Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

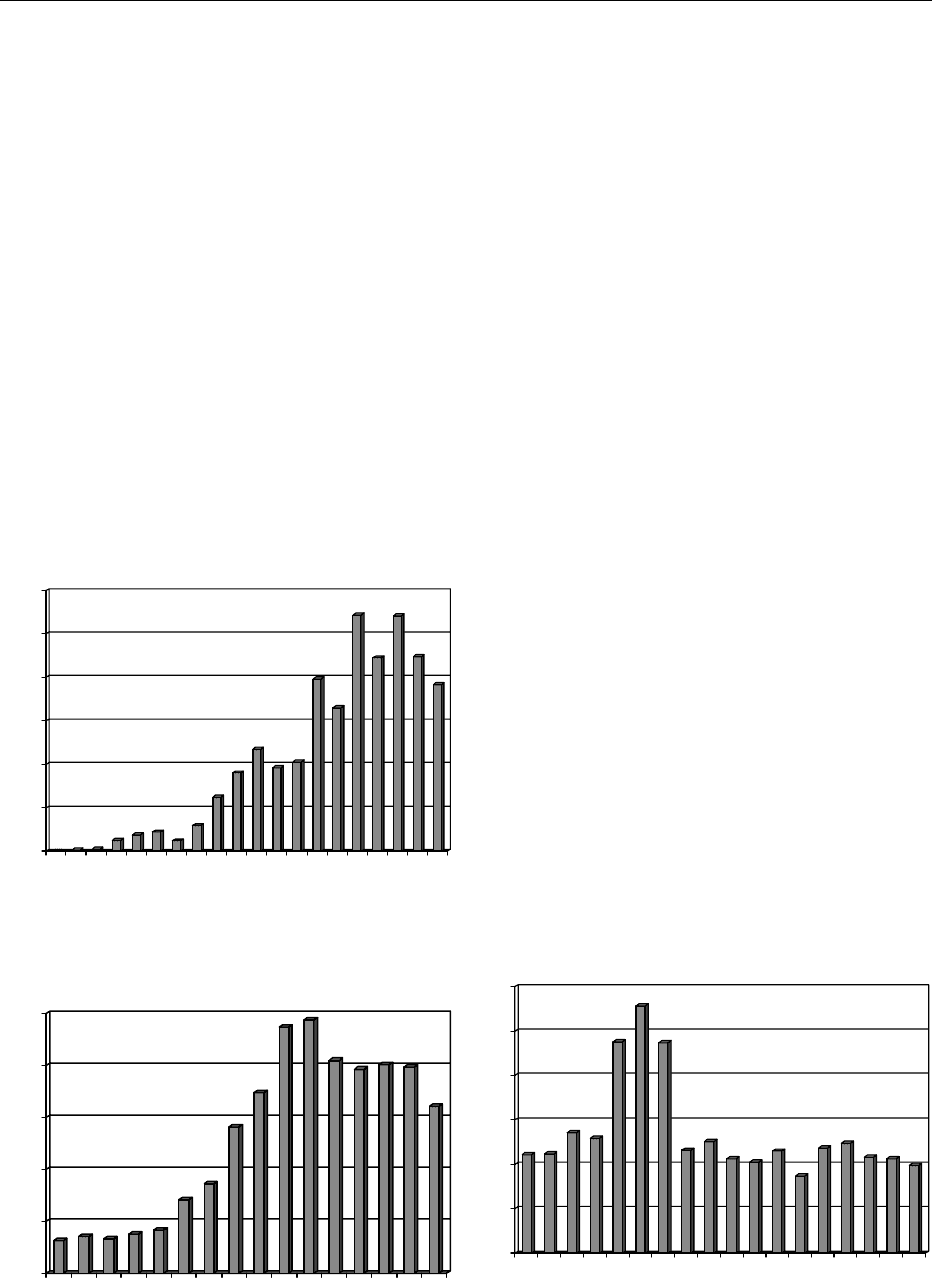
Throughout the 1990s, the annual number of cases in
England and Wales fluctuated, but there is an overall
increasing trend. By 1997, the number of reported
cases was over 1000.
0029 Reports from Scotland are far higher than those
from England and Wales. In part, this may be due to
its higher profile there. For example, in 1989, E. coli
O157 was one of a list of 32 informally selected
organisms which were made ‘reportable infections’
by laboratories in Scotland, in addition to the statu-
torily notifiable diseases, and this coincided with a
doubling (at least) of the recorded incidence in a
12-month period. However, during 1992 and 1993,
and against the background of heightened awareness
and increased screening, the incidence dropped to
about half of the 1991 level (2.3 per 100 000 com-
pared to 4.0 in 1991). The subsequent marked in-
crease, in 1994, also cannot be attributed to changes
in reporting rates or screening, suggesting that
Scotland does have a higher incidence than the rest
of the UK and that there are real significant variations
in the incidence of VTEC from year to year.
0030Figure 5 shows the trends in SRSV infections. Viral
gastroenteritis is much more common than these data
suggest. Most cases are not investigated through la-
boratories. When they are, diagnosis requires electron
microscopy of feces taken within the first hours of the
onset in order to have a high chance of success. Viral
gastroenteritis can be foodborne from contamination
of any food by dirty hands, or airborne contamin-
ation following vomiting or from food contaminated
from sewage such as oysters.
0031Figure 6 shows the laboratory reports of Listeria
infection, which is usually foodborne in origin.
People affected are almost exclusively the elderly,
pregnant women, or immunosuppressed patients.
The peak in cases in 1987–89 coincided with an
outbreak from pa
˚
te
´
produced in Belgium and led to
health advice for the public and considerable work by
the food industry to address the risks from cook-
chilled foods.
The Reporting Pyramid
0032In order to gain a better appreciation of the true
incidence of gastrointestinal infections, a national
study, the Infectious Intestinal Disease (IID) in Eng-
land study, was commissioned by the Department of
Health. This provides the best data to date of the true
incidence of enteric pathogens in the country. The
objectives of the study were: first to estimate the
number, and microbiological causes, of cases of intes-
tinal infectious disease people presenting to their GPs
and from whom stool specimens are routinely sent
for laboratory examination; second, to compare
these data with the data from the national reporting
surveillance system; and third, to estimate the preva-
lence of asymptomatic infection with these agents.
0
200
400
600
800
1000
1200
1982 1985 1988 1991 1994 1997 2000
fig0004 Figure 4 Reports of E. coli O157 in England and Wales.
500
1000
1500
2000
2500
1986 1988 1990 1992 1994 1996 20001998
fig0005 Figure 5 Reports of SRSV infections in England and Wales.
0
50
100
150
200
250
300
1983 1986 1989 1992 1995 1998
fig0006Figure 6 Laboratory reports of Listeria infection in England and
Wales.
2668 FOOD POISONING/Statistics
Seventy practices were selected to be representative of
the socioeconomic characteristics of the area and to
represent an urban and rural mix. Cases of infectious
intestinal disease were defined as persons with loose
stools or significant vomiting lasting less than 2 weeks
in the absence of a known non-infectious cause and
preceded by a symptom-free period of 3 weeks.
Vomiting was considered significant if it occurred
more than once in the 24-h period and if it incapaci-
tated the case or was accompanied by other symptoms
such as cramps or fever. One component of the study
was to draw at random a cohort of people registered
with the 70 GPs, who were followed up for a period of
6 months. These volunteers agreed to fill out diary
cards every week and return them to the GPs. These
cards stated whether the person had suffered gastro-
intestinal (GI) illness or not. If someone developed an
illness, a stool sample was submitted.
0033 Of particular interest in this study was the estimate
of the carriage of potential pathogens in otherwise
healthy people. Ten out of 2264 controls (0.4%) were
found to be excreting Salmonella, 16 out of 2264
(0.7%) were excreting Campylobacter, but none out
of 2264 were excreting E. coli 0157. These data
confirm that VTEC is a rare infection in this country
at the moment.
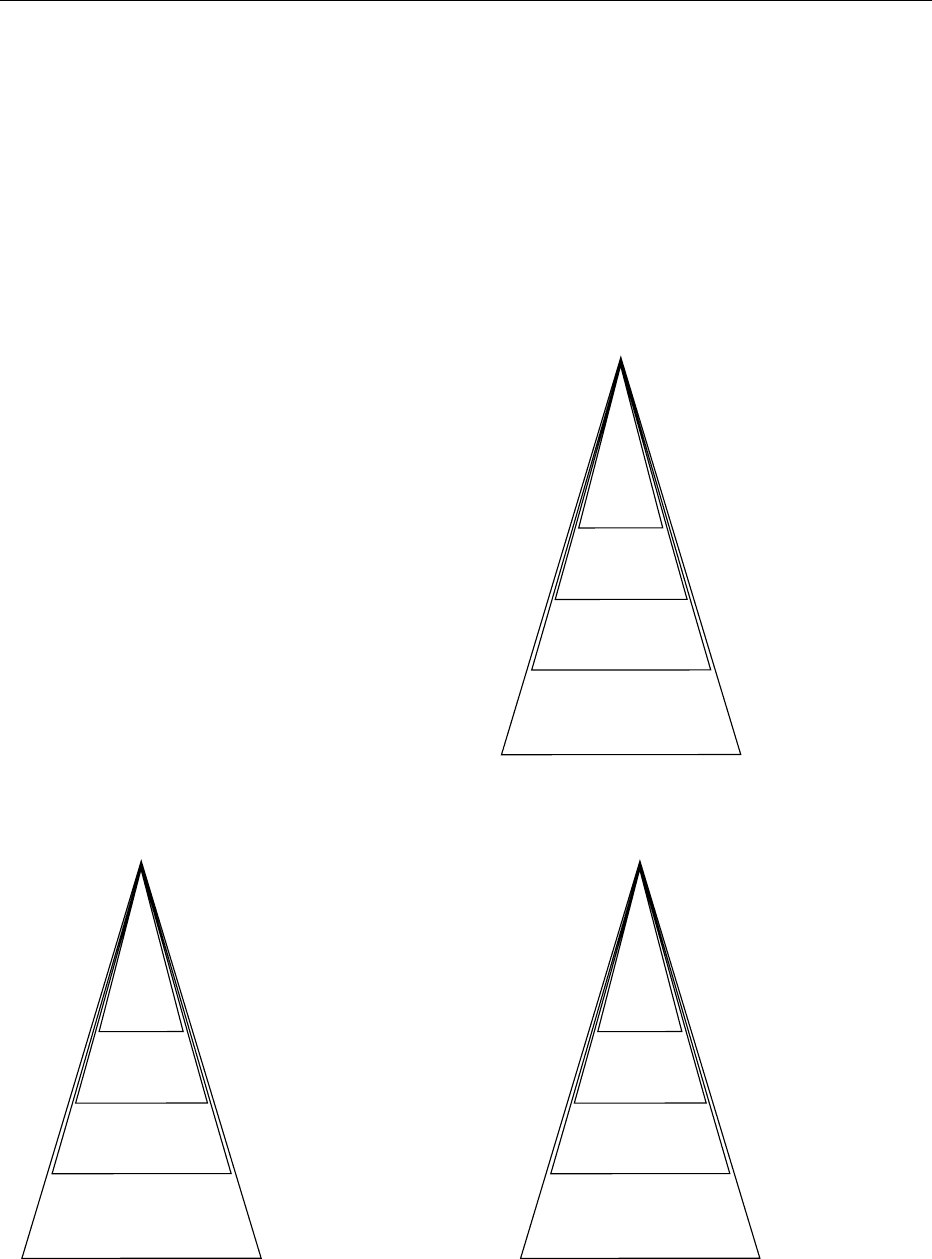
0034 The IID study was able to quantify the reporting
pyramid referred to above using the cohort compon-
ent of the study. For all IIDs, it was estimated that for
every case reported to the CDSC, six patients were
investigated by routine laboratory tests, 23 presented
with GI symptoms to their GP, and there were 136
actual cases in the community. For Salmonella cases,
however, the ratios were much smaller. For every case
reported to CDSC, it was estimated that there were
2.3 cases presenting to their GP and 3.2 actual cases
in the community (see Figures 7 and 8).
Outbreak Reports
0035In addition to the reporting of individual cases, na-
tional surveillance centers receive reports of food-
borne disease outbreaks. A general outbreak is
Reported to CDSC
1
2.3
(1.4−4.3)
3.2
(14−12.0)
1.2
(1.0−1.7)
1
3.6
(2.4−5.8)
7.6
(3.6−17.4)
1.5
(1.2−2.0)
Positive by routine
laboratory investigation
Presenting to the GP
Community case
(a) (b)
Reported to CDSC
Positive by routine
laboratory investigation
Presenting to the GP
Community case
fig0007 Figure 7 Reporting pyramids for (a) Salmonella and (b) Campylobacter.
Reported to CDSC
1
248
(30−2,026)
1,562
(140−17,424)
1.4
(1.3−1.6)
Positive by routine
laboratory investigation
Presenting to the GP
Community case
fig0008Figure 8 Reporting pyramid for SRSV.
FOOD POISONING/Statistics 2669
defined as ‘affecting members of more than one
private residence or residence of an institution.’ Gen-
eral outbreaks are distinguished from family out-
breaks affecting members of the same private
residence only. In 1992, an improved systematic sur-
veillance system for outbreaks was developed by the
PHLS in England and Wales in response to the Rich-
mond’s Committee recommendations. The CDSC is
made aware of outbreaks from laboratory reports,
consultants in communicable disease control, envir-
onmental health officers, and others. Outbreaks are
then followed up using a standard request form that
documents basic details. Participation in the surveil-
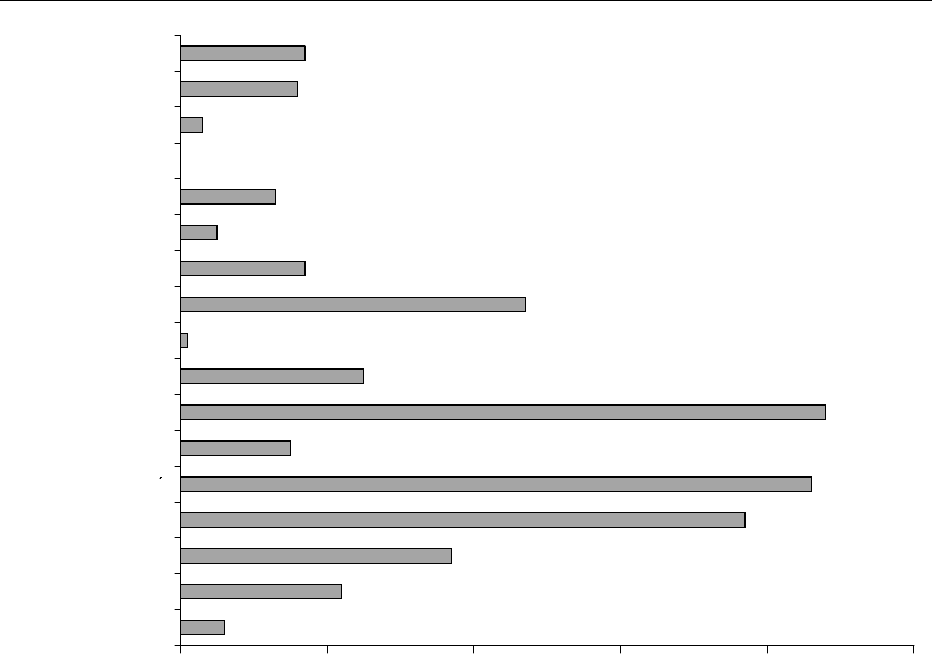
lance scheme is entirely voluntary. Figure 9 shows the
number of outbreaks of Salmonella enteritidis PT4 in
England and Wales for 1992–97.
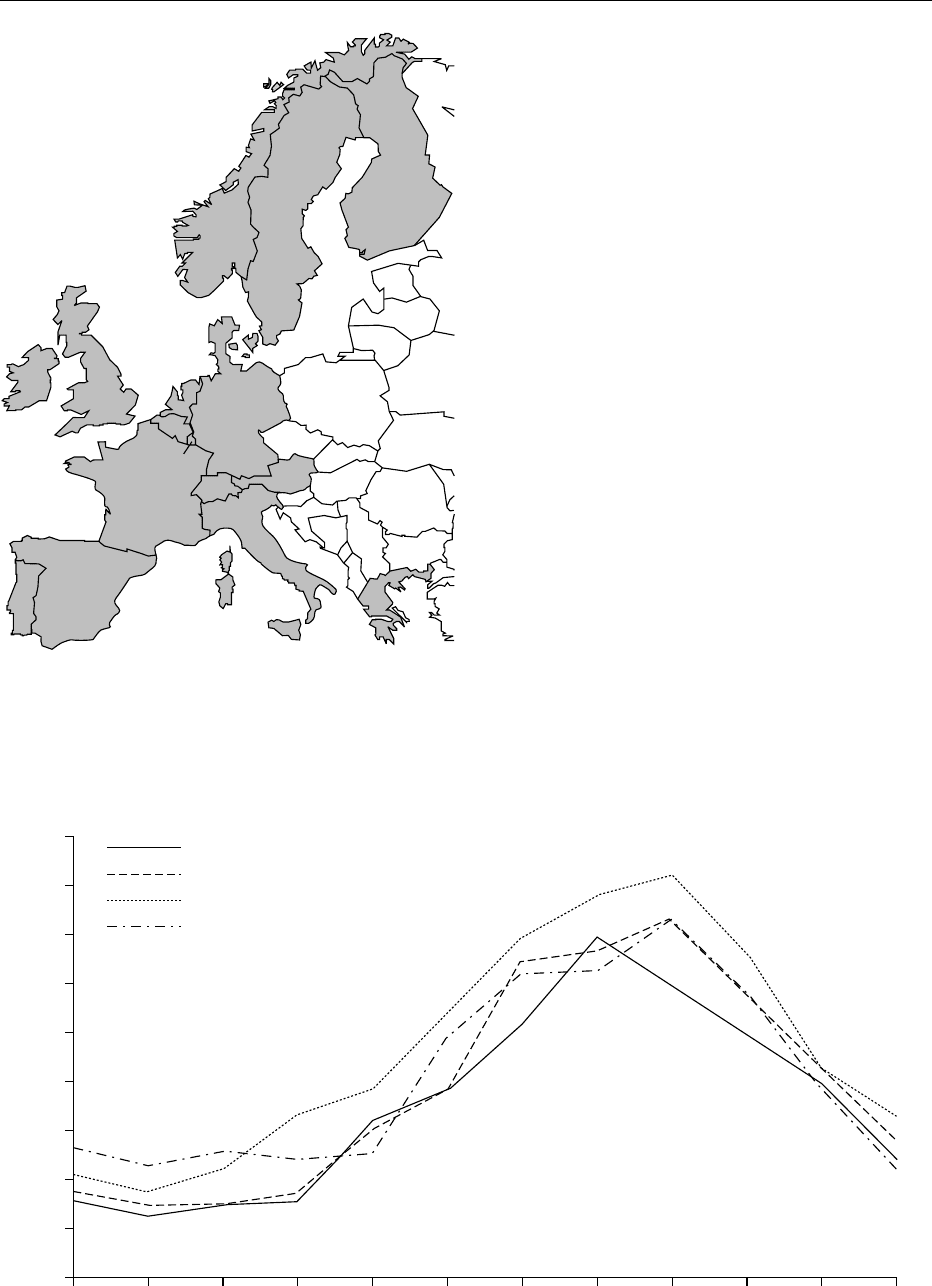
Enter-net
0036 An international surveillance network (Enter-net) for
human gastrointestinal infections involving 15 coun-
tries of the European Union and the USA has been set
up (see Figure 10). The aim of the network is to
conduct international surveillance of human salmon-
ellosis and verocytotoxin producing E. coli 0157.
This project began first of all with Salmonella cases
in 1994 and was funded by the EU. The network
consisted of the microbiologists in charge of the na-
tional reference laboratories in participating coun-
tries and epidemiologists responsible for national
surveillance. The minimum dataset is collected for
each isolate and reported to a central unit.
0037A dynamic database has been created, which shows
that trends in salmonellosis declined throughout
Western Europe from 1996 (see Figure 11). As a result
of this network, international outbreaks were recog-
nized. Individual countries identifying apparently
isolated incidents were linked together to identify
wider outbreaks. One of these outbreaks involved
12 cases of E. coli 0157 in Denmark, England,
Wales, Finland, and Sweden in visitors to Fuerterven-
tura in the Canary Islands.
Other Sources of Statistics
Registrations of Deaths
0038Most countries have statutory deaths registrations
systems that seek to record the causes of death.
These are of limited use in foodborne diseases, since
University/College
0 20406080100
Shop
School
Residential Institution
Pub
Private house
Other
Mobile Retailer
Hotel/Guest House
Hospital
Holiday Camp
Hall
Farm
Community
Canteen
Armed Services Camp
Restaurant/Cafe
fig0009 Figure 9 Salmonella enteritidis PT4 outbreaks in England and Wales, by place of outbreak, from 1992 to 1997.
2670 FOOD POISONING/Statistics
such diseases rarely are primary causes of death, and
even when they are contributory causes, the registra-
tion data may not systematically record this.
Hospital Admissions Data
0039Many countries have statistics on the numbers of
patients admitted or discharged from hospital by dis-
ease. Once again, these data are of very limited use in
developed countries, since foodborne disease rarely
causes admission to hospital. Even when it does, the
microbiological causes may not be recorded.
Clinical Reporting Networks
0040When a new foodborne disease emerges, special
reporting systems may be set up, such as the UK
collaborative study of childhood hemolytic uremic
syndrome (HUS), which began at the end of February
1997 and is conducted by the British Pediatric Sur-
veillance Unit (BPJU), the PHLS, Scottish Centre for
Infection and Environmental Health (SCIEH) and the
Scottish 0157 Reference Laboratory. Pediatricians
report cases of clinically diagnosed HUS directly to
the PHLS, CDSC, or SCIEH by telephone at the time
of the diagnosis and also follow this up with a stand-
ard report card to the BPSU. Clinical and epidemi-
ological data are collected directly from pediatricians.
Routine feces and serum samples are sent for stand-
ard examination and isolation and subtyping of
VTEC. During the first two years of the study, data
January
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
1995
1996
1997
1998
February March April May June July
Number of cases
August September October November December
fig0011 Figure 11 Salmonella enteritidis cases in Western Europe from 1995 to 1998.
fig0010 Figure 10 Enter-net participating countries.
FOOD POISONING/Statistics 2671
were collected from 193 clinically confirmed cases,
and five children were reported to have died. One
hundred and eighty-six cases presented with a diar-
rheal illness, and 156 of these suffered bloody diar-
rhea. Stool and/or serum specimens were obtained
from 185 cases, and of these, 165 were shown to
have suffered VTEC infection.
See also: Campylobacter: Properties and Occurrence;
Escherichia coli: Food Poisoning; Food Poisoning:
Tracing Origins and Testing; Listeria: Properties and
Occurrence; Salmonella: Properties and Occurrence
Further Reading
Adak GK, Long SM and O’Brien SJ (2002) Trends in indi-
genous foodborne disease and deaths, England and
Wales: 1992 to 2000. Gut 51(6): 832–841.
Advisory Committee on the Microbiological Safety of Food
(2001) Second Report on Salmonella in Eggs. London:
The Stationery Office.
Berkelman RL, Stroup DF and Buehler JW (2002) Public
Health Surveillance. In: Detels J, McEwen J, Beaglehole
R and Tanaka H (eds) Oxford Textbook of Public
Health. The Scope of Public Health, Vol. 1, 4th edn.,
pp. 759–781. Oxford University Press.
Cowden JM (2002) Foodborne infectious risks: do we need
a wide system of data collection and survey? The lessons
learned from the study of infectious intestinal disease in
England. Rev Epidemiol Sante Publique 50(1): 89–92.
Fisher IS and Gill ON (2001) International surveillance
networks and principles of collaboration. European
Surveillance 6(2): 17–21.
Food Standards Agency (2000) A Report of the Study of
Infectious Intestinal Disease in England. London: The
Stationery Office.
Frost JA, Gillespie IA and O’Brien SJ (2002) Public health
implications of campylobacter outbreaks in England and
Wales, 1995–1999: epidemiological and microbiological
investigations. Epidemiology and Infection 128(2):
111–118.
Herikstad H, Yang S, Van Gilder TJ et al. (2002) A popula-
tion based estimate of the burden of diarrhoeal illness in
the United States: FoodNet, 1996–97. Epidemiology and
Infection 129(1): 9–17.
Palmer SR, Parry S, Perry D et al. (2000) The role of
outbreaks in developing food safety policy: population
based surveillance of salmonella outbreaks in Wales
1986–1998. Epidemiology and Infection 125(3): 467–
472.
Parry SM and Palmer SR (2002) E. coli. Environmental
Health Issues of VTEC 0157. Clay’s Library of Health
and the Environment. Spon Press.
Economic Implications
R B Raybourne and K M Williams, Center for Food
Safety and Applied Nutrition, Laurel, MD, USA
T Roberts, Economic Research Service, Washington,
DC, USA
Arthritis Working Group
1
,
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001Foodborne diseases are caused by ingesting bacteria,
fungi, parasites, viruses or their toxic metabolites
through contaminated food or water or through
person-to-person contact. Each year, microbial
pathogens cause an estimated 76 million cases of
foodborne illness, including 5200 deaths in the USA,
according to the study by Mead et al. at the Centers
for Disease Control and Prevention (CDC). The Eco-
nomic Research Service (ERS) in the United States
Department of Agriculture and the Center for Food
Safety and Applied Nutrition (CFSAN) in the Food
and Drug Administration have estimated the annual
human illness costs for a number of causes of food-
borne illness. The ERS estimates that the total cost of
five major bacterial pathogens is $6.9 billion annu-
ally. CFSAN estimates a cost of $27.9 billion for nine
major causes of foodborne illness. In their estimates
for human foodborne illness costs, both ERS and
CFSAN include medical costs, productivity losses
from missed work, and an estimate of the value of
premature deaths. CFSAN also includes an estimate
of the cost of pain and suffering due to illness.
0002The vast majority of foodborne illnesses are classi-
fied as ‘acute.’ These are usually self-limiting and
of short duration, although the cases can range
from mild to severe. Gastrointestinal problems and
vomiting are common acute symptoms of many food-
borne illnesses. Deaths from acute foodborne illness,
while rare, are more likely to occur in the very
young (including the fetus), the elderly, or patients
with compromised immune systems (such as those
suffering from AIDS and cancer).
1
The other participants in the Arthritis Working Group of the Risk
Assessment Consortium (RAC) are: ERS – P Frenzen; Centers for Disease
Control and Prevention – J Sobel and S O’ Connor; and Food and Drug
Administration – A Jessup, C McGlaughlin, C Nardinelli, and R Scharff. The
RAC’s members are United States government agencies with food safety
research and management responsibilities. The RAC enhances
communication and coordination among the member agencies and promotes
the conduct of scientific research that facilitates risk assessments. The RAC’s
web page is: http://www.foodriskclearing house.umd.edu/
Risk_Assessment_Consortium.htm.
2672 FOOD POISONING/Economic Implications

0003 Complications of foodborne illness, called chronic
sequelae, can occur in any part of the body including
the joints, nervous system, kidneys, or heart. These
chronic illnesses may afflict the patients for the
remainder of their lives or result in premature death.
For example, Campylobacter infections are estimated
to be responsible for 20–40% of Guillain–Barre
´
syn-
drome (GBS) cases (a major cause of paralysis unre-
lated to trauma) in the USA. About 1.5% of E. coli
O157:H7 disease patients develop hemolytic uremic
syndrome (HUS), which usually involves red blood
cell destruction, kidney failure, and neurological
complications, such as seizures and strokes.
0004 We will focus on a group of chronic sequelae of
foodborne infections composed of reactive arthritis,
Reiter’s syndrome, and ankylosing spondylitis, known
collectively as the spondyloathropathies. We will use
these chronic sequelae as an in depth example of how
cost estimates are developed. These arthritis-like con-
ditions occur in the aftermath of acute infection with
several genera of Gram-negative Enterobacteriaceae
including Salmonella spp., and all involve at a min-
imum some form of joint inflammation. The reported
incidence of postacute joint inflammation can vary
widely. The degree of severity and duration of arthritis
is also highly variable. However, in the most severe
or chronic cases, the consequences may be life-long,
and there is potential to significantly increase the
economic impact beyond the initial cost of acute
foodborne illness.
Exposure to Pathogens and Associated
Costs
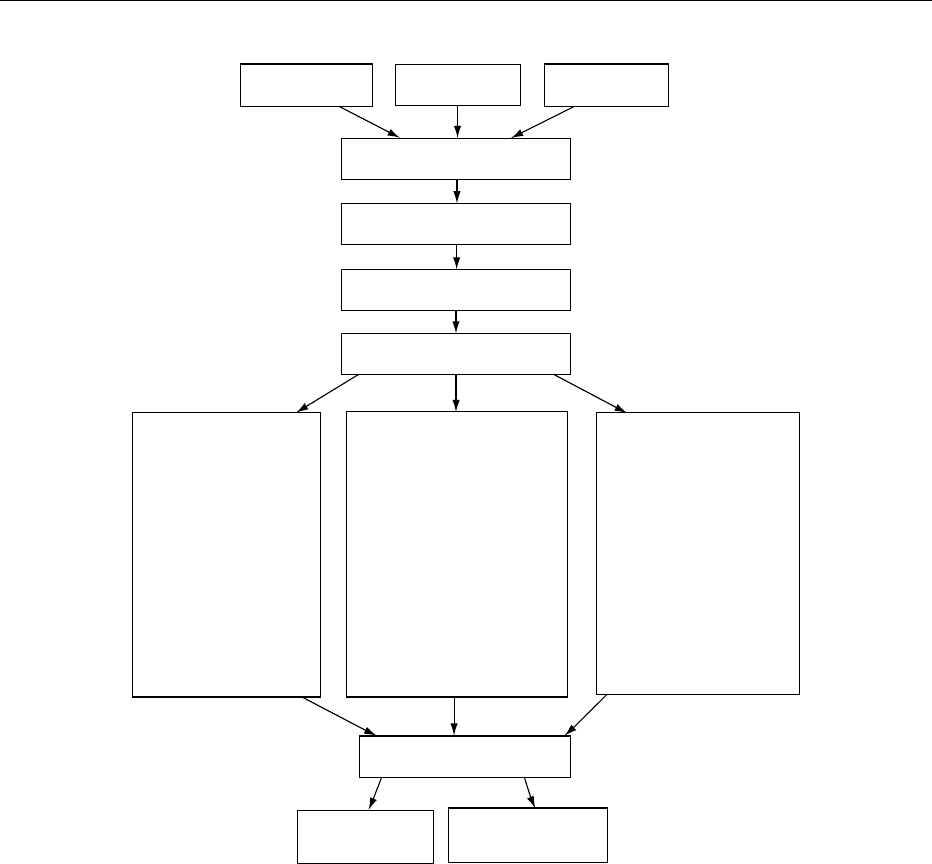
0005 Actions by the food industry, consumers, and the
public health sector all influence how food is pro-
duced, marketed, prepared, and consumed. These
actions influence the probability that a food item
contains pathogens. People who consume contamin-
ated food have some probability of becoming ill.
Foodborne illness generates costs that are borne by
the food industry, households whose members become
ill, and/or the public health sector (Figure 1). A full
accounting of the costs of all sectors of the economy
would include estimates for all the costs listed in
Table 1. Depending on the purpose of the study,
different cost categories can be selected, though
medical costs are those most commonly estimated.
Cost Estimates for Foodborne Disease
0006 The Centers for Disease Control and Prevention esti-
mates that out of a total of 76 million cases of food-
borne illness each year in the USA, as many as 62
million cases are of unknown origin. Thus, in 82% of
cases of foodborne illness, the disease or agent has not
been identified, and costs have not been estimated.
ERS and CFSAN have estimated costs for the most
common identifiable causes of foodborne illness. As
the pioneer of cost estimates for US foodborne illness,
ERS has estimated costs for five common foodborne
pathogens, likely to be associated with meat and
poultry. As the agency with the responsibility for
regulating the safety of the most food groups, CFSAN
has estimated the cost of almost 20 causes of food-
borne illness. Table 2 illustrates the estimated costs of
the most common foodborne illnesses that have been
studied by the two agencies.
0007For each agent or disease that causes foodborne
illness, ERS and CFSAN estimate an annual cost of
illness based on the estimated number of cases, the
expected severity of illness, and whether we expect an
acute illness to result in chronic sequelae. Estimated
costs include medical costs, lost productivity costs,
other illness-specific costs (such as special education
and residential-care costs), and an estimate of the
value of premature deaths. CFSAN also measures
quality-adjusted life year (QALY) losses to value the
pain and suffering associated with foodborne illness.
Costs have not been estimated for the vast majority of
complications associated with foodborne illnesses.
The cost estimates do, however, cover the following
chronic complications in our cost estimates: paralysis
following Campylobacter spp. infections (called the
Guillian-Barre
´
Syndrome), kidney failure following
E. coli O157:H7 infections (HUS), and chronic dis-
ability or impairment following congenital and new-
born infections from Listeria monocytogenes.
CFSAN estimates also include costs for arthritic com-
plications that result from illnesses due to Salmonella
spp. and Shigella spp.
0008Medical costs ERS and CFSAN use similar methods
to estimate medical costs. Disease-outcome trees are
developed for each illness to put the medical data in
perspective. The total number of cases are divided
into different levels of severity of disease:
.
0009cases who recover without seeking medical care,
.
0010cases who visit a physician and recover,
.
0011cases who are hospitalized and recover,
.
0012cases who develop chronic complications (can
overlap with an acute survivor category), and
.
0013those who die prematurely because of their illness.
For the different severity groups, the percentage re-
covering fully, partially recovering, or dying prema-
turely is estimated and entered into the disease
outcome tree. (The disease outcome tree approach
will be illustrated later when discussing the medical
evidence connecting foodborne illness to arthritis.)
Medical costs are estimated for physician and
FOOD POISONING/Economic Implications 2673
hospital services, supplies, medications, and special
procedures unique to treating the particular food-
borne illnesses. Such costs reflect the average number
of days or treatments of a medical service, the average
cost per service or treatment in the USA, and the
number of patients receiving such service or treat-
ment.
0014 ERS estimates of nonmedical costs For the 2000
cost estimates, ERS revised the methodology for
valuing premature deaths due to foodborne illness.
ERS previously assigned all deaths the same value
regardless of age at time of death, based on infor-
mation about the wage premiums for high-risk occu-
pations (the ‘labor market approach’). Now, the
updated cost estimates use information about the
age distribution of deaths to adjust this value to
account for age at death.
0015In essence, the labor market approach values the
economic cost of premature deaths based on the risk
premium revealed by the higher wages paid for dan-
gerous jobs. Under this approach, the value of a stat-
istical life equals $6.5 million in August 2000 dollars
after updating Viscusi’s original 1990 estimate of
$5.0 million to account for inflation. The labor
market approach assumes that risk preferences
observed in job choices are indicative of risk prefer-
ences for food safety.
0016ERS modified the labor market approach by taking
the age distribution of deaths from each pathogen
Foodborne disease, exposure, and types of costs
Food production,
marketing and preparation
Food industry
production
Household
production
Public health
regulations
Presence of a
hazard in food
Incidence of damage
Exposure to a hazard
via consumption of food
Food industry
Product recall
Plant closings
and cleanup
Product liability cost
Reduced product
demand
Insurance
administration
Households
Estimates of the value
of premature death
Medical cost
Income or productivity
loss
Pain and suffering
Leisure time cost
Child care cost
Risk aversion cost
Travel cost
Self protection costs
Home modifications
Vocational and
physical rehabilitation
Public health sector
Disease surveillance
cost
Cost of investigating
outbreak
Cost of cleanup
Public education
Implementation of
HACCP systems
Cost of damage
Monetizable
cost
Nonmonetizable
cost
fig0001 Figure 1 Foodborne disease, exposure, and types of costs.
2674 FOOD POISONING/Economic Implications

into account, in effect treating the value of life as an
annuity paid over the average US life span at an
interest rate of 3.0%. Following age adjustment, the
assumed cost of each death ranges from $8.9 million
for individuals who died before their first birthday to
$1.7 million for individuals who died at age 85 or
older.
0017Since the five microbial pathogens have different
health outcomes for different age groups, adjusting
for the age of death raises the cost of some foodborne
illnesses and lowers the cost of others. For example,
the annual cost of foodborne illness caused by Sal-
monella spp. decreases to $2.2 billion, because over
two-thirds of the deaths from salmonellosis occur
among people over 65 years of age. Adjusting food-
borne illness costs for E. coli O157:H7 by age at time
of death increases the estimates by $200 million, be-
cause most deaths are children under the age of five.
tbl0001 Table 1 Social costs of foodborne illness
Costs to individuals/households
Human illness costs:
Medical costs:
Physician visits
Laboratory costs
Hospitalization or nursing home
Drugs and other medications
Ambulance or other travel costs
Income or productivity loss for:
Ill person or fatal case
Caregiver for ill person
Other illness costs:
Travel costs to visit ill person
Home modifications
Vocational/physical rehabilitation
Child care costs
Special educational programs
Institutional care
Lost leisure time
Psychological costs:
Pain and other psychological costs
Risk aversion
Averting behavior costs:
Extra cleaning/cooking time costs
Extra cost of refrigerator, freezer, etc.
Flavor changes from traditional recipes (especially
meat, milk, egg dishes)
Increased food cost when more expensive but safer
foods are purchased
Altruism (willingness to pay for others to avoid illness)
Industry costs
Impact of pathogens on animal production costs:
Morbidity and mortality of animals on farms
Reduced growth rate/feed efficiency and increased time to
market
Costs of disposal of contaminated animals on farm and at
slaughterhouse
Increased trimming or reworking at slaughterhouse and
processing plant
Lost productivity due to illness among workers caused by
handling contaminated animals or products
Increased meat product spoilage due to pathogen
contamination
Control costs for pathogens at all links in the food chain
a
:
New farm practices (age segregated housing, sterilized
feed, etc.)
Altered animal transport and marketing patterns (animal
identification systems, feeding/watering)
New slaughterhouse procedures (hide wash, knife
sterilization, carcass sterilizing)
New processing procedures (pathogen tests, contract
purchasing requirements)
Altered product transport (increased use of time/
temperature indicators)
New wholesale/retail practices (pathogen tests, employee
training, procedures)
Risk assessment modelling by industry for all links in the
food chain
Price incentives for pathogen-reduced product at each link in
the food chain
Outbreak costs:
Herd slaughter/product recall
Plant closings and cleanup
Regulatory fines
Product liability suits from consumers and other firms
b
Reduced product demand because of outbreak:
Generic animal product – all firms affected
Reduction for specific firm at wholesale or retail level
Increased advertising or consumer assurances following
outbreak
Impact of outbreaks on tourism industry
Regulatory and public health sector costs for foodborne pathogens
Disease surveillance costs to:
Monitor incidence/severity of human disease by foodborne
pathogens
Monitor pathogen incidence in the food chain
Develop integrated database from farm to table for
foodborne pathogens
Research to:
Identify new foodborne pathogens for acute and chronic
human illnesses
Establish high-risk products and production and
consumption practices
Identify which consumers are at high-risk for which
pathogens
Develop cheaper and faster pathogen tests
Risk assessment modelling for all links in the food chain
Outbreak costs:
Costs of investigating outbreak
Testing to contain an outbreak (for example, serum testing
and administration of IG in persons exposed to
Hepatitis A)
Costs of cleanup
Legal suits to enforce regulations that may have been
violated
b
Other considerations
Distributional effects in different regions, industries, etc.
Equity considerations, such as special concern for children
a
Some industry costs may fall with better pathogen control, such as
reduced product spoilage, possible increases in product shelf-life, and
extended shelf-life permitting shipment to more distant markets or
lowering shipment costs to nearby markets.
b
In adding up costs, care must be taken to assure that product liability
costs to firms are not already counted in the estimated pain and suffering
cost to individuals. However, the legal and court expenses incurred by all
parties are social costs.
FOOD POISONING/Economic Implications 2675
0018 One difficult issue is assigning a value to the
productivity losses associated with individuals who
become ill and are unable to return to work, or for
those illnesses that result in a lifetime of disability
(such as prenatal exposure to Listeria monocyto-
genes). ERS currently measures the productivity
losses due to nonfatal foodborne illness by the value
of forgone or lost wages, regardless of whether the
lost wages involved a few days missed from work or a
permanent disability that prevented an individual
from returning to work. Using the value of lost
wages for cases resulting in disability probably under-
states an individual’s willingness to pay to avoid dis-
ability because it does not account for the value
placed on avoiding pain and suffering. The willing-
ness to pay measure derived from labor market stud-
ies that ERS uses to value a premature death is not an
appropriate measure of willingness to pay to avoid
disability because it measures the higher wages paid
to workers to accept a higher risk of premature death,
not disability. Methods have been suggested to adjust
willingness to pay to reduce the risk of premature
death downward to estimate willingness to pay to
avoid disability, such as the approach based on meas-
uring QALYs. As yet, there is no consensus among
economists about how to use these methods to value
willingness to pay to avoid the disability, pain, and
suffering associated with foodborne illnesses. ERS’s
conservative estimates of the annual costs due to
foodborne illness (particularly the chronic conditions
associated with Campylobacter spp.) would be
substantially increased if willingness to pay to avoid
disability, pain, and suffering were also taken into
account.
0019CFSAN estimates of nonmedical costs Medical
costs are a small fraction of the total social cost of
foodborne illness. In addition to the cost of medical
care, economists are concerned with the loss of prod-
uctivity and the loss of well-being (through pain and
suffering) that accompany foodborne illness. CFSAN
routinely estimates these nonmedical costs of food-
borne illness.
0020CFSAN was one of the first government agencies to
use the labor market approach to estimating the eco-
nomic cost of premature death. Economists have long
favored this method, because it is based on observed
tradeoffs that individuals make between dollars and
risk. An unadjusted figure of $5.0 million per prema-
ture death is generally used in CFSAN analyses. As
noted above, this value does not take into account
economic changes that have occurred since 1990.
tbl0002 Table 2 Economic costs of foodborne illness in the USA: estimated annual costs due to selected US foodborne pathogens, 2000
a
Pathogen Estimatedannual foodborne illnesses
b
ERS costs
c
CFSANcosts
d
Cases Hospitalizations Deaths Billion 200 0 dollars
Bacterial infections
Campylobacter spp. 1 963 141 10 539 99 1.2 –
Salmonella 1 341 873 15 608 553 2.4 17.2
Clostridium perfringens 248 520 41 7 – 0.2
Shigella 89 648 1 246 14 – 0.3
E. coli O157:H7 62 458 1 843 52 0.7 2.2
E. coli, non-O157 STEC
e
31 229 921 26 0.3 –
Listeria monocytogenes 2 493 2 298 499 2.3 2.5
Parasitic infections
Giardia lamblia 200 000 500 1 – 0.2
Cryptosporidium parvum 30 000 199 7 – 0.1
Viral infections
Norwalk-like viruses 9 200 000 20 000 124 – 5.3
Hepatitis A 4 170 90 4 – 0.1
To t a l s
ERS total 3 401 194 31 209 1 229 6.9 –
CFSAN total 11 179 162 41 825 1 261 – 28.1
a
As these new estimates of foodborne illness costs are based on new data and improved methodologies for valuing these costs, the estimates presented
here are not directly comparable with earlier ERS and CFSAN estimates of the costs of foodborne disease.
b
Data from the Centers for Disease Control and Prevention published in Mead PS, Slutsker L, Dietz V et al. (1999) Food-related illness and death in the
United States. Emerging Infectious Diseases 5: 607–625.
c
The ERS total estimated costs include specific chronic complications in the case of Campylobacter (Guillain–Barre
´
syndrome), E. coli O157:H7 (hemolytic
uremic syndrome), and Listeria monocytogenes (congenital and newborn infections resulting in chronic disability or impairment). Estimated costs for
Listeria monocytogenes exclude less serious cases that do not require hospitalization.
d
The CFSAN total estimated costs include specific chronic complications in the case of Salmonella (arthritic conditions), Shigella (arthritic conditions and
hemolytic uremic syndrome), and E. coli O157:H7 (hemolytic uremic syndrome). CFSAN uses QALYs to estimate the value of pain and suffereing.
e
STEC stands for Shiga toxin-producing E. coli .
2676 FOOD POISONING/Economic Implications
Economists at CFSAN are currently working on an
adjustment factor based on both nominal and real
changes in society’s valuation of health. As a result,
the figures that are reported in Table 2 are likely to
be an underestimate of the true value of foodborne
illness.
0021 The value of productivity losses and pain and
suffering are measured by placing values on quality
adjusted life years (QALYs). This method uses a two-
step procedure for valuing health losses. In the first
step, the effect of a condition on health is estimated to
be between zero (well-being in the full health state)
and one (death). For example, a QALY loss of 0.14
for arthritis means that for every day of suffering with
arthritis, the affected individual has a level of well-
being 14% lower than they would have had in the
absence of arthritis. In the next step, the value of a
QALY is estimated and multiplied by expected QALY
losses to calculate the value of health losses. QALYs
are designed to measure the loss of well-being both
from symptoms and from activity limitation. Conse-
quently, both pain and suffering and productivity
values are captured by this measure.
0022 ERS and CFSAN use different methods of measur-
ing the nonmedical costs of illness. The net effect of
the differing approaches is that CFSAN estimates for
the value of foodborne illness include a value for pain
and suffering, whereas ERS estimates do not. The
inclusion of a value for pain and suffering is demon-
strated in Table 2. CFSAN estimates of the cost of
foodborne illness are uniformly larger than estimates
made by ERS. In the case of E. coli O157, CFSAN
based its medical cost estimates on estimates calcu-
lated by ERS. Nonetheless, the inclusion of QALY
losses boosts CFSAN estimates of economic loss due
to E. coli O157 to $2.2 billion, as opposed to $0.7
billion for ERS.
Chronic Sequelae of Foodborne Illness
0023A listing of the association of foodborne pathogens
with chronic sequelae (Table 3) illustrates that many
or most of these agents are associated with some type
of complication. Of particular interest is the fact that
several bacterial pathogens are associated with arth-
ritic sequelae. In addition to identifying the various
disease conditions, determining the economic impact
of chronic sequelae associated with foodborne illness
requires not only a systematic method of estimating
costs but also some understanding of the clinical
aspects of these entities. This is particularly
true with respect to the degree of variation that may
tbl0003 Table 3 Chronic complications associated with foodborne pathogens
Bacterialand parasiticinfection transmittedby foods Complications/sequelae
Bacterial infections
Aeromonas hydrophila enteritis Bronchopneumonia, cholecystitis
Brucellosis Aortitis, epididymo-orchitis, meningitis, pericarditis, spondylitis
Campylobacteriosis Arthritis, carditis, cholecystitis, colitis, endocarditis, erythema nodosum, Guillain–
Barre
´
syndrome, hemolytic uremic syndrome, meningitis, pancreatitis,
septicemia
Escherichia coli (EHEC-types) enteritis Erythema nodosum, hemolytic uremic syndrome, seronegative arthropathy,
thrombotic thrombocytopenic purpura
Q-fever Endocarditis, granulomatous hepatitis
Salmonellosis Aortitis, cholecystitis, colitis, endocarditis, epididymo-orchitis, meningitis,
myocarditis, osteomyelitis, pancreatitis, Reiter’s disease, rheumatoid
syndromes, septicemia, splenic abscesses, thyroiditis, septic arthritis
(sickle-cell anemic persons)
Shigellosis Erythema nodosum, hemolytic-uremic syndrome, peripheral neuropathy,
pneumonia, Reiter’s disease, septicemia, splenic abscesses, synovitis
Vibrio parahaemolyticus enteritis Septicemia
Yersiniosis Arthritis, cholangitis, erythema nodosum, liver and splenic abscesses,
lymphadenitis, pneumonia, pyomyositis, Reiter’s disease, septicemia,
spondylitis, Still’s disease
Parasitic infections
Cryptosporidiosis
b
Severe diarrhea, prolonged and sometimes fatal
Giardiasis
b
Cholangitis, dystrophy, joint symptoms, lymphoidal hyperplasia
Taeniasis Arthritis, cysticercosis (T. solium)
Toxoplasmosis Encephalitis and other central nervous system diseases, pancarditis, polymyositis
Trichinosis Cardiac dysfunction, neurologic sequelae
a
Suspected of being foodborne or waterborne.
b
Waterborne.
Source: Council for Agricultural Science and Technology (CAST) (1994) Foodborne Pathogens: Risks and Consequences. Ames, IA: CAST.
FOOD POISONING/Economic Implications 2677