Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

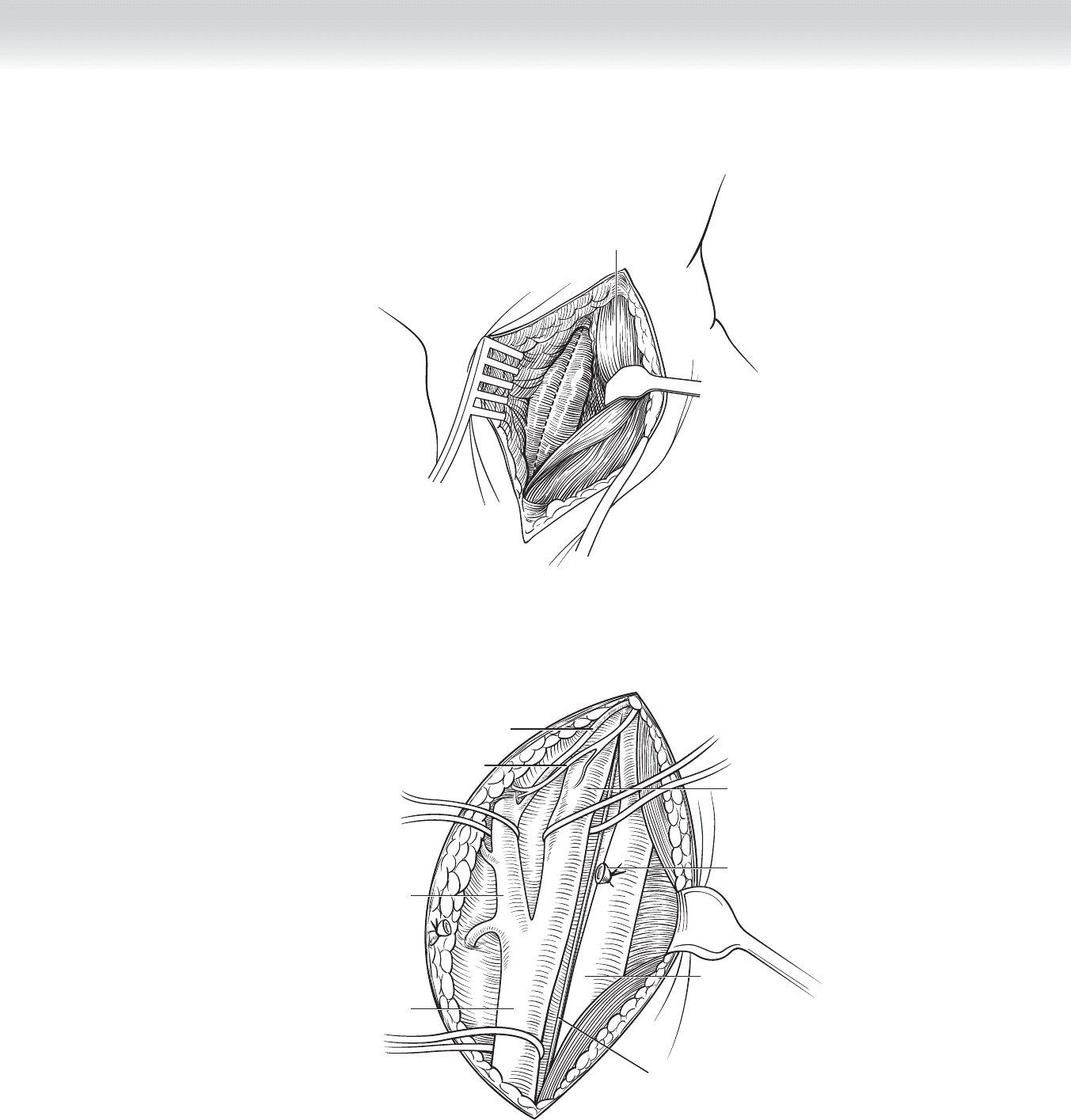
CHAPTER 84 • Carotid Endarterectomy 911
Sternocleidomastoid
FIGURE 84 –3
Common carotid
artery
External carotid
artery
Occipital artery
Hypoglossal nerve
Ligated anterior
facial vein
Internal carotid
artery
Internal
jugular
vein
Vagus
nerve
FIGURE 84 –4
912 Section XII • Vascular
◆ Other methods for shunt determination include electroencephalogram, somatosensory
evoked potentials, or awake patient monitoring. The electroencephalogram measures global
hemispheric functioning, and evoked potentials measure peripheral nerve function. In gen-
eral, a fl attening of amplitude on the affected side indicates the need for a shunt. If the
patient is awake and a shunt is required, the patient will lose function of the contralateral
hand or foot, or both, and be unable to follow commands. It should be emphasized that
these changes are almost immediate, so this assessment requires at most 3 minutes.
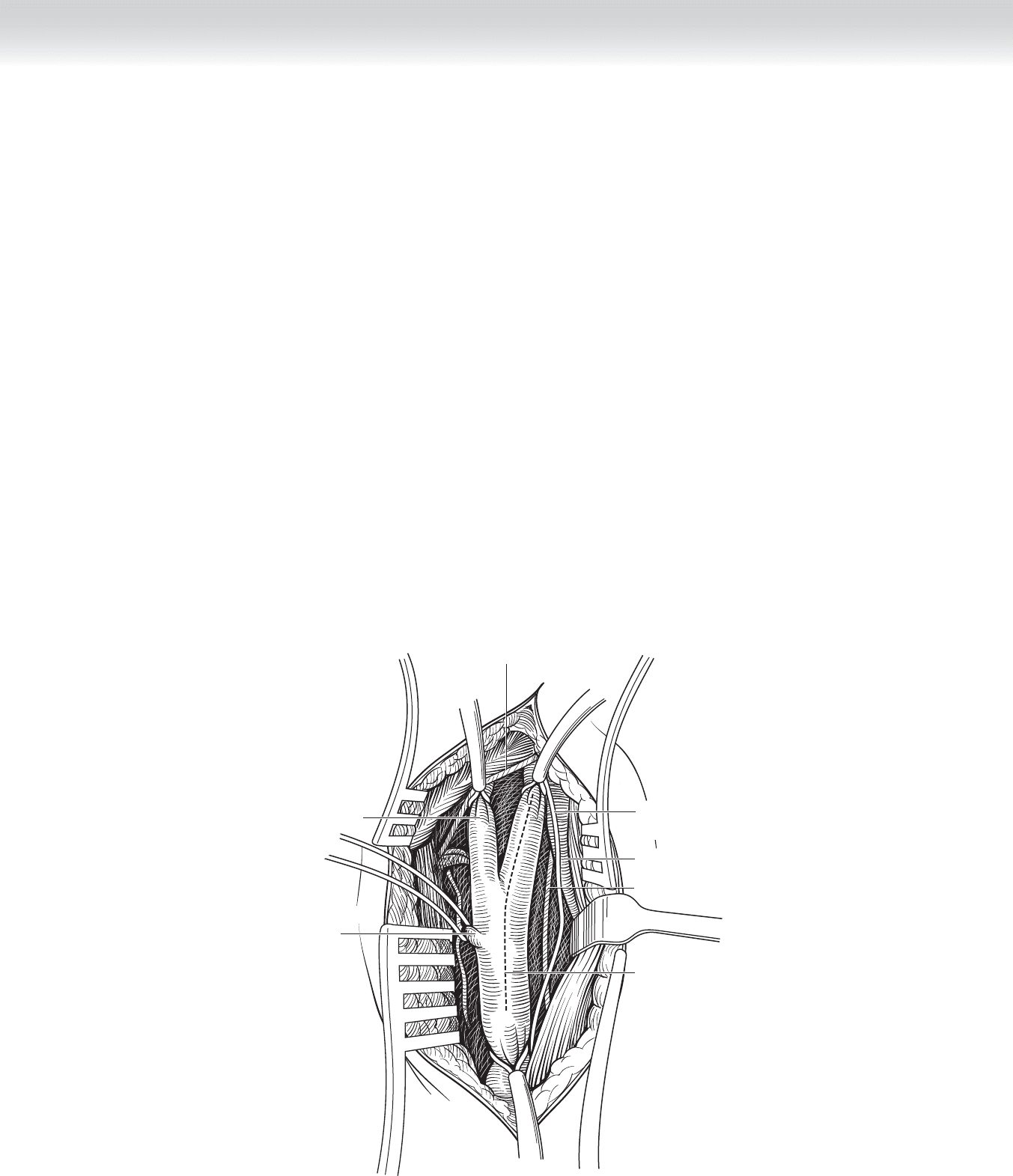
◆ Once the decision regarding shunting has been made, an arteriotomy is created on the distal
anterior surface of the common carotid artery using a no. 11 blade and is extended through
the region of plaque in the internal carotid artery using Potts scissors (Figure 84-5).
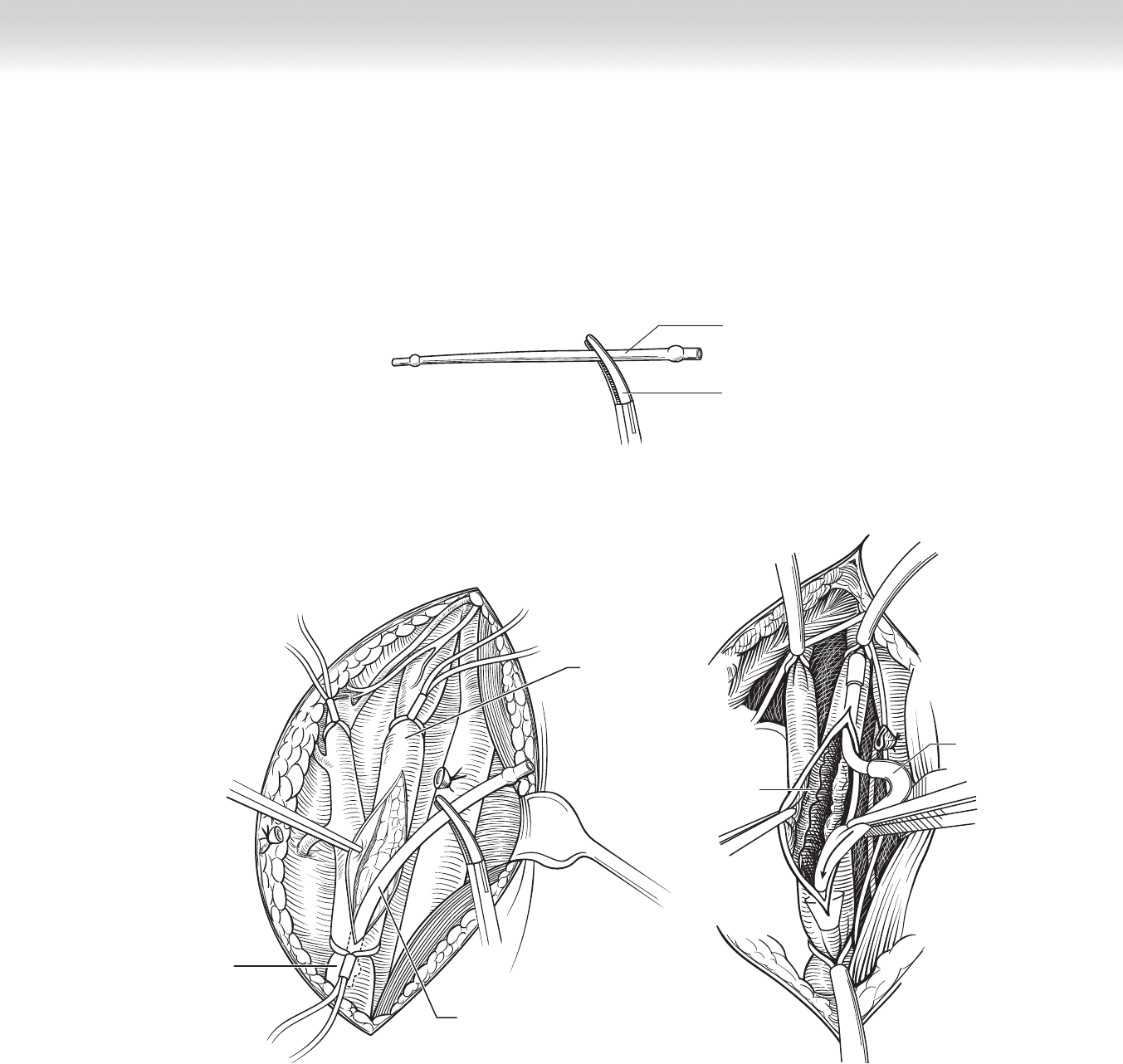
◆ If a shunt is to be used, it should be fl ushed with heparinized saline and clamped in the mid-
portion before insertion (Figure 84-6, A). I insert the proximal end into the common carotid
fi rst, fl ush blood out the distal end, reclamp the mid-portion, insert the distal end into the
internal carotid artery, check for bubbles, and then release the clamp (Figure 84-6, B-C).
Either specially designed shunt clamps or Rumel tourniquets can be used to fi x the shunt in
the arterial ends during endarterectomy. During the shunt insertion, the common and internal
carotid arteries should be controlled with doubly looped vessel loops.
Hypoglossal nerve
External
carotid
artery
Superior thyroid
artery with Pott’s ligature
Ansa cervicalis
nerve
Internal jugular vein
Proposed
arteriotomy
Vagus nerve
FIGURE 84 –5
CHAPTER 84 • Carotid Endarterectomy 913
Shunt
Clamp
A
B
Common carotid
artery
Internal carotid
artery
Shunt
Plaque
Shunt
C
FIGURE 84 –6

914 Section XII • Vascular
4. ENDARTERECTOMY
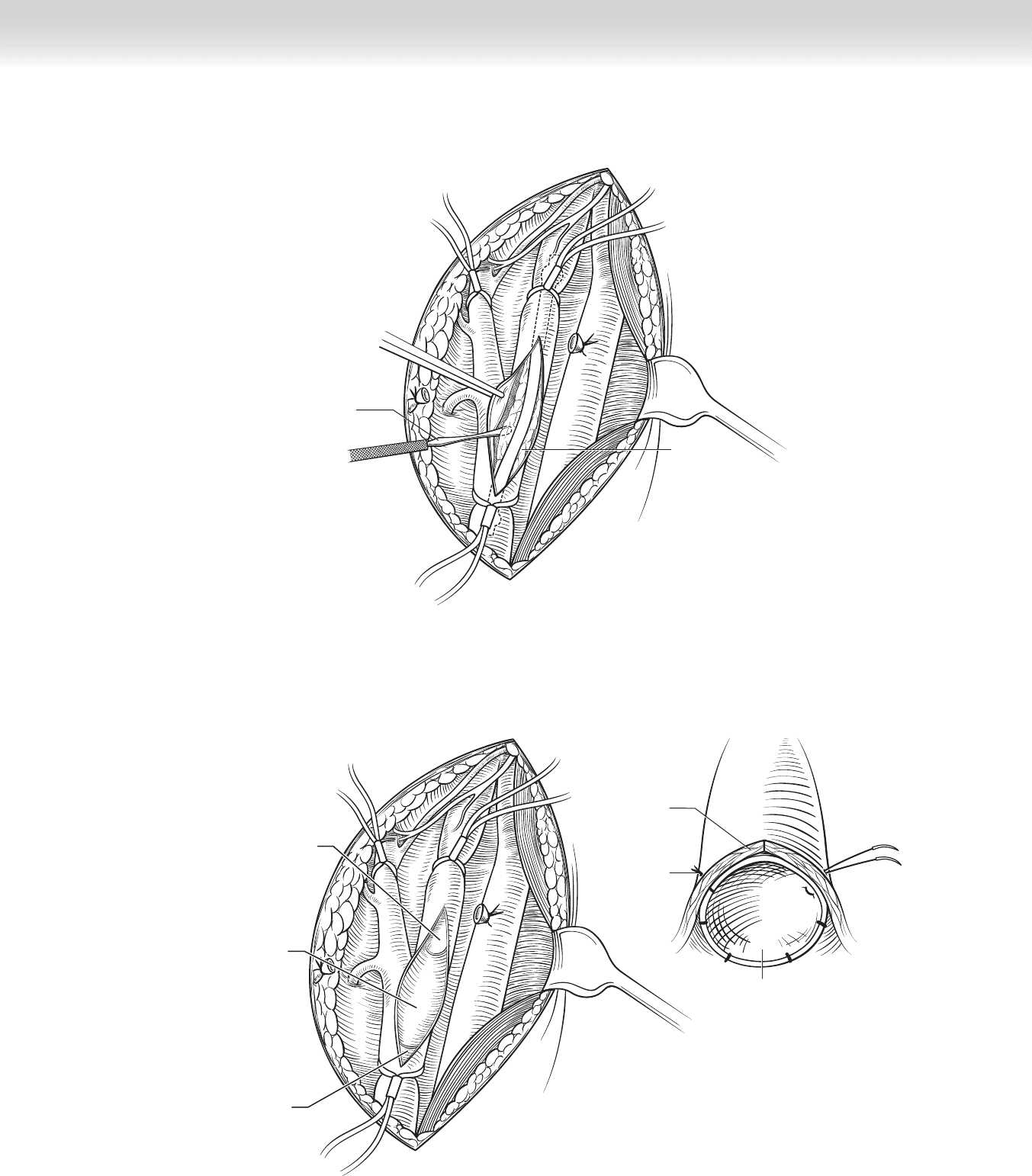
◆ The endarterectomy is performed using a Freer elevator (Figure 84-7). This is inserted into
the plane between the circular muscle fi bers and the adventitia, beginning in the common
carotid artery. The adventitia is pushed away from the muscle fi bers extending distally.
When the end of the plaque is reached, gentle pressure on the plaque pulling inferiorly and
toward the contralateral side will usually separate it from the normal distal artery. Alterna-
tively, a Beaver blade can be used to divide the plaque from the normal artery. The plaque
can then be peeled off transversely. The remainder of the plaque is removed from the inter-
nal and common carotid arteries in a similar fashion.
◆ The plaque is removed from the external carotid artery using an eversion technique. The
adventitia of the artery is everted by the surgical assistant, while the plaque and circular
muscle fi bers are dissected away circumferentially by the surgeon using the Freer elevator.
The plaque is avulsed at its natural end.
◆ Once the specimen is removed, any remaining debris or circular smooth muscle fi bers can
be removed by scraping transversely with the Freer elevator or a Kittner sponge. If the edge
of the distal endpoint has been lifted up, it should be tacked down with 7-0 Prolene as
shown in Figure 84-8. The proximal endpoint does not need to be tacked because it will
be pushed into the adventitia of the artery by the blood fl ow.
CHAPTER 84 • Carotid Endarterectomy 915
Freer
elevator
Plaque
FIGURE 84 –7
Circular
muscle fibers
Tacking
suture
Proximal
intima
Endarterectomized
artery
Distal intima
Endarterectomized
section
FIGURE 84 –8
916 Section XII • Vascular
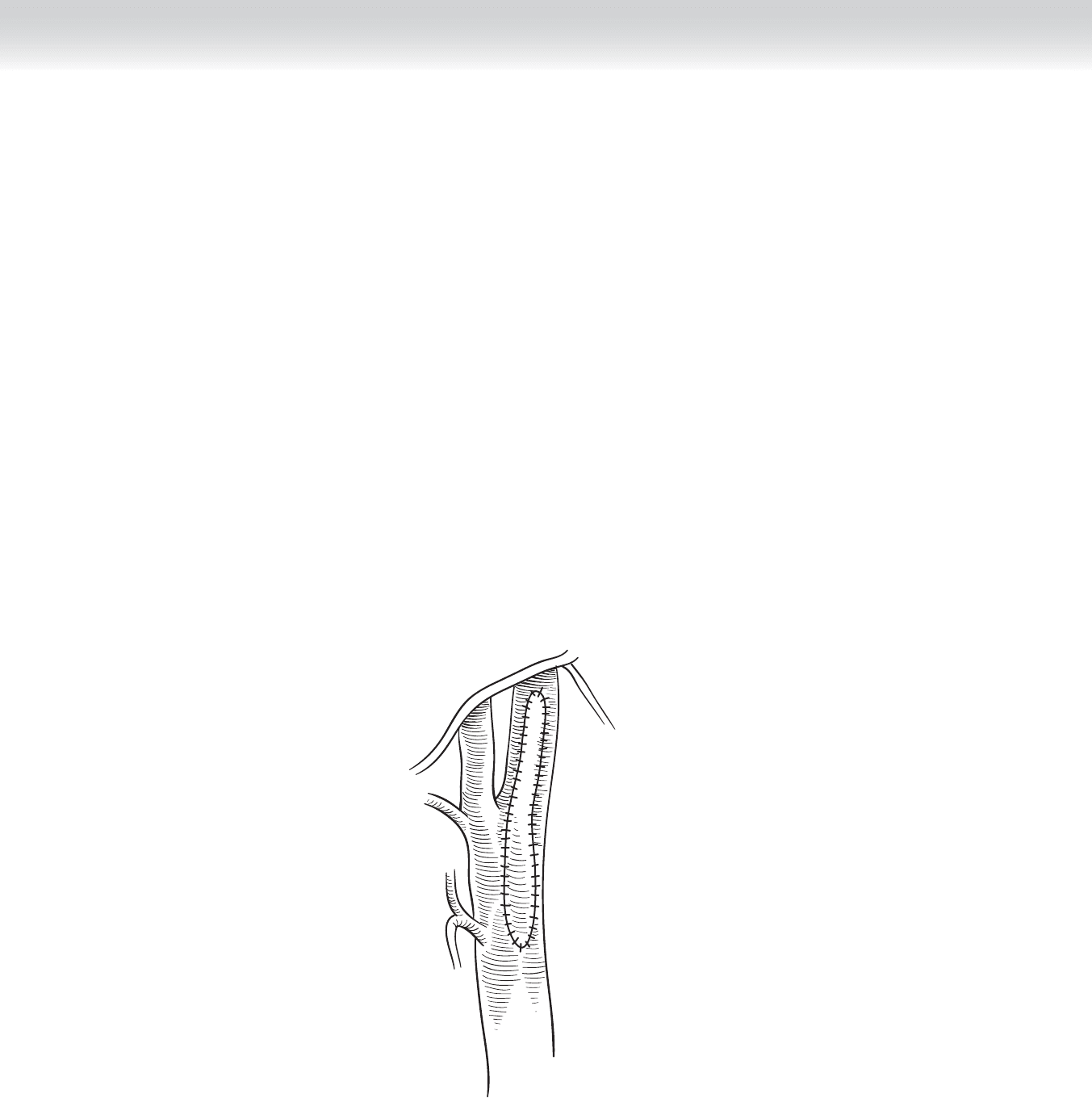
◆ It is the current standard of care to close the arteriotomy with a patch, as shown in
Figure 84-9. Prosthetic patches are used most commonly, either Dacron or expanded
polytetrafl uoroethylene (ePTFE). Before the fi nal closure, fl ushing should be performed
with care taken to ensure that the internal carotid artery is fl ushed last. If a shunt has been
used, this should be removed before fl ushing. Once fl ushing is completed, the inner surface
of the endarterectomized vessel is irrigated copiously with heparinized saline, and the clo-
sure is completed. The internal carotid artery is then back-bled into the common carotid ar-
tery and gently clamped across its origin. (I use DeBakey pickups.) Flow is then restored
through the common carotid artery into the external carotid artery, providing an additional
means for fl ushing any remaining debris or air, or both, into the external carotid artery
rather than the intracranial circulation. After 10 seconds, fl ow is restored through the inter-
nal carotid artery.
◆ It is possible to perform an intraoperative duplex ultrasound or angiogram to check the
operative result, although this has not been my practice.
FIGURE 84 –9

CHAPTER 84 • Carotid Endarterectomy 917
5. CLOSING
◆ The heparin can be reversed using protamine, if necessary. The platysma is closed with
running 3-0 Vicryl. The skin is closed with 4-0 Monocryl and surgical glue. In some cases,
I place a drain in the surgical site, bringing it out through a lateral skin stab incision. If a
drain is used, it should be removed on the morning of the fi rst postoperative day.
STEP 4: POSTOPERATIVE CARE
◆ Aspirin or clopidogrel, or both, should be continued daily throughout the postoperative
period. Most surgeons would continue at least one of these medications for life.
◆ Drains should be removed on the fi rst postoperative day.
◆ Hematoma in the neck can cause respiratory compromise. If a rapidly expanding hematoma
or any evidence of respiratory compromise exists, the patient should be return emergently
to the operating room for evacuation and control of the hemorrhage.
◆ Cranial nerves, which can be injured during the surgery, include the vagus, recurrent laryn-
geal, external branch of the superior laryngeal, hypoglossal, and marginal mandibular branch
of the facial. Vagal and recurrent laryngeal injuries result in hoarseness secondary to vocal
cord paresis or paralysis in the midline. A patient who is hoarse after carotid surgery should
have a vocal cord assessment, in particular if contralateral carotid surgery is contemplated.
Bilateral vocal cord paralysis requires emergent intubation or tracheostomy, or both. Injury
to the external branch of the superior laryngeal nerve results in loss of the resonance and
high tones in the voice. Hypoglossal nerve injury results in deviation of the tongue to the
side of the injury; this can result in reduced ability to move food around in the mouth and
drooling. Injury to the marginal mandibular nerve results in pulling of the inferior aspect of
the mouth in a direction away from the injury. In general, hypoglossal and marginal mandib-
ular nerve injuries are temporary.
◆ Patients, particularly those who undergo carotid endarterectomy under general anesthesia,
can experience blood pressure instability after surgery. Most commonly, this is manifested as
hypertension, which can be treated with intravenous medication such as nitroprusside.
Hypotension, which is less common, can be treated with medication such as phenylephrine.
◆ The most feared complication after carotid endarterectomy is stroke, which can occur intra-
operatively or postoperatively. Intraoperative strokes are usually treated with anticoagulant
or antiplatelet therapy postoperatively. Postoperative strokes (in other words, the patient’s
neurologic examination is normal immediately after surgery, but changes within the fi rst
12 to 24 hours) should be treated by emergent return to the operating room because of the
possibility of carotid thrombosis. This can be treated with thrombectomy and possibly
thrombolytic therapy.

918 Section XII • Vascular
STEP 5: PEARLS AND PITFALLS
◆ Injury to the marginal mandibular nerve can be avoided by not retracting the mandible too
strongly.
◆ Division of an unusually large ansa cervicalis crossing anterior to the carotid bifurcation will
usually result in hoarseness. Avoid cutting it if possible.
◆ Because of the risk of infection and carotid rupture, a tracheostomy adjacent to a fresh ca-
rotid endarterectomy is a disaster and should be avoided at all costs.
SELECTED REFERENCES
1. North American Symptomatic Carotid Endarterectomy Trial Collaborators: Benefi t of carotid endarterec-
tomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med 1991;325:445-453.
2. North American Symptomatic Carotid Endarterectomy Trial Collaborators: Benefi t of carotid endarterec-
tomy in patients with symptomatic moderate or severe stenosis. N Engl J Med 1998;339:1415-1425.
3. Executive committee for Asymptomatic Carotid Atherosclerosis Study: Endarterectomy for asymptomatic
carotid artery stenosis. JAMA 1995;273:1421-1428.
4. Ricotta JJ Jr, Malgor RD: A review of the trials comparing endarterectomy and carotid angioplasty and
stenting. Perspect Vasc Surg Endovasc Ther 2008;20:299-308.

919
STEP 1: SURGICAL ANATOMY
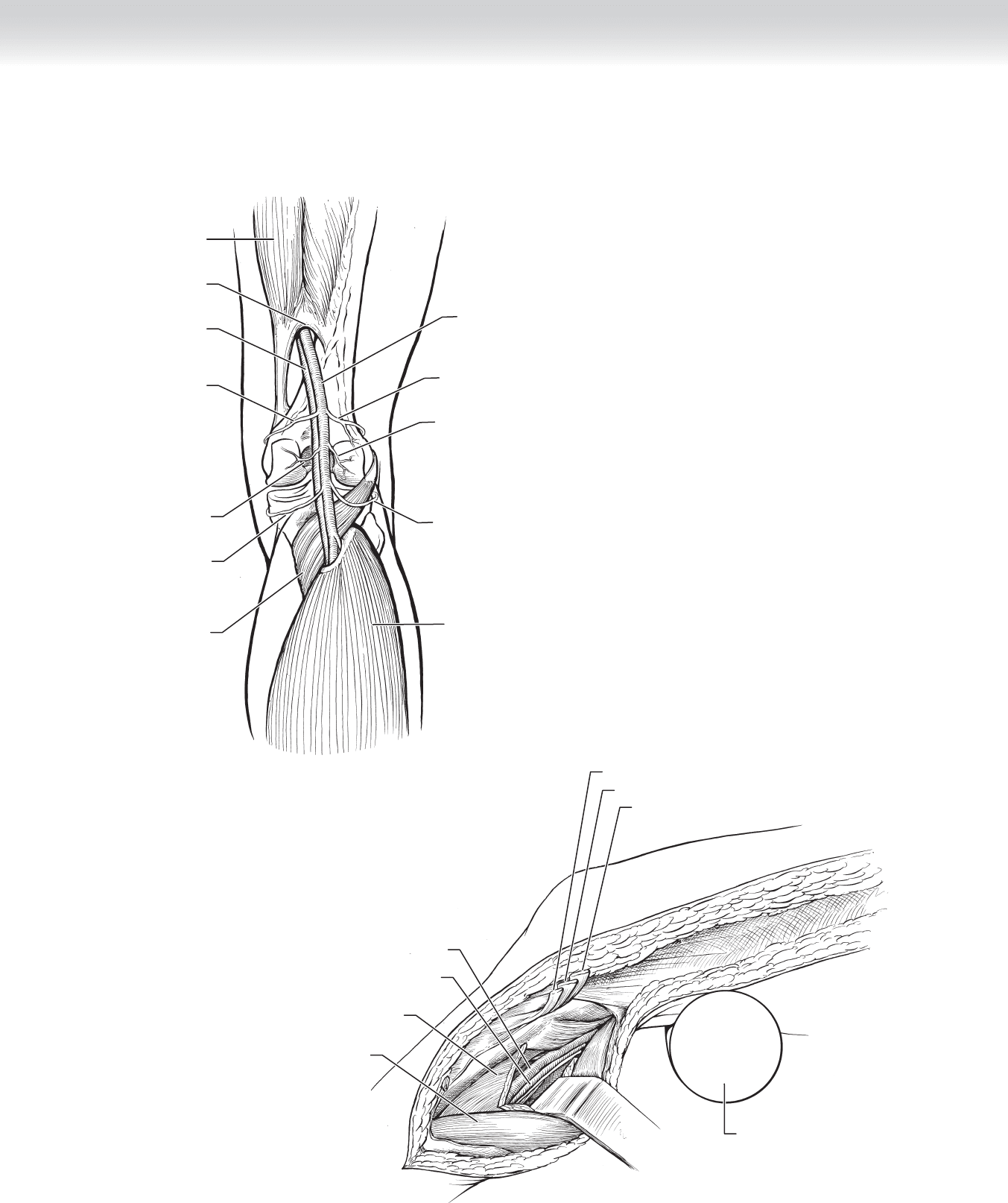
◆ A comprehensive understanding of the anatomy of the leg is essential to performing the
procedure and avoiding future complications. This anatomy includes the femoral triangle
and the popliteal space below the knee. The saphenous vein can have many variations in
its course in the thigh. Identifying the main branch and avoiding a fl ap are key points
(Figures 85-1 through 85-3).
CHAPTER
85
Femoropopliteal Bypass
(In Situ)
Lori Cindrick Pounds
Medial accessory
saphenous vein
Superficial external
pudendal vein
Great
saphenous vein
Sartorius muscle
Femoral vein
Inguinal ligament
Femoral nerve
Femoral triangle
Profunda artery
Femoral artery
Superficial
femoral artery
Anterior lateral accessory
saphenous vein
MC
FIGURE 85 –1
920 Section XII • Vascular
Medial superior
geniculate artery
Popliteal vein
Hunter’s canal
Adductor
magnus muscle
Posterior View
Sural artery
Medial inferior
geniculate artery
Popliteal
muscle
A
Lateral inferior
geniculate artery
Soleus muscle
Popliteal artery
Lateral superior
geniculate artery
Sural artery
B
Popliteal vein
Popliteal artery
Soleus muscle
Medial head
gastrocnemius muscle
Semitendinosus muscle
Gracilis muscle
Sartorius muscle
Round
pillow bump
FIGURE 85 –2