Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 62 • Total Colectomy 707
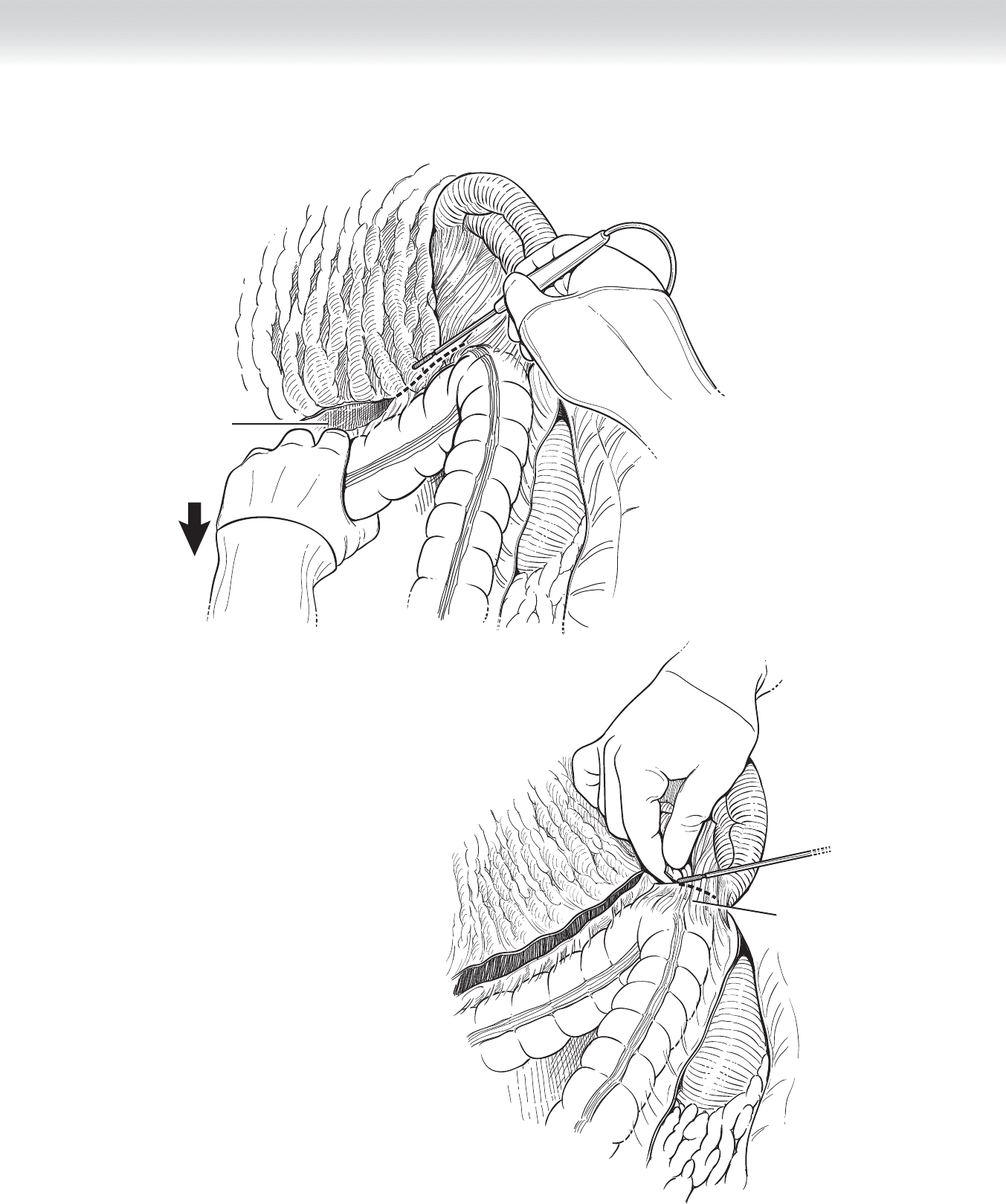
Gastrocolic ligament
incised
Splenocolic ligament
FIGURE 62–8
FIGURE 62–9
708 Section IX • Colon
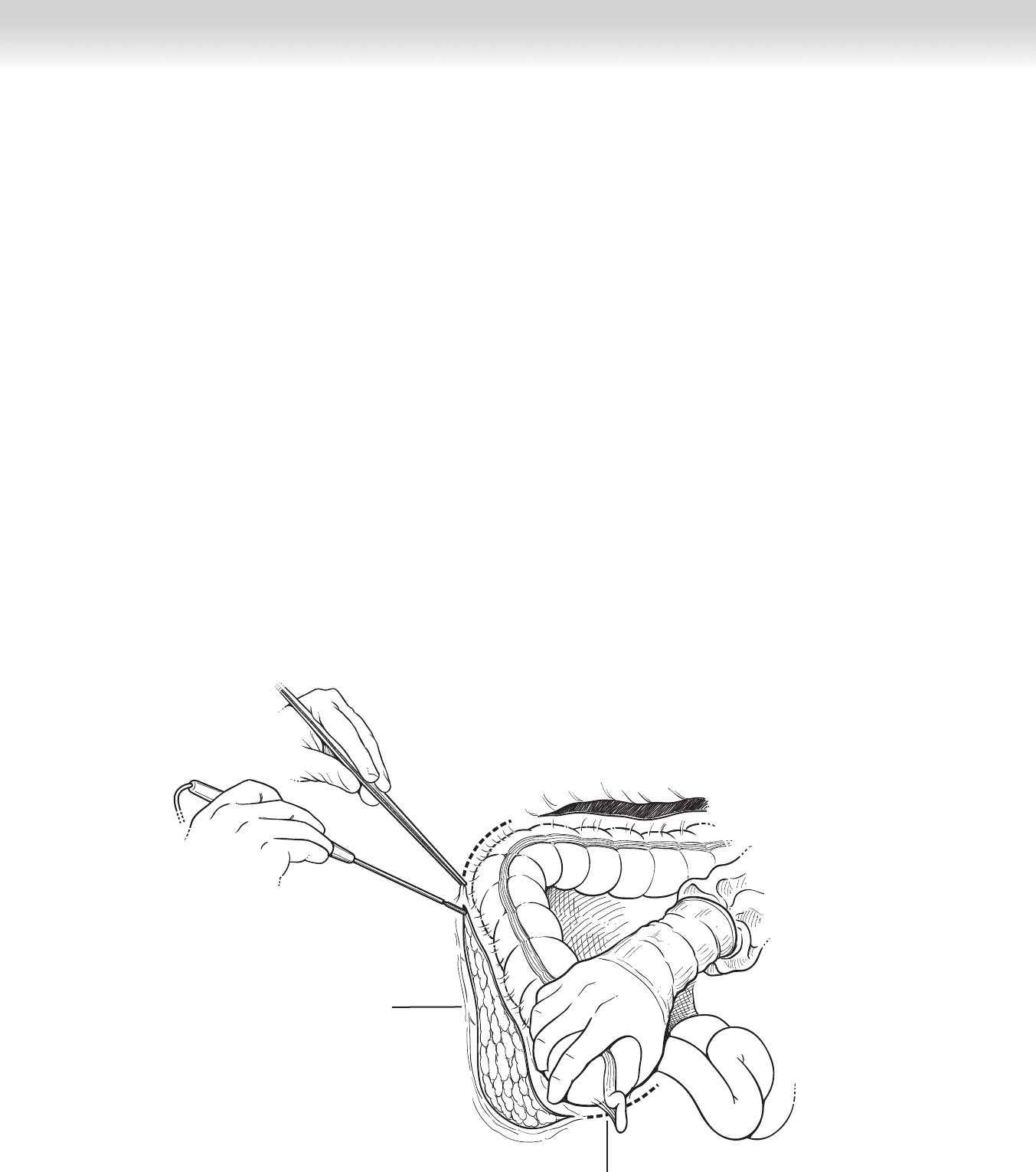
◆ The cecum is retracted up away from the pelvic brim. The lateral peritoneal attachment is
divided, and gentle blunt dissection is used to separate the ascending colon from the retro-
peritoneum. The duodenum is identifi ed and dissected downward and away from colonic
mesentery (Figure 62-10).
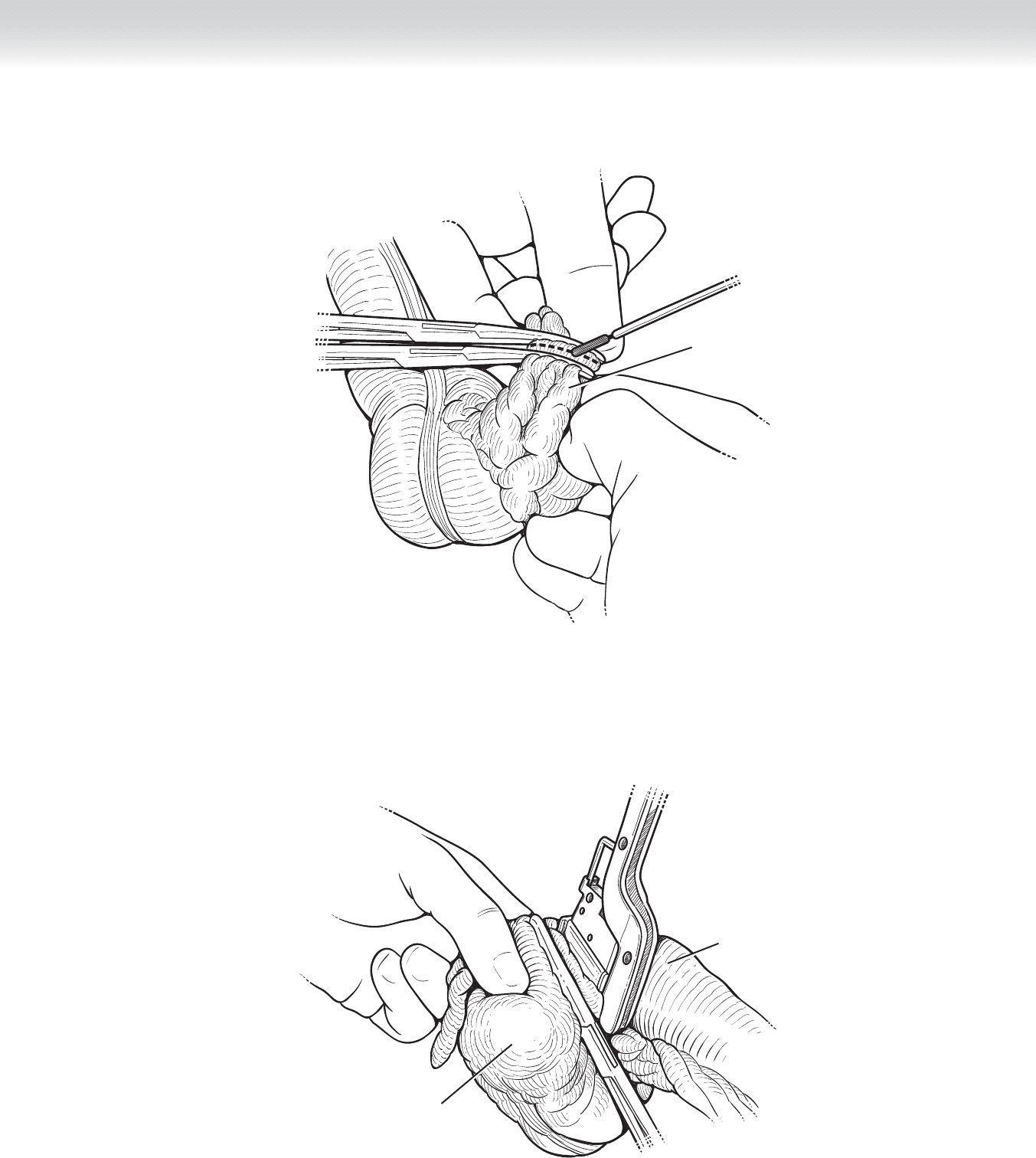
◆ The phrenocolic and hepatocolic ligaments are clamped, divided, and ligated using 2-0 Vicryl
suture.
◆ The ligament of Treves is identifi ed and divided along with the parietal peritoneum of the
terminal ileum. The ileocolic vascular pedicle is identifi ed, clamped, divided, and ligated in
similar fashion, as mentioned earlier (Figure 62-11).
◆ The mesentery is scored to the point of ileal resection. The vascular arcades are clamped,
divided, and ligated, and the ileum is divided between two Ochsner clamps.
◆ It is important to note that the method of pedicle ligation and mesenteric division will
vary drastically for patients with ulcerative colitis. The possibility of having an ileal anal
pouch in the future mandates that ileal length and vasculature be preserved. In this cir-
cumstance, the ileocolic artery is preserved, and the mesentery is divided close to the right
colon (Figure 62-12).
Cecal recess
Division of
lateral peritoneal
attachment
FIGURE 62–10
CHAPTER 62 • Total Colectomy 709
Ileocolic pedicle
FIGURE 62–11
Terminal ileum
Cecum
FIGURE 62–12

710 Section IX • Colon
◆ The remaining vascular pedicles of the ascending, transverse, and descending colon are
sequentially visualized, clamped, divided, and ligated. Remaining proximal to the vessels
decreases the number of vessels that need to be divided.
◆ The specimen is removed from the table and opened off the fi eld to confi rm pathologic
fi ndings and rule out additional fi ndings.
◆ All laparotomy pads are removed from the abdomen, and the Bookwalter retractor is taken
down. If a retraction stitch was placed in the uterus, the stitch should be tied down to pre-
vent bleeding from the myometrium.
◆ The abdomen is irrigated with warm sterile saline.
Brooke Ileostomy
◆ Two Ochsner clamps are placed on the anterior fascia of the rectus muscle, and an Allys
clamp is placed on the skin between the two. The assistant maintains even traction so that
all layers are parallel and aligned.
◆ An Ochsner clamp is placed on the skin over the ileostomy site and pulled up. A no. 10
blade knife is used to cut out a circular disc. The ileostomy is placed through the summit of
the infraumbilical bulge through the split thickness of the rectus muscle. Electrocautery is
used to cut through the subcutaneous tissue down to the anterior fascia of the rectus mus-
cle, which is sharply divided. Muscle fi bers are spread perpendicularly, and the peritoneum
is cut longitudinally enough to snugly fi t two fi ngers. Injury to the inferior epigastric vessels
should be avoided.
◆ The ileostomy is brought out of the abdominal cavity for a length of approximately 5 cm,
taking care not to twist the mesentery. If the ileostomy is temporary, it should be wrapped
in a sheet of Seprafi lm to prevent adhesions and facilitate takedown in the future.
◆ The abdomen is closed before the ileostomy is matured (see following section, Abdominal
Closure), and the incision is protected with a clean, dry towel.
◆ Stitches using 2-0 chromic are placed through the mucosa at points equidistant from each
other and through the seromuscular layer proximally at the skin level. The ileostomy is
everted so that the end falls away from the mucocutaneous junction. The appliance is cut
to fi t circumferentially so that there are no gaps exposing the skin.
Ileorectal Anastomosis
◆ The decision to restore bowel continuity depends on the primary diagnosis and clinical
scenario.
◆ Dissection for ileorectal anastomosis differs in sequence from the previously mentioned
steps in that the operation begins with takedown of the right colon and proceeds clockwise
to the fi nal step of division of the sigmoid colon from the rectum.

CHAPTER 62 • Total Colectomy 711
◆ Preparation for open lumen of bowl mandates meticulous attention to detail to prevent fecal
spillage into the abdominal cavity. A blue towel is folded and placed on the fi eld, which will
contain contaminated instruments: a metal pool sucker, Allys bowel clamps, and sponge
stick. Moist laparotomy pads are packed around the rectum.
◆ A Glassman clamp is placed across the distal sigmoid colon, and a knife is used to detach
the colon. Allys clamps are placed on the mesenteric and antimesenteric edges of the open
lumen of bowel, and a sponge stick is used to blot and clean the edges.
◆ The terminal ileum is similarly divided off the Ochsner clamp and grasped with Allys
clamps. Care is taken to place the Ochsner obliquely on the small bowel to match the size
of the rectum. A Cheatle incision may be made on the antimesenteric border to enlarge the
lumen.
◆ The antimesenteric and mesenteric borders of each lumen are lined up. Care is taken to
ensure that the small bowel is not twisted around its mesentery.
◆ A double-armed 4-0 Maxon monofi lament suture is used to create a single-layered running
anastomosis.
◆ The integrity of the anastomosis may be checked using the proctoscope to insuffl ate
through the rectum while submerged under saline. Presence of bubbles requires single
interrupted sutures to repair the leak.
◆ The surgeons’ gloves are changed before skin closure.
4. ABDOMINAL CLOSURE
◆ The omentum is moved to the side and placed in either paracolic gutter. One sheet of
Seprafi lm is cut in half and placed over the bowel under the incision. This minimizes adhe-
sion formation and makes reentry easier for future operations.
◆ The abdomen is closed using no. 1 polydioxanone (PDS) running suture.
◆ The subcutaneous tissue is irrigated with bacitracin irrigation, and the skin is closed with
staples.
◆ The umbilicus is reapproximated. A bacitracin-soaked cotton ball wrapped in Adaptic is
packed into the umbilicus as a bolster.

712 Section IX • Colon
STEP 4: POSTOPERATIVE CARE
◆ Adherence to a postoperative colorectal clinical pathway ensures standardization of care.
◆ Adequate pain control is achieved using patient-controlled analgesia or epidural catheter.
◆ Stress ulcer prophylaxis, such as famotidine (Pepcid) 20 mg IV every 12 hours, should be
used if indicated.
◆ All patients should receive prophylaxis for deep venous thrombosis, consisting of sequential
compression devices while in bed and heparin 5000 U subcutaneously every 8 hours or
enoxaparin 40 mg subcutaneously within 24 hours of surgery. Dosing schedules should
start on postoperative day 1 after results of morning laboratory tests are back to ensure that
there is no signifi cant drop in hemoglobin to suggest postoperative bleeding.
◆ Adequate intravenous fl uid should be administered with monitoring of urine output via
urimeter on the Foley bag.
◆ The diet may be limited to ice chips and sips of water in the postanesthesia care unit and
on postoperative day 1. Return of bowel function is measured by the frequency and pitch of
bowel sounds, lack of abdominal distention, and the patient’s subjective will to eat. A clear
liquid diet may be offered as sips of clear liquids without carbonation and without a straw
to minimize accumulation of air in the intestine. This may be advanced ad lib as bowel
function returns.
◆ Early ambulation is crucial for return of bowel function. Patients should be instructed to
walk multiple times a day beginning on postoperative day 1, and should be encouraged to
do so frequently.
◆ The umbilical bolster should be removed before the patient leaves the hospital. Skin staples
are removed on postoperative day 10.
STEP 5: PEARLS AND PITFALLS
◆ Placement of deep ratcheted Richardson retractors may impinge on the femoral nerve
against the psoas muscle, causing compression and femoral nerve neuropathy. The short
ratcheted retractors should be used to avoid this, even in patients with thick body walls.
◆ The use of ertapenem 1 g IV for prophylaxis of surgical site infections after colon surgery
has the advantage of once-a-day dosing so that therapeutic levels persist throughout the sur-
gery without need for additional doses during long cases. Ertapenem is a broad-spectrum

CHAPTER 62 • Total Colectomy 713
antibiotic covering enteric fl ora and has been approved by the SCIP as an acceptable prophy-
lactic antibiotic for elective colorectal surgery.
◆ Visualizing the left ureter before dividing the inferior mesenteric artery will decrease the
probability of inadvertent ureteral ligation. This step should be done every time after
clamps are placed across the pedicle, before the artery is cut.
◆ In patients who may need future completion proctectomy, such as those with ulcerative
colitis, care should be taken not to enter the avascular mesorectal plane after division of the
mesosigmoid. This preserves the integrity of the tissue plane and improves the relative ease
of future dissection.
◆ Every measure should be taken to preserve the ileal blood supply in patients with ulcerative
colitis for potential future ileal pouch creation.
◆ Care should be taken not to twist the small bowel mesentery when bringing out an ileos-
tomy or creating an ileorectal anastomosis. This can be done by identifying the superior
mesenteric artery at the root and “shaking hands” with the mesentery to feel for twists.
◆ The use of Seprafi lm underneath the incision minimizes abdominal adhesions and improves
ease of entry on subsequent laparotomies. In addition, wrapping a temporary ileostomy
with Seprafi lm allows for easier takedown later.
SELECTED REFERENCES
1 Beck DE, Opelka FG: Perioperative steroid use in colorectal patients. Dis Colon Rectum 1996;39:
995-999.
2. Itani KMF, Wilson SE, Awad SS, et al: Ertapenem versus cefotetan prophylaxis in elective colorectal sur-
gery. N Engl J Med 2006;355:2640-2651.
3. Zeng Q, Yu Z, You J, Zhang Q: Effi cacy and safety of Seprafi lm for preventing postoperative abdominal
adhesion: Systematic review and meta-analysis. World J Surg 2007;31:2125-2131; 2132 [discussion].
4. Law WL, Bailey HR, Max E, et al: Single-layer continuous colon and rectal anastomosis using monofi la-
ment absorbable suture (Maxon): Study of 500 cases. Dis Colon Rectum 1999;42:736-740.
5. Max E, Sweeney WB, Bailey HR, et al: Results of 1,000 single-layer continuous polypropylene intestinal
anastomoses. Am J Surg 1991;162:461-467.
714
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the anatomy of the abdomen is critical before undertak-
ing proctocolectomy.
◆ The relationship of the colon to intraperitoneal and retroperitoneal attachments and struc-
tures should be fully understood.
◆ The anatomy of the rectum and surrounding pelvic structures should also be appreciated.
This includes understanding of the fascial relationship of the rectum to the anterior and
posterior avascular planes of Denonvillier and Waldeyer; the sympathetic and parasympa-
thetic innervation of the superior and inferior hypogastric nerve plexus and nervi erigentes;
and arterial, venous, and lymphatic drainage of the rectum and anal canal.
◆ Particular attention should be paid to the location of the left ureter relative to the inferior
mesenteric vascular pedicle. This is the most commonly injured area after inferior mesen-
teric artery (IMA) vascular pedicle ligation.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for proctocolectomy involve both emergent and elective scenarios for treatment
of:
◆ Ulcerative colitis
◆ Crohn’s disease of the large bowel and rectum
◆ Familial adenomatosis coli
◆ Synchronous multiple cancers
◆ Bowel continuity may or may not be restored depending on the clinical circumstance.
CHAPTER
63
Ileoanal Anastomosis
(Straight and J Pouch)
Valerie P. Bauer

CHAPTER 63 • Ileoanal Anastomosis (Straight and J Pouch) 715
◆ Temporary loop ileostomy is used to protect the ileal pouch anal anastomosis (IPAA), and
should be strongly considered in this operation. The patient should be marked preopera-
tively and educated concerning both the new ostomy and pouch.
◆ Consideration for ureteral stenting should be made based on the extent of disease and prior
abdominal operations.
◆ Aspirin, other blood thinners, and vitamin E should be stopped for 10 days before the pro-
cedure.
◆ Preoperative laboratory and cardiac evaluations should be obtained based on the patient’s
comorbidities.
◆ Patients taking steroids preoperatively should receive a stress dose of hydrocortisone
100 mg intravenously (IV) before the operation. This should be continued postopera-
tively and tapered accordingly.
◆ Consideration toward placing an epidural catheter preoperatively should be made for post-
operative pain control and minimization of parenteral narcotic use and associated postoper-
ative ileus.
◆ Bowel preparation should include mechanical bowel preparation as per the surgeon’s prefer-
ence. Caution should be taken when using sodium phosphate preparation because of the
risk of acute phosphate nephropathy.
◆ Appropriate antibiotics should be given parenterally within 1 hour of the incision.

716 Section IX • Colon
1. POSITIONING
◆ Proper positioning of the patient should be directed by the primary surgeon to ensure con-
sistency and safety to the patient.
◆ The patient should be placed supine on the operating table. A thromboembolism-deterrent
(TED) hose and sequential compression devices should be placed on the legs, and a Foley
catheter should be inserted.
◆ The legs are placed in low lithotomy position using Allen stirrups (Figure 63-1). The boots
are adjusted so that each leg rests in a fl exed position without pressure on the popliteal
fossa. Padding is used to shield the skin from all hard objects.
◆ Abdominal and pubic hair is clipped off.
◆ A warmer is placed appropriately on the patient to ensure normothermia during the
procedure.
◆ An orogastric or nasogastric tube is placed after induction of anesthesia.
◆ A small roll is placed under the patient’s lower back.
◆ Rigid proctoscopy is performed to clean the rectum of residual stool and to confi rm absence
of pathologic abnormalities in the rectum that may need to be addressed in the operating
room.
◆ The premarked ileostomy site is scored using a needle to avoid losing the mark during the
skin preparation.
◆ The abdomen and perineum are prepped. The scrotum should be positioned away from the
perineum.
◆ Draping the patient:
◆ The patient is draped in standard fashion according to the surgeon’s preference.
◆ An under buttocks drape should be included, because there will be work from the peri-
neal side.