Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 60 • Left and Sigmoid Colectomy 677
2. DISSECTION
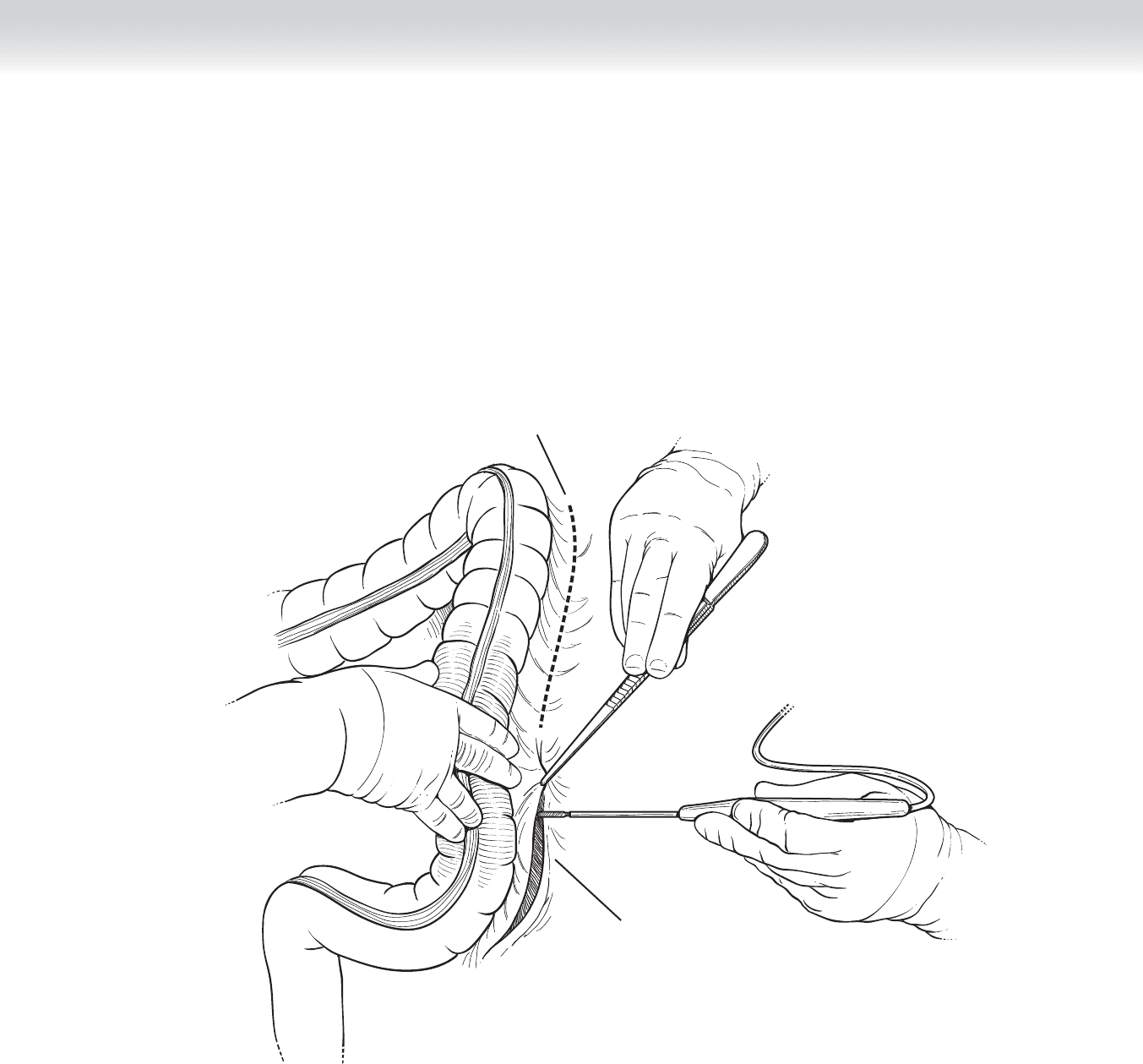
◆ An intra-abdominal exploration is performed to determine the extent of disease and resect-
ability. The small bowel is packed and tucked away to the right upper quadrant of the ab-
dominal cavity. The left colon is mobilized from its retroperitoneal attachments by incising
the white line of Toldt (Figure 60-2).
Lateral peritoneal
attachment
White line of Toldt
FIGURE 60 –2
678 Section IX • Colon
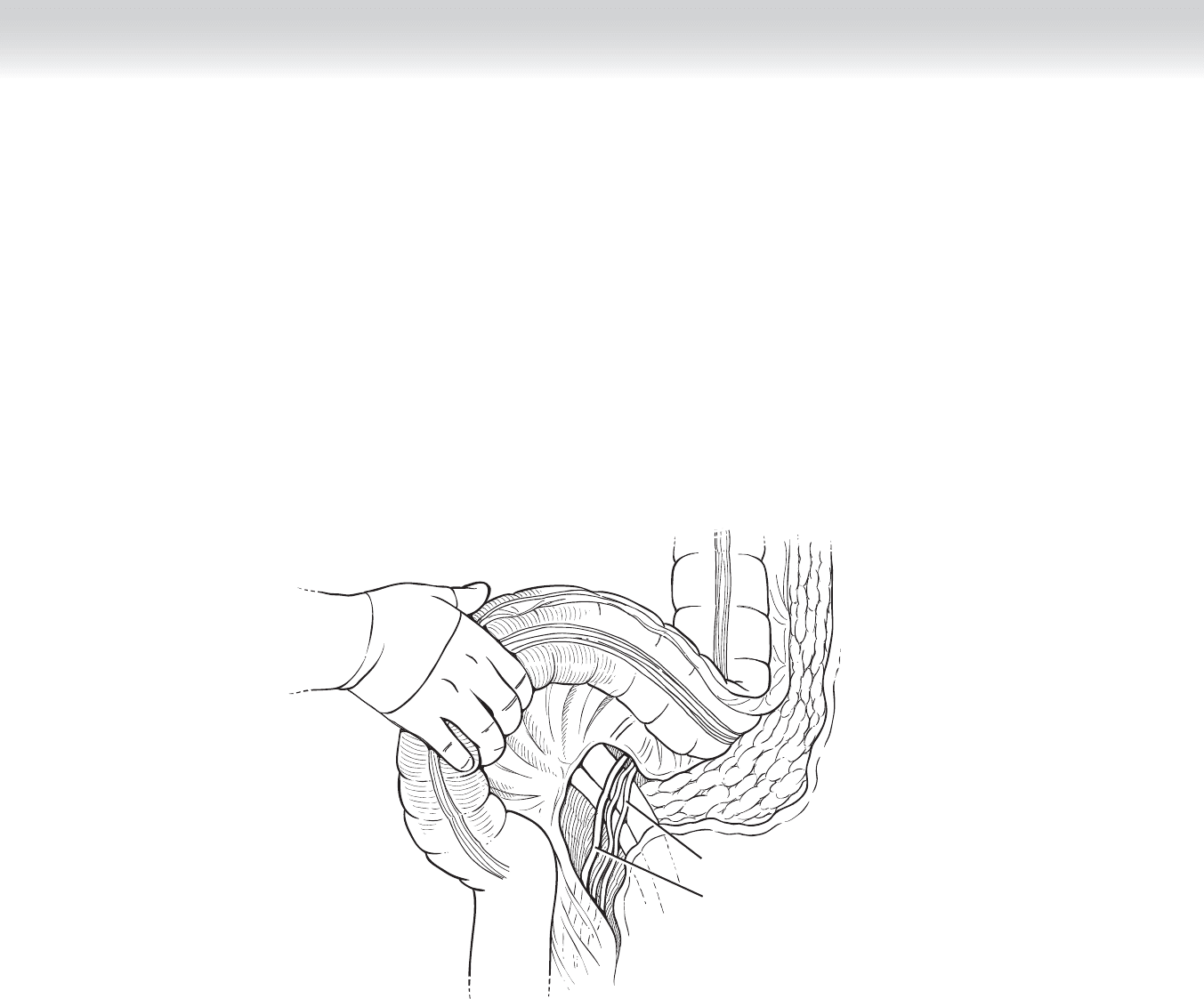
◆ The sigmoid and descending colon is retracted medially, exposing the left ureter and gonadal
vessel (Figure 60-3).
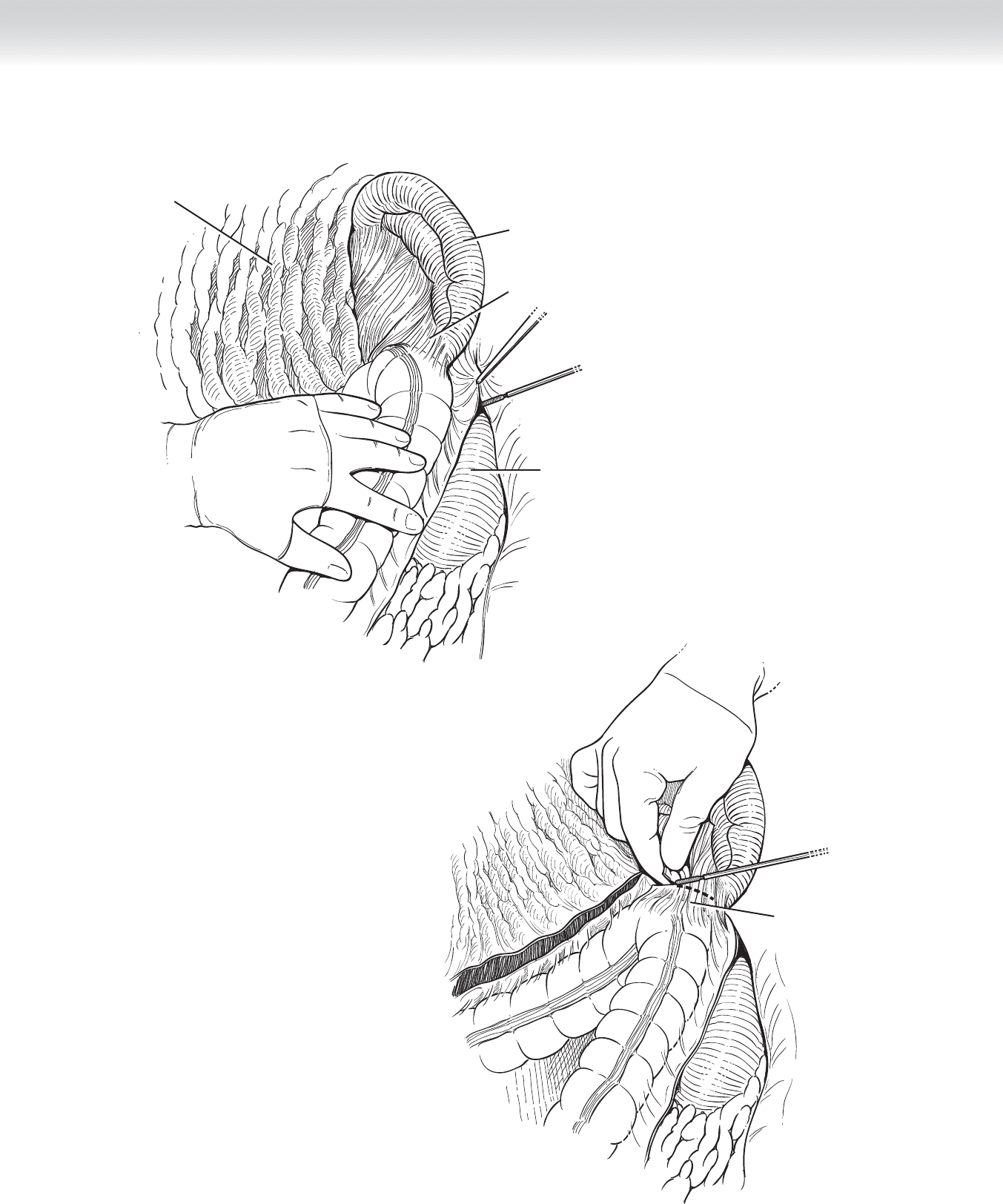
◆ Continuing cephalad along this retroperitoneal plane, divide the renocolic and splenocolic
ligament to release the splenic fl exure (Figures 60-4 and 60-5).
Ureter
Gonadal vessels
FIGURE 60 –3
CHAPTER 60 • Left and Sigmoid Colectomy 679
Splenocolic ligament
FIGURE 60 –5
Spleen
Kidney
Omentum
Splenocolic ligament
FIGURE 60 –4
680 Section IX • Colon
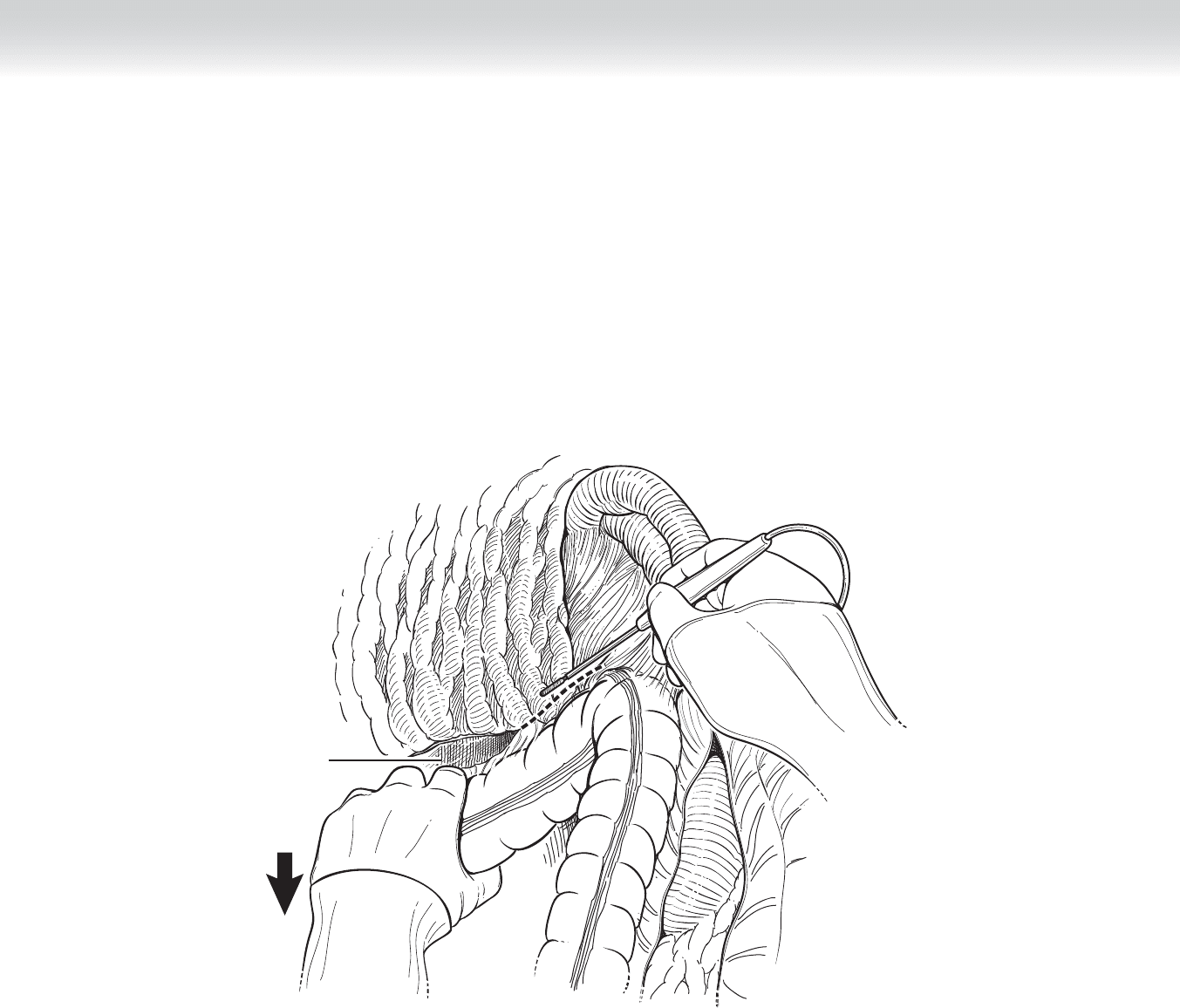
◆ Dissecting from the left aspect of the omentum, mobilize the gastrocolic ligament off the
transverse colon and splenic fl exure (Figure 60-6).
◆ The least traumatic way of taking down the splenic fl exure involves dividing these avascular
ligaments from either side of the splenic fl exure (see Figure 60-5) rather than pulling on the
fl exure with downward traction.
Gastrocolic ligament
incised
FIGURE 60 –6
CHAPTER 60 • Left and Sigmoid Colectomy 681
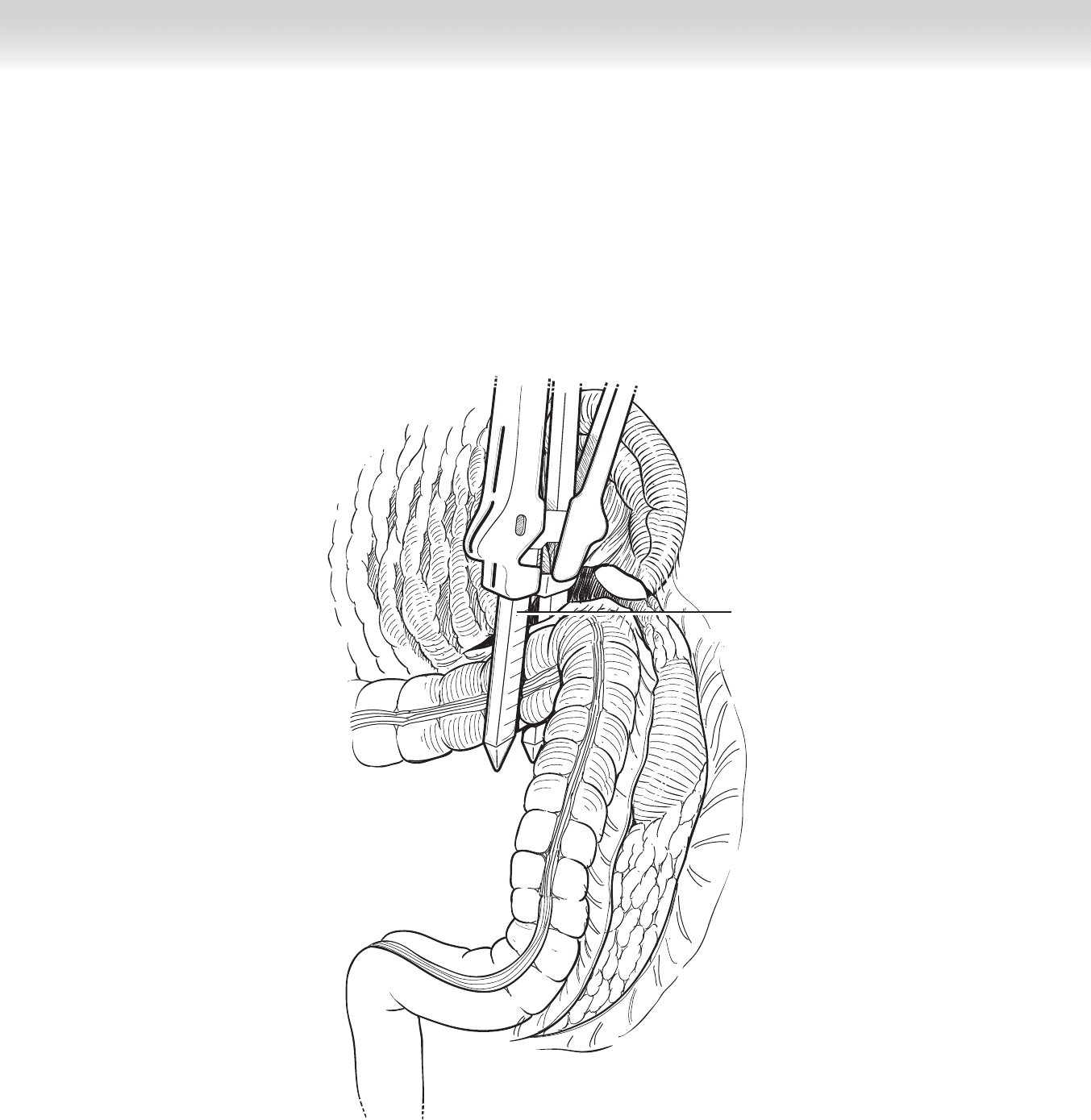
◆ The blood supply to the left colon originates from the inferior mesenteric artery and mainly
involves the left colic artery. The points of transection of the proximal and distal large bowel
are decided upon based on the mesenteric blood supply. The colon is then divided with
the gastrointestinal anastomosis (GIA) stapler at the proximal and distal resection margins
(Figure 60-7). The left colic artery and proximal sigmoid arteries are ligated at their ori-
gins. Careful attention must be paid to the bowel ends to ensure a healthy blood supply
and that the ends would reapproximate without tension.
Bowel divided
with GIA stapler
FIGURE 60 –7
682 Section IX • Colon
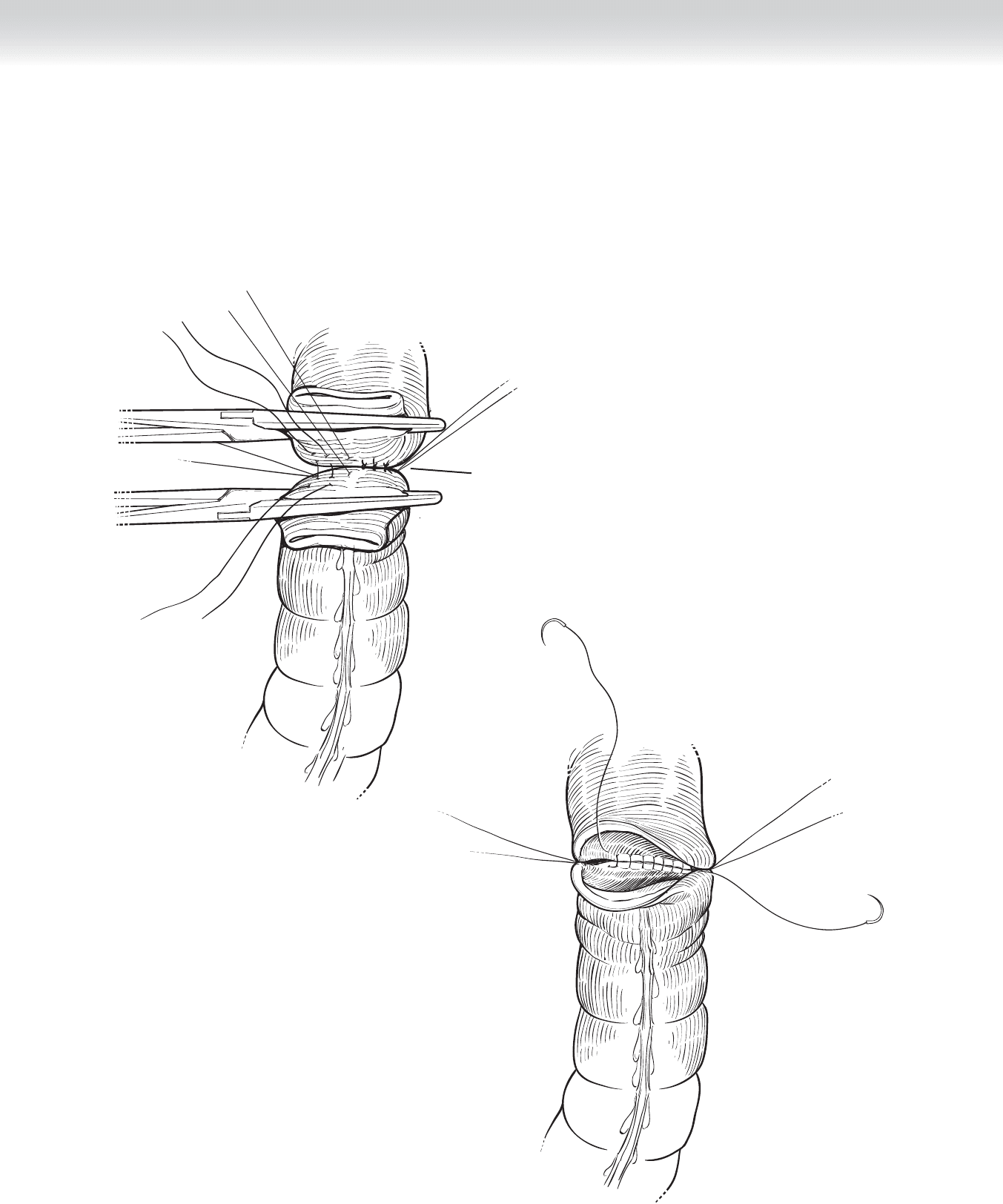
◆ The anastomosis joining the distal transverse and distal sigmoid colon can be hand-sewn
(Figures 60-8 through 60-11) or stapled, as described previously. When performing an
anastomosis using an end of bowel, such as an end-to-end anastomosis, at least a 1-cm
edge of bowel must be cleared of fat, mesentery, and appendices epiploicae, exposing the
serosa.
Posterior layer of interrupted
seromuscular stitches (Lembert)
FIGURE 60 –8
FIGURE 60 –9
CHAPTER 60 • Left and Sigmoid Colectomy 683
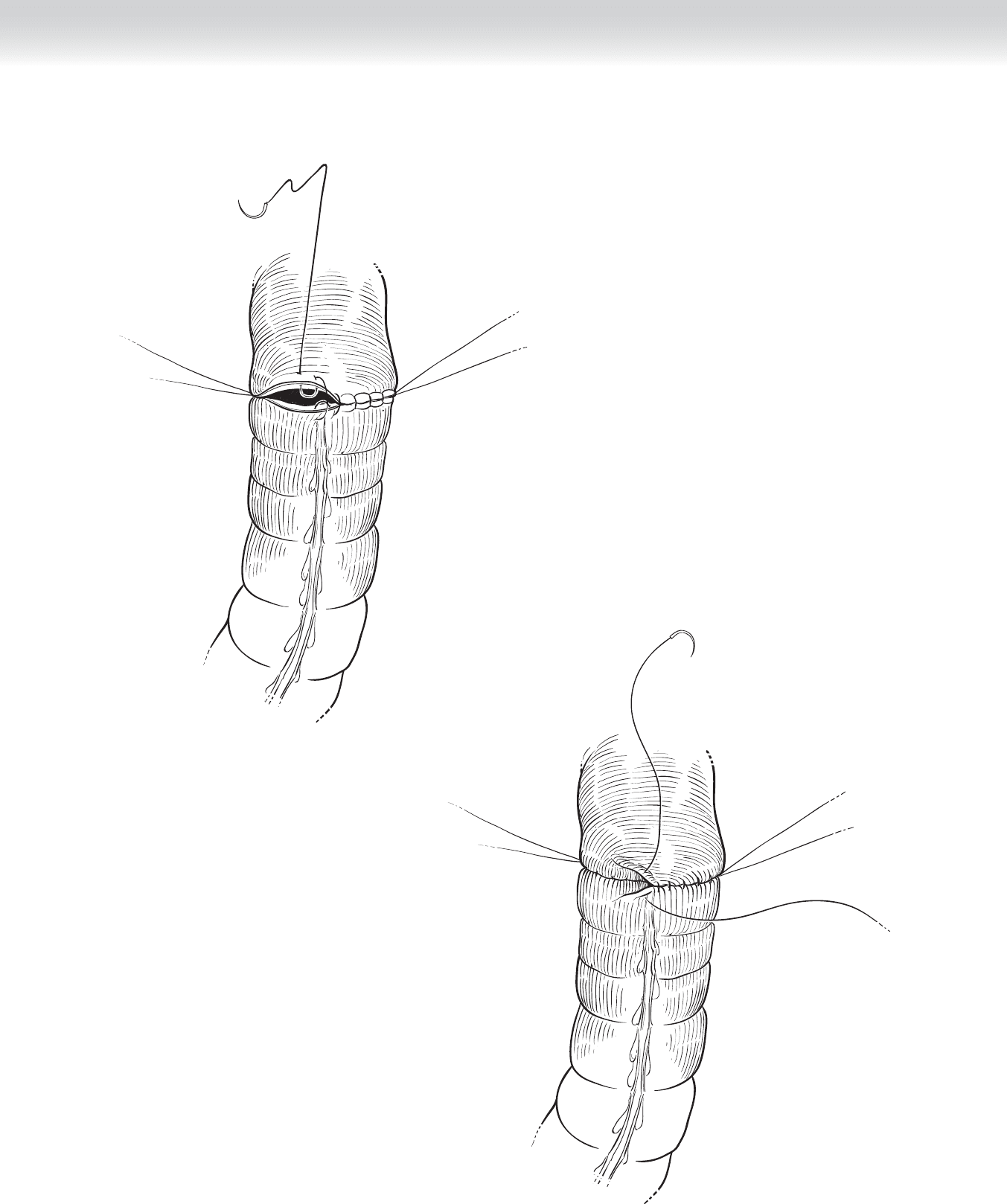
Connell sutures
anterior anastomosis
FIGURE 60 –10
FIGURE 60 –11
Lembert sutures

684 Section IX • Colon
◆ The sigmoid colon may be resected if the tumor is located in the distal descending colon
or sigmoid colon. As the retroperitoneum is exposed, the left ureter should be identifi ed,
typically anterior to the external iliac vessels. The limits of resection are determined: proxi-
mal sigmoid tumors will involve sacrifi ce of branches of the left colic artery, and distal sig-
moid tumors will involve sacrifi ce of branches of the superior rectal artery and transecting
the colon to the level of the sacral promontory. The splenic fl exure may have to be mobi-
lized to create a tension-free anastomosis.
◆ Hand-sewn end-to-end (see Figures 60-8 through 60-11) anastomosis: After noncrushing
bowel clamps are applied proximal to the bowel ends, the staple lines are cut using electro-
cautery or Metzenbaum scissors. In a standard two-layer anastomosis, the posterior (outer)
layer of the transverse colon and proximal rectum are reapproximated with 3-0 silk inter-
rupted (Lembert) sutures. Two continuous absorbable sutures are used in the posterior
inner row (see Figure 60-9), and each is brought anteriorly, where the transition to Connell
sutures is made (see Figure 60-10).
◆ Finally, the anterior (outer) layer is completed with interrupted Lembert sutures (see
Figure 60-11). The mesenteric defect can be reapproximated with a continuous absorb-
able stitch, with care to ensure that the underlying vessels supplying the bowel are not
compromised.
3. CLOSING
◆ The abdominal cavity is irrigated with copious warm saline. The omentum can be overlaid
on top of the newly formed anastomosis. After ensuring hemostasis, sponge counts, and
instrument counts, close the abdomen using a no. 1 polydioxanone (PDS) suture. The sub-
cutaneous tissue is irrigated again, and the skin is closed with skin clips.
STEP 4: POSTOPERATIVE CARE
◆ Ambulation and incentive spirometry on postoperative day 1 is important for the preven-
tion of postoperative atelectasis. Oral intake of clear liquids can begin after removal of the
nasogastric tube. The Foley catheter is left in place for a few days because of the high inci-
dence of urinary retention in male patients.
STEP 5: PEARLS AND PITFALLS
◆ Injury to the spleen: Omental adhesions between the omentum and splenic capsule can
cause inadvertent avulsion or injury to the splenic capsule if traction on the omentum is
applied.
◆ Injury to the left ureter: After division of the renocolic ligament, the left ureter is visualized
in the left retroperitoneum. The entire length of the ureter can be traced down to the pelvis
if necessary.

CHAPTER 60 • Left and Sigmoid Colectomy 685
SELECTED REFERENCES
1. Wille-Jørgensen P, Rasmussen MS, Andersen BR, Borly L: Heparins and mechanical methods for thrombo-
prophylaxis in colorectal surgery. Cochrane Database Syst Rev 2004(4):CD001217.
2. Stahl TJ, Gregorcyk SG, Hyman NH, et al: Practice parameters for the prevention of venous thrombosis.
Dis Colon Rectum 2006;49:1477-1483.
686
STEP 1: SURGICAL ANATOMY
◆ The descending colon is covered by peritoneum on the anterior and lateral surfaces and
attaches to the retroperitoneum on the posterior side.
◆ Structures beneath the descending colon include the left kidney, the proximal ureter, and
the inferior mesenteric vein.
◆ The splenic fl exure is much higher than the hepatic fl exure, a consideration to be noted when
placing ports for laparoscopic dissection. Mobilization of the fl exure requires division of the
lienocolic ligament, a maneuver that must be carefully done to prevent splenic capsular tear.
◆ The main blood supply to the left colon includes the left colic artery and the superior
sigmoid arteries. Collateral fl ow may be provided by the marginal arteries and the arc of
Riolan, a meandering artery from the middle colic artery to the inferior mesenteric artery.
◆ The sigmoid colon is highly mobile, typically with a long mesentery and variable length. It
is completely covered by peritoneum and is attached to the abdominal wall by the lateral
peritoneal attachment called the “white line of Toldt,” which extends upward to include
attachment of the left colon, as well. Preservation of this attachment allows for countertrac-
tion during laparoscopic mobilization.
◆ The blood supply of the sigmoid colon includes the inferior mesenteric artery and its sig-
moidal branches.
◆ The intersigmoid fossa is a recess at the base of the mesosigmoid that provides an anatomic
landmark for locating the left ureter, which courses beneath the fossa and parallel just
medial to the gonadal vein.
◆ The superior hypogastric plexus provides sympathetic innervation for erectile function and is
situated at the bifurcation of the aorta in close proximity to the inferior mesenteric artery (IMA)
CHAPTER
61
Left and Sigmoid Colectomy
(Laparoscopic-Assisted)
Valerie P. Bauer