Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 881
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ A search for thoracic and iliac aneurysms and other associated anomalies, such as suprare-
nal extension, venous anomalies, horseshoe kidney, or aortocaval fi stula, with computed
tomography (CT) scanning, magnetic resonance imaging (MRI), or duplex ultrasound imag-
ing should be made before repair of an abdominal aortic aneurysm. Assessment of cardiac,
respiratory, and renal function should be undertaken and any abnormalities optimized
before proceeding with aneurysm repair. A mechanical bowel preparation the night before
surgery facilitates the operation. Prophylactic antibiotics are administered 1 hour before the
incision.
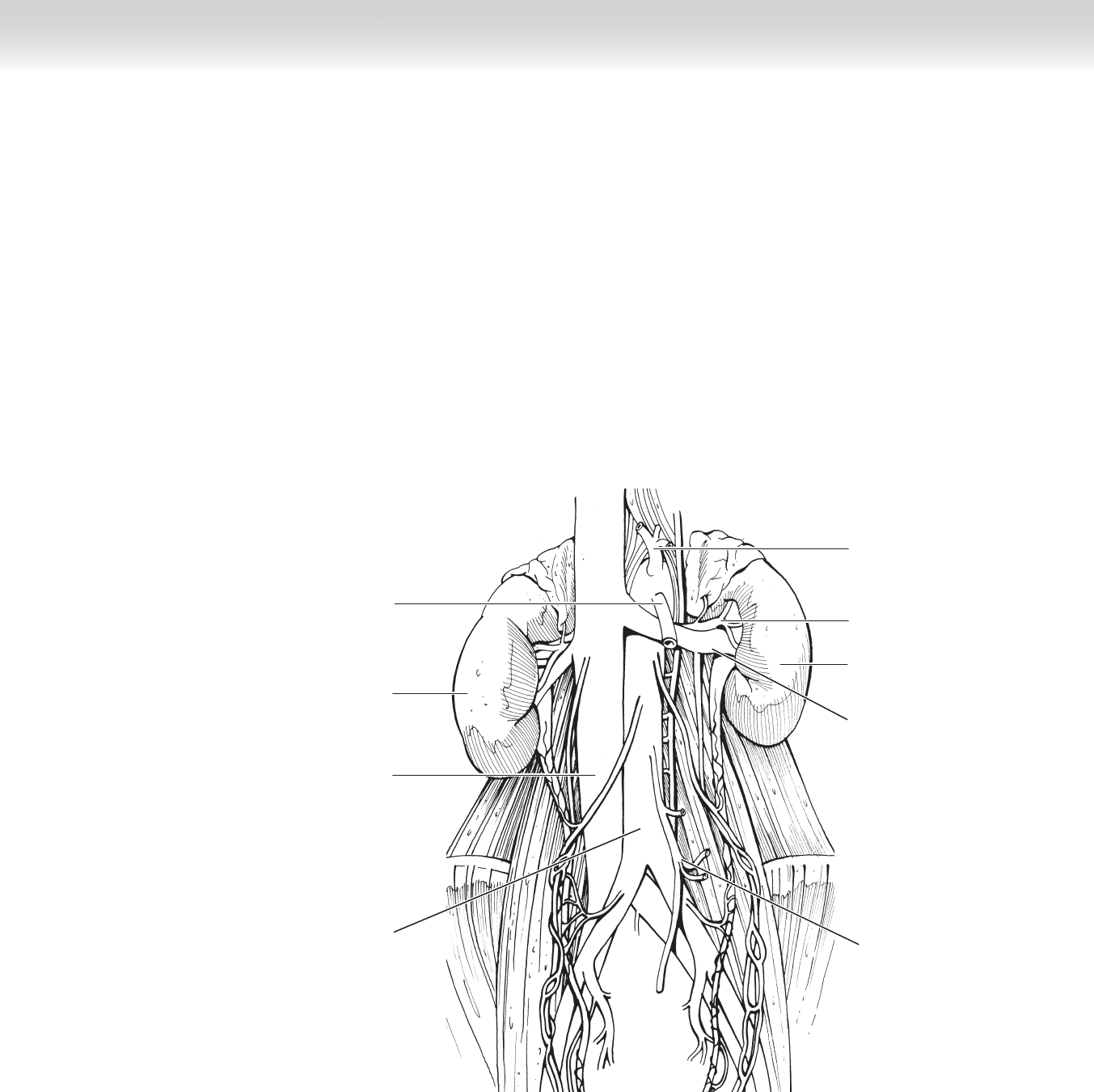
Abdominal
aorta
Inferior vena
cava
Right kidney
Celiac trunk
Left renal artery
Left renal vein
Inferior mesenteric
artery
Left kidney
Superior
mesenteric
artery
FIGURE 82 –1

882 Section XII • Vascular
STEP 3: OPERATIVE STEPS
1. INCISION
◆ For elective aneurysm repair, the operative fi eld is prepped from the nipples to the knees
after induction of general anesthesia and placement of central venous and arterial monitoring
lines. In the setting of a ruptured abdominal aortic aneurysm, the chest, abdomen, and
groins should be prepared and draped before the induction of general anesthesia. Additional
large-bore catheters are inserted peripherally and centrally, with the latter connected to a
rapid infusion device capable of delivering large volumes of blood and blood products.
◆ Aortic aneurysm repair can be undertaken using either a transperitoneal or a retroperitoneal
approach. With the transperitoneal approach, the patient is positioned supine on the oper-
ating table and in the right lateral decubitus position for retroperitoneal exposure of the
aorta (Figure 82-2).
◆ A midline incision extending from the xiphoid process to the pubic symphysis or a transverse
incision extending from fl ank to fl ank above or below the umbilicus provides excellent expo-
sure of the entire intra-abdominal aorta.
◆ The retroperitoneal exposure is particularly helpful in patients with infl ammatory aneurysms,
horseshoe kidney, ostomies, or hostile abdomens. Although this approach allows exposure of
the suprarenal aorta, exposure of the right iliac vessels may be limited and a counterincision
required.
◆ The patient is placed in the right lateral decubitus position over a kidney rest, with the hips
allowed to rotate to the supine position after induction of anesthesia and placement of
monitoring lines.
◆ An oblique incision extending from the lateral border of the rectus sheath 2 cm below the
umbilicus over the tip of the 12th rib is made. Dissection is continued through the external
oblique, internal oblique, and transverse abdominis muscles. The retroperitoneal space is
entered by incising the most lateral aspect of the posterior rectus sheath. Dissection is con-
tinued toward the midline anterior or posterior to the left kidney. The retroperitoneal struc-
tures are retracted to the right of the midline, and repair of the aneurysm is undertaken in
the usual fashion.
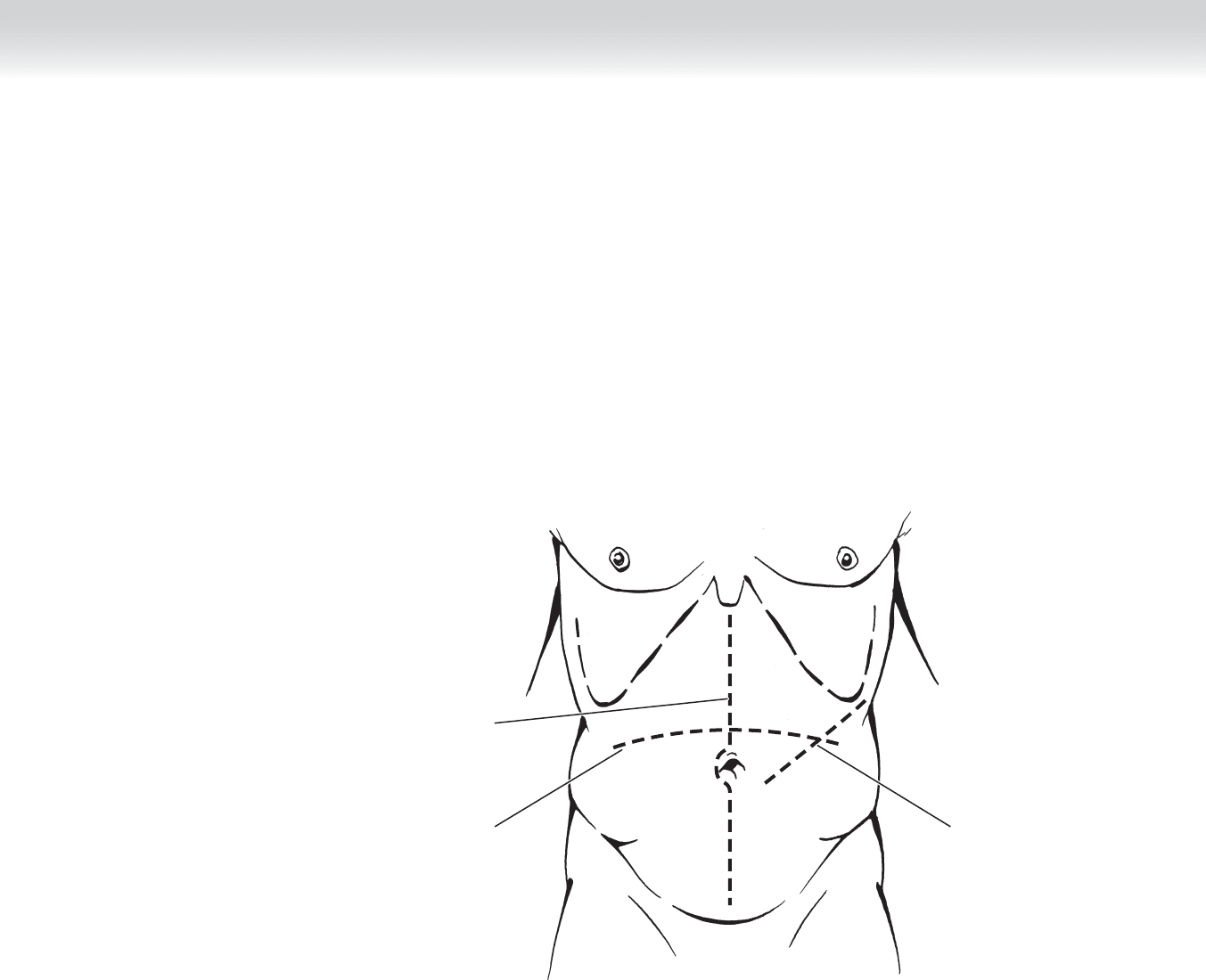
CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 883
Transverse
incision
Oblique incision
for retroperitoneal
exposure
Midline
incision
FIGURE 82 –2
884 Section XII • Vascular
2. DISSECTION
◆ The abdomen is explored to determine the presence of any other pathology.
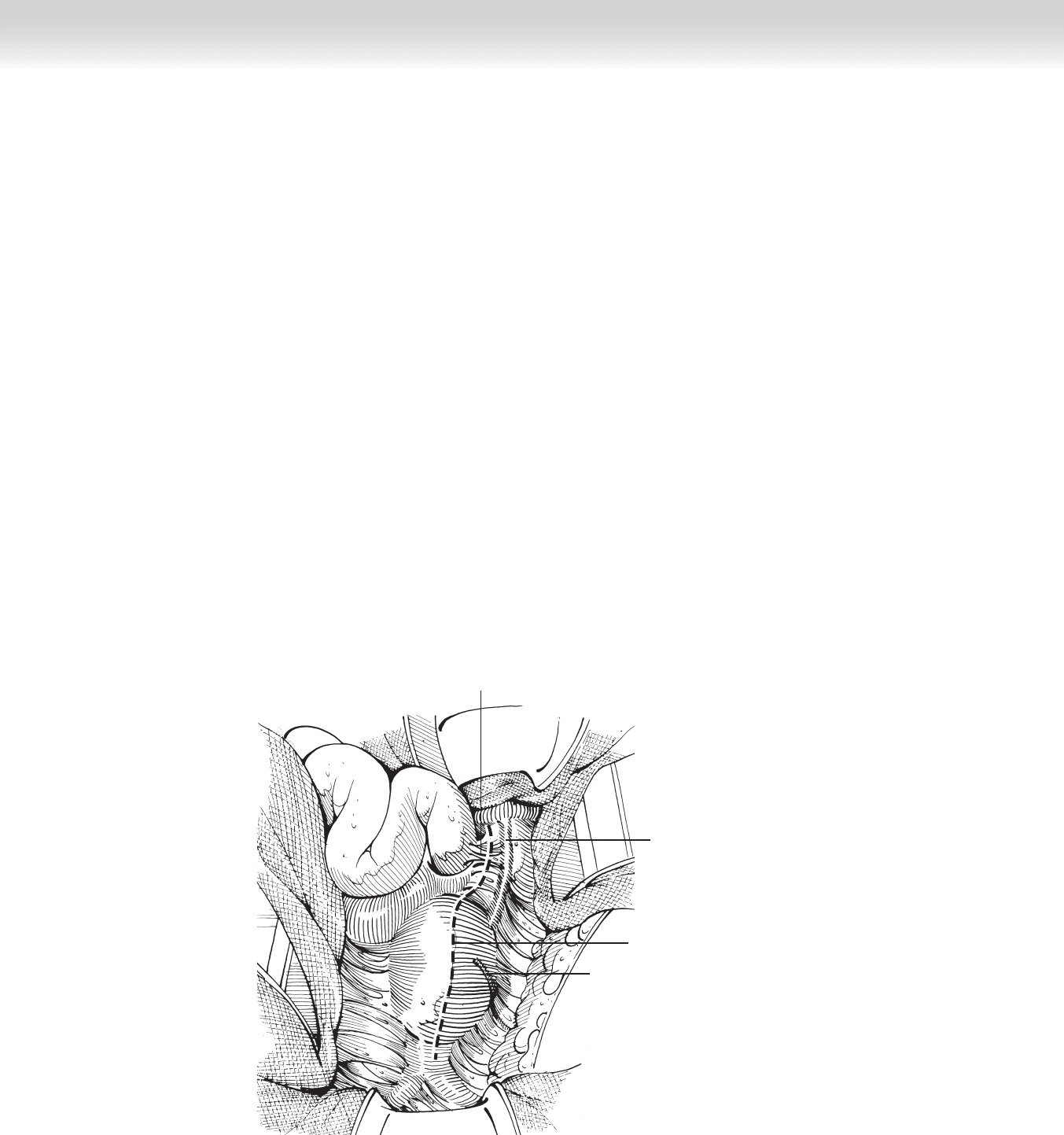
◆ The transverse colon and mesocolon are then lifted cephalad, and the small intestine is
moved to the right side of the abdomen. The peritoneum over the aneurysm is incised from
the level of the left renal vein into the pelvis, a self-retaining retractor such as the Omni-
Tract retractor is placed, and the small bowel returned into the abdomen (Figure 82-3).
◆ Proximal control must be immediately obtained if the aneurysm is ruptured. This is best
achieved by dividing the triangular ligament and retracting the left lobe of the liver cepha-
lad and to the right. The lesser omentum is entered near the level of the esophagogastric
junction. The aorta is palpated through the fi bers of the diaphragm, and the median arcuate
ligament is divided. The fi bers of the diaphragm are bluntly separated, a large angled aortic
clamp is maneuvered into position, and the aorta is occluded. It is unnecessary to dissect
and encircle the aorta before clamping. Once the bleeding is controlled, the dissection can
proceed as for elective aneurysm repair.
Ligament of Treitz
Inferior
mesenteric vein
Inferior
mesenteric artery
Peritoneal incision
FIGURE 82 –3
CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 885
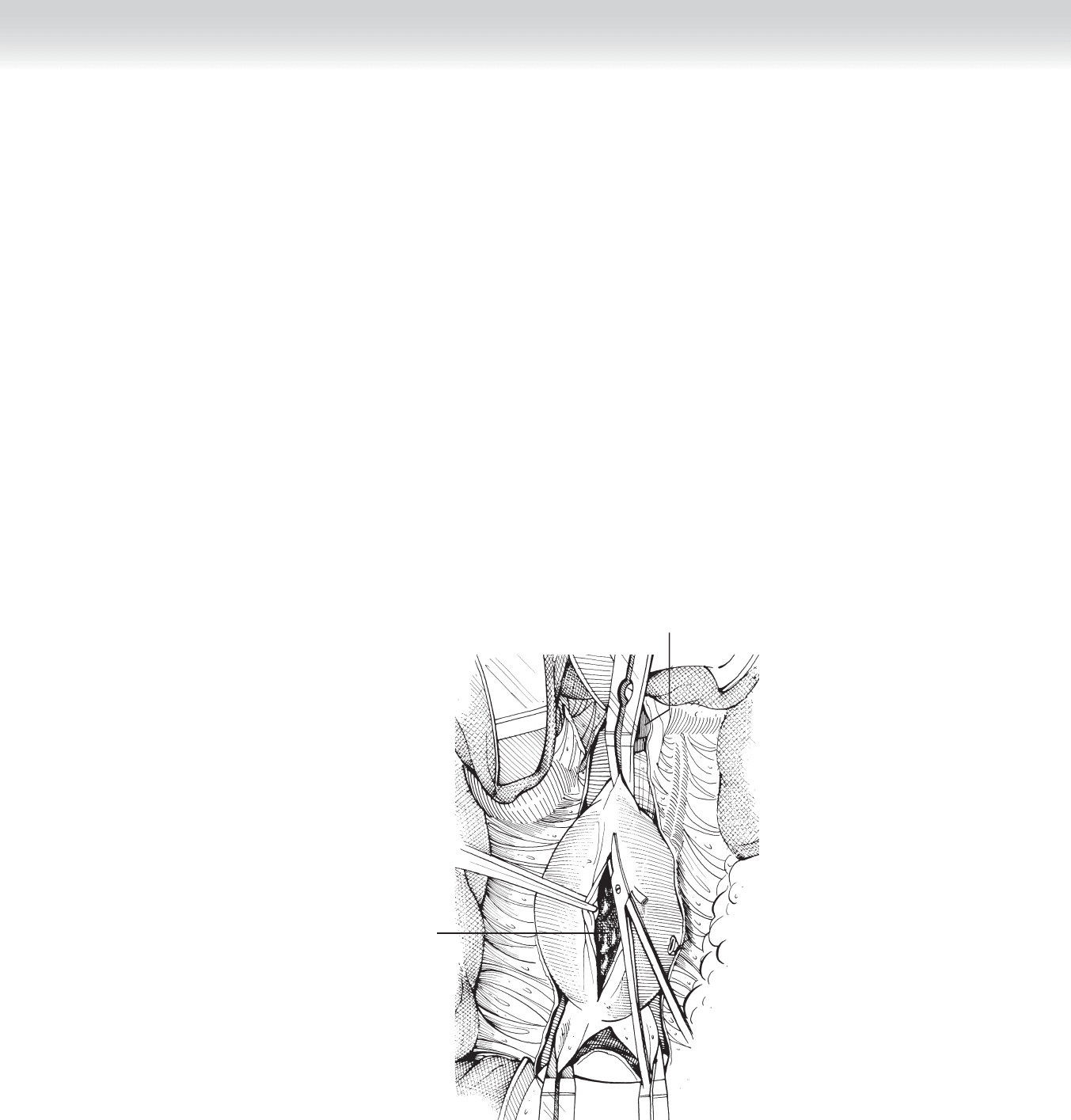
Thrombus
Left renal vein
FIGURE 82 –4
◆ The aorta is dissected between the aneurysm and the renal arteries; in 5% to 10% of patients,
the suprarenal or pararenal aorta is involved. The surgeon should avoid injury to the left renal
vein, which may be fl attened over the proximal end of the aneurysm. Care should be taken to
avoid injury to the iliac veins, which may be closely adherent to the arteriosclerotic arterial
wall. This is best avoided by dissecting only the anterior and lateral surfaces of the common
iliac arteries close to the arterial wall.
◆ The anterior and lateral surfaces of the aneurysm are more completely freed of overlying tis-
sue, care being taken not to interrupt the collateral arterial supply to the descending and
sigmoid colon as it descends in the arcade on the left side of the aneurysm. After the sys-
temic administration of heparin (100 U/kg) and mannitol (12.5 to 25 g), the aorta and iliac
vessels are occluded with vascular clamps. The clamps are placed on the iliac vessels fi rst
and then on the aorta to minimize the risk of distal embolization. When the aorta and iliac
arteries are heavily calcifi ed, occlusion of the aorta at the diaphragmatic hiatus and balloon
catheter occlusion of the iliac arteries may be necessary. The anterior wall of the aneurysm
is incised with a no. 11 blade or electrocautery, and the arteriotomy is continued to the
right of the origin of the inferior mesenteric artery to avoid injury to the hypogastric auto-
nomic plexus on the left (Figure 82-4).
886 Section XII • Vascular
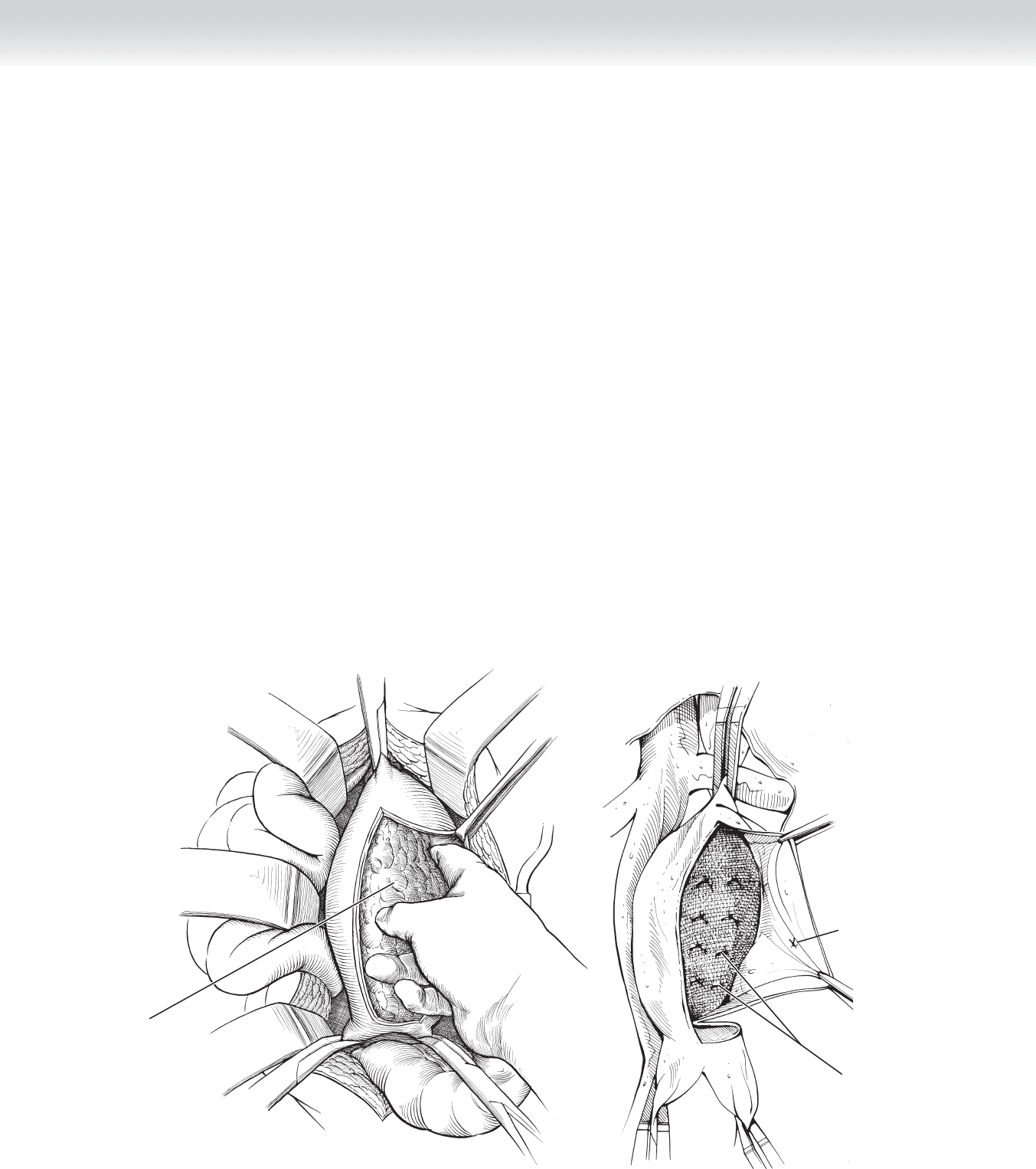
◆ The laminated thrombus and the atherosclerotic debris are removed from within the
aneurysmal sac, often by a sweep of the fi nger. Only adventitia and some media remain
(Figure 82-5).
◆ Back-bleeding from lumbar and median sacral artery orifi ces is controlled with mattress
sutures of 2-0 silk placed from within the opened aneurysm. Assessment of inferior mesen-
teric artery (IMA) backfl ow is then undertaken. If a large orifi ce with pulsatile back-bleeding
is present, the vessel is ligated from within the aneurysm. If a large orifi ce with minimal
back-bleeding is encountered, consideration should be given to reimplantation of the IMA
(Figure 82-6).
◆ The aneurysm wall is cut transversely just distal to its beginning, except for the posterior
third of the circumference if the neck is small. There is no objection to complete transection
of the aorta unless the posterior aortic tissues are thin and friable, in which case it is helpful
to have the retroaortic prevertebral fascia to aid in securing the posterior sutures. In most
cases, the proximal anastomosis can be constructed using the Creech technique, in which
the wall of the aneurysm is used to reinforce the suture line. A prosthetic graft of suitable
diameter is selected, and the body of the graft is shortened to approximately 5 cm if a bifur-
cated graft is to be used. (The aortic portion of the graft is equal, under tension, to the
length of the aortic aneurysm.) The iliac limbs of the graft are left long and appropriately
trimmed just before completion of each anastomosis.
Ligated inferior
mesenteric artery
from within
Ligated lumbar
arteries
FIGURE 82 –6
After Teoli
Laminated
thrombus
FIGURE 82 –5
CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 887
A
Inferior vena
cava
Left renal vein
Construction of
proximal anastomosis
using Creech
technique
Aortic bifurcation
B
Completing distal
anastomosis
FIGURE 82 –7
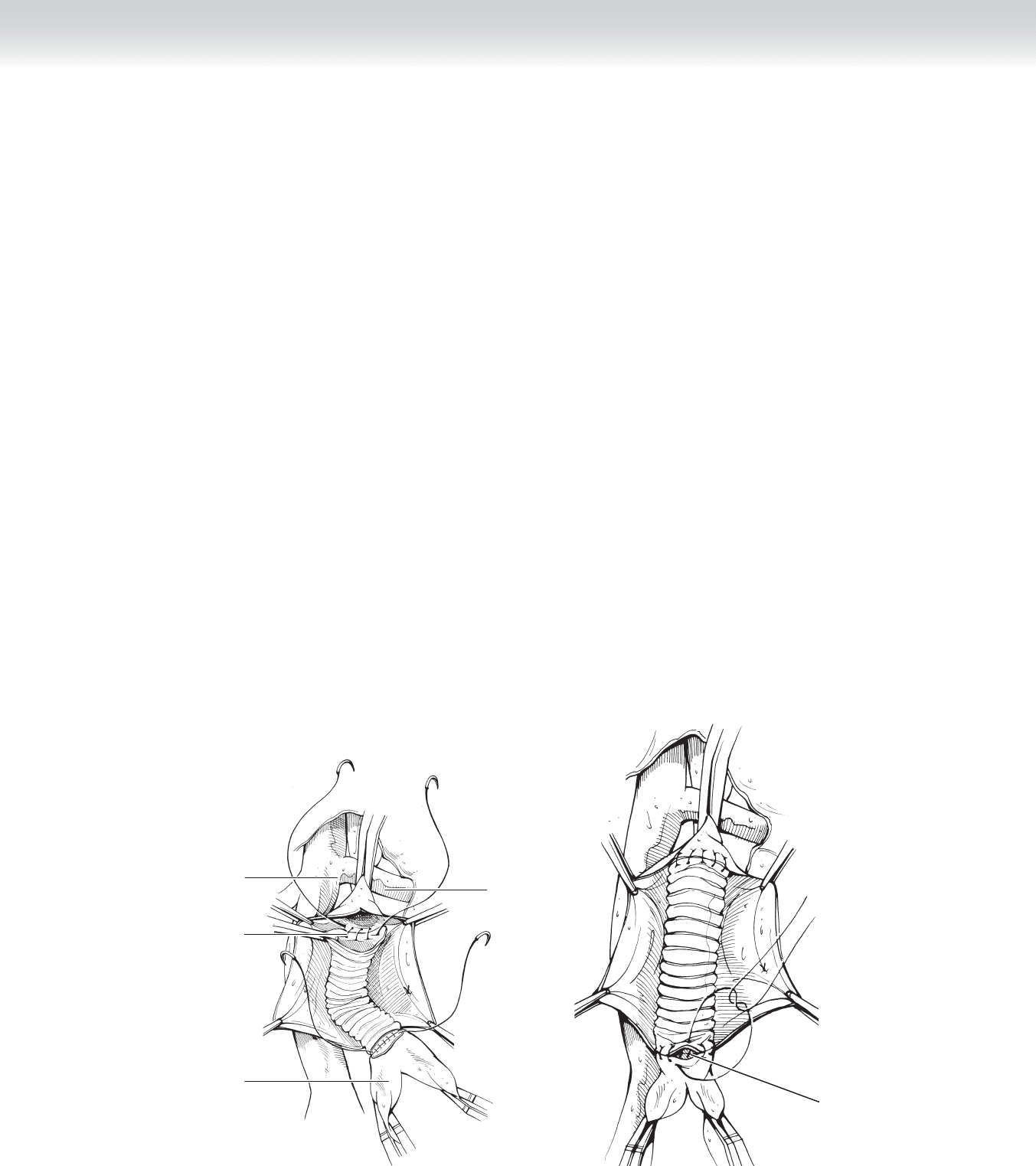
◆ Suturing the graft to the aorta is begun by passing the suture fi rst through the graft and
then through the aorta. Generous deep bites are taken through the aortic tissue to ensure a
strong, blood-tight anastomosis. Several suturing techniques may be used. In this instance,
a single 3-0 monofi lament arterial suture is begun laterally at approximately the 3 o’clock
position, sewing the posterior wall and continuing each end of the suture laterally and ante-
riorly where it is tied. Care must be taken to ensure that the suture is pulled tight before it
is tied (Figure 82-7, A).
◆ The graft should lie within the aortic lumen to allow better hemostasis and to prevent dis-
section beneath an atherosclerotic plaque at the suture line.
◆ The integrity of the aortic anastomosis is assessed by temporarily releasing the aortic clamp
while the graft is occluded digitally or with a shod clamp. This is the time to be certain that
the posterior suture line is secure, because it is diffi cult to expose this area later in the oper-
ation. A shod clamp is placed across the aortic tube graft or each limb of a bifurcated graft.
◆ Liquid blood, clots, and loose debris are aspirated from within the graft before proceeding
with the distal aortic or iliac anastomosis. When a tube graft is used, the aorta above the
bifurcation is partially divided transversely, leaving the posterior wall intact. The anastomo-
sis is constructed using 3-0 polypropylene suture beginning at approximately the 3 o’clock
position, taking deep bites of the posterior wall. Before placement of the fi nal sutures, the
graft and iliac arteries are fl ushed and the anastomosis completed (Figure 82-7, B).
888 Section XII • Vascular
◆ When the distal anastomosis is to the iliac arteries, each iliac bifurcation is dissected, isolat-
ing the external and internal iliac arteries. The common iliac artery is divided 1 cm proximal
to its bifurcation. If the common iliac artery is aneurysmal or otherwise unsuitable for anas-
tomosis, the common iliac artery is oversewn or stapled and the external iliac or femoral ar-
teries used for the distal anastomosis. The external iliac artery is allowed to back-bleed to en-
sure the absence of clot or debris and then fl ushed with heparinized saline. The limbs of the
bifurcated graft are routed within the aneurysm bed to the iliac arteries.
◆ The proximal clamp on the right limb is removed with the distal end occluded digitally to
assess the appropriate length of the graft so that it is long enough to allow for a tension-free
anastomosis but not so long that kinking occurs.
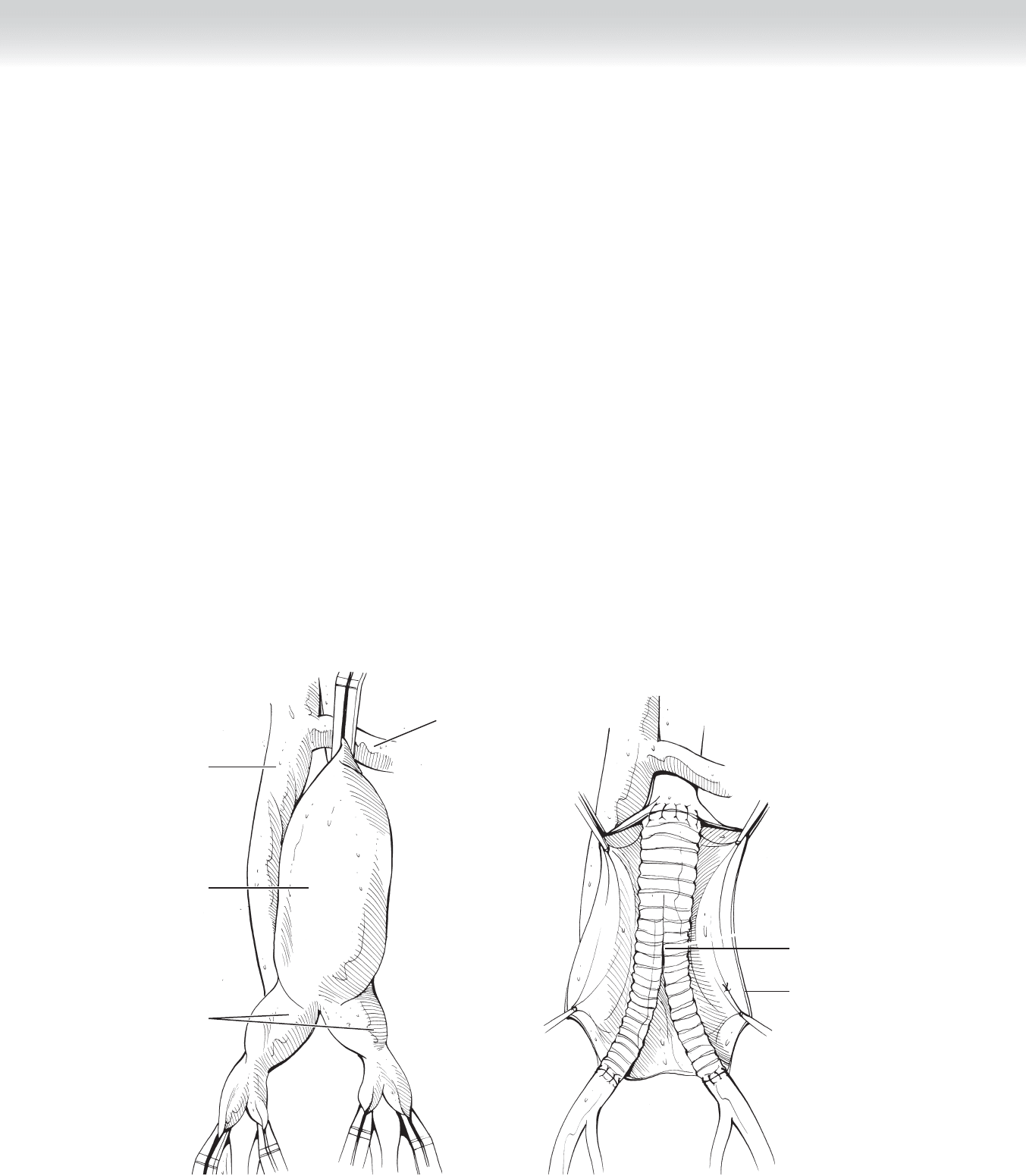
◆ The distal anastomosis on the right is constructed fi rst with a running 4-0 polypropylene
suture. Before fl ow is reestablished, the iliac arteries are allowed to back-bleed, the iliac
limb of the graft is fl ushed, and the remaining sutures are placed (Figure 82-8).
◆ The order of clamp removal is important in preventing of air or atheromatous debris material
from passing into the legs. The clamps on the right internal iliac artery, the right limb of the
graft, and the external iliac artery are removed in sequence and fl ow is reestablished.
A
Inferior vena
cava
Left renal
vein
Aortic aneurysm
Iliac aneurysms
B
Completed aortoiliac
bypass
Aortic wall
FIGURE 82 –8
CHAPTER 82 • Resection of Abdominal Aortic Aneurysm 889
◆ The left limb of the graft is routed through the lumen of the left common iliac artery, and
the anastomosis is completed in a similar fashion as on the right.
◆ After the aneurysmectomy is completed, hemostasis is secured and systemic heparin is
reversed with protamine sulfate (1 mg/100 U heparin).
3. CLOSING
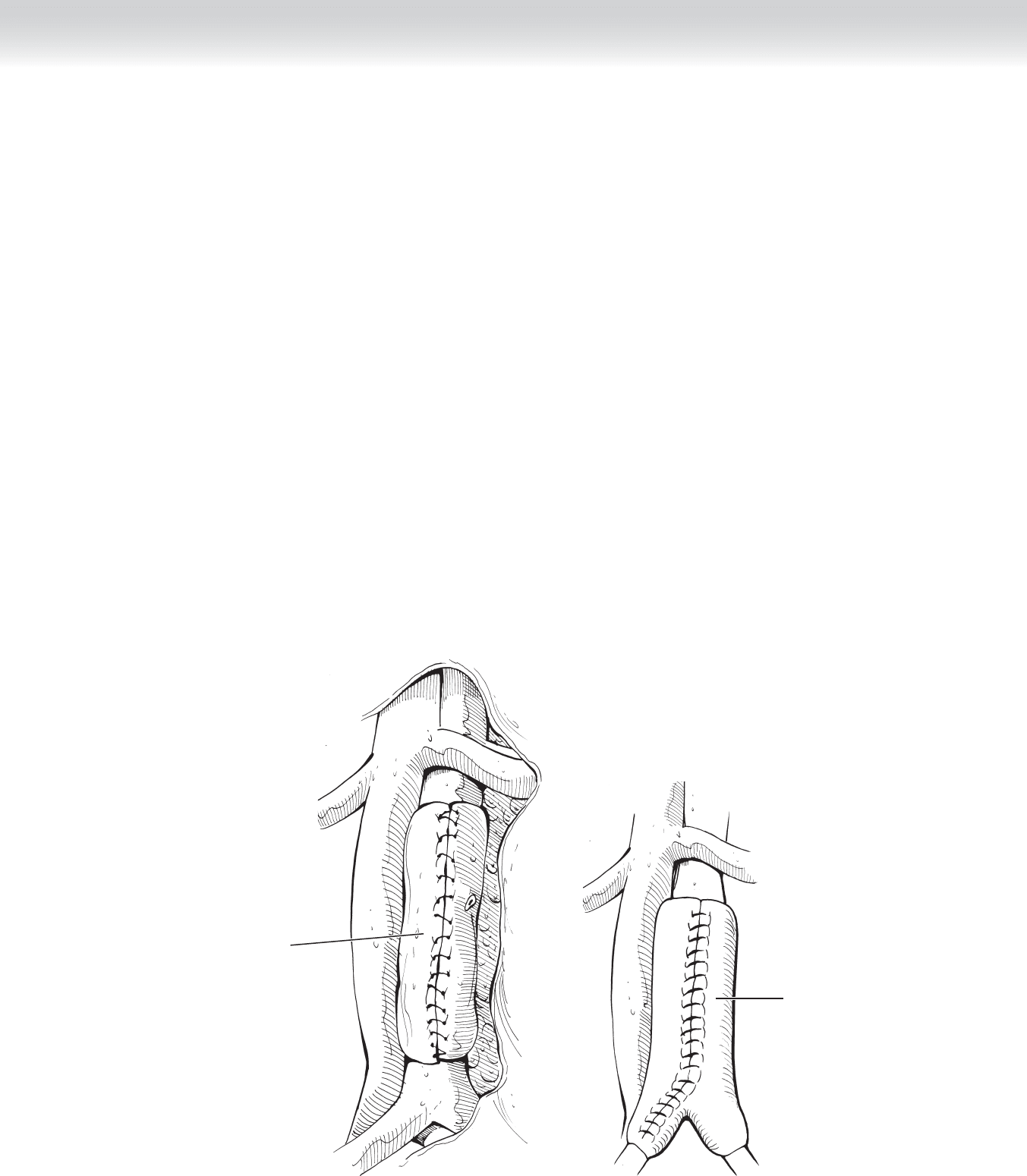
◆ The aneurysm wall is closed over the graft with 0 Vicryl suture (Figure 82-9). To lessen the
risk of an aortoduodenal fi stula, omentum is placed adjacent to the anastomosis. The perito-
neum is closed with absorbable suture, and the abdomen wall structures are reapproximated
with a looped 1-0 running monofi lament polydioxanone (PDS) or polypropylene suture.
A
Aneurysm wall
closed over a
tube graft
B
Aneurysm wall
closed over a
bifurcated graft
FIGURE 82 –9

890 Section XII • Vascular
STEP 4: POSTOPERATIVE CARE
◆ Careful control of fl uid volume and heart rate are essential. Swan-Ganz catheter monitoring
to assess cardiac output and fl uid volume status is a useful adjunct. These patients often
require large volumes of fl uid within the fi rst 24 to 48 hours postoperatively. Suffi cient pain
medication should be administered. Beta blockade begun preoperatively should be contin-
ued throughout the postoperative period. Inotropic agents should be used to ensure ade-
quate cardiac output. Careful monitoring for evidence of mesenteric ischemia is especially
important in patients with ruptured aneurysms.
STEP 5: PEARLS AND PITFALLS
JUXTARENAL ANEURYSM
◆ When the aneurysm involves the pararenal aorta, infrarenal clamping is unsafe. In this situ-
ation, supraceliac occlusion of the aorta and occlusion of the renal and superior mesentery
arteries are necessary. The aorta and graft are appropriately beveled, and the patch of aorta
with the visceral vessels is included in the repair. These maneuvers may require division of
the left renal vein, which may be ligated or reapproximated at the completion of the aortic
anastomosis.
HORSESHOE KIDNEY
◆ A horseshoe kidney occurs in 1 in 600 to 1800 individuals. The lower pole is most often
fused. Each half of the kidney is usually supplied by a single renal artery. Vascular anoma-
lies are often present, and great care should be taken to preserve the aberrant vessels.
HYPOGASTRIC ANEURYSM
◆ Although uncommon, hypogastric aneurysms usually occur deep inside the pelvis and are
diffi cult to control with clamps. Endoluminal suture ligation of the orifi ce or preoperative
coiling will control bleeding from the aneurysm.
AORTOCAVAL FISTULA
◆ Rarely, an undiagnosed communication between the aneurysm and the vena cava is encoun-
tered. This should be suspected if venous blood is seen fl owing into the aneurysm after the
thrombus has been removed from the aneurysm sac. Finger or sponge stick control of the
venous bleeding and endoaneurysm repair of the communication with pledgeted monofi la-
ment sutures will usually suffi ce.