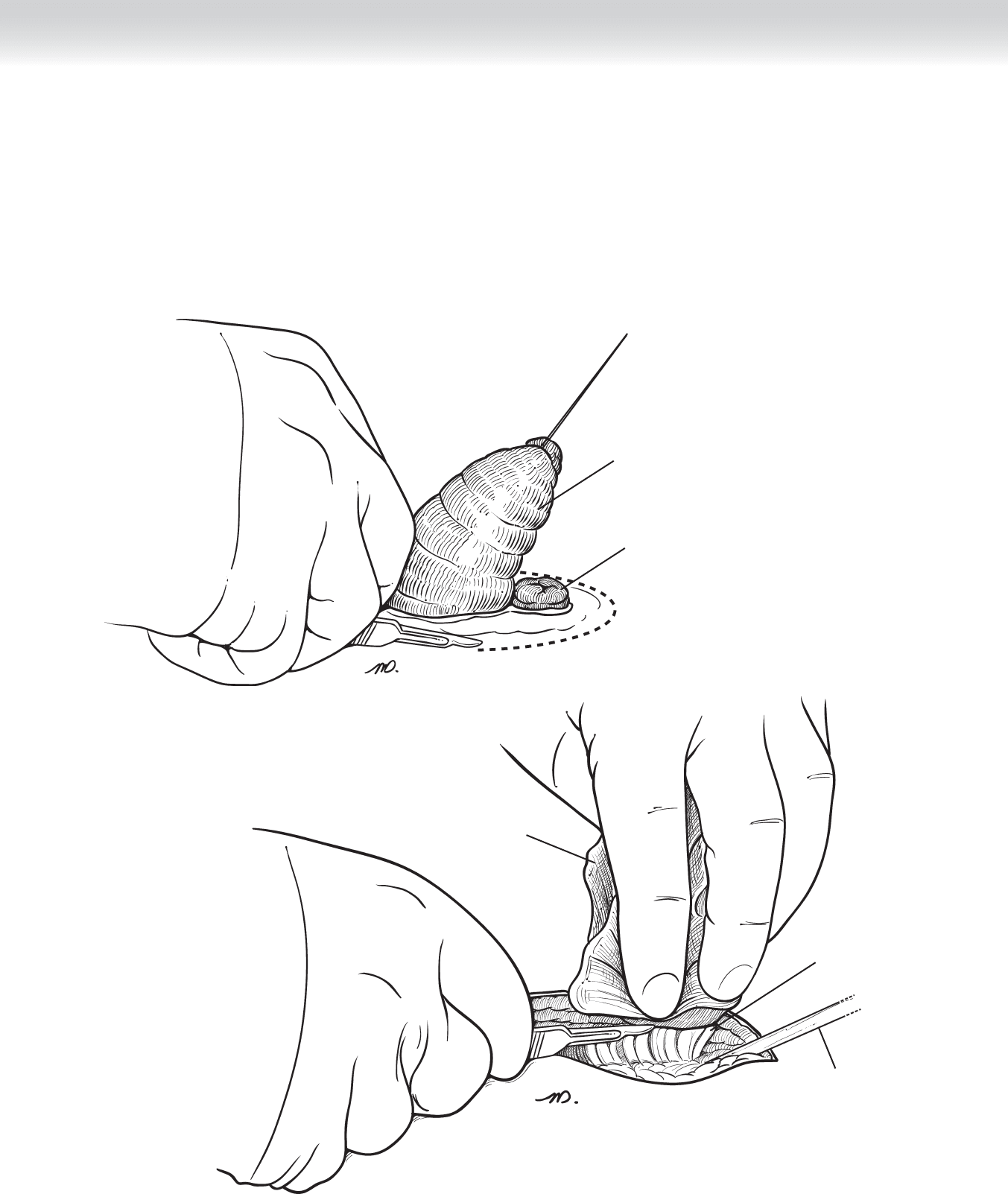
◆ A no. 15 blade knife is used to make an elliptical incision parallel to the skin lines but staying close
to the edge of the ostomy. The incision is carried vertically down to the anterior abdominal fascia
(Figure 57-2). Figure 57-2 shows an elliptical incision through the skin.
◆ Once the white line of fascia is identifi ed, it is retracted away from the plane of dissection. The
knife is drawn gently toward the bowel circumferentially and the peritoneum is cut (Figure 57-3).
Figure 57-3 shows a circumferential dissection around the stoma.
Soft tissue/
subcutaneous fat
Richardson
retractor
Barrel loop
FIGURE 57 –3
Proximal bowel
Distal bowel
FIGURE 57 –2
644 Section IX • Colon
◆ As the stoma is lifted up, care is taken to ensure that the mesentery is not cut or ripped.
Excess traction can cause tears leading to unrecognized intra-abdominal bleeding
(Figure 57-4). A Richardson retractor is used for circumferential exposure to free the
stoma.
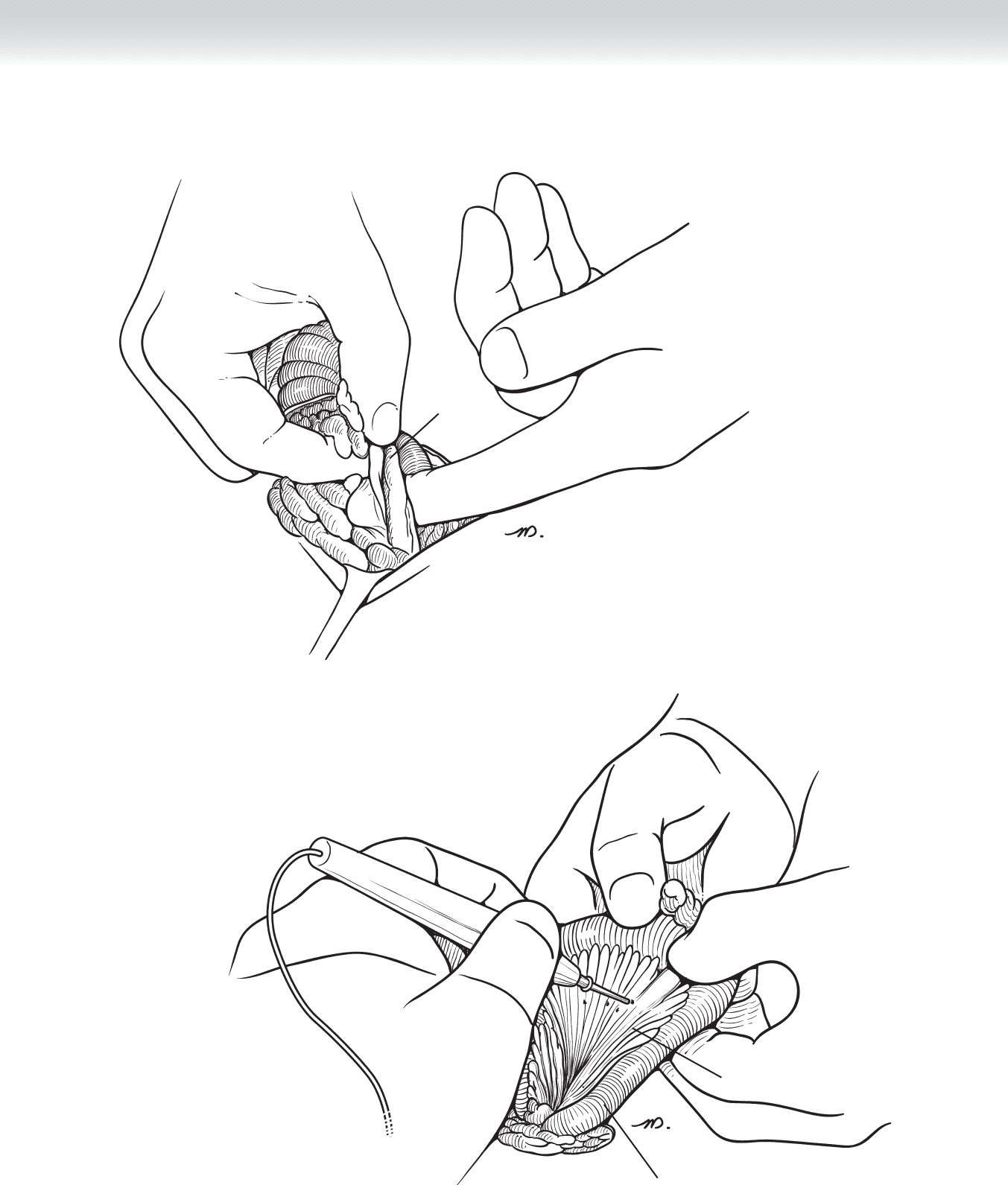
◆ A fi nger is placed beneath the incision and passed against the abdominal wall. Small adhe-
sions are freed (Figure 57-5).
◆ The mesentery is fanned out, scored, and divided using hemostats clamps and 2-0 Vicryl
suture (Figure 57-6).
Proximal bowel
Distal bowel
Mesentery intact
FIGURE 57–4
CHAPTER 57 • Stoma Takedown: Takedown of Loop Colostomy or Ileostomy 645
Adhesions
FIGURE 57 –5
Bowel
Mesentary
FIGURE 57 –6
646 Section IX • Colon
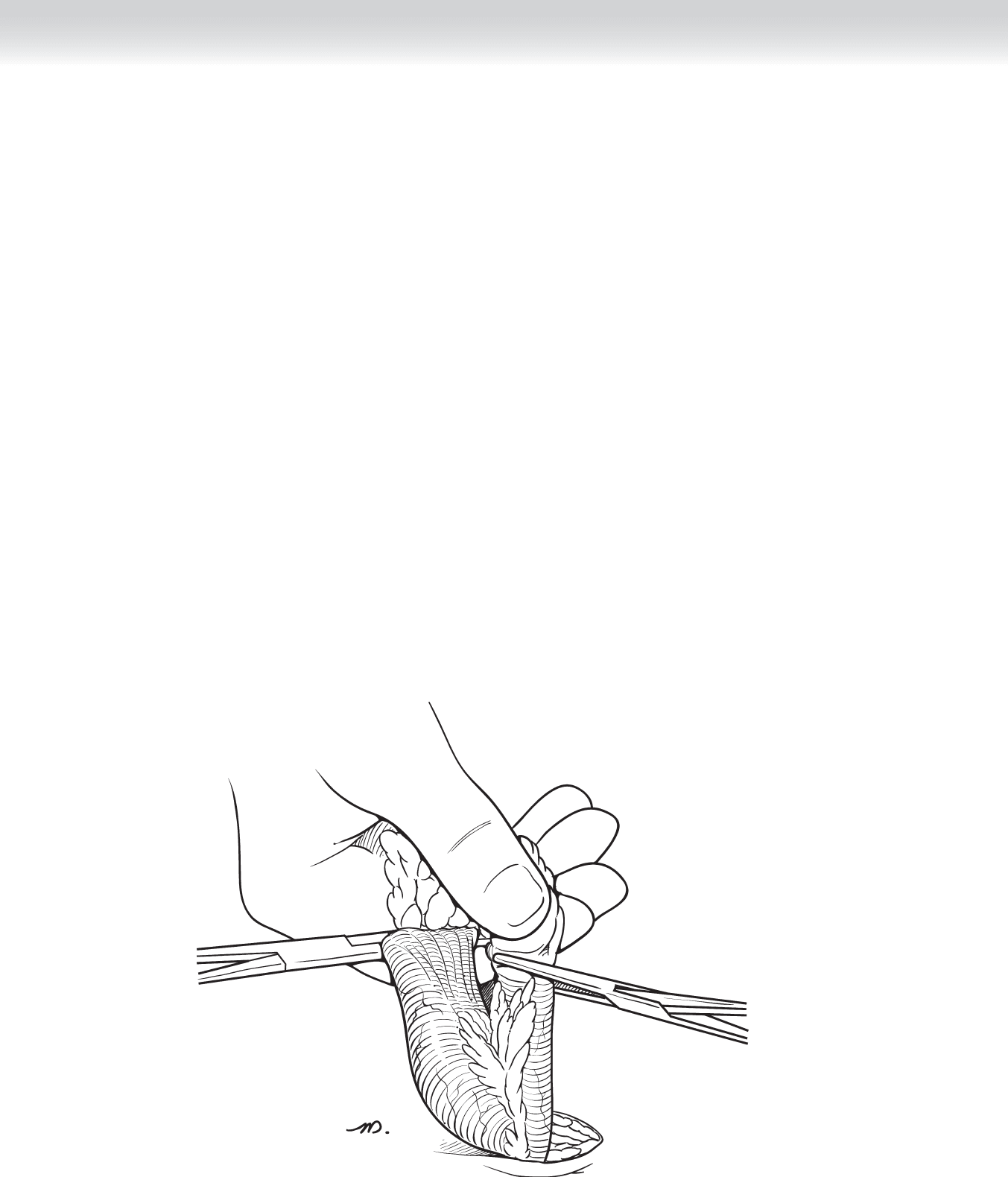
◆ The serosal edge of the bowel is cleaned and Ochsner clamps are placed from the antimes-
entric border to the mesentery in oblique fashion (Figure 57-7).
◆ The fi eld is prepared for opening the bowel. Every measure should be taken to prevent fecal
or enteral spillage into the abdominal cavity. A blue towel is folded and placed on the fi eld,
which will contain contaminated instruments: a metal pool sucker, Allys bowel clamps, and
sponge stick. Moist laparotomy pads are packed around the stoma.
◆ A no. 10 blade knife is used to divide the bowel (Figure 57-8). Allys clamps are placed on
the antimesenteric and mesenteric side of each lumen (Figure 57-9). The proximal limb is
held open with the Allys clamps and the pool sucker is placed into the lumen triangulating
the bowel. A bulb syringe with saline is used to irrigate the lumen, taking care not to touch
open colon with the tip of the syringe or spill saline over the edge of the lumen.
FIGURE 57 –7