Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 59 • Right Colectomy (Laparoscopic-Assisted) 667
2. INCISION
◆ The abdomen is prepped and draped in standard fashion according to the surgeon’s preference.
◆ Using a marking pen, mark the midline from pubic symphysis to xiphoid process to aid
midline entry if rapid conversion to an open procedure is needed.
◆ The laparoscopic instruments are positioned accordingly on the operative fi eld to include a
30-degree laparoscope, two insuffl ation tubing devices attached to CO
2
tanks, electrocau-
tery, suction, and consideration for harmonic scalpel or LigaSure device.
◆ Port placement
◆ Hand-assisted laparoscopic technique
◆ A vertical midline incision is made 1 cm less than the width of the hand. I prefer to
carry the incision through the center of the umbilicus, which will make up for the dif-
ference in length.
◆ The abdomen is entered sharply. The midline fascia is divided beyond the limit of the
skin incision both proximally and distally. Visible adhesions are taken down in stan-
dard fashion.
◆ The GelPort (Applied Medical) is used by placing the Alexis retractor into the wound
and rotating the outer ring inward, thus tightening the fi t. A 5-mm blunt-tipped port
is placed through the GelPort, which is attached to the outer ring. Insuffl ation is initi-
ated on high fl ow to 15 mm Hg.
◆ The left hand is introduced through the GelPort and the laparoscope through the
5-mm port.
◆ A 12-mm port is placed in the upper midline.
◆ The patient is placed in steep Trendelenburg position and airplaned to the right.
◆ Conventional technique
◆ The Veress needle or Hassan technique may be used to access the abdomen below the
umbilicus. A 12-mm port is placed in the left upper quadrant and a 5-mm port is
placed at the upper midline. A second 5-mm port may be placed in the right lower
quadrant for traction.
◆ The liver is visualized and inspected along with the peritoneal cavity for evidence of meta-
static disease. Laparoscopic intraoperative ultrasound may be performed at this time.
668 Section IX • Colon
3. DISSECTION
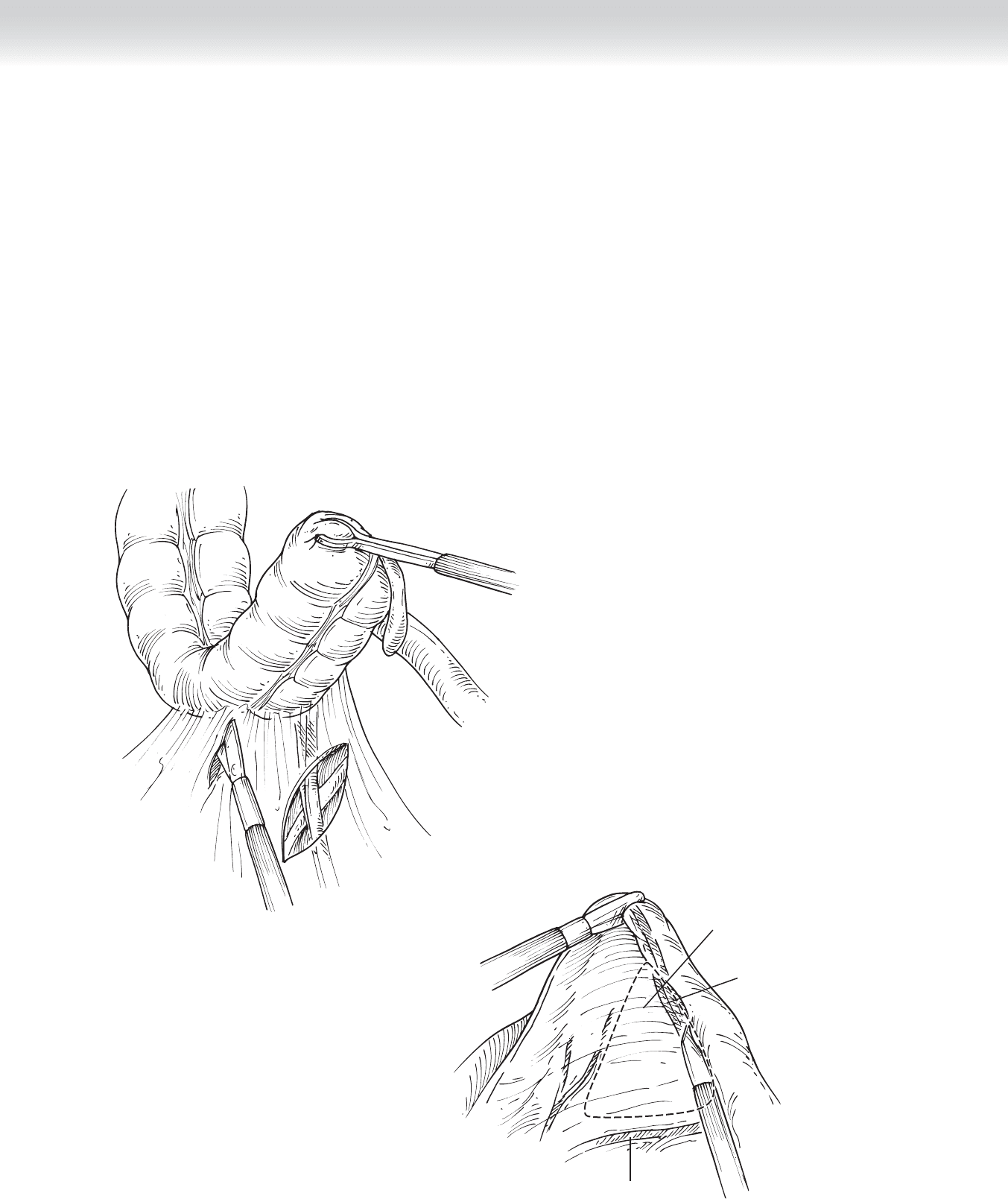
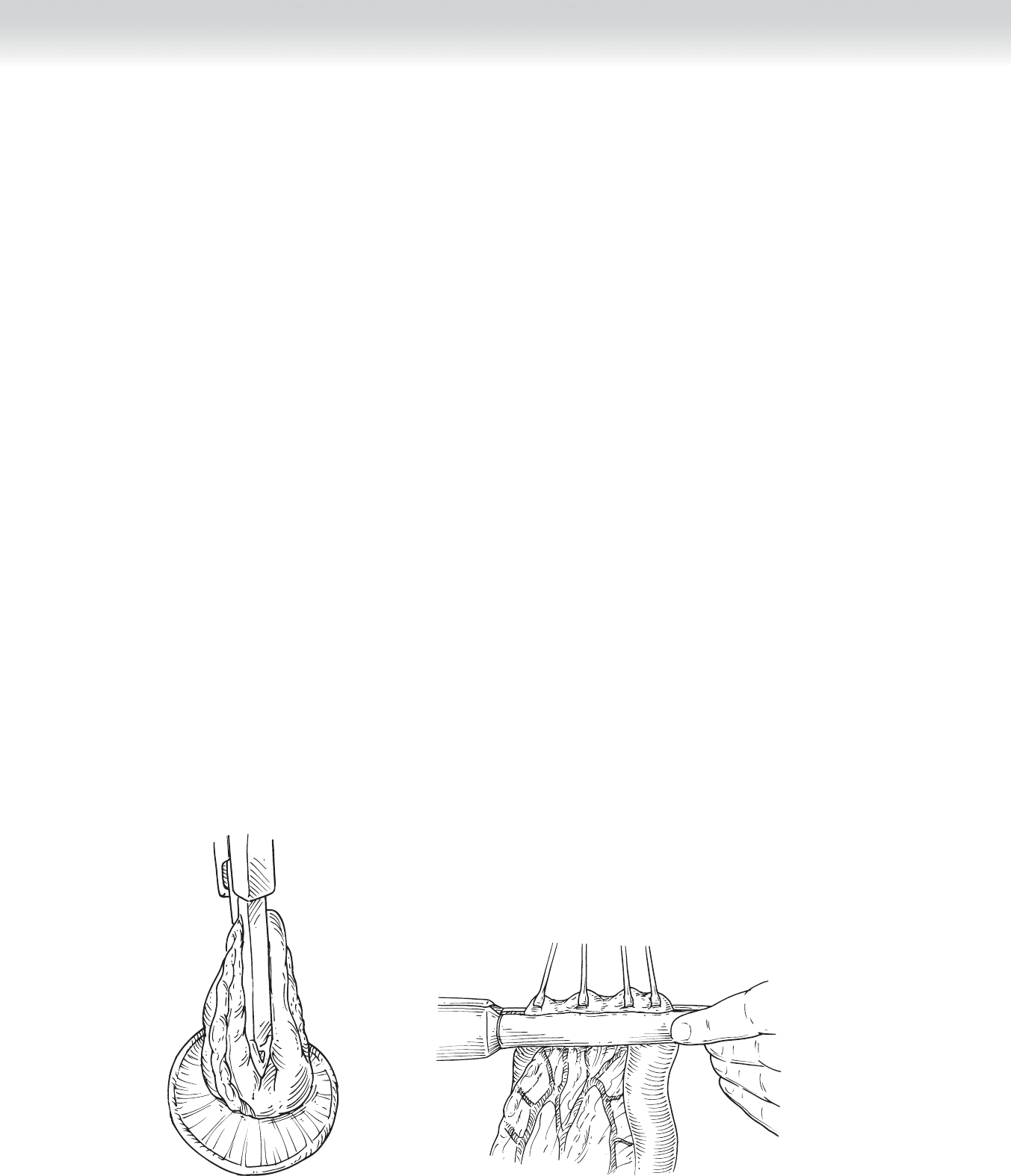
◆ The small bowel is retracted to the left upper abdominal cavity. The cecum is pushed upward
to expose the inferior and retrocecal recesses where the cecum attaches to the retroperito-
neum (Figure 59-1). A subtle fi ne white line may be visible, marking the location where
electrocautery incision is made. This is extended proximally and medially toward the root of
the ascending colon mesentery, just to the right of the superior mesenteric artery.
◆ The ileocolic artery is isolated and divided. A high ligation is performed at its origin of the
superior mesenteric artery for oncologic resection (Figure 59-2). Before ligation, the vessels
are lifted off the retroperitoneal plane and the pedicle skeletonized. The right ureter should
be visualized before ligation of the pedicle. The pedicle is taken using an endoscopie gastro-
intestinal anastomosis (GIA) vascular load stapling device.
FIGURE 59 –1
Window in ileocolic
mesentery
Ileocolic vessels
within mesentery
Superior
mesenteric artery
FIGURE 59 –2
CHAPTER 59 • Right Colectomy (Laparoscopic-Assisted) 669
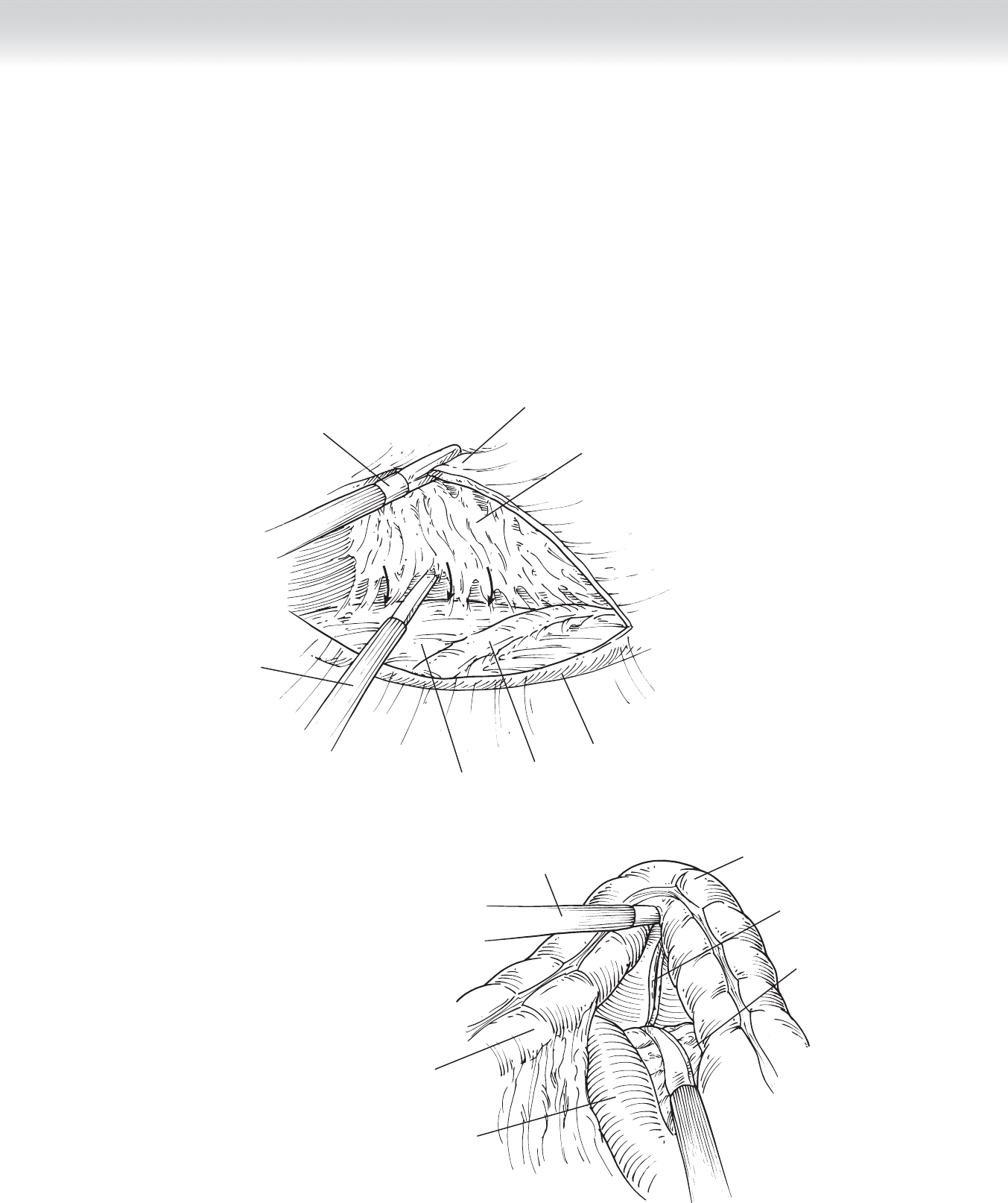
◆ The ascending colon and mesentery are further dissected off the retroperitoneum
(Figure 59-3).
◆ In the hand-assisted technique, this is done by “walking” the left index and second fi nger
up the posterior surface toward the liver. The lateral peritoneal attachment is maintained
for countertraction.
◆ In the conventional technique, the trochar is used to bluntly create this pocket while the
colon is held up in countertraction with atraumatic graspers.
◆ The duodenum is identifi ed and swept downward (Figure 59-4). Similarly, the right kidney
is maintained posterior to the plane of dissection.
Hand or
suprapubic trocar
Mesentery of
right colon
Areolar tissue
behind right colon
Iliac artery
Ureter
Psoas muscle
Left upper
quadrant trocar
FIGURE 59 –3
Hand or
suprapubic trocar
Right colon and
terminal ileum
mesentery
Duodenum
(second portion)
Middle colic vessels
Head of pancreas
Transverse colon
FIGURE 59 –4
670 Section IX • Colon
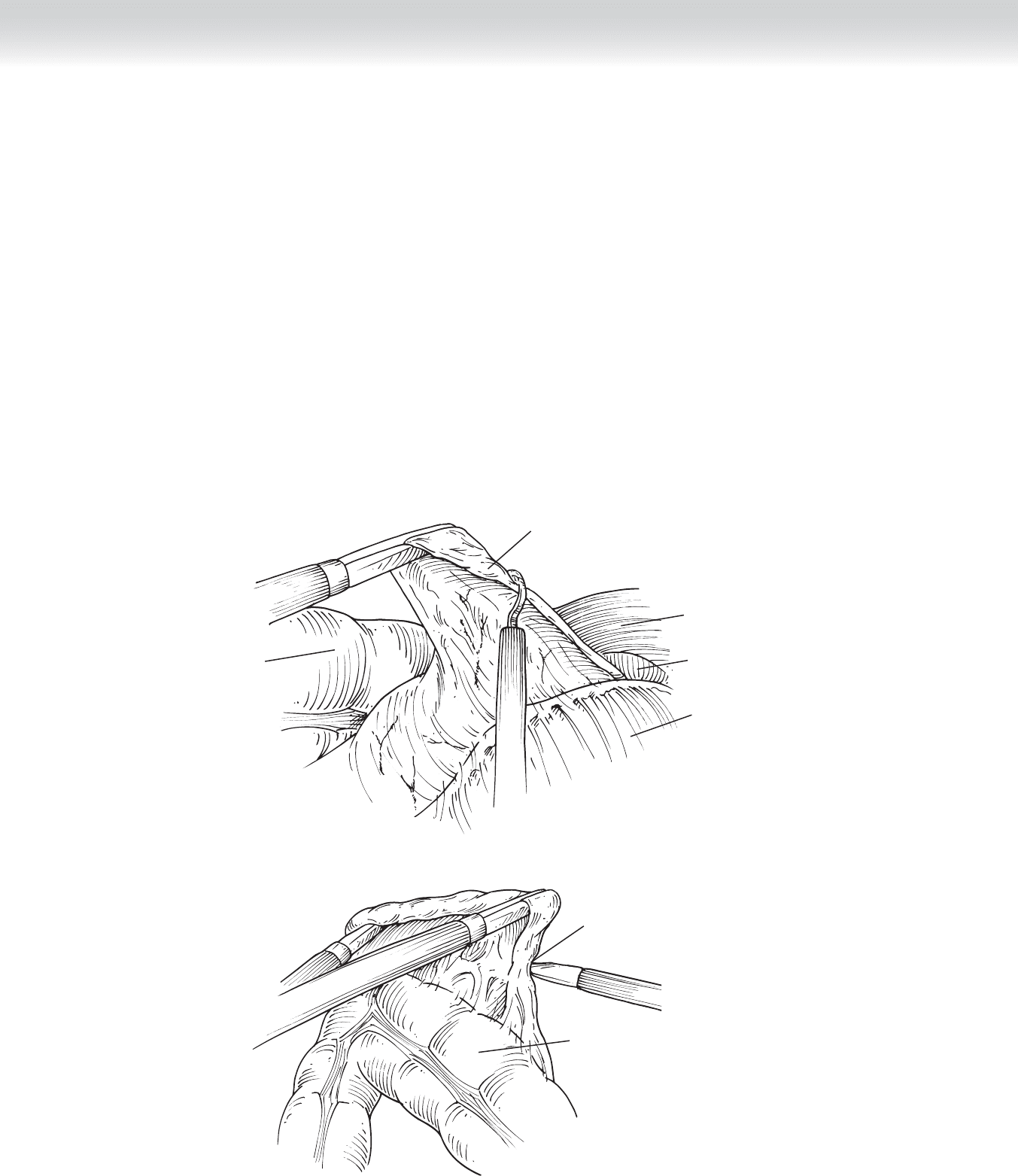
◆ The right colic artery, if present, is isolated and divided, as is the hepatic branch of the
middle colic artery.
◆ The lateral attachment is divided and dissection is carried around the hepatic fl exure, taking
the hepatocolic ligaments down (Figure 59-5, A). The gastrocolic ligament is detached from
the transverse colon just distal to the point where the colon will be divided (Figure 59-5, B).
For an oncologic resection, the omentum should be resected with the specimen, taking care to
preserve the gastroepiploic artery.
◆ The mesentery is divided to the point of vascular demarcation of the transverse colon.
◆ Pneumoperitoneum is reversed and the mobilized segment is exteriorized.
Transverse
colon
Liver
Gallbladder
Release of
hepatocolic flexure
Stomach
A
Transverse
colon
B
Release of
gastrocolic
ligament
FIGURE 59 –5
CHAPTER 59 • Right Colectomy (Laparoscopic-Assisted) 671
◆ The mesentery to the terminal ileum is clamped, divided, and ligated to a point 5 to 15 cm
away from the ileocecal valve. The mesentery is similarly cleared from the transverse colon.
◆ Hand-sewn end-to-end anastomosis:
◆ An Ochsner bowel clamp is placed obliquely on the small bowel to make up for the
size difference between the small bowel and colon lumen.
◆ An Ochsner bowel clamp is placed perpendicularly on the transverse colon.
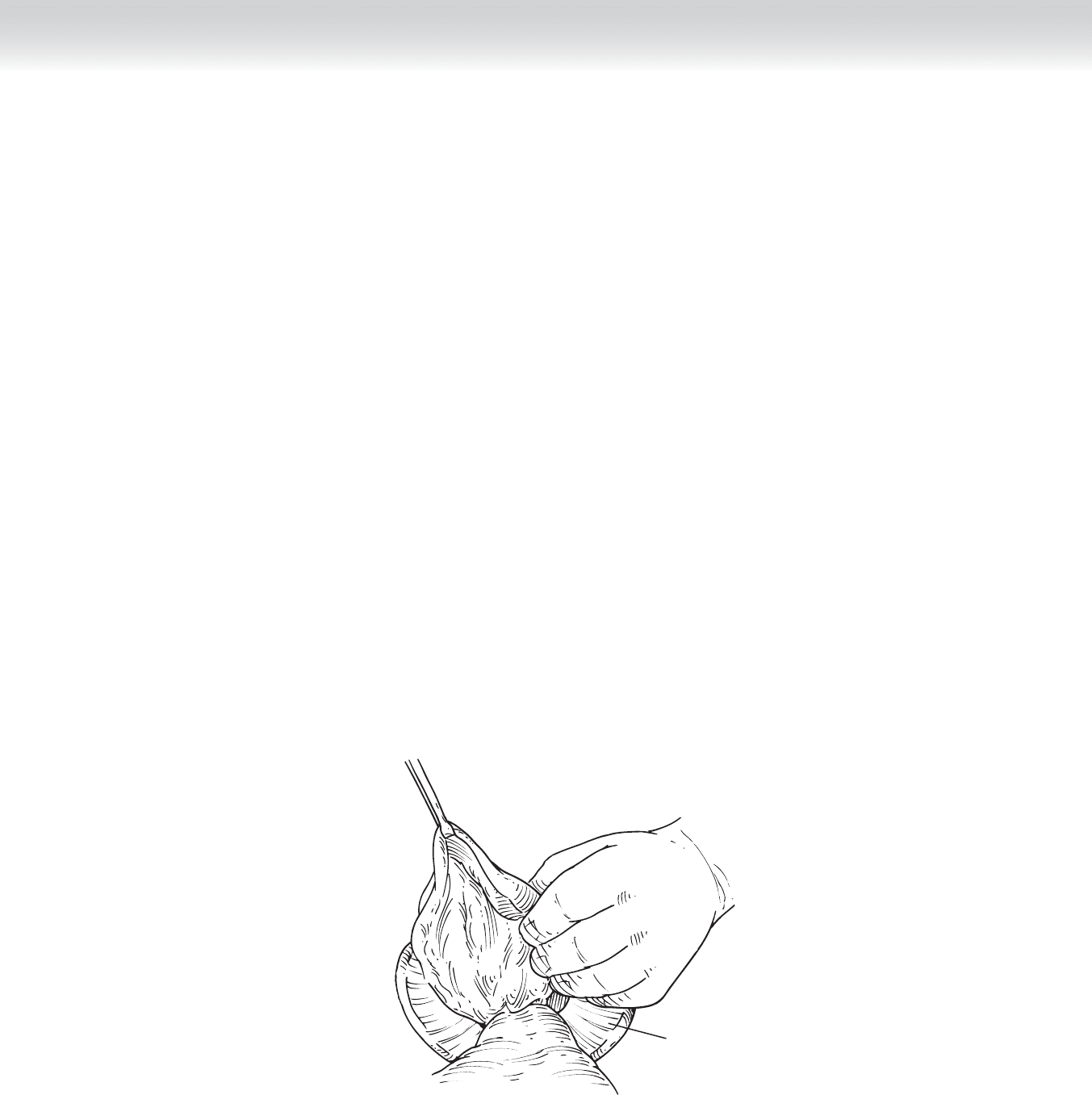
◆ The specimen is transected and removed from the table (Figure 59-6).
◆ The two ends of bowel are positioned so that the antimesenteric and mesenteric ends
are aligned.
◆ Both lumens are inspected and irrigated, taking care to maintain sterile technique and
minimize fecal spillage.
◆ A double-armed 4-0 Maxon monofi lament suture is used to create a single-layered
running anastomosis. The serosal edge is grasped and the mucosa and submucosal
edges are reapproximated. This is done by placing the knot on the outer portion of the
bowel at the antimesenteric border. One arm of suture is passed under the knot and
used to complete half of the anastomosis, as is the other arm on the other side. The
suture line is inspected for integrity.
◆ Stapled side-to-side anastomosis:
◆ The exteriorized segment is laid out so that the antimesenteric limb of the small bowel
is aligned with the antimesenteric limb of the transverse colon. A stay stitch using 2-0
Vicryl suture may be used to maintain alignment.
◆ A colotomy and enterotomy are made on the antimesenteric side over the proximal
and distal resection lines using Bovie electrocautery.
Wound protector
Deliver specimen
FIGURE 59 –6
672 Section IX • Colon
◆ A 75-mm blue load linear GIA stapling device is introduced through each opening,
and a common wall is created between the two, taking care to ensure that the mesen-
tery is away from the staple line.
◆ The linear stapler is reloaded and fi red perpendicularly to the staple line, closing the
colostomy and releasing the specimen from the fi eld (Figure 59-7).
◆ The staple line is inspected for integrity. It is our preference to place a 2-0 Vicryl stitch
between the colon and ileum to take tension off the staple line. The intersection of the
staple line may also be reinforced with a fi gure-of-eight stitch, because this is a natural
weak point.
◆ The mesenteric defect may be closed according to the surgeon’s preference.
◆ The completed anastomosis is dropped back into the abdominal cavity.
◆ Surgical gloves are changed, and the Alexis wound retractor is removed. It is our preference
to place Seprafi lm over the midline incision to minimize postoperative adhesions. The abdo-
men is reapproximated using 0 polydioxanone (PDS) in fi gure-of-eight interrupted sutures.
◆ The subcutaneous skin is irrigated with bacitracin antibiotic (50,000 U in 1 L saline).
◆ Staples are used to close skin. A small umbilical bolster is created by placing a bacitracin-
soaked cotton ball wrapped in Adaptic into the umbilical depression. This is left in place
during the hospital stay and removed before discharge home.
◆ The orogastric tube is removed before extubation, provided there is no extensive lysis of
adhesions or indication for maintenance of a nasogastric tube postoperatively.
Side-to-side
anastomosis
with GIA stapler
A
Transverse closure
B
FIGURE 59 –7

CHAPTER 59 • Right Colectomy (Laparoscopic-Assisted) 673
STEP 4: POSTOPERATIVE CARE
◆ Adherence to a postoperative colorectal clinical pathway ensures standardization of care and
facilitates timely discharge from the hospital.
◆ Adequate pain control is achieved using patient-controlled analgesia. Use of a nonopioid anal-
gesic such as ketorolac (Toradol) should be considered. In our protocol, this is administered
on postoperative day 1, provided there are no contraindications such as renal insuffi ciency,
and given on a scheduled basis of 15 mg intravenously every 8 hours for 9 doses. Patients are
transitioned to an oral analgesic on postoperative day 2.
◆ Consideration for stress ulcer prophylaxis should be made for patients with symptoms or
history of gastroesophageal refl ux disease (GERD) or peptic ulcer disease (PUD).
◆ All patients should receive prophylaxis for deep venous thrombosis, consisting of sequential
compression devices while in bed, and heparin 5000 U subcutaneously every 8 hours or
enoxaparin 40 mg subcutaneously every morning, starting within 24 hours after surgery.
◆ Adequate IV fl uid should be administered with monitoring of urine output. The Foley cath-
eter may be removed on postoperative day 1.
◆ The diet may be limited to ice chips and sips of water in the postanesthesia care unit. A
clear liquid diet is started on postoperative day 1. Return of bowel function is measured by
the frequency and pitch of bowel sounds, lack of abdominal distention, amount of belch-
ing, presence of nausea and vomiting, and the patient’s subjective will to eat. Diet may be
advanced ad lib as bowel function returns.
◆ Early ambulation is crucial for aid in return of bowel function. Patients should be instructed
to walk multiple times a day beginning on postoperative day 1.
◆ The dressing over the incision site is removed on postoperative day 2, and the incision is
checked daily thereafter to ensure absence of infection. The umbilical bolster remains in
place until the patient is discharged from the hospital.
STEP 5: PEARLS AND PITFALLS
◆ The use of SCIP approved prophylactic antibiotic for colorectal surgery, ertapenem (Invanz)
1 g intravenously, before surgery, requires only a single dose for 24-hour coverage. Further-
more, it lasts for the duration of the procedure and does not require additional dosing.
◆ The hepatic fl exure suspensory ligaments should be divided with caution, because there are
often large veins here. Careful dissection and the use of energy ligatures should strongly be
considered to avoid uncontrollable bleeding and subsequent conversion to open laparotomy.

674 Section IX • Colon
◆ Smaller lesions in the colon should be marked with tattoo ink for confi rmation of location,
which will assist in removal of the primary lesion with adequate 5-cm margin and areas of
lymphatic drainage.
◆ Placement of Seprafi lm under the midline incision minimizes adhesions on reentry for sub-
sequent operations. This should be considered, especially for indications such as Crohn’s
disease and colon cancer.
SELECTED REFERENCES
1. Tinley HS, Constantinides VA, Heriot AG, et al: Comparison of laparoscopic and open ileocecal resection
for Crohn’s disease: A meta-analysis. Surg Endosc 2007;20:1036-1044.
2. Kaban GK, Novitsky YW, Perugini RA, et al: Use of laparoscopy in evaluation and treatment of penetrating
and blunt abdominal injuries. Surg Innov 2008;15:26-31.
3. Kang JC, Chung MH, Yeh CC, et al: Hand assisted laparoscopic colectomy versus open colectomy: A pro-
spective randomized study. Surg Endosc 2004;18:577-581.
4. Itani KMF, Wilson SE, Awad SS, et al: Ertapenem versus cefotetan prophylaxis in elective colorectal sur-
gery. N Engl J Med 2006;355:2640-2651.
5. Guidelines from the Joint Commission on Surgical Care Improvement Project Core Measurement Set.
Available on Internet: www.jointcommission.org/PerformanceMeasurement.
6. Law WL, Bailey HR, Max E, et al: Single-layer continuous colon and rectal anastomosis using monofi la-
ment absorbable suture (Maxon): Study of 500 cases. Dis Colon Rectum 1999;42:736-740.
7. Max E, Sweeney WB, Bailey HR, et al: Results of 1,000 single-layer continuous polypropylene intestinal
anastomoses. Am J Surg 1991;162:461-467.
8. Zeng Q, Yu Z, You J, Zhang Q: Effi cacy and safety of Seprafi lm for preventing postoperative abdominal
adhesion: Systematic review and meta-analysis. World J Surg 2007; 31:2125-2131;2132 [discussion].

675
STEP 1: SURGICAL ANATOMY
◆ The left colon begins at the mid-transverse colon and includes the splenic fl exure, left
(descending) colon, and sigmoid colon. The marginal artery of Drummond provides a
vascular anastomosis between the superior and inferior mesenteric arteries. The blood
supply to the left colon is derived from the inferior mesenteric artery. The fi rst branch,
the left colic artery, supplies the splenic fl exure and descending colon. The sigmoid
arteries and the superior rectal artery are the most distal branches of the inferior mesen-
teric artery and supply the sigmoid colon. The lymphatics follow its arterial blood sup-
ply. A minimum of 12 lymph nodes within the mesentery is considered an adequate
resection when performing a left hemicolectomy or sigmoidectomy for cancer.
STEP 2: PREOPERATIVE CONSIDERATIONS
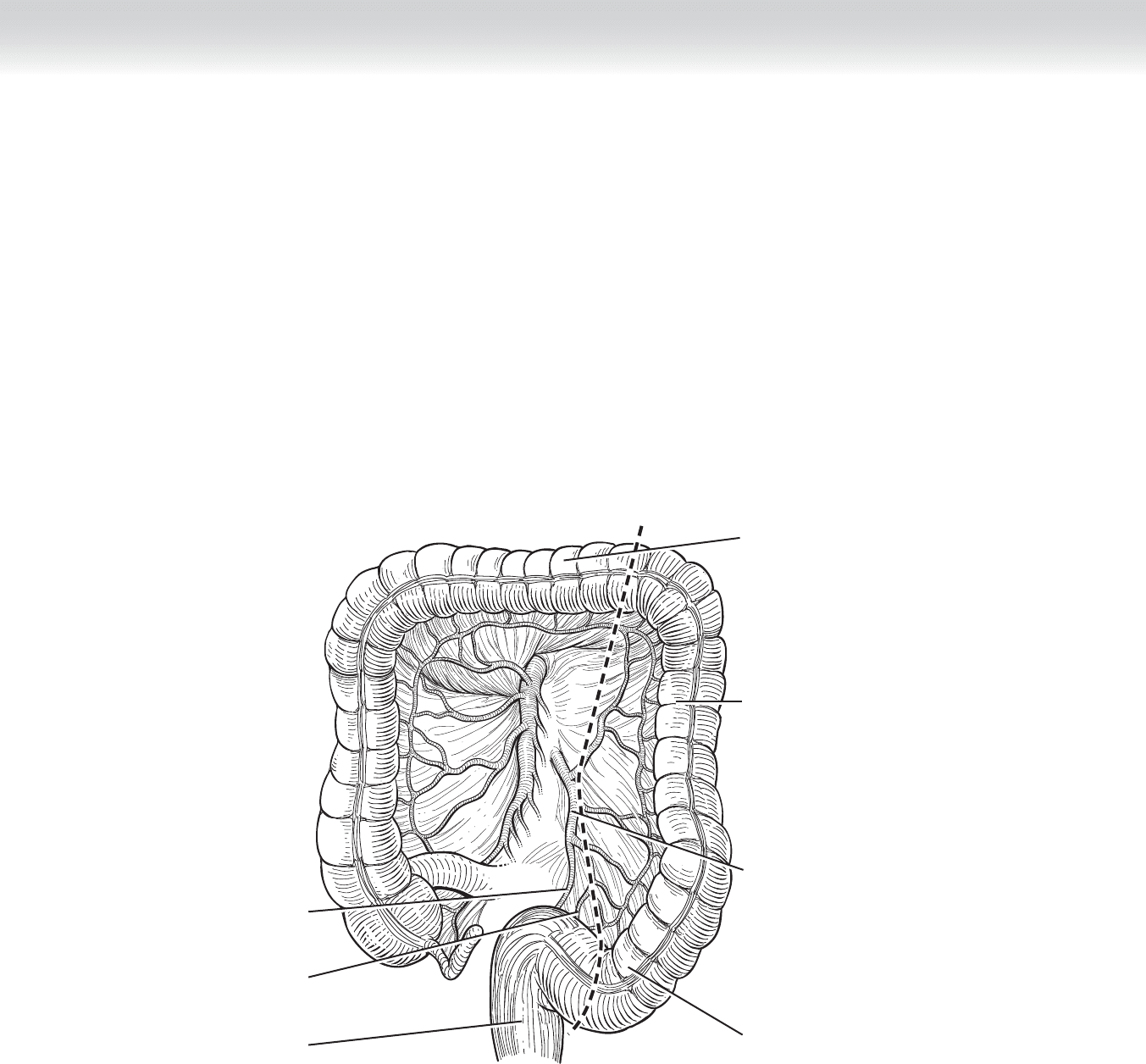
◆ Indications: Tumors of the left colon can be resected with a left hemicolectomy, which
involves sacrifi cing the inferior mesenteric blood supply, along with its branches (left
colic artery and sigmoid arteries), which supply the splenic fl exure to the proximal sig-
moid colon. Tumors of the sigmoid colon can be removed with a sigmoid resection,
encompassing the distal descending colon and the sigmoid colon, sacrifi cing the sigmoid
and superior rectal arteries (Figure 60-1).
◆ Preoperative planning: Evaluation of the entire colorectal lumen is necessary to rule out
synchronous lesions before surgical intervention. This can be accomplished with either
colonoscopy or barium enema, assuming that the patient does not have an obstructing or
near-obstructing lesion. An adequate mechanical bowel preparation is generally performed
the day before surgical resection, but is not considered necessary. Preoperatively, intrave-
nous antibiotics must be administered before the skin incision. A preoperative dose of sub-
cutaneous heparin (5000 U) or a low-molecular-weight heparin is recommended to prevent
deep venous thrombosis. Before induction of general anesthesia, pneumatic compression
boots are placed on both lower extremities and continued postoperatively until the patient
ambulates on the fi rst postoperative day. A Foley catheter is placed after induction of gen-
eral anesthesia. Stress ulcer prophylaxis may be given until the patient tolerates oral intake.
◆ Anesthesia: General anesthesia is used.
CHAPTER
60
Left and Sigmoid
Colectomy
Celia Chao
676 Section IX • Colon
STEP 3: OPERATIVE STEPS
1. INCISION
◆ A midline incision is made. A Thompson retractor is used to retract the abdominal wall,
particularly the left costal margin, which is necessary to facilitate adequate exposure of the
splenic fl exure.
Transverse colon
Descending colon
Sigmoid colon
Inferior mesenteric artery
Superior rectal artery
Sigmoid artery
Rectum
FIGURE 60 –1