Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 901
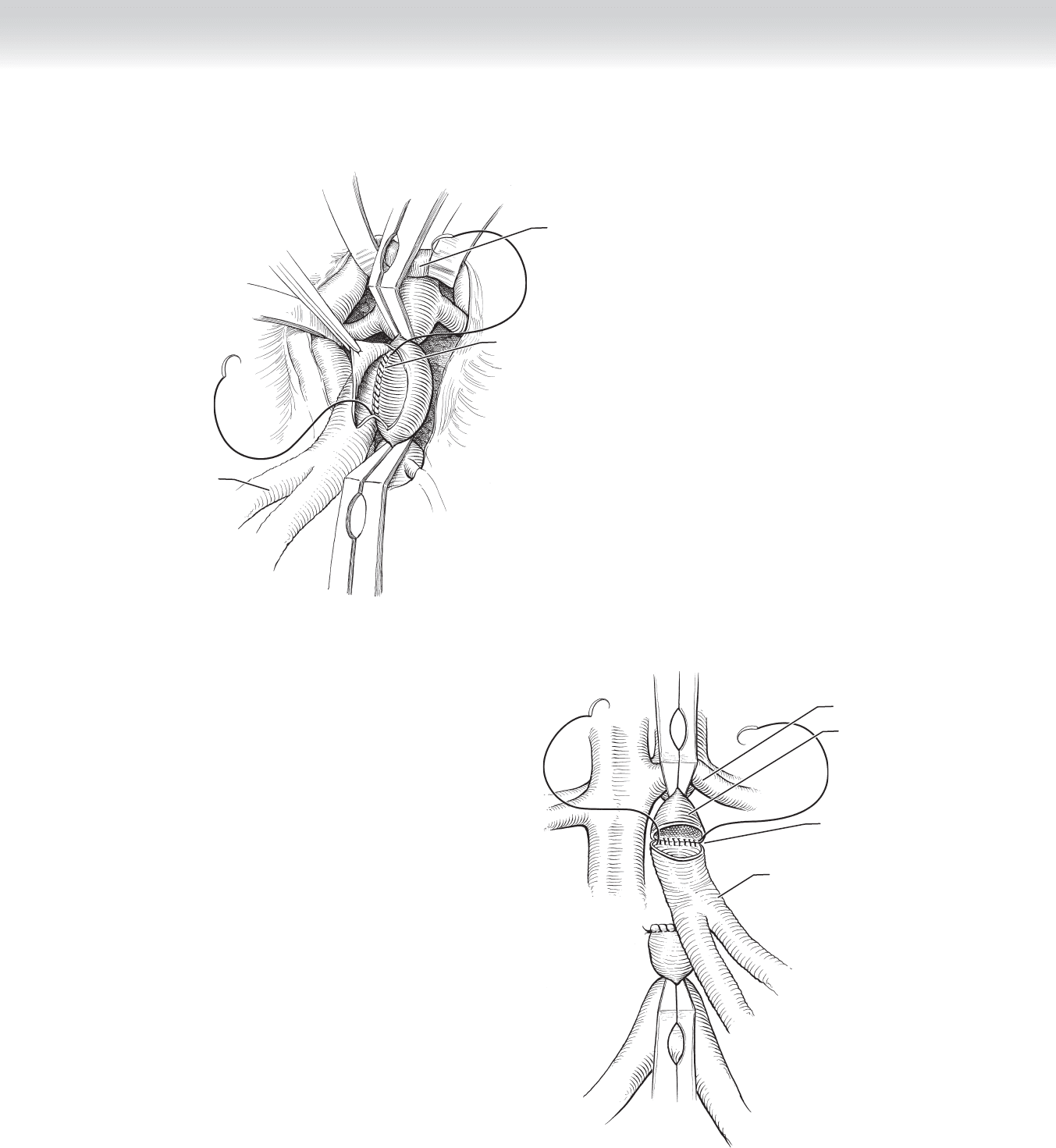
FIGURE 83 –6
Left renal vein
Suture in posterior
anastomosis
Graft
FIGURE 83 –7
Suture in posterior
row of anastomosis
Left renal vein
Abdominal aorta
Graft

902 Section XII • V
ASCULAR
◆ After the aortic anastomosis is completed, the clamp is released for several beats to fl ush
clots, debris, and air. The limb to be used fi rst is then fl ushed with heparinized saline. An
aortic clamp is placed through the tunnel from the groin, and the limb is pulled out of
the abdominal cavity (Figure 83-8).
◆ A plaque-free area in the distal common femoral artery is selected, and the artery is
opened on the anterior surface. The length of the limb is trimmed, and the end of the
graft is beveled. The anastomosis is performed with a 5-0 nonabsorbable monofi lament
suture, starting at the heel (Figure 83-9).
◆ Before the anastomosis is completed, the limb is fl ushed by removing the clamp from the
limb, and the aortic clamp is released. The anastomosis is completed, and the fl ow is
restored fi rst to the common femoral artery and allowed to retrogradely fi ll the iliac artery
in the pelvis so that debris is swept into this vessel rather than toward the feet. The super-
fi cial and deep femoral arteries are then reopened to restore fl ow to the lower extremity.
◆ The procedure is repeated for the other limb.
3. CLOSING
◆ The retroperitoneal tissue is closed over the graft to separate it from the viscera to prevent
future adhesion or erosion of bowel. If this tissue is insuffi cient, the omentum can be used
by bringing it around the left side of the colon and tacking it down on top of the graft. The
bowel is returned to the abdominal cavity, and the nasogastric tube location is reconfi rmed
in the mid-portion of the stomach. The abdominal wall is closed using standard technique.
◆ The groin wound is closed in multiple layers with interrupted and/or running adsorbable
2-0 and/or 3-0 sutures using standard technique.

CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 903
FIGURE 83 –8
Graft
Adominal aorta
Left renal artery
Common
femoral artery
FIGURE 83 –9
Common
femoral artery
Graft
Deep
femoral artery

904 Section XII • V
ASCULAR
STEP 4: POSTOPERATIVE CARE
◆ Patients are monitored in the intensive care unit immediately after surgery for several days
and then transferred to the fl oor unit. Most patients are discharged on their seventh or
eighth postoperative day.
◆ The nasogastric tube is removed with return of bowel function, usually on the third or
fourth postoperative day.
◆ Patients are assisted by physical therapists for early mobilization with ambulation. Aggres-
sive use of incentive spirometry is encouraged. Deep vein thrombosis prophylaxis is used.
◆ Patients are discharged when they have good pain control, exhibit return of bowel function,
and are ambulatory.
◆ Surveillance of the bypass graft patency uses clinical cues, such as pulse examination, and
objective criteria such as ankle-brachial indices (ABIs). Distal perfusion to the feet is verifi ed
in the operating room before closure of the wounds. Any unexpected fi ndings require imag-
ing and possible embolectomy. ABIs are followed in the postoperative period, at the fi rst
postdischarge clinic visit, and then at 6-month intervals.
◆ Initial graft patency rates are nearly 100%. The 5-year patency rates range from 80% to
90%. Long-term patency rate at 10 years is approximately 75%.
◆ Complications include pelvic ischemia caused by interruption of pelvic blood fl ow. Patients
may develop colon ischemia, neurologic defi cit from lumbar ischemia, and infarction of the
pelvic musculature and skin.
◆ Embolization of large atheromatous debris may cause occlusion of major named vessels. Micro-
scopic debris may cause injury ranging from minor focal toe ischemia to extensive tissue loss
involving the major muscle groups of the buttocks, thigh, and leg.
◆ Other complications include lower extremity ischemia, male sexual dysfunction, and
wound infection. Long-term complications include anastomotic pseudoaneurysms or steno-
ses. The most serious complication is aortic graft infection with development of aortoenteric
fi stula. Patients with this complication may present with acute gastrointestinal bleeding or
chronic anemia.
STEP 5: PEARLS AND PITFALLS
◆ The lateral femoral circumfl ex vein is located between the origins of the superfi cial femoral
and deep femoral arteries. Injury to this vein should be avoided during dissection of the
deep femoral artery. When the vein is identifi ed, it may be ligated to provide direct access
to the deep femoral artery.

CHAPTER 83 • Aortofemoral Bypass Graft for Occlusive Disease 905
◆ The inferior epigastric and deep circumfl ex iliac arteries and veins can be found on the
anterior surface of distal external iliac or proximal common femoral arteries beneath the
inguinal ligament. Injury to these branches should be avoided during proximal dissection
of the common femoral artery. Tunneling from the groin wound should be performed under
direct visualization.
◆ In men, distal dissection should avoid the fi broareolar tissue on the anterior surface of the left
common iliac artery. This tissue contains the autonomic nerves that control sexual function.
Extended dissection can lead to nervous disruption and resultant retrograde ejaculation.
◆ The left renal vein anterior to the aorta can be divided to facilitate aortic exposure.
◆ A large pulsatile artery next to the inferior mesenteric artery on the left side of the aorta is
likely a meandering mesenteric artery. This artery provides collateral circulation in the pres-
ence of mesenteric occlusive disease of the celiac or superior mesenteric artery, or both, and
should not be divided.
◆ Interruption of pelvic blood fl ow should be avoided. The use of end-to-end or end-to-side
aortic anastomosis is determined by preoperative arteriography of the abdominal aorta and
bilateral iliac arteries. The end-to-end technique is used for patients who are not dependent
on prograde fl ow in the abdominal aorta. The end-to-side technique is used for patients who
require prograde fl ow to perfuse an important hypogastric or inferior mesenteric artery.
◆ The deep femoral artery can serve as the only outfl ow despite complete occlusion of the
superfi cial femoral artery from atherosclerotic disease. The deep femoral artery is a low-
resistance vessel that is usually free of atherosclerotic disease beyond its secondary
branches.
◆ The common trunk of the bifurcated graft should be short, approximately 3 or 4 cm. This
facilitates coverage of the graft with retroperitoneal tissue to separate the anastomosis from
the overlying viscera. This also reduces the chance of kinking the graft limbs by decreasing
the angle at the bifurcation.
◆ Proximal anastomosis on the aorta is performed just distal to the origins of the renal arter-
ies. The infrarenal aorta can be affected by disease progression from atherosclerosis and
later compromise graft patency.
SELECTED REFERENCES
1. Zarins C, Gewertz B: Atlas of Vascular Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2005.
2. Valentine RJ, Wind GG: Anatomic Exposures in Vascular Surgery, 2nd ed. Philadelphia, Lippincott
Williams & Wilkins, 2003.
3. Moore WS: Vascular and Endovascular Surgery: A Comprehensive Review, 7th ed. Saint Louis, Saunders,
2006.
4. Zelenock GB, et al: Mastery of Vascular and Endovascular Surgery, 4th ed. Philadelphia, Lippincott
Williams & Wilkins, 2005.

906
STEP 1: SURGICAL ANATOMY
◆ The carotid sheath and its contents—including the extracranial carotid artery, the internal
jugular vein, and the vagus nerve—are located in the anterior triangle of the neck, which is
bounded by the mandible, the midline, and the strap muscles. Successful carotid endarter-
ectomy requires a thorough understanding of the anatomy of the anterior triangle, in partic-
ular because a number of cranial nerves are located in the area and are easily injured if care
is not taken to identify and preserve them.
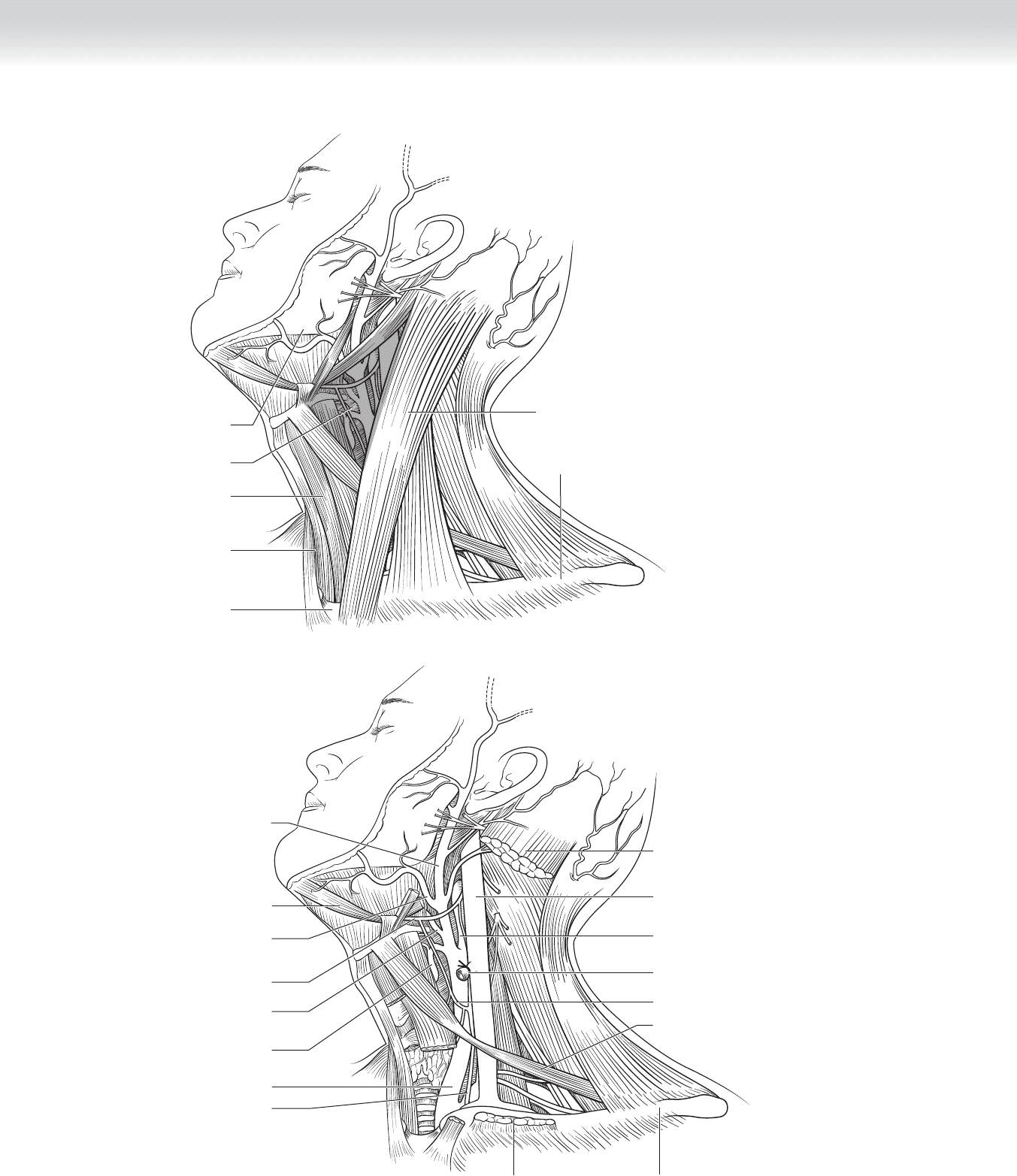
◆ Figure 84-1 demonstrates the structures found in the anterior triangle of the neck. The
venous anatomy is variable. In the most commonly found situation, the anterior facial trib-
utary crosses anterior to the carotid arteries at the level of the common carotid bifurcation
and joins the internal jugular vein.
◆ The common carotid artery in the cervical region has no branches other than the external
and internal carotid arteries. The internal carotid artery in this region also has no branches,
except in rare situations. The persistent hypoglossal artery, a fetal structure that normally
regresses before birth, is found in less than 0.1% of cases. The external carotid artery most
commonly has three branches in the immediate region of the carotid bifurcation—the supe-
rior thyroid, lingual, and facial—although this anatomy can also be highly variable (see
Figure 84-1, A and B).
CHAPTER
84
Carotid Endarterectomy
Lois A. Killewich
CHAPTER 84 • Carotid Endarterectomy 907
Sternocleidomastoid
muscle
Clavicle
Sternum
Strap
muscles
Mandible
Anterior
triangle
Midline
A
External carotid
artery
Facial artery
Digastric muscle
Lingual artery
Superior thyroid
artery
Hypoglossal
nerve
Common
carotid artery
Vagus nerve
Sternocleidomastoid (cut)
Sternocleidomastoid (cut
)
Clavicle
Omohyoid muscle
Ansa cervicalis
Anterior facial
vein (ligated)
Internal carotid
artery
Internal jugular
vein
B
FIGURE 84 –1

908 Section XII • Vascular
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Standard indications for carotid endarterectomy include a stenosis of 50% or higher in a
patient with a transient ischemic attack or stroke thought to originate from internal carotid
artery plaque and 60% to 80% stenosis in an asymptomatic patient. Recurrent stenosis,
stenosis secondary to radiation therapy, and high-risk patients with severe coronary artery
or pulmonary disease are often treated with carotid stenting.
◆ Carotid endarterectomy can be safely performed with the patient under general, regional,
or local anesthesia. Whichever technique is selected, a method must be used to ensure that
the patient has adequate intracranial blood fl ow while fl ow through the operated internal
carotid artery is interrupted. When local or regional anesthesia is used, the patient’s neuro-
logic status can be monitored by assessing contralateral motor function and, in some cases,
speech. Many surgeons use a squeeze toy in the contralateral hand and instruct the patient
to squeeze the toy to demonstrate that neurologic function is maintained when the carotid
arteries are clamped. If general anesthesia is used, neurologic function can be monitored
by measuring carotid back-pressure (the internal carotid artery pressure with the common
and external carotid arteries; a mean arterial pressure of 25 to 40 mm Hg is suffi cient), by
using electroencephalographic or evoked potential monitoring, or by using routine carotid
shunting.
◆ Patients should be administered 325 mg of aspirin by mouth daily, starting before the surgi-
cal procedure. In selected instances, clopidogrel (75 mg by mouth daily) may be used in
addition to or in place of aspirin.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The head should be positioned with the neck hyperextended and rotated to the contra-
lateral side. This can be facilitated by placement of a rolled sheet between the shoulder
blades. The standard incision is placed along the medial border of the sternocleidomas-
toid muscle. The superior aspect should be extended posteriorly to the ear to ensure
against division of the greater auricular nerve (Figure 84-2, A).
◆ For a more cosmetically pleasing result, the incision can be created in a mid-cervical skin
crease, with an extension superiorly toward the ear (Figure 84-2, B).
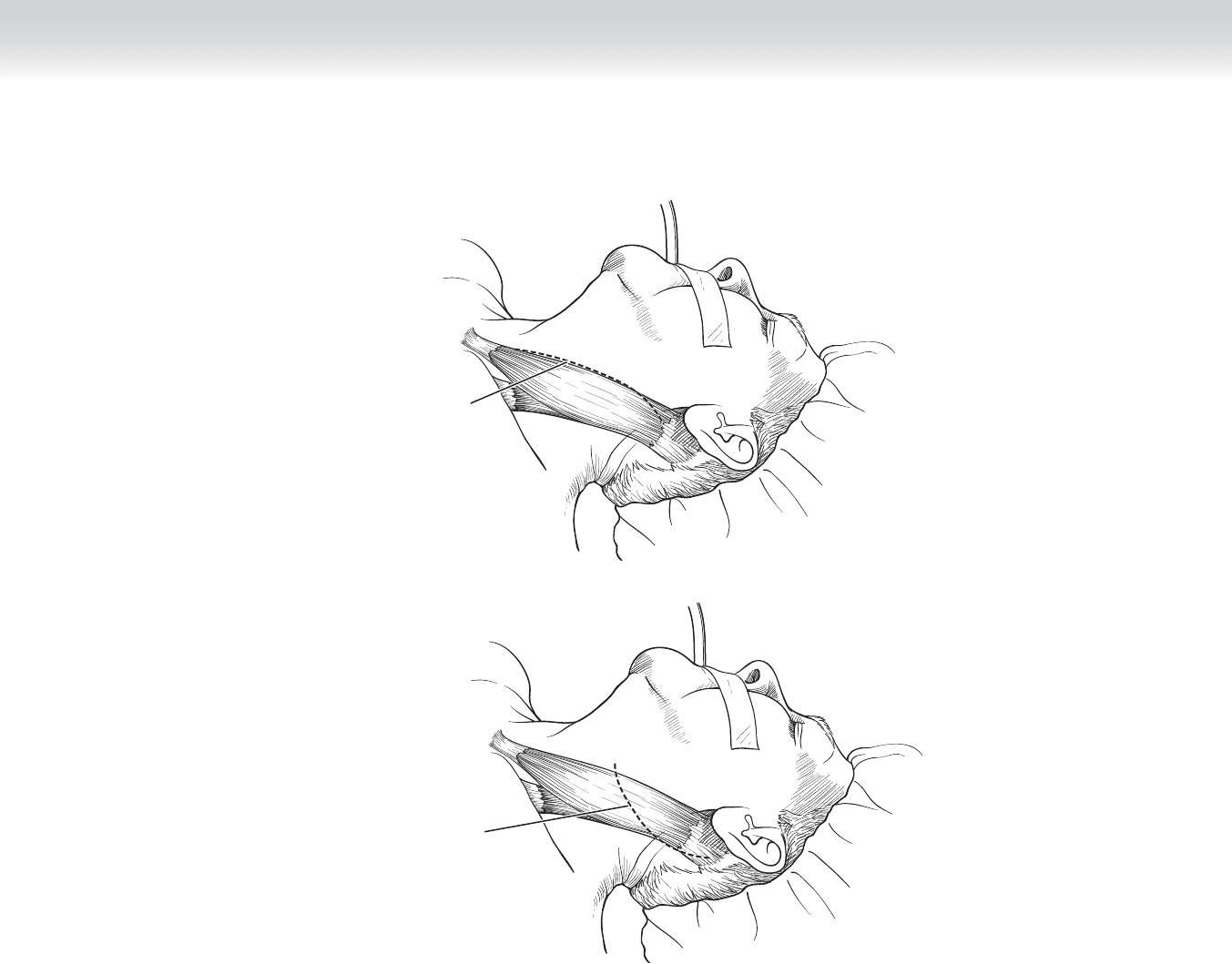
CHAPTER 84 • Carotid Endarterectomy 909
A
Incision
for carotid
endarterectomy
Alternative
incision for carotid
endarterectomy
B
FIGURE 84 –2

910 Section XII • Vascular
2. DISSECTION
◆ After the incision is created, the platysma muscle is divided with electrocautery parallel to
the skin incision. If the cervical skin crease incision is used, fl aps must be created deep
to the platysma muscle and extended superiorly toward the mandible and inferiorly toward
the clavicle. This can be accomplished using a combination of electrocautery and blunt
dissection, which enlarges the operative fi eld to allow the dissection to be continued in
standard fashion.
◆ The dissection is deepened along the medial border of the sternocleidomastoid muscle until
the carotid sheath is identifi ed (Figure 84-3). Small arteries and veins, which extend across
the dissection line to supply the sternocleidomastoid muscle, are cauterized. The
carotid sheath is opened using sharp dissection. (I prefer 7-inch Potts-Smith scissors, but
either Metzenbaum or tenotomy scissors can also be used.)
◆ Once the sheath is opened, the dissection of the carotid arteries is completed using scissors
(Figure 84-4). The common carotid artery is dissected fi rst, followed by the external
carotid artery and the superior thyroid artery. It is generally not necessary to continue the
dissection of the external carotid artery beyond the second branch, which may be the lingual
artery or a combined trunk of the lingual and facial arteries. Once this dissection is com-
pleted, anticoagulants are administered to the patient systemically, usually with unfraction-
ated heparin at a dose of 100 units/kg body weight. The dissection of the internal carotid
artery is completed while the heparin is circulating, which provides some measure of protec-
tion from embolization of plaque from the internal carotid artery during the dissection.
When the dissection is completed, the arteries are controlled with vessel loops, sutures, or
Rumel tourniquets.
3. DETERMINING THE NEED FOR INSERTION OF A SHUNT
◆ The dissected vessels are clamped so that the need for shunting can be determined. Except
in the case of back-pressure monitoring, the internal carotid artery beyond the area of
plaque is clamped fi rst to prevent embolization into the intracranial circulation. I prefer a
Gregory bulldog for clamping of the internal carotid artery; other choices include a Yasargil
aneurysm clip or a small vascular clamp such as a Karchner. The common and external ca-
rotid arteries are also clamped with small vascular clamps; branches of the external carotid
artery can be controlled with Yasargil clips, hemoclips, or Pott’s knots.
◆ If back-pressure monitoring is used to determine the need for shunting, the internal carotid
artery is not clamped. A 19-gauge butterfl y needle or a small angiocatheter connected to pres-
sure tubing is inserted into the artery distal to the plaque. It is imperative that this tubing be
fl ushed thoroughly with heparinized saline before insertion to prevent introduction of air into
the carotid, and hence intracranial, circulation. The back-pressure is then measured; I use a
cutoff of 40 mm Hg mean arterial pressure to determine the need for insertion of a shunt.