Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 80 • Umbilical Hernia (Child and Adult) 869
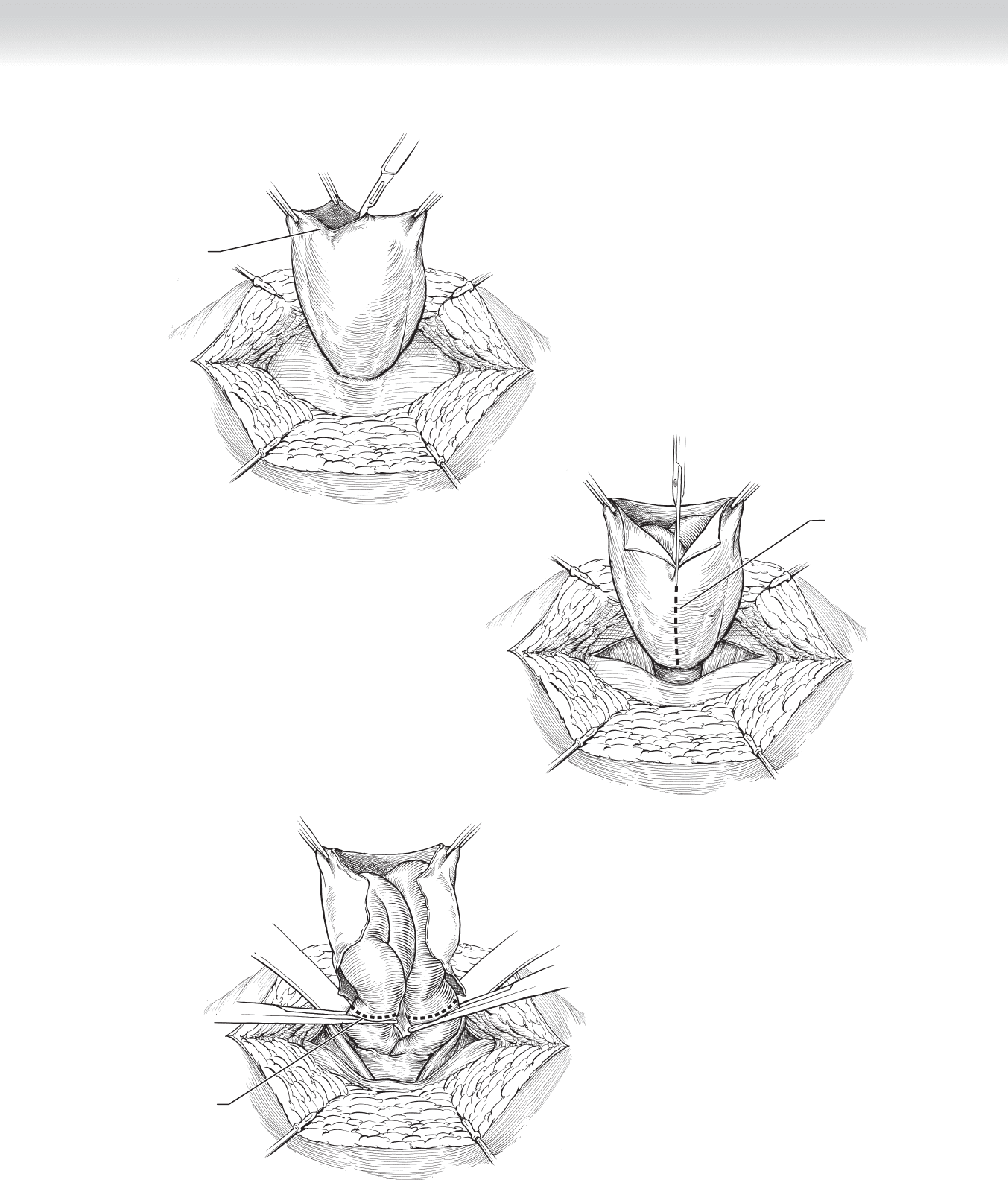
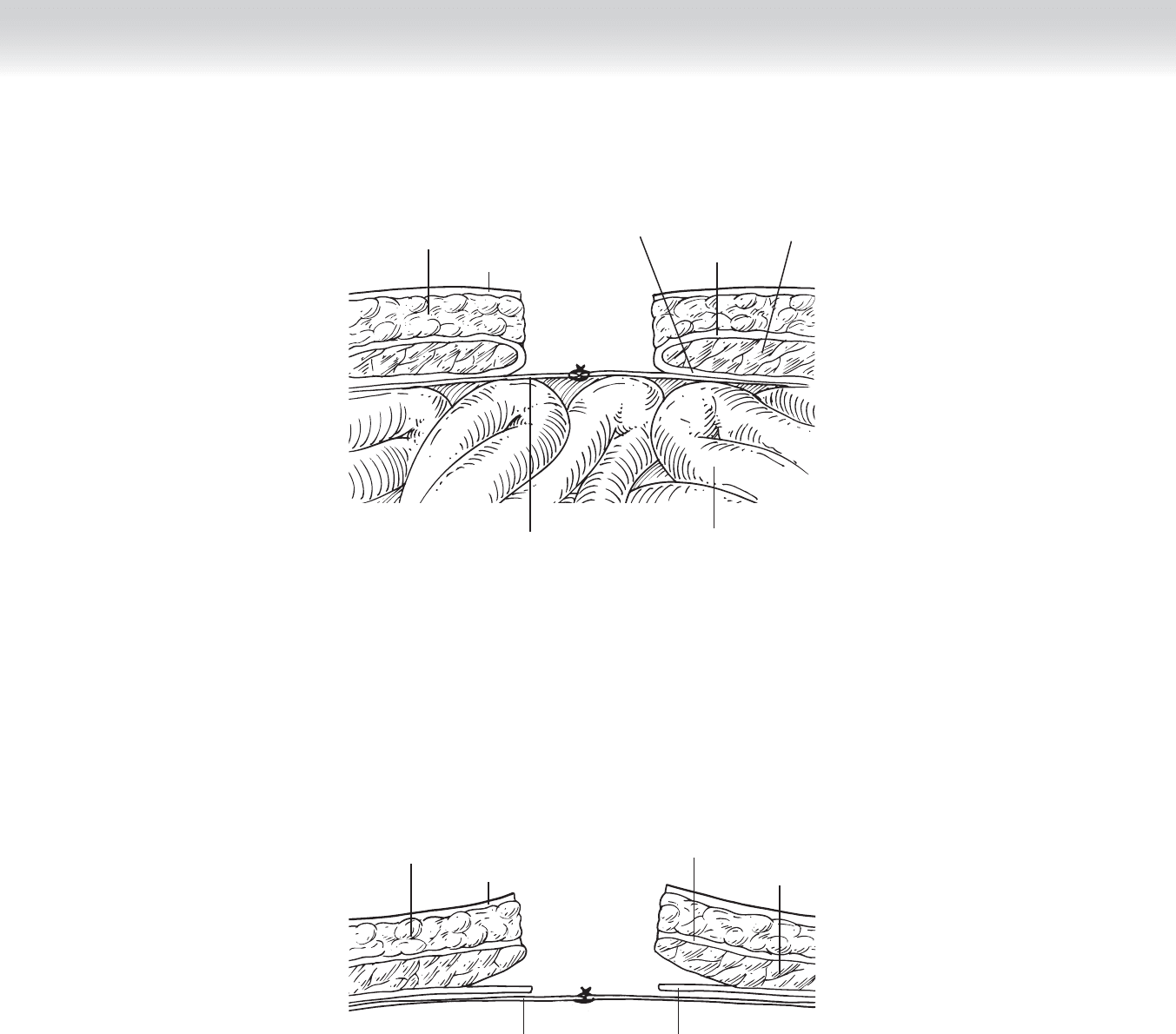
Opening hernia sac
FIGURE 80 –7
Midline incision
of hernia sac
FIGURE 80 –8
Excise hernia content
FIGURE 80 –9
870 Section XI • Hernias
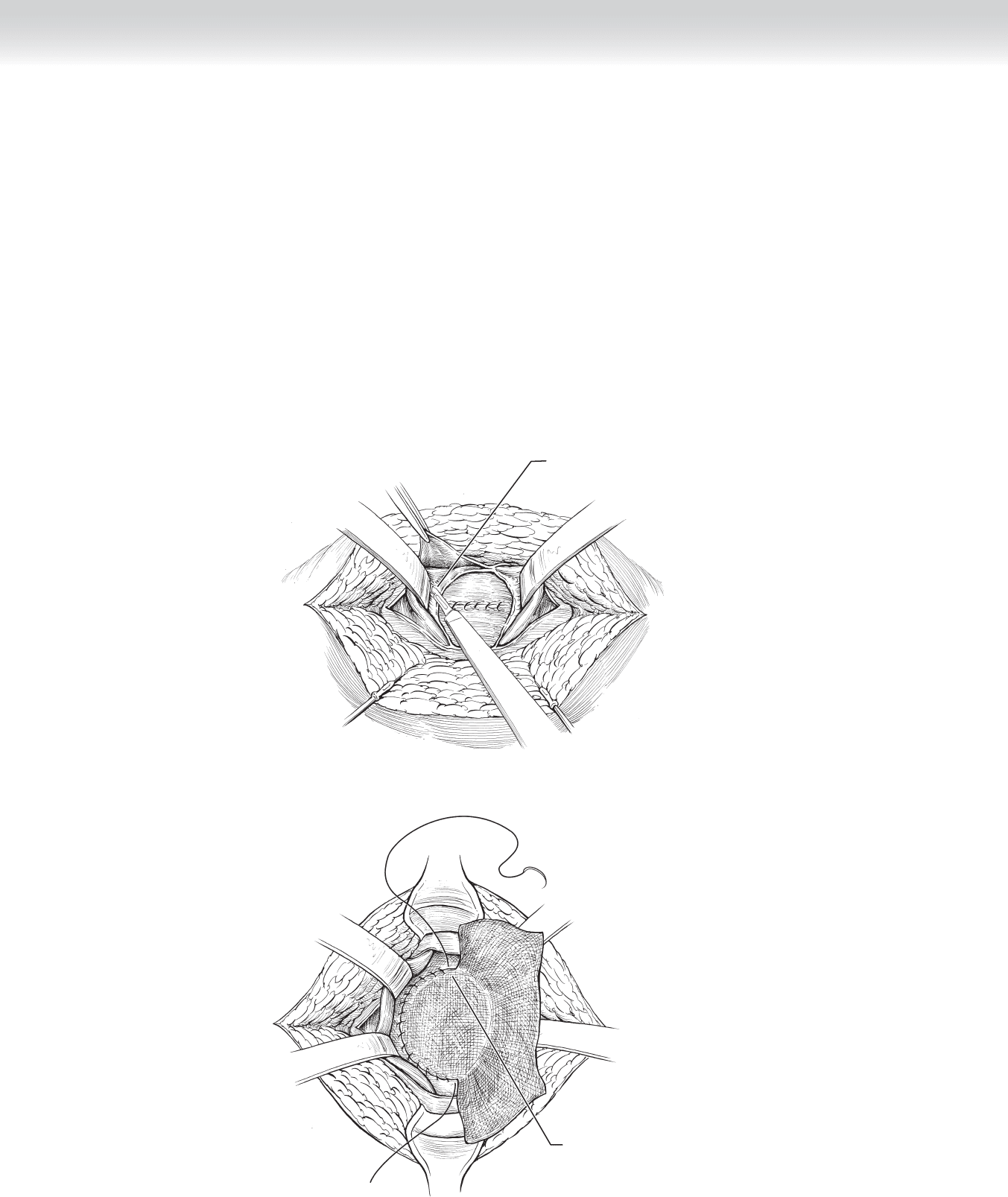
◆ After complete reduction of the hernia contents, the sac is closed and the plane between the
peritoneum and the posterior abdominal fascia is sharply dissected for a distance of 3 cm
circumferentially if mesh is to be used. If this plane is not accessible, the mesh may be
placed on the posterior rectus sheath, posterior to the rectus muscles (Figure 80-10).
◆ Consideration may be given to primary midline approximation of smaller fascial defects
using 2-0 interrupted nonabsorbable suture, especially if intestinal ischemia was encoun-
tered, but lower recurrence rates have been shown with mesh repairs.
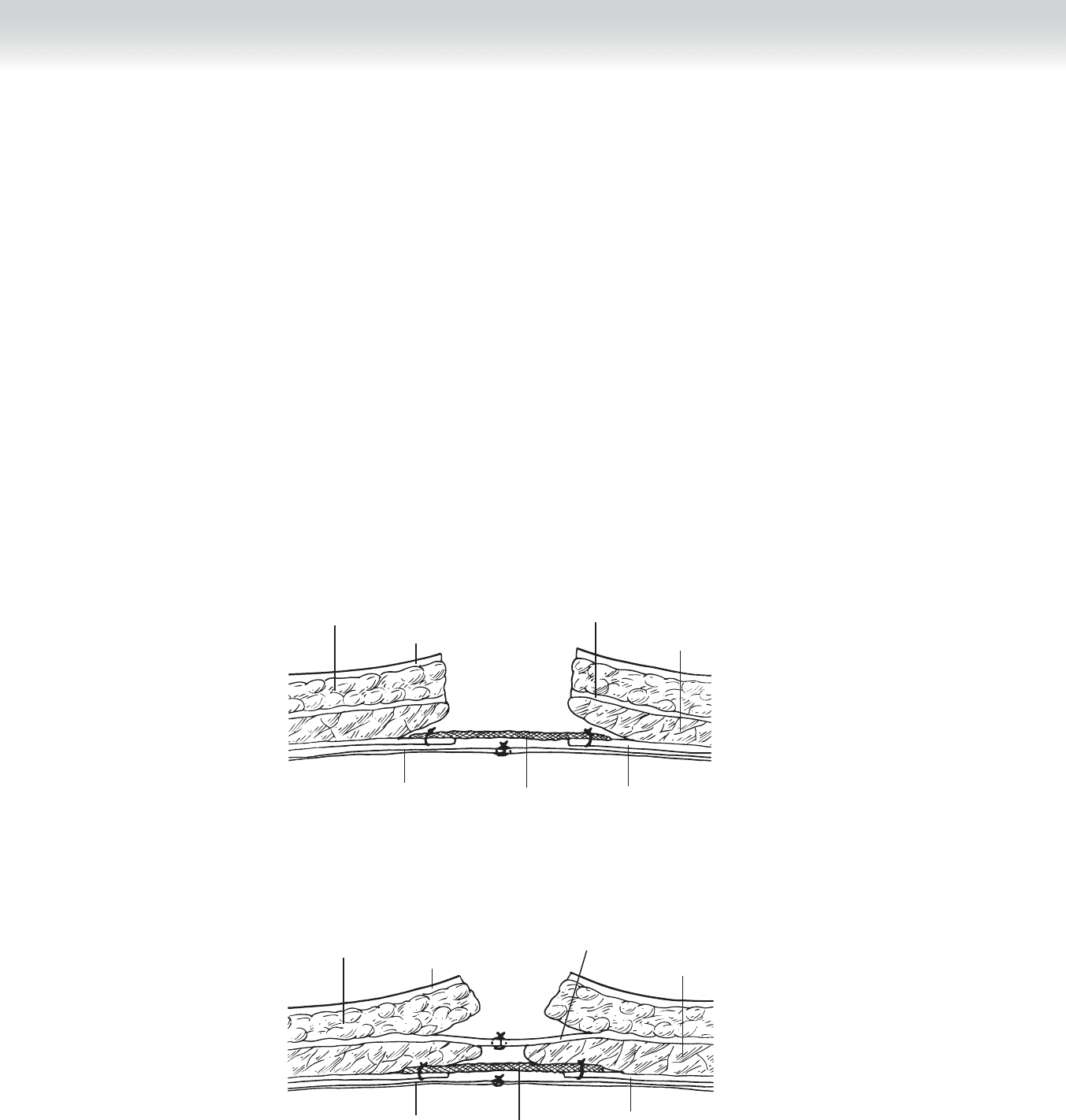
◆ Polypropylene mesh is placed in the preperitoneal space with 3 cm of overlap with the fas-
cia. The mesh is sutured circumferentially to the fascia without tension, and the edges of
the fascia are sutured to the center of the mesh (Figure 80-11).
Sharp dissection
FIGURE 80 –10
Securing
polypropylene mesh
FIGURE 80 –11
CHAPTER 80 • Umbilical Hernia (Child and Adult) 871
3. CLOSING
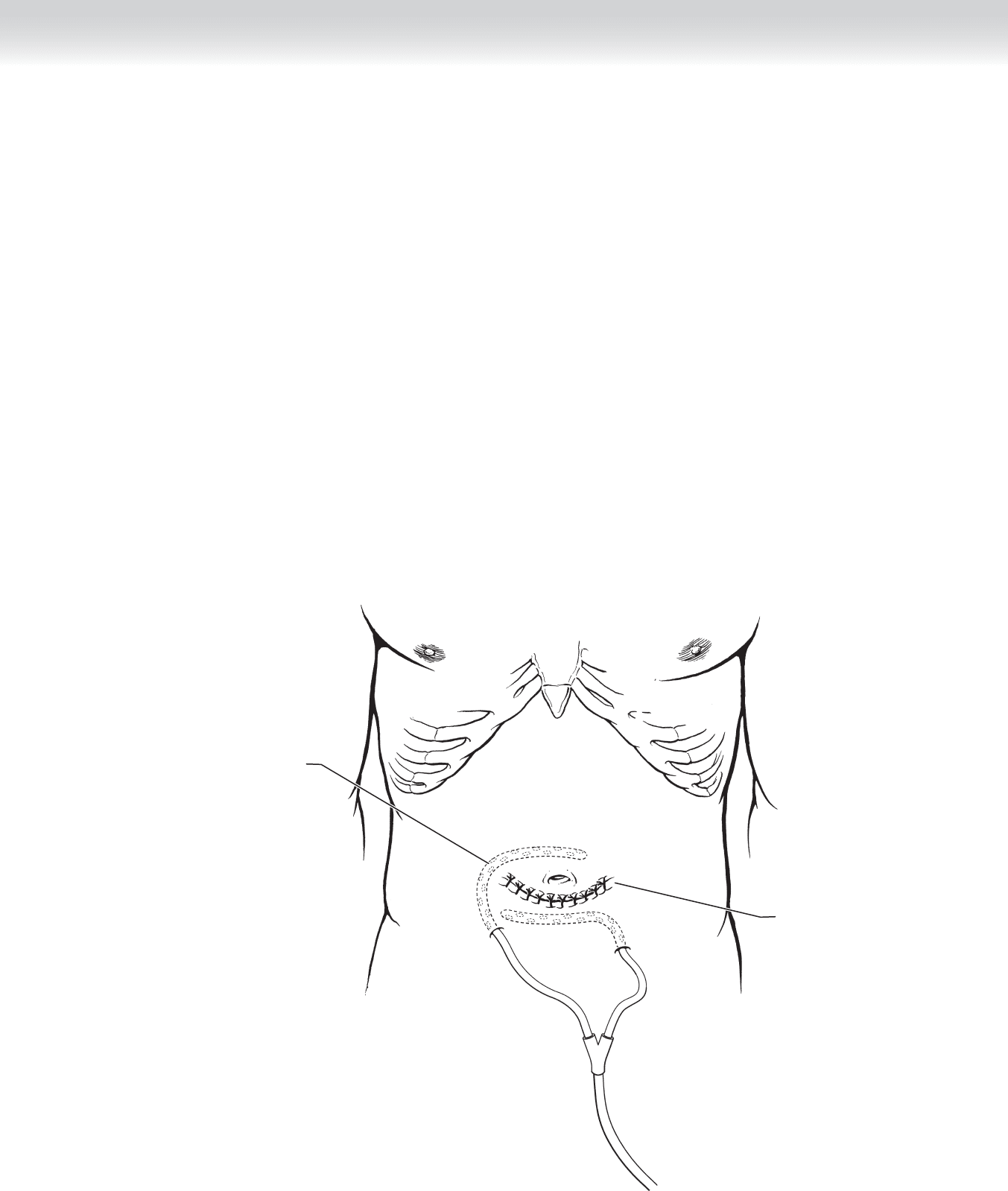
◆ A closed suction drain may be required to prevent postoperative seroma if the soft tissue
space is excessive. The drain should exit the skin remote from the surgical wound. A
two-layer closure using absorbable suture or skin staples completes the operation
(Figure 80-12).
◆ To help prevent a wound seroma, a ball of cotton or gauze should be placed in the umbilicus
and held in place with an abdominal binder.
Closed
skin incision
Subcutaneous
drain
FIGURE 80 –12

872 Section XI • Hernias
STEP 4: POSTOPERATIVE CONSIDERATIONS
◆ Drains usually may be safely removed once the output declines to less than 30 mL per day.
STEP 5: PEARLS AND PITFALLS
◆ In a contaminated fi eld (e.g., resection of gangrenous intestine), an absorbable or biologic
fascia substitute may be used with the expectation that a recurrence of the hernia is likely
but may be repaired later after the eradication of the contamination.
◆ Polypropylene mesh should not be placed within the peritoneal cavity. If there is insuffi -
cient peritoneum to close in the midline, an expanded polytetrafl uoroethylene mesh prod-
uct may be placed, because formation of adhesions to this surface or erosion into adjacent
viscera is unlikely.
SELECTED REFERENCES
1. Radhakrishnan J: Umbilical hernia. In Nyhus LM, Condon RE (eds): Hernia, 4th ed. Philadelphia,
JB Lippincott, 1995.
2. Skinner MA, Grosfeld JL: Inguinal and umbilical hernia repair in infants and children. Surg Clin North Am
1993;73:439-449.
873
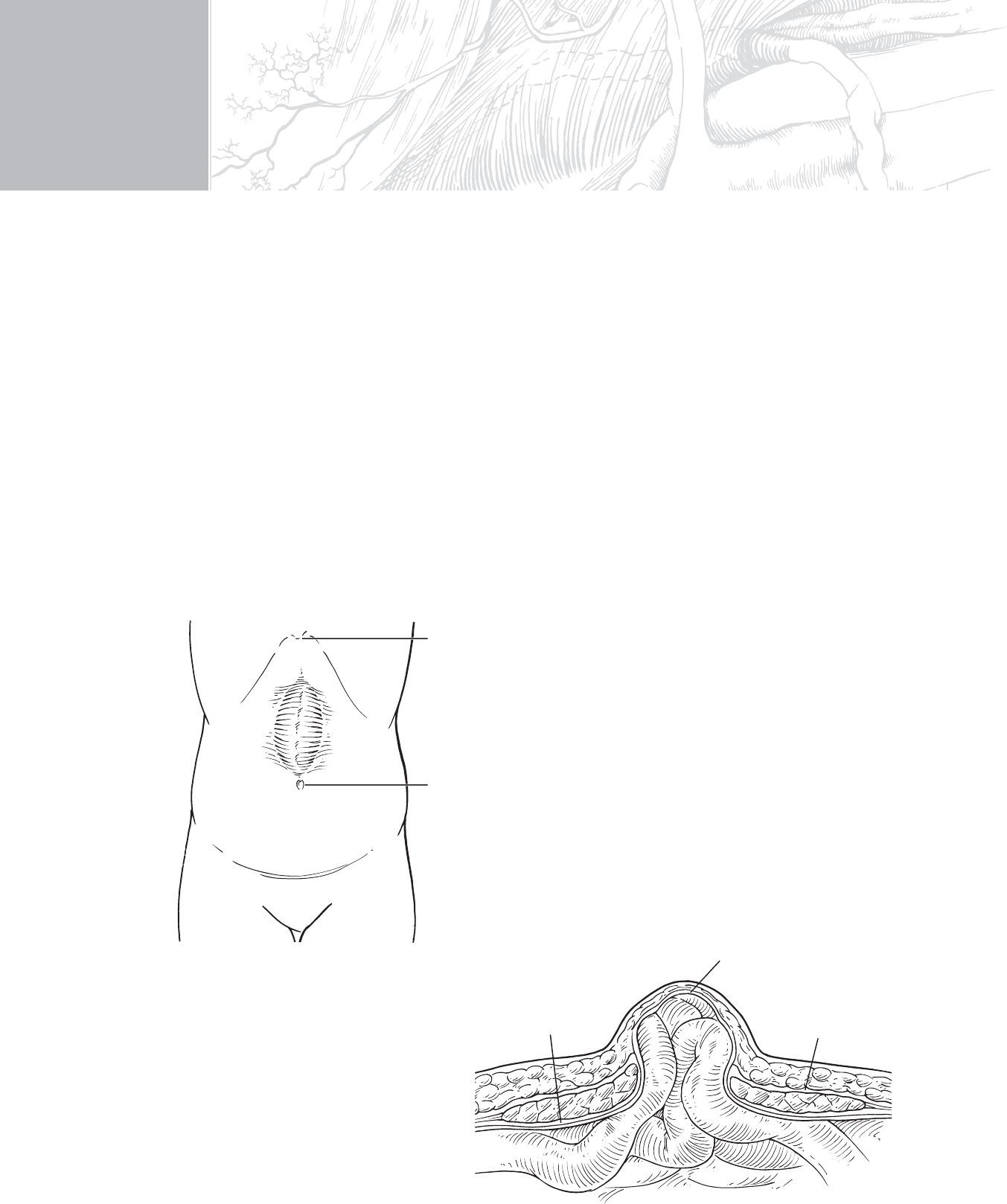
STEP 1: SURGICAL ANATOMY
◆ A midline epigastric incisional hernia is represented in Figure 81-1.
◆ Figure 81-2 is a cross-section of the hernia illustrating the relevant layers.
CHAPTER
81
Incisional/Ventral Hernia—
Mesh and Tissue Flap
Thomas D. Kimbrough
Xiphoid
Umbilicus
FIGURE 81 –1
Posterior
rectus sheath
Anterior
rectus sheath
Peritoneum
FIGURE 81 –2

874 Section XI • Hernias
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The most important preoperative consideration is whether the hernia should be repaired.
Because the risk to the patient from the hernia decreases as its diameter increases, and the
chance of recurrence and other surgical complications increases, the risk-to-benefi t ratio
should be carefully assessed.
◆ In the event repair is deemed desirable, many of these patients have signifi cant comorbidi-
ties that must be addressed preoperatively and managed perioperatively. Neglect of these
can lead to failure in spite of a technically superb surgical repair.
◆ There are many techniques for repair of incisional hernias, illustrating among other things
that no one method has been judged superior. The technique illustrated here is but one of
many acceptable available.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ In the case of incisional hernias, the new incision is made by excising the old scar.
◆ In the case of a ventral hernia not related to a previous surgical procedure, the incision is
best placed along the longer axis of the fascial defect.
◆ If the fascial defect is circular with no signifi cant difference in the length of axes, transverse
incisions leave better scars.
2. DISSECTION
◆ After the hernia sac is identifi ed, its external peritoneal lining is dissected free from sur-
rounding structures, including the innermost fascial layer of the abdominal wall.
◆ Although it is often necessary to open the peritoneum and even resect portions of it, preser-
vation of enough of the peritoneum to close allows the imposition of a tissue layer between
the mesh to be used and the contents of the intra-abdominal cavity. The end result is illus-
trated in Figure 81-3.
◆ Figure 81-4 shows the next step, which is separation of the posterior rectus sheath from
the overlying rectus abdominis muscle.
◆ Primarily the cut edges of the posterior sheath are then closed, even if under tension. This
closure can be facilitated by application of the techniques of component separation.
CHAPTER 81 • Incisional/Ventral Hernia—Mesh and Tissue Flap 875
FIGURE 81 –3
Posterior
rectus sheath
Anterior
rectus sheath
Peritoneum
Rectus
muscles
Skin
Bowel
Subcutaneous fat
FIGURE 81 –4
Posterior
rectus sheath
Anterior
rectus sheath
Peritoneum
Rectus
muscles
Skin
Subcutaneous fat
876 Section XI • Hernias
◆ A sheet of polypropylene mesh is then positioned on top of the posterior sheath and under
the rectus muscle. There should be an overlap of 3 to 5 cm on all sides. Some choose to
tack the mesh in place with mattress sutures through the rectus muscle and anterior sheath.
I have found it suffi cient to tack the mesh to the underlying posterior sheath with absorb-
able sutures. Either way the mesh should be tacked down as tautly as possible. The com-
pletion of these steps is illustrated in Figure 81-5.
◆ Figure 81-6 shows the completed repair after primary closure of the anterior sheath. Again,
fascial release techniques such as component separation can facilitate this process.
◆ It is, of course, not always possible to completely close the posterior and anterior fascial
layers, even with releases. In that event, as much as possible is closed, even if under ten-
sion. Every effort is made to close some type of tissue layer between the abdominal contents
and the mesh, and the mesh and the skin. As mentioned earlier, the peritoneum can be
used in the fi rst instance, and the subcutaneous tissues in the latter.
FIGURE 81 –5
Posterior
rectus sheath
Anterior
rectus sheath
Peritoneum
Rectus
muscles
Skin
Subcutaneous fat
Mesh
FIGURE 81 –6
Posterior
rectus sheath
Anterior
rectus sheath
Peritoneum
Rectus
muscles
Skin
Subcutaneous fat
Mesh

CHAPTER 81 • Incisional/Ventral Hernia—Mesh and Tissue Flap 877
3. CLOSING
◆ Scrupulous attention should be paid to hemostasis, because postoperative hematomas are
not uncommon and can create signifi cant problems.
◆ Whether to use drains in any or all of the spaces created by the dissection is the choice of
the individual surgeon. The drains are no substitute for good technique and offer a route
for the introduction of bacteria.
STEP 4: POSTOPERATIVE CARE
◆ Most patients require a day or two in the hospital for adequate pain control.
◆ Patients are instructed to refrain from lifting or doing strenuous work for 4 to 6 weeks.
SELECTED REFERENCE
1. Zinner MJ, Schwartz SI, Ellis H: Hernias. In Maingot R, Zinner M (eds): Maingot’s Abdominal Operations,
vol 1, 10th ed. Stamford, Conn, Appleton & Lang, 1997, pp 479-580.

880
ELECTIVE ANEURYSM REPAIR
◆ Most patients with asymptomatic abdominal aortic aneurysms are operated on electively
once the aneurysm exceeds 5.5 cm in diameter. If the aneurysm has ruptured, immediate
operative repair is indicated. Some steps appropriate to emergency aneurysmectomy will be
included in the discussion of elective aneurysm repair.
STEP 1: SURGICAL ANATOMY
◆ The aorta enters the abdomen between the crura of the diaphragm at the level of the 12th
thoracic vertebra and bifurcates into the right and left common iliac arteries at the inter-
space between the fourth and fi fth lumbar vertebrae. The aorta is crossed successively by
the fourth portion of the duodenum, the left renal vein, and the root of the mesentery, and
it is intimately related to the vena cava and iliac veins. The left common iliac vein runs
posterior medial to the artery and is densely adherent to it (Figure 82-1).
◆ In most patients with abdominal aortic aneurysm, dilation begins distal to the origins of
renal arteries and extends to the aortic bifurcation and iliac arteries. The elongation accom-
panying the aortic dilation results in tortuosity displacing the aorta off the vertebral column
anteriorly or off to one side of the midline. The tortuosity may also involve the iliac arteries,
resulting in their displacement into the pelvis.
◆ The inferior mesenteric vein is located in the mesentery anterior to the aneurysm. Care must
be taken when ligating the inferior mesenteric vein to ensure that only the vein is ligated,
because the collateral arterial supply to the colon often accompanies the vein in this location.
CHAPTER
82
Resection of Abdominal
Aortic Aneurysm
Glenn C. Hunter