Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 61 • Left and Sigmoid Colectomy (Laparoscopic-Assisted) 697
◆ The clamp is pulled through, taking care that there are no twists in the mesentery and no
tension on the colostomy.
◆ The colostomy is matured in standard fashion after the abdomen is closed and the midline
incision is protected.
4. CLOSING
◆ Surgical gloves are changed, and the Alexis wound retractor is removed, as are all other
ports. Seprafi lm is placed, and the anterior rectus fascia is reapproximated using 0
polydioxanone (PDS) in fi gure-of-eight interrupted sutures.
◆ The subcutaneous skin is irrigated with bacitracin antibiotic (50,000 U in 1 L saline).
◆ Staples are used to close the skin. A small umbilical bolster is created by placing a bacitracin-
soaked cotton ball wrapped in Adaptic into the umbilical depression. This is left in place
during the hospital stay and removed before discharge home.
◆ The orogastric tube is removed before extubation. A nasogastric tube should be placed if
there is extensive lysis of adhesions or other indication for maintenance of a nasogastric
tube postoperatively.
STEP 4: POSTOPERATIVE CARE
◆ The same principles of postoperative care followed for laparoscopic-assisted right colectomy
apply to laparoscopic-assisted left and sigmoid colectomy, and can be referred to in
Chapter 59.
STEP 5: PEARLS AND PITFALLS
◆ Division of the left colic artery may be necessary for adequate mobilization in creating a
tension-free anastomosis. The ascending branch of the left colic artery should be preserved,
allowing collateral fl ow from the middle colic artery back to the ascending left colic artery
through the marginal arteries.
◆ Oncologic resection of the sigmoid colon mandates attention to preserve the meandering
artery of Riolan during high ligation of the IMA for maintaining collateral blood fl ow to the
proximal left colon.

698 Section IX • Colon
◆ Consideration for placement of ureteral stents should be made for cases involving complicated
diverticulitis or large bulky tumors. Although stents have not been shown to prevent injury,
palpation of the stent may assist in timely recognition of ureteral location. In addition, injuries
may be identifi ed earlier during the intraoperative period by visualization of the stent, thus
facilitating repair.
◆ The left ureter should be visualized and swept laterally before division of the IMA pedicle.
Failure to do this may involve inclusion of the ureter with the pedicle, leading to one of the
most common causes of ureteral injury during this procedure.
◆ High ligation of the IMA pedicle may injure the superior hypogatric (sympathetic) plexus
because of entrapment and division of the nerves. This results in retrograde ejaculation.
Care should be taken to identify the nerves and dissect them laterally before division of the
pedicle.
◆ A lip of omentum may be mobilized to buttress the anastomosis, a consideration to make if
the tissues are infl amed or friable.
◆ The inferior epigastric artery may be visualized and avoided before making the incision for
an ostomy by transillumination of the anterior abdominal wall with the laparoscopic light.
◆ Tension on the ileostomy due to foreshortened mesentery or large abdominal pannus may
be relieved by mobilization of the right colon.
SELECTED REFERENCES
1. Aalbers AG, Biere SS, van Berge Henegouwen MI, Bemelman WA: Hand-assisted or laparoscopic-assisted
approach in colorectal surgery: A systematic review and meta-analysis. Surg Endosc 2008; 22:1769-1780.
2. Guidelines from the Joint Commission on Surgical Care Improvement Project Core Measurement Set.
Available on the Internet: www.jointcommission.org/PerformanceMeasurement.
3. Zeng Q, Yu Z, You J, Zhang Q: Effi cacy and safety of Seprafi lm for preventing postoperative abdominal
adhesion: Systematic review and meta-analysis. World J Surg 2007;31:2125-2131;2132 [discussion].
699
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the anatomy of the abdomen is critical before undertak-
ing total abdominal colectomy (Figure 62-1).
◆ The relationship of the colon to intraperitoneal and retroperitoneal attachments and struc-
tures should be fully understood.
◆ Particular attention should be paid to the location of the left ureter relative to the inferior mes-
enteric vascular pedicle. This is the most commonly injured area after vascular pedicle ligation.
CHAPTER
62
Total Colectomy
Valerie P. Bauer
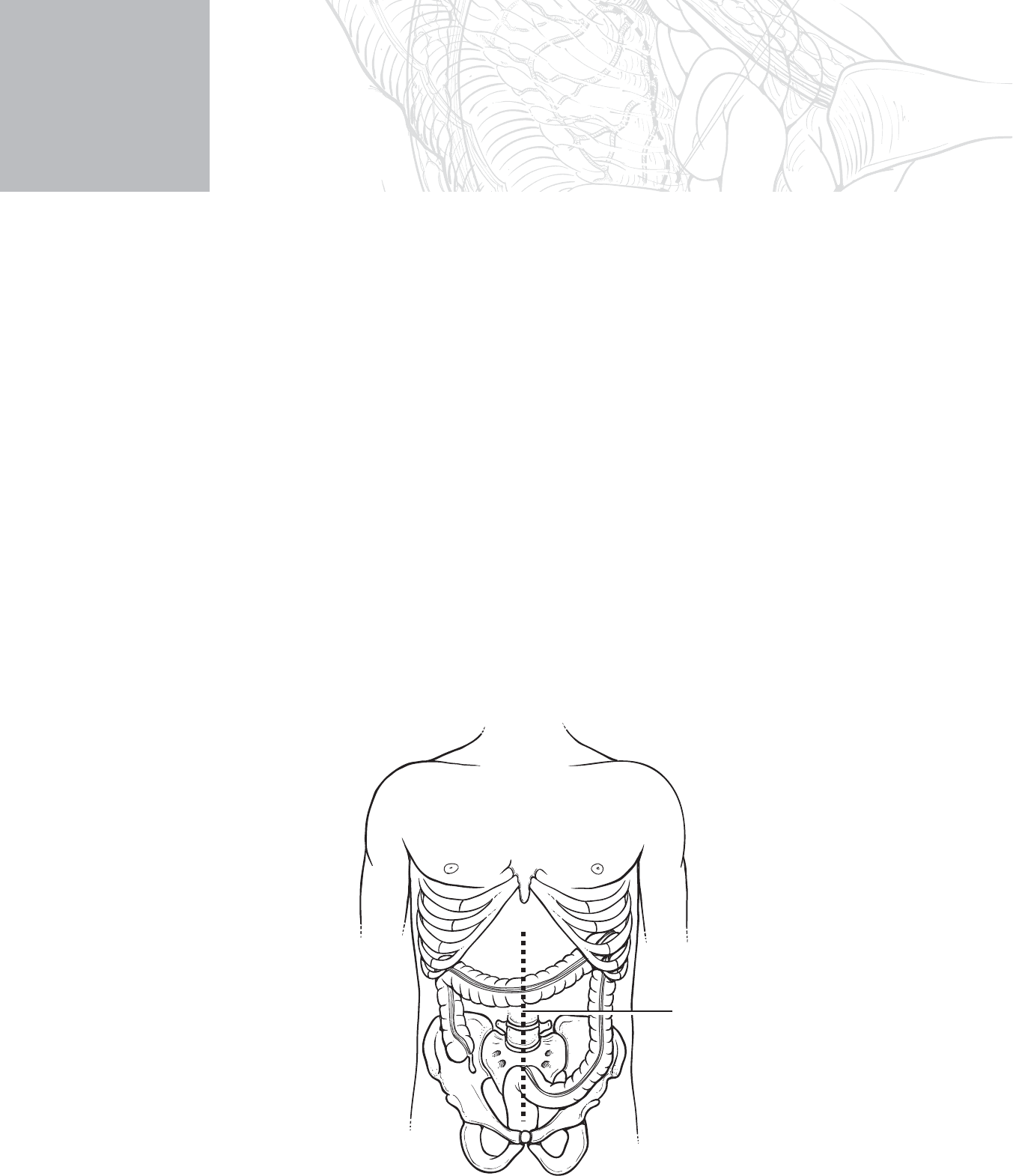
Incision
FIGURE 62–1

700 Section IX • Colon
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for total abdominal colectomy involve both emergent and elective scenarios for
treatment of:
◆ Ulcerative colitis
◆ Crohn’s disease of the large bowel with sparing of the distal sigmoid colon and rectum
◆ Attenuated familial adenomatous polyposis
◆ Synchronous multiple cancers
◆ Perforated cecum due to distal colon cancer obstruction
◆ Constipation
◆ Bowel continuity may or may not be restored depending on the clinical circumstance.
◆ If temporary or permanent ileostomy is planned, the patient should be marked preopera-
tively for either an end or loop ileostomy and educated concerning the new ostomy.
◆ Consideration for ureteral stenting should be made based on the extent of disease and prior
abdominal operations.
◆ Aspirin, other blood thinners, and vitamin E should be stopped for 10 days before the
procedure.
◆ Preoperative laboratory and cardiac evaluations should be obtained based on patient
comorbidities.
◆ Patients taking steroids preoperatively should receive a stress dose of hydrocortisone
100 mg intravenously (IV) before the operation. This should be continued postoperatively
and tapered accordingly.
◆ Consideration toward placing an epidural catheter preoperatively should be made for post-
operative pain control and minimization of parenteral narcotic use and associated postoper-
ative ileus.
◆ Bowel preparation should include mechanical bowel preparation of the surgeon’s choice.
Sodium phosphate bowel preparations should be used with caution because of acute phos-
phate nephropathy.
◆ Appropriate preoperative antibiotics are administered parenterally within 1 hour before cut
time, according to the Surgical Care Improvement Project (SCIP) quality measures defi ned
for elective colorectal operations. We use ertapenem (Invanz) 1 g IV without redosing,
because it has 24-hour duration of action.

CHAPTER 62 • Total Colectomy 701
STEP 3: OPERATIVE STEPS
1. POSITIONING
◆ Proper positioning of the patient should be directed by the primary surgeon to ensure con-
sistency and safety to the patient.
◆ The patient should be placed supine on the operating table. After administration of anes-
thesia, sequential compression devices should be placed on the legs and a Foley catheter
inserted. The legs are placed in low lithotomy position with Allen stirrups. The boots are
adjusted so that each leg rests in a fl exed position without pressure on the popliteal fossa.
Padding is used to shield the skin from all hard objects.
◆ Abdominal and pubic hair is clipped off.
◆ A Bair Hugger Warmer is placed across the patient’s chest.
◆ An orogastric tube is placed, to be removed after surgery unless a nasogastric tube is indi-
cated, as in cases of extensive lysis of adhesions.
◆ Rigid proctoscopy is performed to clean the rectum of residual stool and to confi rm absence
of pathologic fi ndings in the rectum that may need to be addressed in the operating room.
◆ The abdomen and perineum are prepped in standard fashion according to the surgeon’s
preference. The scrotum should be positioned away from the perineum.
702 Section IX • Colon
2. INCISION
◆ The pubic symphysis and manubrial notch are palpated and marked. A line is drawn down
the entire midline in case the incision needs to be extended during the later part of the pro-
cedure (Figure 62-2).
◆ A no. 10 blade knife is used to make an incision from a point 2 cm above the umbilicus
down to the pubic symphysis.
◆ The abdomen is entered sharply. Care is taken to dissect around the bladder obliquely. The
incision is extended through the pyramidalis muscle to the pubic symphysis.
◆ The abdomen is explored for additional pathologic abnormalities. The terminal ileum is
identifi ed and the entire small bowel is run proximally to the ligament of Treitz. The liver is
palpated for the presence of masses.
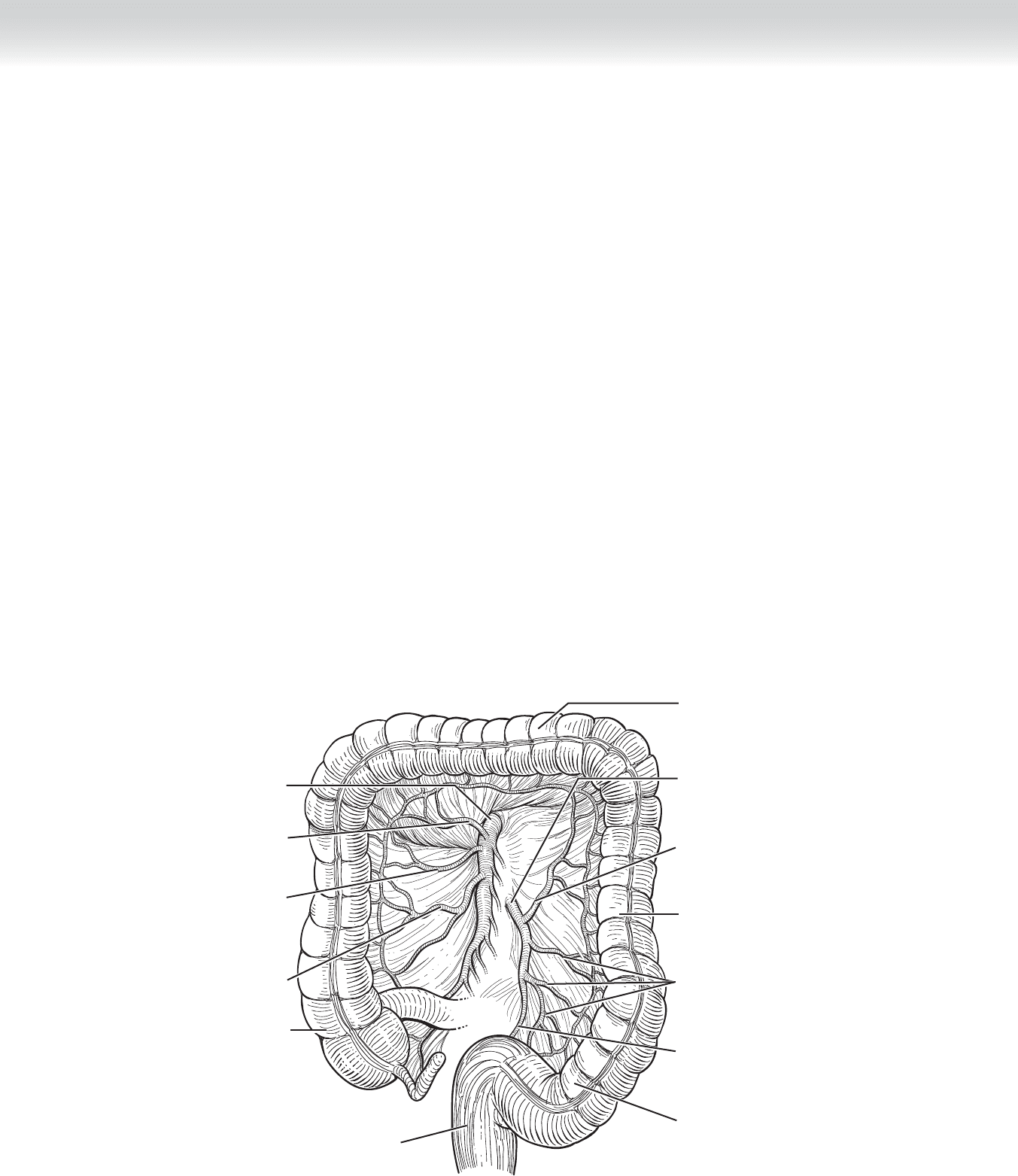
Transverse colon
Descending colon
Ascending colon
Sigmoid colon
Inferior mesenteric artery
Superior rectal artery
Superior mesenteric artery
Middle colic artery
Right colic artery
Left colic artery
Ileocolic artery
Sigmoid arteries
Rectum
FIGURE 62–2
CHAPTER 62 • Total Colectomy 703
3. DISSECTION
◆ A Bookwalter retractor is set up. Laparotomy pads are placed along each side of the
abdominal wall. Two ratcheted short Richardson retractors are positioned opposite each
other in lower oblique fashion, taking care not to impinge on the femoral canal.
◆ The small bowel is packed upward using a moist blue towel with a radiopaque loop
attached to it, and a wide Deaver ratcheted retractor is bent and placed to maintain
exposure without compression of the aorta or inferior vena cava.
◆ In female patients, the uterus should be retracted by placing a fi gure-of-eight stitch with
2-0 Vicryl through the posterior wall of the uterus as a retraction stitch. A ratcheted bladder
blade is then placed to retract the uterus and bladder.
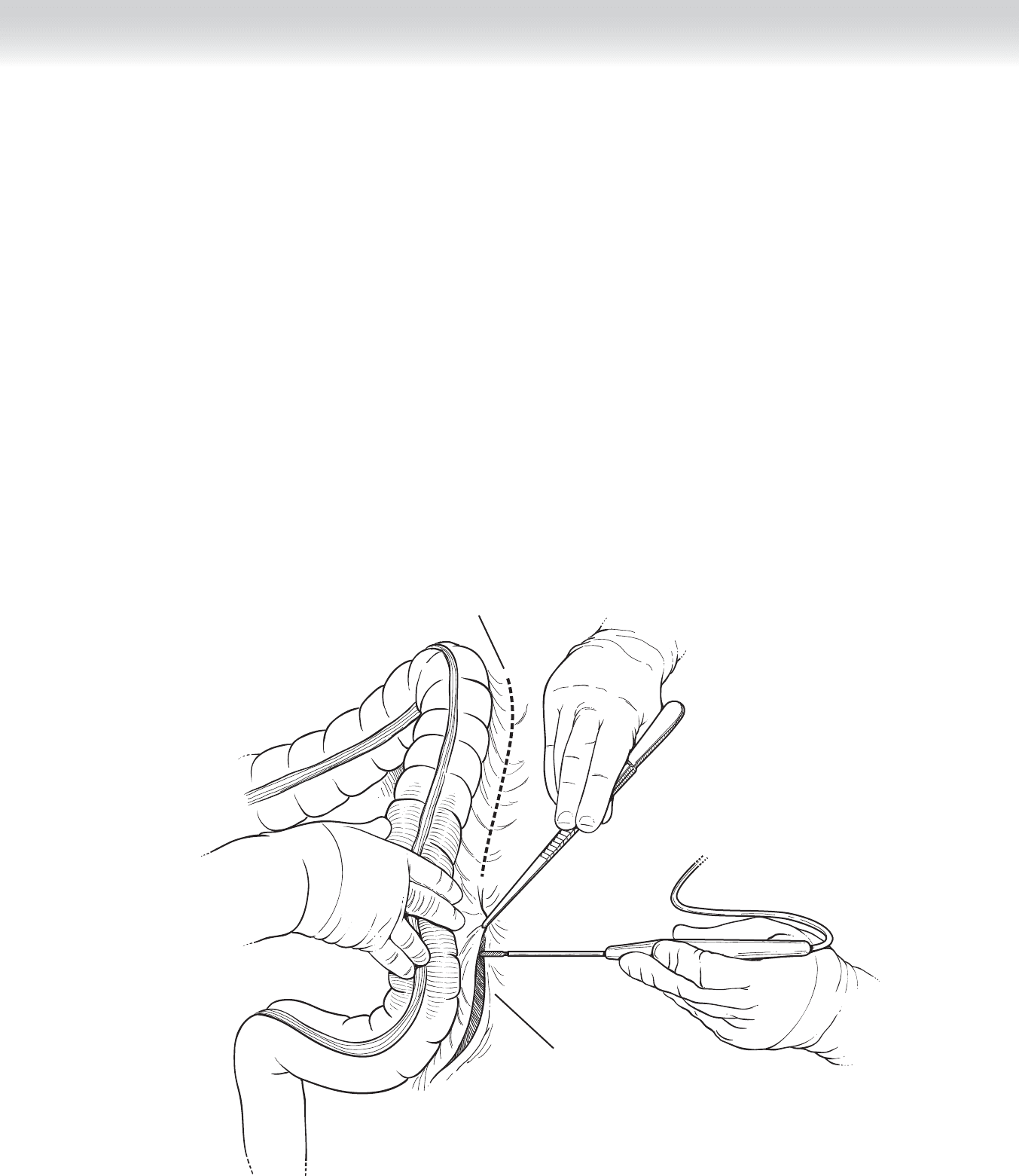
◆ The surgeon on the right side of the patient pulls up on the sigmoid colon so that the lateral
peritoneal attachment is on tension (Figure 62-3). Electrocautery is used to divide the
attachment.
Lateral peritoneal
attachment
White line of Toldt
FIGURE 62–3
704 Section IX • Colon
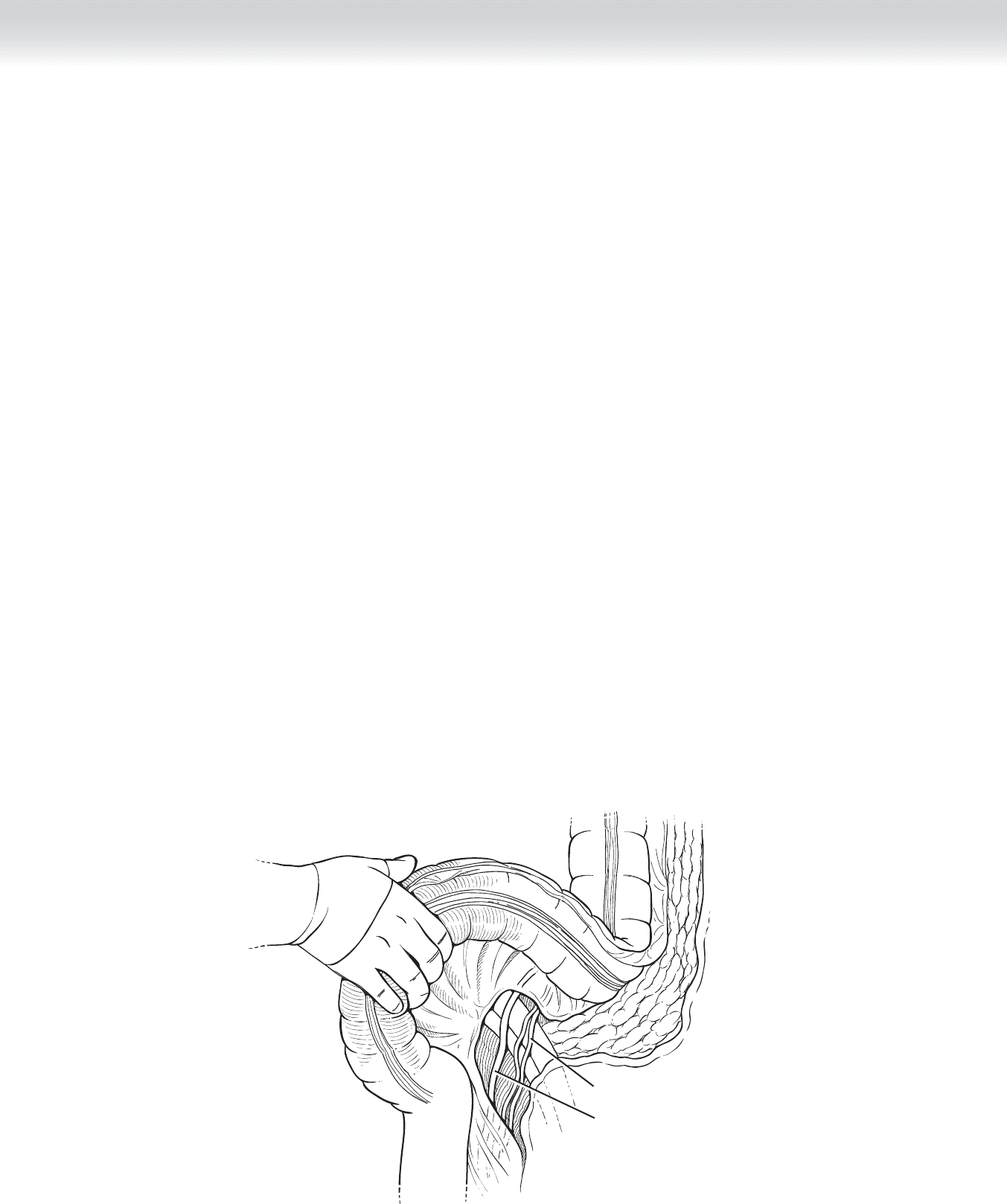
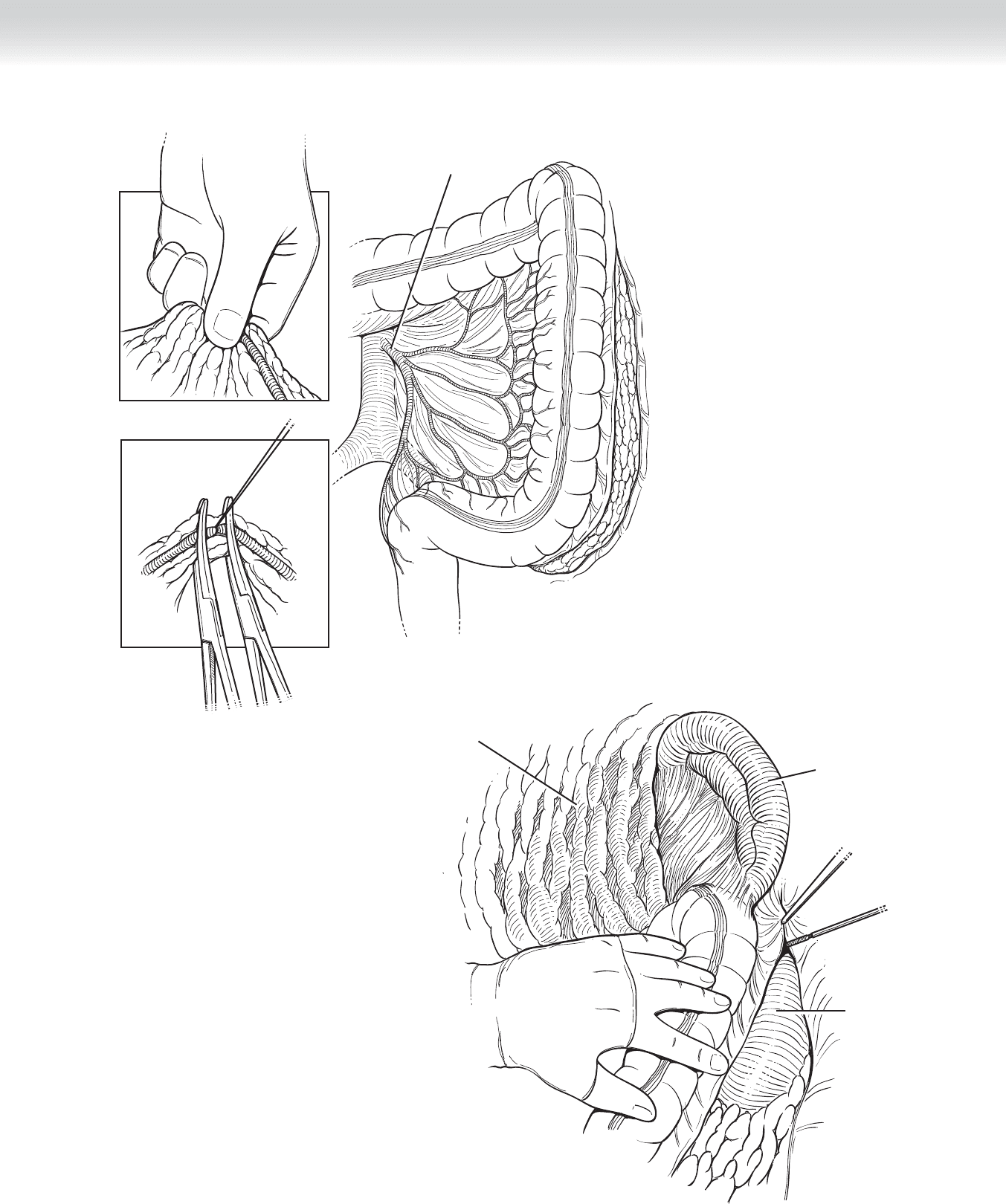
◆ The recess at the base of the mesosigmoid, called the intersigmoid fossa, is identifi ed and
delicately incised. The left ureter lies just deep to it and is identifi ed and mobilized laterally.
The ureter courses medially and parallel to the gonadal vessels, another important land-
mark to identify (Figure 62-4).
◆ The surgeon to the left of the patient isolates the inferior mesenteric pedicle. This is done
by identifying the avascular window at the base of the mesosigmoid while tenting the mes-
entery up. The window is incised against the surgeon’s fi nger from the right with electro-
cautery, and is extended proximally to the pelvic brim and distally down to the level of the
sacral promontory bilaterally.
◆ The peritoneal covering of pedicle is cut, and excess mesenteric fat is thinned in preparation
for ligation.
◆ Seurat clamps are used to divide the pedicle. A 2-0 Vicryl tie is used to ligate both the base
and specimen side of the pedicle. If the artery feels calcifi ed or has atherosclerotic plaque
visibly extruding from the vessel after clamping, a 2-0 Vicryl stick tie should be placed to
ensure hemostasis of the pedicle base (Figure 62-5).
◆ The rectosigmoid mesentery is sequentially clamped, divided, and ligated to the serosal
edge of the colon. The surface is cleaned of excess mesenteric and epiploic fat in prepara-
tion for division.
◆ Before division, the left colon is mobilized as much as possible by being divided from its
retroperitoneal lateral attachments upward toward the spleen (Figure 62-6).
Ureter
Gonadal vessels
FIGURE 62–4
CHAPTER 62 • Total Colectomy 705
Inferior mesentery artery
FIGURE 62–5
Spleen
Kidney
Omentum
FIGURE 62–6
706 Section IX • Colon
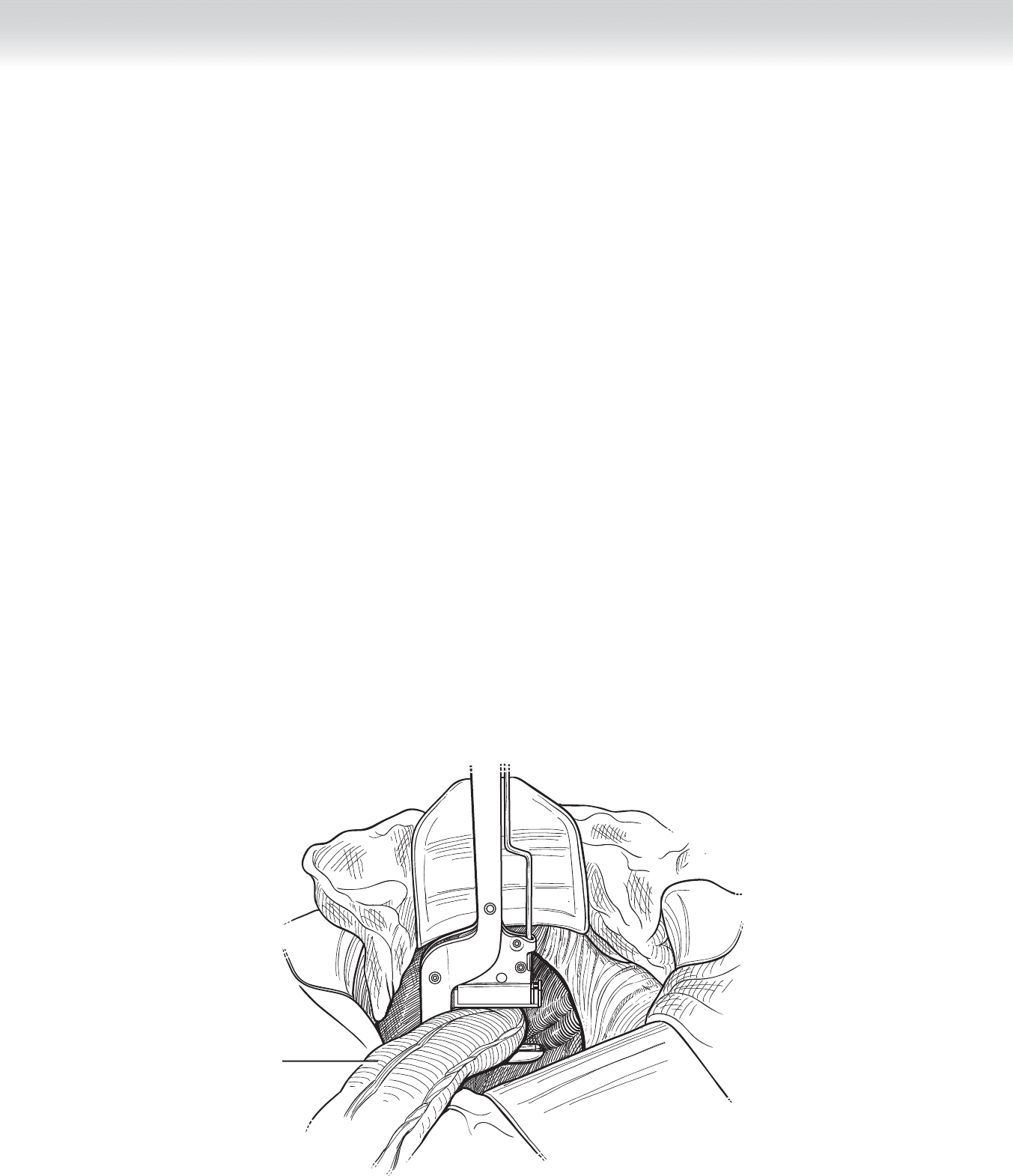
◆ Method of division of the rectosigmoid depends on whether intestinal continuity will be
reestablished. Either a linear stapler or division between two Ochsner bowel clamps may be
used to divide the bowel at the level of the sacral promontory (Figure 62-7). The proximal
rectosigmoid end is wrapped with a laparotomy pad and may be clamped if there is con-
cern for fecal leakage through the staple line during mobilization. The distal stump is
marked with a 2-0 Prolene suture for future recognition if reversal is a possibility.
◆ The Deaver blade is removed along with the blue towel. The transverse colon is pulled
downward, and the lesser sac entered by incising the fi lmy attachment of the gastrocolic lig-
ament to the colon (Figure 62-8).
◆ The splenic fl exure is mobilized by the surgeon standing on the patient’s right side. The
assistant may move to the position between the patient’s legs for improved visualization.
The splenocolic ligament is divided close to the bowel wall to avoid injury to the spleen
(Figure 62-9).
◆ Once the splenic fl exure is down, the remainder of the gastrocolic ligament is detached
from the transverse colon.
◆ Attention is then turned to the right colon. The small bowel may be loosely packed away,
once again, depending on the surgeon’s preference.
Division of the
rectosigmoid
FIGURE 62–7