Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 891
INFLAMMATORY ANEURYSM
◆ In approximately 5% of patients with abdominal aortic aneurysms, a dense fi brotic reaction
involving the aortic wall and retroperitoneum is encountered. The infl ammatory reaction
may involve the duodenum, inferior vena cava, left renal vein, and ureters and is manifested
as a thick white plaque overlying the aorta. Infl ammatory aneurysm is an important cause of
abdominal pain in patients with abdominal aortic aneurysms that must be distinguished
from ruptured aneurysms on CT scans or MRI. These aneurysms are best repaired via the
retro peritoneal approach mobilizing the aorta above the renal vein, taking care not to dissect
the duodenum off the aneurysm wall. Venous anomalies such as left-sided or double inferior
vena cava should be identifi ed and preserved.
◆ No attempt should be made to dissect the aorta or iliac arteries circumferentially to mini-
mize the risk of venous bleeding.
◆ Elective ligation and division of the left lumbar vein allows cephalad retraction of the renal
vein, reduces the risk of bleeding, and improves exposure.
◆ Large lymphatic vessels and the cisterna chyli are often present at the level of the renal vein
and should be suture ligated to prevent the rare occurrence of chylous ascites.
◆ Dissection of the left common iliac artery bifurcation should be undertaken by dividing the
lateral peritoneal attachments of the descending colon, thus avoiding injury to the hypogas-
tric nerves bilaterally. Routing the left limb of the graft through the lumen of the common
iliac artery also minimizes the risk of this complication.
◆ If the renal vein is not present in its usual anterior location, a retroaortic renal vein should
be suspected and care taken in placing the proximal clamp.
◆ Rectal bleeding in the early postoperative period should prompt careful sigmoidoscopy and
prompt return to the operating room if signifi cant ischemia is present or acidosis persists.
SELECTED REFERENCES
1. Standring S (ed): Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 39th ed. Philadelphia,
Churchill Livingstone, 2005.
2. Lederle FA, Johnson GR, Wilson SE, et al: Prevalence and associations of abdominal aortic aneurysm de-
tected through screening. Ann Intern Med 1997;126:441-449.
3. Sicard GA, Reilly JM, Rubin BG, et al: Transabdominal versus retroperitoneal incision for abdominal aortic
surgery: report of a prospective randomized trial. J Vasc Surg 1995;21:174-181.

892
STEP 1: SURGICAL ANATOMY
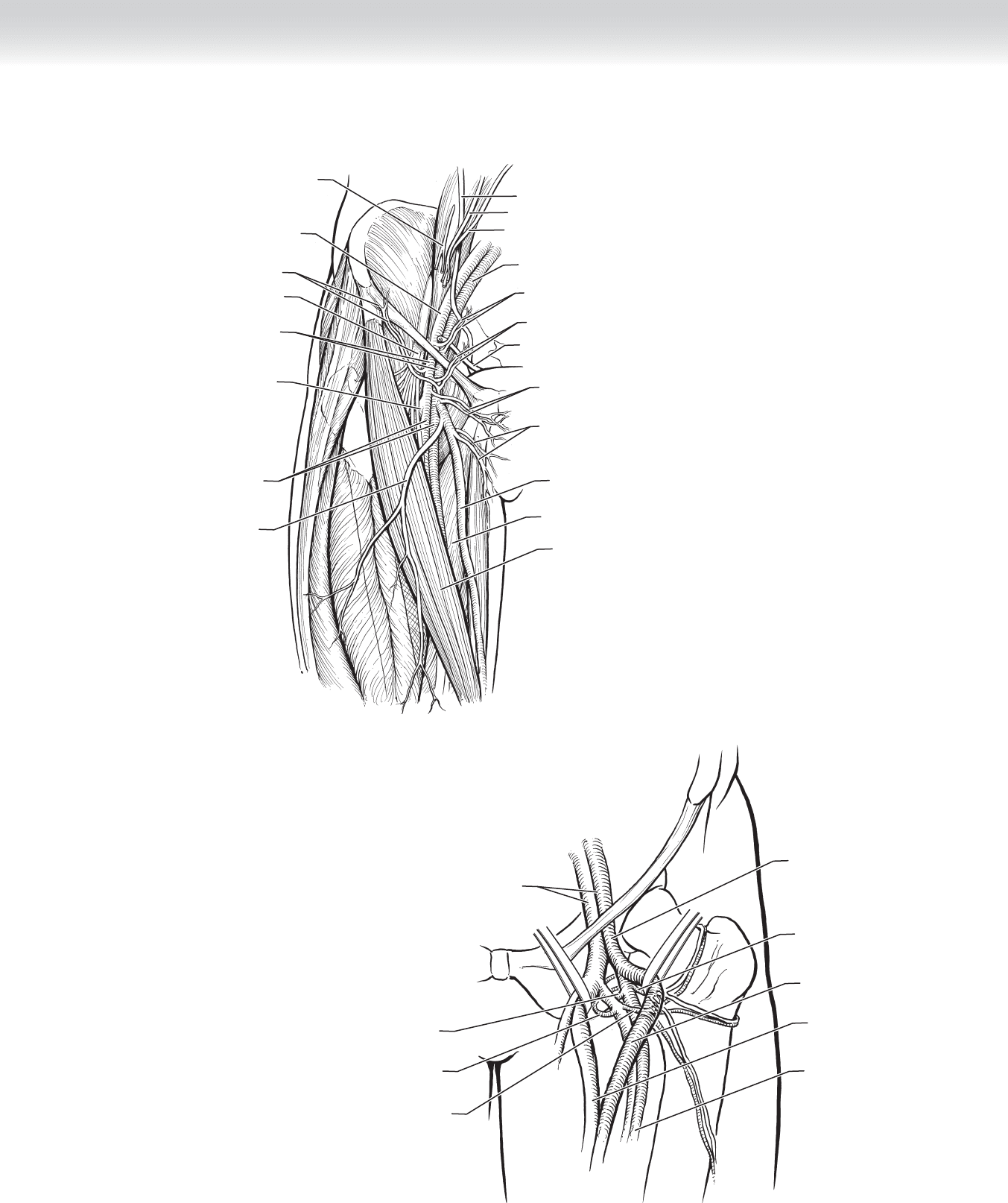
SURGICAL ANATOMY OF THE FEMORAL REGION
◆ The inguinal ligament defi nes the transition from the external iliac to the common femoral
artery. The common femoral artery and vein are encased in the femoral sheath in the proxi-
mal thigh bounded by the femoral triangle (Figure 83-1). The lateral boundary of this trian-
gle is formed by the sartorius muscle, the medial boundary by the adductor longus muscle,
and the cephalad base by the inguinal ligament.
◆ Just proximal to the inguinal ligament, the external iliac artery has two branches: the infe-
rior epigastric and the deep circumfl ex iliac arteries. Just distal to the inguinal ligament, the
common femoral artery has three branches: the superfi cial epigastric, the superfi cial cir-
cumfl ex iliac, and the superfi cial external pudendal arteries.
◆ The common femoral artery divides into the superfi cial and the deep femoral arteries as it
crosses the pectineus muscle. The superfi cial femoral artery traverses the thigh between the
quadriceps and adductor muscles in the adductor, or Hunter’s, canal. The origin of the deep
femoral artery is 3 to 5 cm distal to the inguinal ligament. This artery is crossed by the lat-
eral femoral circumfl ex vein (see Figure 83-1).
Aortofemoral Bypass Graft
for Occlusive Disease
Charlie C. Cheng and Michael B. Silva, Jr.
CHAPTER
83
CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 893
FIGURE 83 –1
Deep external
pudendal artery and vein
Superficial external
pudendal artery and vein
Great saphenous vein
Adductor longus muscle
Sartorius muscle
Superficial epigastric artery and vein
Ductus deferens
Inferior epigastric artery and vein
External iliac vein
Ureter
Testicular artery
Testicular vein
Superficial
circumflex iliac artery and vein
Genitofemoral nerve
External iliac artery
Deep femoral artery
Common femoral
artery and vein
Femoral nerve
Superficial
femoral artery and vein
Anterior lateral accessory
saphenous vein
MC
A
Deep femoral
artery
Superficial
femoral artery
Superficial
femoral vein
Lateral circumflex
femoral artery
Common
femoral artery
External
iliac artery and vein
Medial circumflex
femoral artery
Medial circumflex
femoral vein
Lateral circumflex
femoral vein
B

894 Section XII • V
ASCULAR
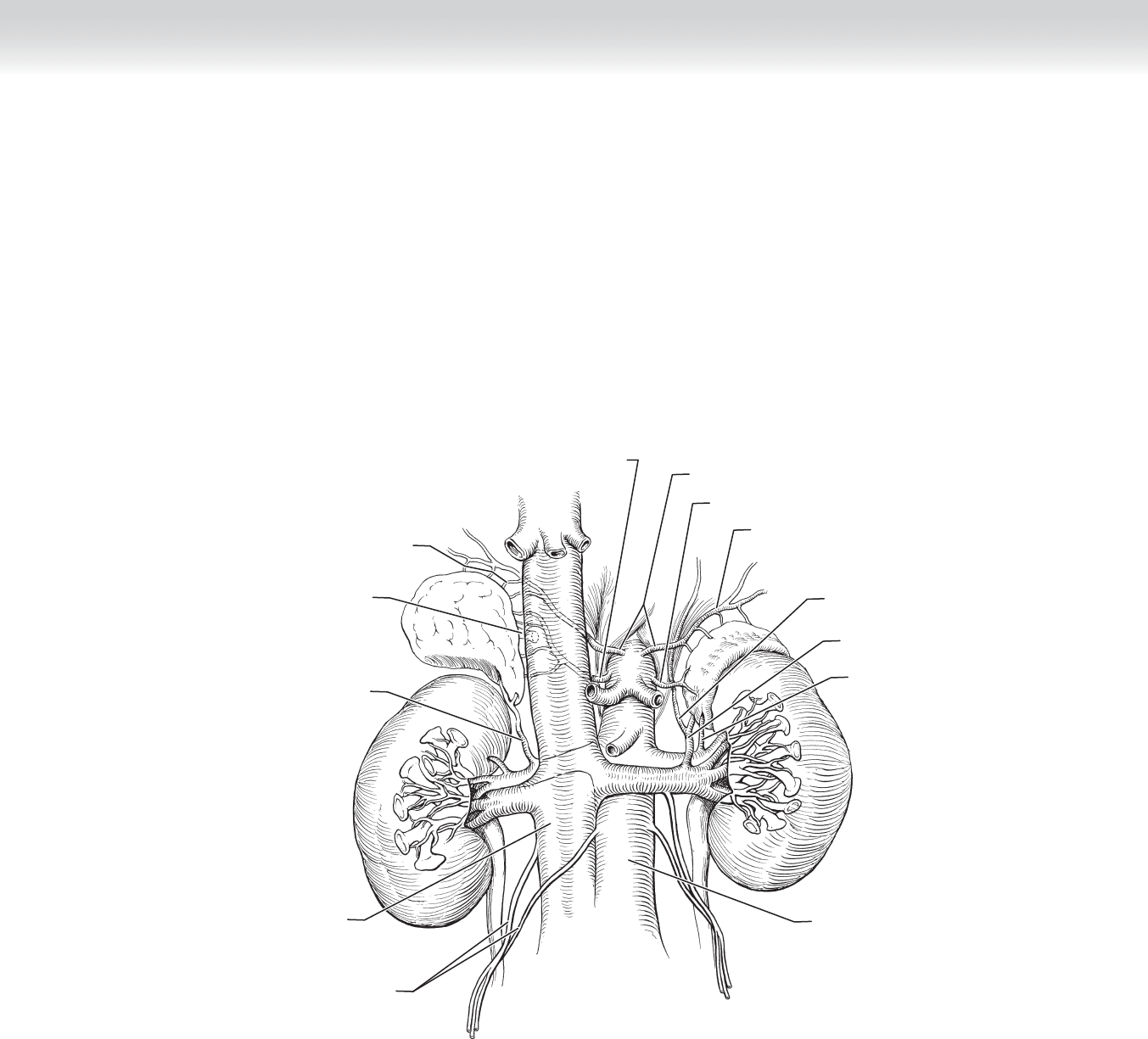
SURGICAL ANATOMY OF THE ABDOMINAL AORTA
◆ The abdominal aorta has three large, unpaired midline branches that supply most organs:
the celiac, superior mesenteric, and inferior mesenteric arteries (Figure 83-2). The celiac
and superior mesenteric arteries arise at the level of the fi rst lumbar vertebra. The
inferior mesenteric artery arises at the third lumbar vertebra.
◆ The renal arteries arise at the level of the disc between the fi rst two lumbar vertebrae from
the lateral walls of the aorta (see Figure 83-2). The left-sided artery is usually slightly more
cephalad than the right. The renal arteries lie posterior to the corresponding veins on each
side. The left renal vein usually passes anterior to the aorta, whereas the right renal artery
passes behind the inferior vena cava. A retroaortic left renal vein is a relatively common
venous variant with an incidence of approximately 3%.
◆ The left renal vein serves as a landmark for cephalad dissection of the abdominal aorta.
Beneath this vein, the origins of the right and left renal arteries can be located.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for aortobifemoral bypass are symptomatic atherosclerotic occlusive disease of
the infrarenal aorta and both iliac systems, and peripheral atheromatous embolization (blue
toe syndrome). Symptoms of occlusive disease include claudication, rest pain, and tissue
loss. The presence of rest pain or tissue loss usually results from multilevel occlusive disease
involving both the aortoiliac segment and the infrainguinal segment. Seventy-fi ve percent to
80% of these patients can initially be managed with treatment of the infl ow aortoiliac dis-
ease without treatment of the distal infrainguinal disease. This is usually adequate for
patients with claudication or rest pain. However, in patients with tissue loss, the distal dis-
ease should also be treated to provide pulsatile fl ow to the foot. Embolization from athero-
sclerotic plaques in the aortoiliac system requires exclusion of the native aortoiliac arteries,
even if the plaque lesions are not associated with hemodynamically signifi cant stenoses.
◆ Up to 50% of patients with aortoiliac disease may have clinically evident coronary artery
disease. The 30-day operative mortality for this bypass has decreased from 5% to 8% in the
early 1970s to 2% in the past decade as a result of improved preoperative management of
coronary artery disease. Patients should routinely be evaluated preoperatively for the pres-
ence of coronary artery disease and pulmonary, renal, and coagulation disorders.
◆ Preoperative imaging is needed in the evaluation of the entire abdominal aorta, the bilateral
iliac arteries, and down to the origins of the deep femoral arteries. Arteriography has histor-
ically been the main imaging modality. Other contemporary alternatives include magnetic
resonance imaging and computed tomography angiography. Complete bilateral lower
extremity arteriography is also recommended.
CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 895
FIGURE 83 –2
Right middle
adrenal artery
Right
adrenal vein
Left middle adrenal artery
Right and left inferior phrenic arteries
Left superior
adrenal artery
Right inferior
adrenal artery
Inferior
vena cava
Testicular, ovarian
artery and vein
Right superior
adrenal artery
Left adrenal
vein
Left inferior
adrenal artery
Aorta
Left inferior
phrenic vein
MC

896 Section XII • V
ASCULAR
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The patient is placed supine, and the abdomen, groin, and thighs are prepared and draped.
A narrow perineal towel is used, ensuring that it does not extend laterally to the groins. The
perineum should remain excluded from the surgical fi eld throughout the procedure. A
povidone-iodine (Betadine)–impregnated self-adherent drape can be used to cover the
abdomen, perineal towel, and groin areas to prevent the towel from becoming loose on the
medial side of the femoral incisions.
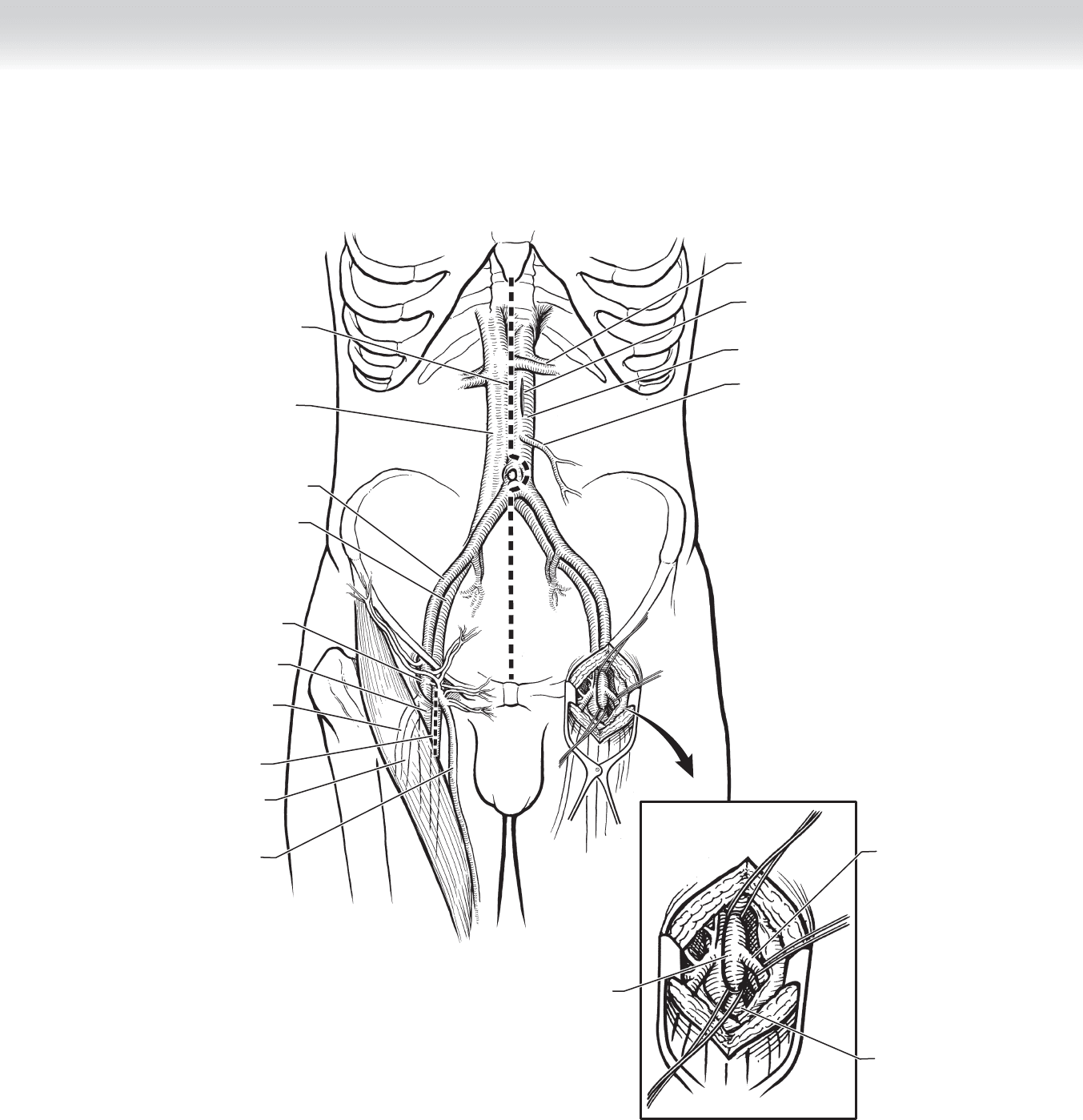
◆ The groins are opened through vertical incisions directly over the femoral pulse, crossing
the inguinal crease to expose the femoral arteries (Figure 83-3). The incision is made with
one third of the incision above the inguinal ligament, and two thirds below it. If femoral
pulse is not palpable, the vertical incision is made slightly medial to the midpoint of the
inguinal ligament.
◆ The abdomen is opened through a full midline incision from the xiphoid process to the
symphysis pubis. The peritoneal cavity is entered through the linea alba, and the abdominal
aorta is exposed (see Figure 83-3). Alternatively, a retroperitoneal incision may be used.
This may be the approach of choice in patients with a hostile abdomen from previous
abdominal or aortic surgeries and poor pulmonary function. This incision is started from
the lateral border of the rectus muscle, 2 cm below the level of the umbilicus, and is
extended laterally to the tip of the 12th rib.
2. DISSECTION
◆ Femoral artery exposure
◆ The groin incisions are deepened and extended proximally to the inguinal ligament. The
fascia lata is opened along the medial margin of the sartorius muscle to expose the femo-
ral sheath underneath. This sheath is opened to access the common femoral artery, and
the artery is easily dissected free by separating the areolar tissue.
◆ The common femoral artery branches into the superfi cial and deep (profunda) femoral
arteries. The superfi cial femoral artery is exposed by dissecting distally from the common
femoral artery on its anterior surface. The deep femoral artery often originates 3 to 5 cm
distal to the inguinal ligament on the posterior lateral surface of the common femoral
artery. The lateral femoral circumfl ex vein crosses anteriorly to the deep femoral artery,
and caution should be used during dissection of this artery to avoid venous injury (see
Figure 83-1).
◆ The femoral arteries are examined for atherosclerotic occlusive disease and their suitabil-
ity for distal anastomosis. The common, superfi cial, and deep femoral arteries are each
encircled with tapes or vessel loops for control.
◆ Abdominal aorta exposure
◆ Following the exploration of the abdomen for any incidental pathology, the transverse
colon and the omentum are retracted upward toward the chest and protected from
retraction injury. The small bowel is gathered and retracted to the patient’s right side and
wrapped in a moist laparotomy towel.
CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 897
FIGURE 83 –3
Line of incision
Inferior vena cava
Site of anastomosis
of graft
Abdominal aorta
Inferior mesenteric artery
Left renal vessels
Line of
incision
External iliac artery
External iliac vein
Common
femoral artery
Common
femoral artery
Superficial
femoral artery
Deep
femoral artery
Deep
femoral vein
Deep femoral
artery
Superficial
femoral artery
Great
saphenous
vein
MC

898 Section XII • V
ASCULAR
◆ The peritoneum is opened over the upper part of the aorta, and the ligament of Treitz is
divided to mobilize the fourth portion of the duodenum and the fi rst part of the jeju-
num. The patency of the celiac axis and the superior and inferior mesenteric arteries are
confi rmed by palpation.
◆ The aorta is exposed proximally to the left renal vein and distally to the inferior mesen-
teric artery using both sharp dissection and electrocautery of the small veins in the retro-
peritoneal tissue (Figure 83-4).
◆ The aorta is dissected free using blunt fi nger dissection or a curved instrument just below
the left renal vein. The left renal vein is usually anterior to the aorta but can occasionally
be retroaortic. Failure to accurately identify the left renal vein may result in iatrogenic
injury during aortic cross-clamping.
◆ Aortofemoral bypass tunnel
◆ The tunnel is used to connect the exposed aorta from the abdomen and the femoral
arteries in the groins. It follows the course of the iliac and femoral arteries, lying anterior
to the arteries and posterior to the ureter. This prevents compression of the ureter by the
graft. The graft is protected in the retroperitoneal tissues.
◆ Tunneling is started from the groin incision, with blunt fi nger dissection along the ante-
rior surface of the common femoral artery. The inferior epigastric and deep circumfl ex
iliac veins course anterior to the external iliac artery, and caution is used. These veins are
routinely divided and ligated under direct vision to preclude inadvertent avulsion.
◆ In the abdomen, tunneling is started on the anterior surface of the aortic bifurcation and
continued onto the common iliac artery. The fi nger is passed blindly to meet with the
fi nger advancing from the groin incision (Figure 83-5). The tunnel tract is maintained
with passage of umbilical tape. The patient is systemically treated with anticoagulants,
usually with unfractionated heparin, after the tunnel has been dissected and inspected
for hemostasis.

CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 899
FIGURE 83 –4
Proximal jejunum
Abdominal aorta
Abdominal bifurcation
Bilateral groin incision
Inferior vena cava
Colon
MC
FIGURE 83 –5
Creating tunnel through
groin incision

900 Section XII • V
ASCULAR
◆ Aortic anastomosis
◆ The diameter of the aorta just below the left renal vein is assessed, and the size of the
bifurcated prosthetic graft is chosen. The typical location of the proximal anastomosis is
approximately 1 to 2 inches below the renal arteries. The aorta can be partially clamped
or cross-clamped below the renal arteries.
◆ The aortic limb of the aortic bifurcation graft is trimmed so that after the aortic anasto-
mosis, the two limbs lie in a natural position through the tunnels in the pelvis and exit
into the groin anterior to the femoral arteries. If the common trunk is too long, there is a
risk of kinking of the two limbs, compromising fl ow.
◆ The proximal aortic anastomosis can be performed in an end-to-end or end-to-side fashion.
The end-to-end technique is used for patients who will not suffer circulatory compromise
from interruption of prograde fl ow in the abdominal aorta. The end-to-side technique is
used for patients who require prograde fl ow to perfuse an important hypogastric or inferior
mesenteric artery.
◆ For an end-to-side anastomosis, an arteriotomy is made on the aorta just below the renal
vein, and the anastomosis is sutured with a running technique using a 3-0 nonabsorbable
monofi lament suture (Figure 83-6). The suture can be tightened with a nerve hook.
◆ For an end-to-end anastomosis, the aorta is divided sharply and the distal segment is
oversewn with a heavy suture (3-0 nonabsorbable monofi lament) using mattress stitches,
followed by a second row using a running stitch over the cut edge. The graft is then
anastomosed to the proximal aortic segment (Figure 83-7).