Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 58 • Right Hemicolectomy 657
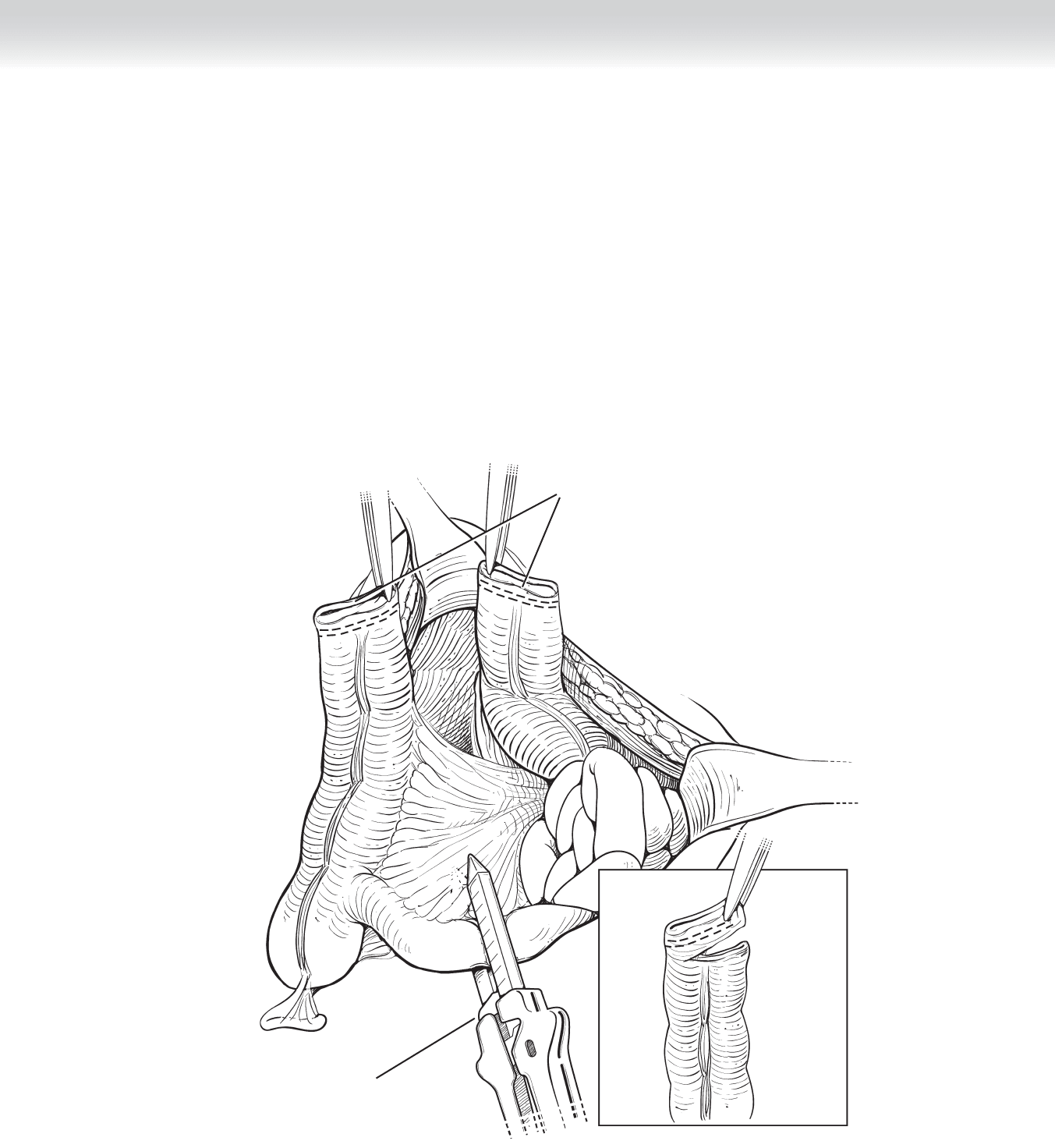
Ends of divided
transverse colon
GIA stapler used to
divide ileum
FIGURE 58 –6
658 Section IX • Colon
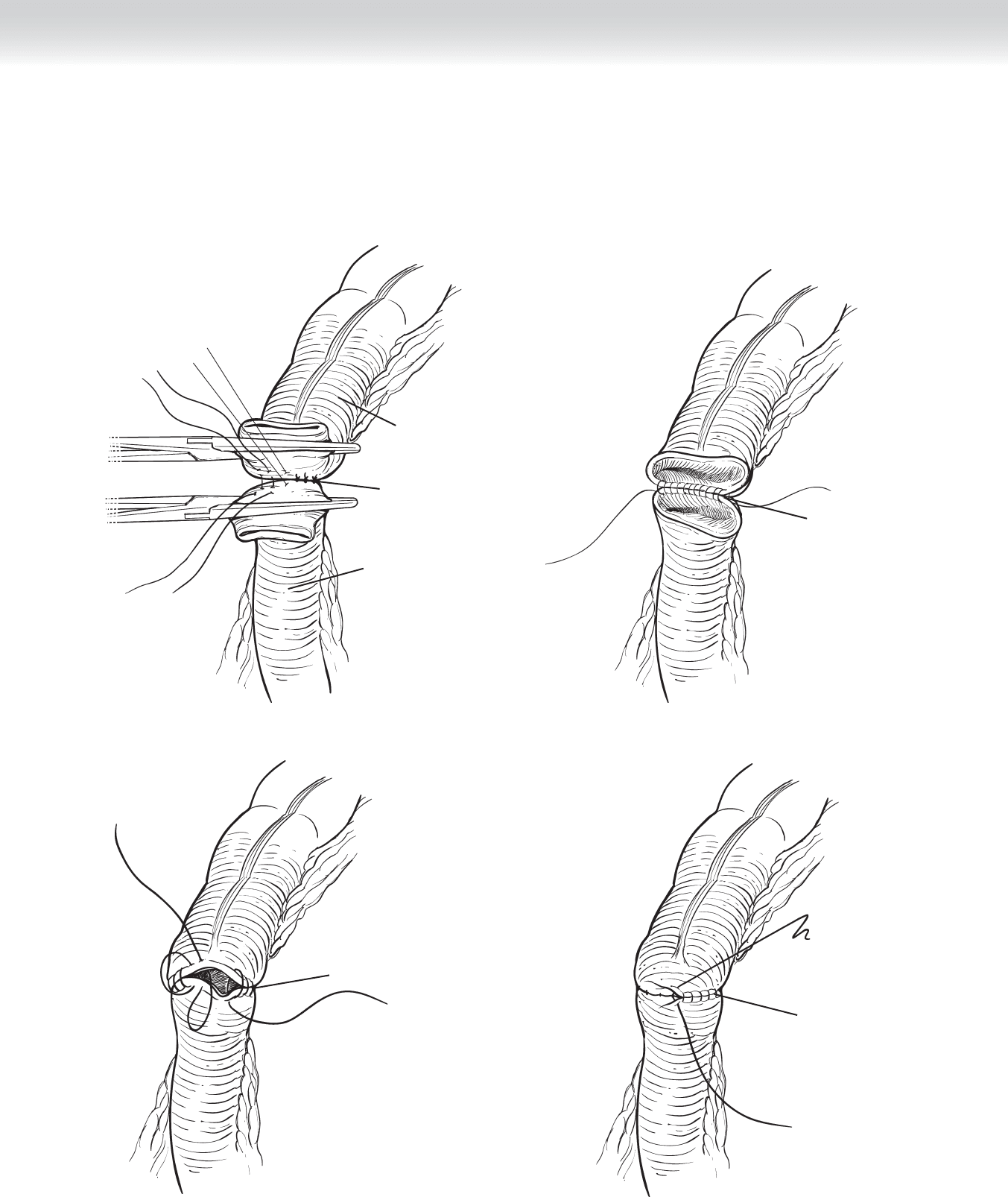
◆ Creation of continuity between the terminal ileum and transverse colon can be performed
using either a hand-sewn or a stapled technique. A standard end-to-end (Figures 58-7
through 58-10) or side-to-side anastomosis (Figures 58-11 and 58-12) are then performed.
Transverse colon
Ileum
Posterior interrupted sutures
Two continuous
running sutures
FIGURE 58 –7
FIGURE 58 –8
Anterior running sutures
FIGURE 58 –9
Lembert sutures
FIGURE 58 –10
CHAPTER 58 • Right Hemicolectomy 659
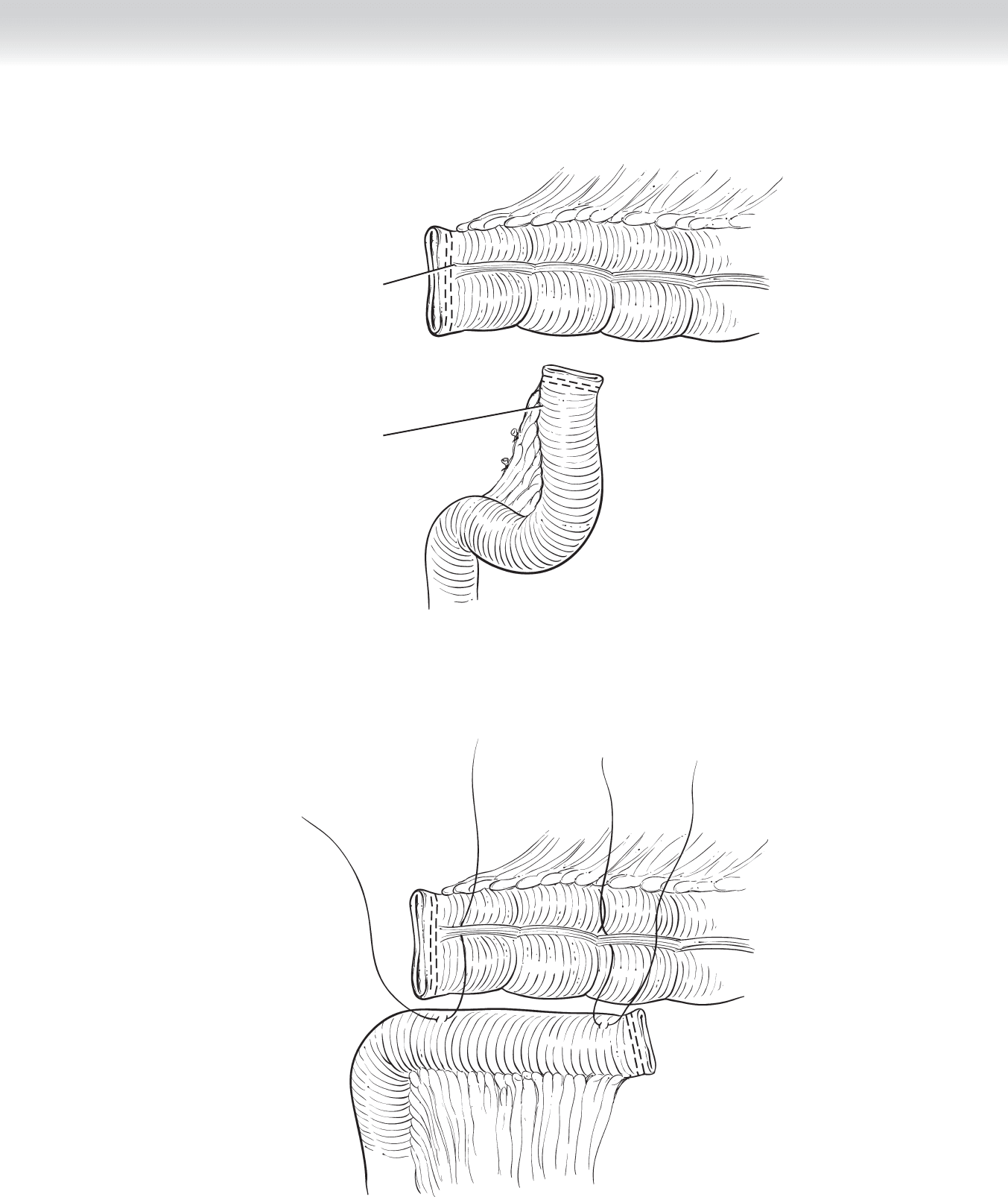
Ileum
Transverse colon
FIGURE 58 –11
FIGURE 58 –12
660 Section IX • Colon
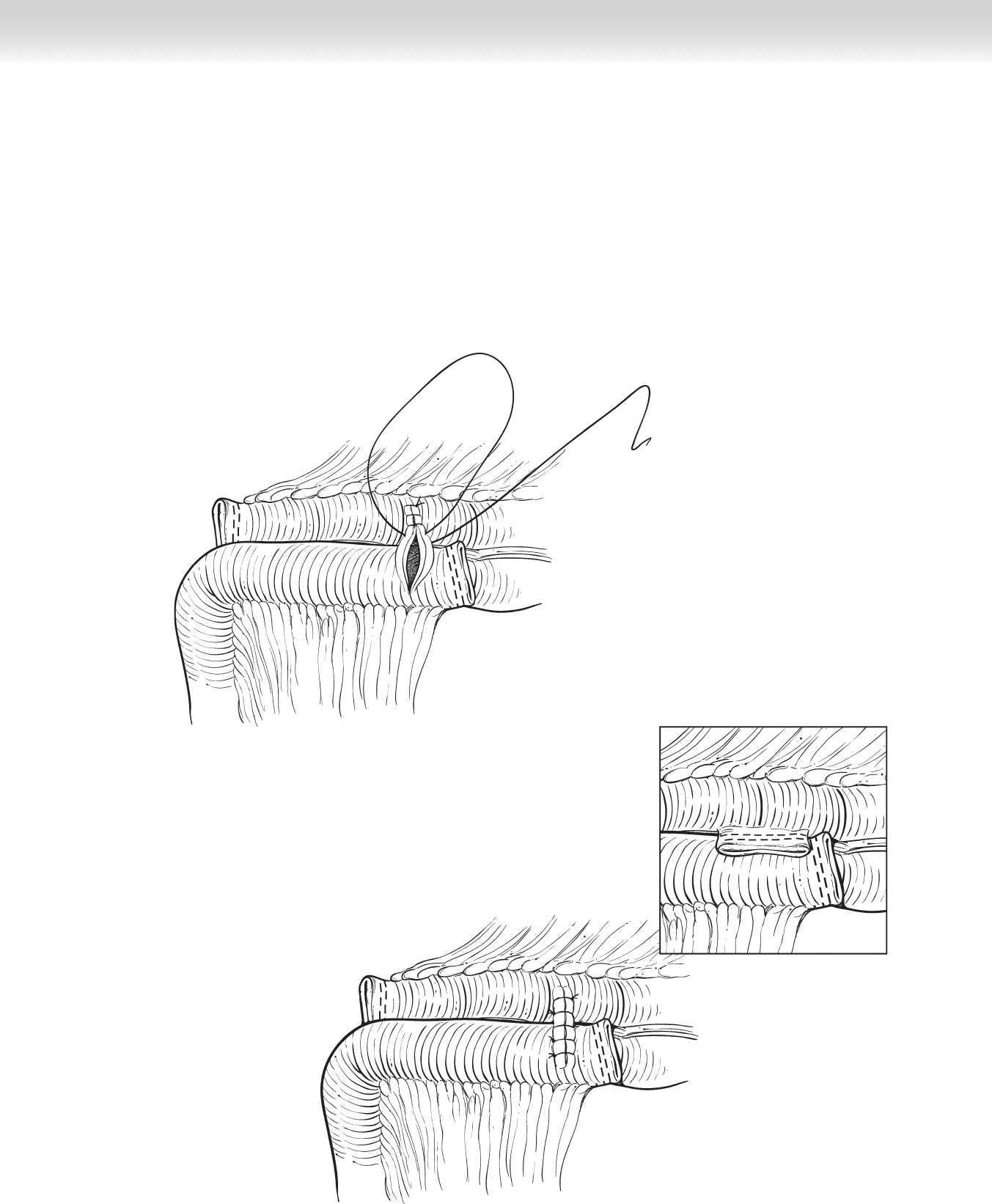
◆ The two ends of bowel are aligned for the anastomosis so that their respective mesenteries
are not twisted. Both the hand-sewn and stapled techniques are acceptable and have been
shown to have equivalent functional results. A hand-sewn anastomosis is standardly per-
formed in two layers: a posterior Lembert layer (see Figure 58-7); an inner full-thickness
(a good seromuscular bite with a small ridge of mucosa) running continuous layer using
absorbable sutures beginning posteriorly and continuing anteriorly as a Connell inverting
suture (see Figures 58-8 and 58-9); and fi nally, an outer row of interrupted Lembert sero-
muscular stitches, using nonabsorbable sutures (see Figure 58-10).
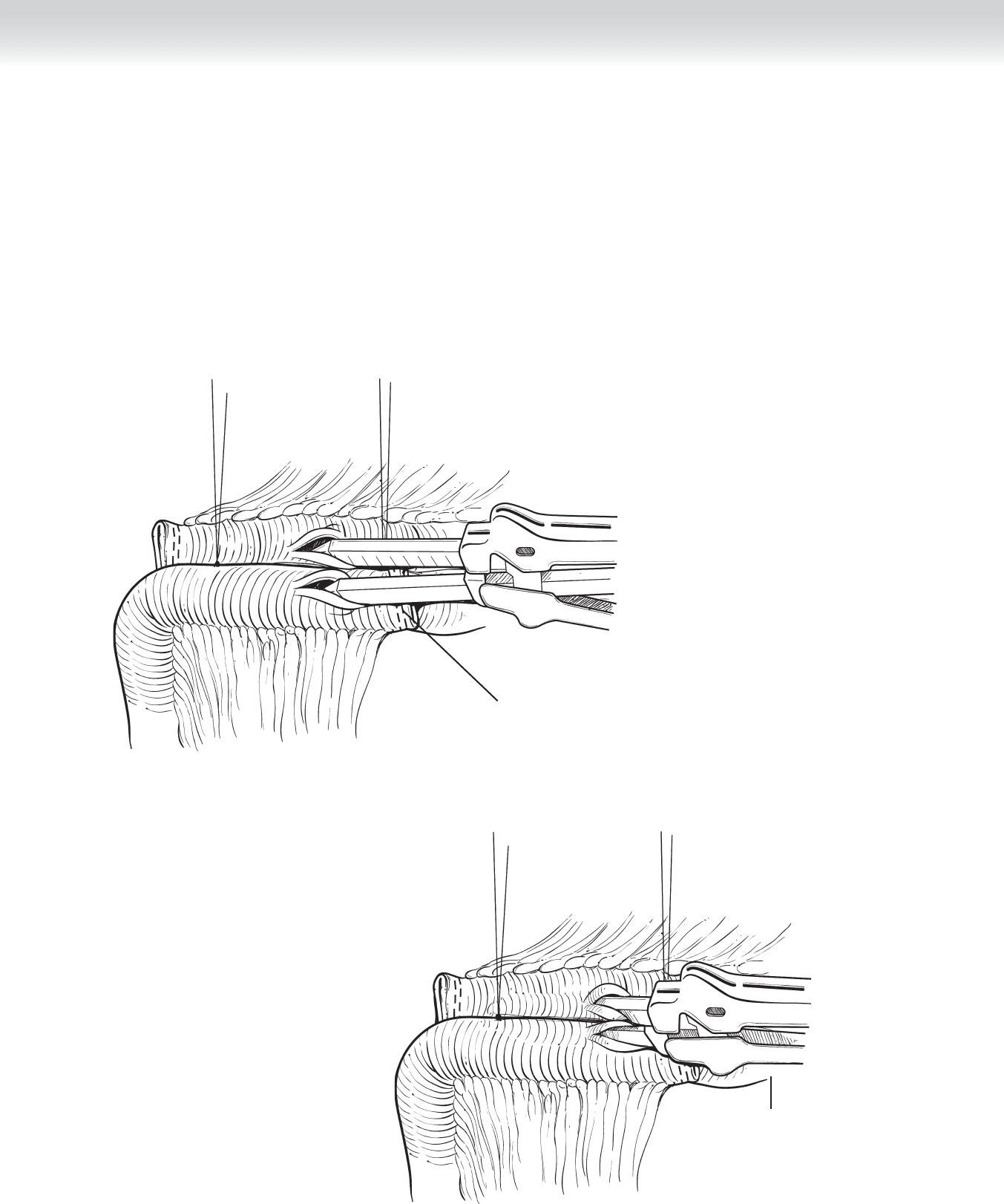
GIA stapler used for
enterotomy anastomosis
FIGURE 58 –13
Prior to firing
stapler, ensure
anti-mesenteric
borders of bowel
are aligned
FIGURE 58 –14
CHAPTER 58 • Right Hemicolectomy 661
◆ The arms of the GIA stapler are then inserted into each bowel lumen (the ileum and transverse co-
lon), and the antimesenteric borders of the bowel are aligned. Two silk stay sutures are useful to assist
with the alignment—one proximal, near the cut edge of bowel, and the other distal, beyond the
length of the staple line. The stapled anastomosis is performed by fi rst creating colotomies near the
stapled ends of the bowel (Figures 58-13 and 58-14). After fi ring the GIA stapler, check the mucosa
of the bowel along the staple line for bleeding. The resultant ileocolostomy is closed with a TA-55
stapler or by using a single layer of absorbable suture incorporating full thickness of bowel wall in a
running continuous fashion (Figures 58-15 and 58-16).
FIGURE 58 –15
Alternative closure with TA-55 stapler
FIGURE 58 –16
662 Section IX • Colon
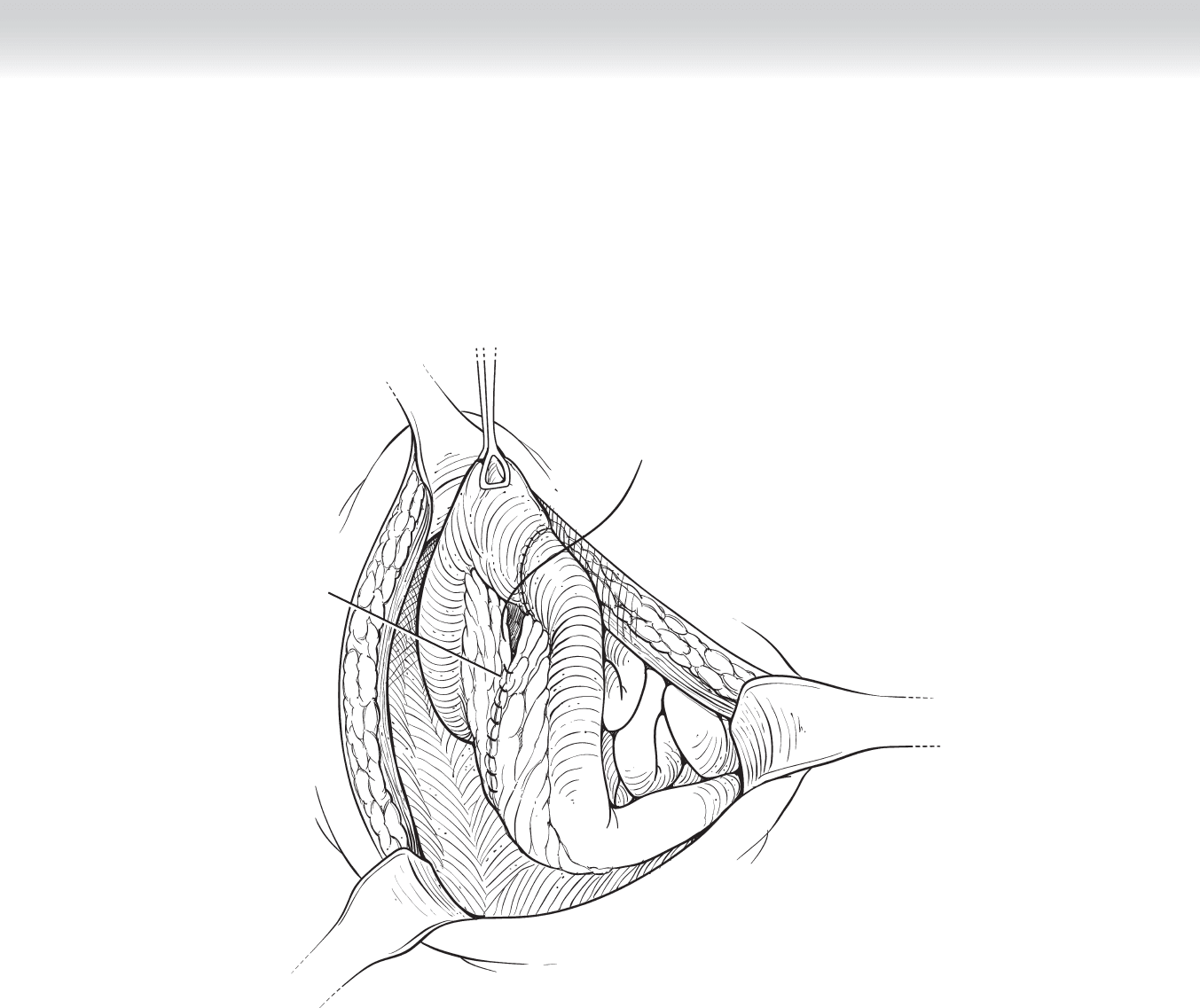
◆ Reapproximating the mesenteric defect must be performed with care to ensure that the
underlying vessels supplying the bowel are not compromised. This can be sutured using
a continuous absorbable stitch (Figure 58-17).
Closure of mesentery
FIGURE 58 –17

CHAPTER 58 • Right Hemicolectomy 663
3. CLOSING
◆ The abdominal cavity is irrigated with copious warm saline. The omentum can be overlaid
on top of the newly formed anastomosis. After ensuring hemostasis, sponge counts, and
instrument counts, close the abdomen using a no. 1 polydioxanone (PDS) suture. The sub-
cutaneous tissue is irrigated again and the skin is closed with skin clips (see Figure 58-17).
STEP 4: POSTOPERATIVE CARE
◆ A nasogastric tube is generally not required for a routine right hemicolectomy. Patients can
generally tolerate sips of clear liquids and progress to a regular diet over the next few post-
operative days.
STEP 5: PEARLS AND PITFALLS
◆ Be careful of injury to retroperitoneal structures such as the duodenum and right ureter.
◆ When performing the operation for cancer, it is important to ensure that the pathologists
process and look at an adequate number of lymph nodes. This will ensure more accurate
nodal staging, which is essential for the decision to treat with adjuvant chemotherapy.
SELECTED REFERENCES
1. Wille-Jørgensen P, Rasmussen MS, Andersen BR, Borly L: Heparins and mechanical methods for thrombo-
prophylaxis in colorectal surgery. Cochrane Database Syst Rev 2004(4):CD001217.
2. Stahl TJ, Gregorcyk SG, Hyman NH, et al: Practice parameters for the prevention of venous thrombosis.
Dis Colon Rectum 2006;49:1477-1483.
3. Docherty JG, McGregor JR, Akyol AM, et al: Comparison of manually constructed and stapled anastomo-
ses in colorectal surgery. Ann Surg 1995;221:176-184.
4. LeVoyer TE, Sigurdson ER, Hanlon AL, et al: Colon cancer is associated with increasing number of lymph
nodes analyzed: A secondary survey of intergroup trial INT-0089. J Clin Oncol 2003;21:2912-2919.
664
STEP 1: SURGICAL ANATOMY
◆ The surgeon must be familiar with the fascial attachments of the ascending colon, which
can be used for countertraction during laparoscopic resection. The white line of Toldt is the
lateral peritoneal attachment of the ascending colon to the abdominal wall and serves as a
guide during surgical mobilization.
◆ The ascending colon is covered by peritoneum on the anterior and lateral sides. The retro-
cecal and inferior cecal recesses mark the attachment of the cecum to the retroperitoneum.
Division of the peritoneum here allows entry behind the cecum and dissection of the fi ne
areolar tissue called the fascia of Toldt. Beneath this plane lie Gerota’s fascia and the right
kidney. Care should be taken to avoid lifting this structure along with the colon, especially
when the areolar plane is fi brotic or densely adhesive (as seen in desmoplastic reactions). In
addition, the right ureter lies beneath this plane and parallel to the gonadal vessels and thus
should be avoided.
◆ The second portion of the duodenum is exposed during the retroperitoneal dissection and
should be swept downward, away from the posterior wall of the colon.
◆ The inferior vena cava lies medially in the retroperitoneal plane and should be avoided
during the retroperitoneal dissection.
◆ The main blood supply to the ascending colon is the ileocolic and right colic arteries.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for laparoscopic right colectomy are the same as for conventional operations.
The decision to chose this operative approach depends on the skill and experience of the
surgeon. Laparoscopic surgery traditionally has been used to treat conditions on an elective
basis but has expanded to include selective emergent situations, such as those seen in
CHAPTER
59
Right Colectomy
(Laparoscopic-Assisted)
Valerie P. Bauer

CHAPTER 59 • Right Colectomy (Laparoscopic-Assisted) 665
penetrating abdominal trauma and repair of endoscopically created perforations. Other
indications include:
◆ Benign polyps or lesions not amenable to endoscopic resection
◆ Malignant lesions located in the appendix, cecum, ascending colon, and hepatic fl exure
◆ Crohn’s disease of the terminal ileum and ascending colon
◆ Cecal volvulus
◆ The hand-assisted technique allows for use of one hand in the abdomen while maintain-
ing pneumoperitoneum. Advantages include preservation of tactile sensation and ease of
dissection and should be considered for potentially diffi cult cases such as those having
anticipated adhesions or infl ammatory conditions as in cancer and infl ammatory bowel
disease (IBD). Operative times are shorter and the benefi ts of the laparoscopic approach
are preserved.
◆ Informed consent should address such complications as anastomotic stricture or leak,
bowel obstruction, wound infection at the port sites, intra-abdominal infection, hematoma,
injury to adjacent bowel or mesentery, injury to adjacent structures such as the ureter and
great vessels, port site hernias, and the need for creation of an ostomy.
◆ Preoperative evaluation of the patient’s comorbidities should be obtained, including deter-
mination of nutritional status, evidence of anemia, and cardiac risk factors. Appropriate
laboratory and cardiac evaluations should be obtained.
◆ Patients undergoing resection for malignant or potentially malignant pathologic conditions
should have preoperative staging computed tomography (CT) scan of the chest, abdomen,
and pelvis, with oral and intravenous (IV) contrast, and a baseline carcinoembryonic
antigen (CEA) level drawn. In addition, a complete colonoscopy should be performed to
confi rm location of the lesion and to rule out synchronous lesions.
◆ Aspirin, other blood thinners, and vitamin E should be stopped for 10 days before the
procedure.
◆ A mechanical bowel preparation may be given based on the surgeon’s preference.
◆ An accepted parenteral antibiotic is given within 1 hour of the incision to prevent surgical
site infection on colorectal cases in accordance with the Surgical Care Improvement Project
(SCIP) guidelines. Ertapenem is given once a day and covers the 24-hour postoperative
period.
◆ Prophylaxis for thrombophlebitis is administered either preoperatively or within 24 hours
from surgery in accordance with the SCIP guidelines.
◆ Patients on steroids preoperatively should get a stress dose of IV hydrocortisone 100 mg
before the operation. This should be continued postoperatively and tapered accordingly.

666 Section IX • Colon
◆ Implementing a postoperative colorectal pathway facilitates timely recovery and decreased
length of hospital stay. The pathway is reviewed with the patient to outline expectations for
ambulation and pain control after surgery. It is imperative that patients understand the
importance of ambulation on postoperative return of bowel function.
STEP 3: OPERATIVE STEPS
1. POSITIONING
◆ The patient is placed supine on the operating table on a defl ated bean bag covered with two
hospital sheets.
◆ After general endotracheal anesthesia is administered, a Foley catheter is placed along with
sequential compression devices on the lower extremities.
◆ Depending on the surgeon’s preference, the patient may remain supine or be placed in low
lithotomy using Allen stirrups. Lithotomy allows for additional mobility for the assistant or
the surgeon, should an alternative position be needed.
◆ The arms are padded and tucked so that the top sheet comes over and underneath the bot-
tom sheet. Care is taken to ensure that all IV lines are padded away from the skin to pre-
vent pressure necrosis. The hands are placed in slightly fl exed position with circular roll to
prevent intraoperative movement.
◆ Abdominal and pubic hair is clipped off as needed.
◆ A warmer is placed appropriately to ensure normothermia during the surgery.
◆ An orogastric tube is placed by the anesthesia team for the duration of the procedure, to be
removed upon completion of the procedure.
◆ The surgeon will stand on the patient’s left, with the assistant between the legs or next to
the surgeon on the left.
◆ Monitors are placed on the upper and lower right side of the patient.