Markovchick Vincent J., Pons Peter T., Bakes Katherine M.(ed.) Emergency medicine secrets. 5th ed
Подождите немного. Документ загружается.


Chapter 86 CHEST TRAUMA598
10. How do I diagnose a rib fracture by physical examination?
A rib fracture and chest wall contusion will both exhibit localized tenderness to palpation.
However, only a rib fracture will exhibit referred pain when the rib is compressed posterior or
anterior to the area of localized tenderness. In a stable patient in no respiratory distress, a
chest X-ray is unnecessary and may not reveal an insolated, nondisplaced rib fracture.
11. What are the radiologic findings of pulmonary contusion?
Characteristic findings on chest radiographs consist of solitary or multiple patchy, ill-defined
areas that may be either localized or diffuse resulting from blood accumulating in the alveoli
and interstitial spaces of the lung. Areas of opacification of the lung seen on chest X-ray
within 6 hours of blunt trauma are usually considered pulmonary contusions. Although often
visible within 1 to 2 hours following blunt chest trauma injury, these findings sometimes may
not appear until several hours after injury. The findings on chest X-ray often lag behind those
seen on clinical examination and chest CT.
12. What is the significance of a sternal fracture?
The significance of a sternal fracture lies in the fact that it is often associated with more
serious injuries such as damage to the great vessels or blunt myocardial injury (BMI)
requiring further investigation. Sternal fractures are often missed on initial chest X-ray and are
best viewed on lateral films or by CT scan.
13. When should BMI be suspected, and what types of injuries occur?
BMI is most commonly caused by high speed motor vehicle accidents, but it is also seen
with direct blows to the chest, crush injuries, falls from heights, blast injuries, and athletic
trauma. Mechanisms of blunt injury to the heart include sudden anterior-posterior
acceleration or deceleration forces causing the heart to impact against the sternum and
vertebrae, direct compression from a forceful blow to the chest or abdomen, any sudden
increase in intrathoracic and intracardiac pressures, and prolonged cardiopulmonary
resuscitation (CPR). BMI injuries include wall rupture, septal rupture, valvular injuries (aortic
most common), direct myocardial injury (contusion), coronary laceration or thrombosis, and
pericardial injury.
14. What are the symptoms of BMI and how is it diagnosed?
The symptoms of BMI vary with the severity of injury, but most commonly include chest pain,
tachycardia unexplained by the degree of blood loss, trauma, pain and dysrhythmias. Although
there are no good screening tests available, a reasonable approach to diagnosis includes
obtaining an initial electrocardiogram (ECG) for any patient who has sustained blunt trauma to
the mid-anterior chest. If normal, the patient may be discharged from the ED. If the initial ECG
is abnormal, they should be admitted to telemetry and a repeat ECG obtained in 24 hours. A
negative troponin obtained 6-8 hours post injury may further help to exclude BMI.
15. What are the most common ECG abnormalities in a patient with BMI?
A persistent supraventricular tachycardia (after all other causes have been treated or ruled
out), premature ventricular contractions (PVCs), transient right bundle branch block, or any
other new ECG abnormalities may commonly be seen in patients with BMI.
16. What are the clinical findings of pericardial tamponade?
Pericardial tamponade occurs when blood and clots accumulate in the pericardial space,
compromising cardiac filling pressure and ultimately leading to shock and death. Pericardial
tamponade should be suspected in any penetrating wound of the chest and is typically
associated with hypotension, tachycardia, and elevated central venous pressure (CVP).
Paradoxical pulse, characterized by a drop in systolic blood pressure of more than 10 to
15 mm Hg during normal spontaneous inspiration may also be seen. All of these findings
are also seen with tension pneumothorax and this must first be clinically ruled out. Bedside
ultrasonography is the most rapid and reliable means of diagnosis.
Chapter 86 CHEST TRAUMA 599
17. How is pericardial tamponade treated?
Pericardiocentesis should be immediately performed in unstable patients with tamponade.
Preferably this should be ultrasound-guided, followed by immediate transfer to the operating
room. If vital signs are lost in the ED, an immediate thoracotomy is indicated. Patients with
less severe hypotension, or in situations in which an operating room is not immediately
available, may benefit from placement of a pericardial catheter to allow for repeat aspirations
until arrangements can be made for transfer for more definitive therapy.
18. What is the mechanism and what are common locations of a traumatic
aortic tear?
The thoracic aorta is particularly susceptible to acceleration-deceleration shearing forces
because the arch is less mobile than the heart and the aorta distal to the ligamentum
arteriosum. Frontal or transverse deceleration causes shearing forces at the points of fixation,
with the most common site for disruption being just distal to the left subclavian artery. Vertical
acceleration-deceleration injuries such as falls may result in a tear of the ascending aorta with
coronary artery compromise or acute pericardial tamponade. At least 90% of blunt aortic
injuries in patients who reach the hospital alive occur in the isthmus of the aorta, between the
left subclavian artery and the ligamentum arteriosum.
19. How is acute traumatic rupture of the aorta (TRA) diagnosed?
Maintaining a high index of suspicion in any patient who has sustained sudden severe
deceleration or a high speed impact from the side is the first step to making this diagnosis.
TRA should also be considered in the presence of multiple rib fractures or flail chest,
although one third of blunt aortic injuries have no obvious external trauma. Physical findings
suggesting aortic injury include acute onset of upper extremity hypertension, difference in
pulse amplitude between upper and lower extremities, and a harsh murmur over the
precordium or space between the scapula. Widened mediastinum visualized on an upright
chest X-ray remains the most sensitive and specific finding in patients subsequently shown
to have TRA. Less predictive findings on chest X-ray include esophageal deviation, an apical
cap, left pleural effusion, obscuration of the aortic knob, loss of the paraspinal stripe, and
depression of the left mainstem bronchus. Keep in mind that 10% of initial chest X-rays in
patients with TRA are completely normal! Any suspicion based on mechanism or clinical
findings warrants further evaluation by CT of the chest with contrast or consideration of
transesophageal echocardiogram performed at the bedside for unstable patients.
20. What is the prognosis for blunt aortic injury and what emergent treatment is
necessary?
Approximately 85% to 90% of patients with aortic rupture die before medical aid reaches them.
The 10% to 15% who survive do so because not all three layers of the aorta are ruptured; the
adventitia remains intact and temporarily contains the hemorrhage. Left untreated, this injury
usually results in complete rupture and exsanguination, usually in hours to days, but this may
be delayed for years in the form of a pseudoaneurysm rupture. Therefore, diagnosis and
1. Hypotension.
2. Tachycardia.
3. Elevated central venous pressure or jugular venous distension.
4. Remember these are also seen in tension pneumothorax!
KEY POINTS: CLINICAL FINDINGS OF PERICARDIAL
TAMPONADE
Chapter 86 CHEST TRAUMA600
treatment is truly lifesaving. Treatment includes use of b-blockade with an esmolol drip
infusion to control blood pressure, maintaining a systolic pressure of less than 120 mm Hg,
and careful replacement of fluids to prevent worsening tear or rupture. Operative repair is
almost always necessary, but the optimal timing or method is determined based on the
individual patient.
21. How is penetrating chest trauma managed, and what is the significance of
wound location?
Wound location dictates the clinical approach by virtue of the organs at risk. From a functional
standpoint, wounds are categorized as central, peripheral, thoracoabdominal, and those in
adjacent areas (abdomen and neck). Multiple diagnostic and therapeutic approaches exist,
depending on the location of the chest wound and the nature of the wounding implement.
22. How are penetrating wounds of the central region managed?
Patients who are grossly unstable require transfer to an operating room for an emergent
thoracotomy with essentially no ED workup. Stable patients should be monitored closely
while a diagnostic workup (consisting of aortography, an esophagogram with or without
esophagoscopy, and possibly bronchoscopy) is done. If the workup is negative, observation
for 24 to 48 hours is appropriate; if positive, surgical intervention is needed. A helical CT scan
of the chest can be extremely useful to determine the presence and location of mediastinal
hemorrhage.
23. Should all patients with a penetrating peripheral wound of the chest be
admitted to the hospital?
Patients with peripheral wounds not in the thoracoabdominal area who are stable and have an
initial normal chest X-ray usually do not require admission. They should be observed in the
ED and have a repeat upright chest X-ray and hematocrit done in 4 to 6 hours. If repeat
studies are normal, the patient may be discharged.
24. Which trauma victims can potentially benefit from ED thoracotomy (EDT)?
Victims of blunt trauma with documented asystole, or who require more than 5 to 10 minutes of
prehospital CPR and arrive to the ED with no signs of life (i.e., pupillary response, respiration,
or motor activity), are generally regarded as being unsalvageable. Because survival is essentially
0% for this population, EDT is considered futile care. Victims of penetrating trauma who arrest
in the field but arrive with less than 15 minutes of prehospital CPR are potentially salvageable
and candidates for EDT. The population that appears to benefit the most from EDT are those
victims of penetrating chest trauma who arrest immediately on, or after, their arrival to the ED.
Immediate release of a pericardial tamponade or temporary repair of a cardiac laceration can be
life saving.
1. Blunt traumatic arrest with documented asystole.
2. Blunt traumatic arrest with prehospital CPR more than 5 minutes and no signs of life.
3. Penetrating traumatic arrest with CPR more than 15 minutes and no signs of life.
4. Penetrating traumatic arrest and asystole without the possibility of cardiac tamponade.
KEY POINTS: CONTRAINDICATIONS FOR ED THORACOTOMY

Chapter 86 CHEST TRAUMA 601
BIBLIOGRAPHY
1. Cook CC, Gleason TG: Great vessel and cardiac trauma. Surg Clin North Am 89:797–820, 2009.
2. Dulchavsky SA, Swarz KL, Kirkpatrick AW, et al: Prospective evaluation of thoracic ultrasound in the detection
of pneumothorax. J Trauma Injury Infect Crit Care 50:201, 2001.
3. Elie MC: Blunt cardiac injury. Mount Sinai J of Med 73(2):542–552, 2006.
4. Garofalo G, Busso M, Perotto F, et al: Ultrasound diagnosis of pneumothorax. Radiol Med 111:516–525,
2006.
5. Lindstaedt M, Germing A, Lawo T, et al: Acute and long-term clinical significance of myocardial contusion
following blunt thoracic trauma: results of a prospective study. J Trauma 52(3):479–485, 2002.
6. Ma, JO, Norvell JG, Subramanian S: Ultrasound applications in mass casualties and extreme environments.
Crit Care Med 35(5):275–279, 2007.
7. Maenza RL, Seaberg D, D’Amico F: A meta analysis of blunt cardiac trauma: ending myocardial confusion.
Am J Emerg Med 14:237, 1996.
8. McGillicuddy D, Rosen P: Diagnostic dilemmas and current controversies in blunt chest trauma. Emerg Med
Clin North Am 695–711, 2007.
9. Tintinalli JE, Kelen GD , Stapczynski JS, et al: Tintinalli’s emergency medicine: a comprehensive study guide,
ed 6, New York, 2004, McGraw-Hill.
10. Velmahos G, Karaiskakis M, Salim A, et al: Normal electrocardiography and serum troponin I levels preclude
the presence of clinically significant blunt cardiac injury. J Trauma 54:45–51, 2003.
602
Max V. Wohlauer, MD, and Ernest E. Moore, MD
ABDOMINAL TRAUMA
CHAPTER 87
1. Why is ABCDE relevant to the evaluation of significant abdominal trauma?
ABCDE (airway [with cervical spine control], breathing, circulation, disability, and exposure)
and clinical examination are the most important elements in the evaluation of a trauma patient.
Significant disability renders the clinical examination ineffective, requiring the use of diagnostic
studies. Exposure is a reminder that a complete examination of the abdomen, back, and pelvis
is essential.
Diffuse peritonitis or persistent hemodynamic instability is an absolute indication for prompt
laparotomy, regardless of injury mechanism.
1. Diffuse peritonitis
2. Hemodynamic instability
KEY POINTS: INDICATIONS FOR LAPAROTOMY
2. Discuss the key aspects of the history and physical examination in the initial
evaluation of abdominal trauma.
A good history is important in establishing the tempo, sequence, and extent of early
diagnostic efforts. Glean as much relevant information as possible from the prehospital
providers. They were at the scene and can provide a picture of what transpired. Key
information includes: extent of vehicular damage, duration of extrication, whether a passenger
died at the scene, use of seat belts and airbags, whether the person was ejected from the
vehicle, the presence of alcohol or drug use, and the trends in vital signs.
The primary survey consists of the initial identification and correction of life-threatening
injuries and is followed by a comprehensive head-to-toe examination of the patient, the
secondary survey. Lower thoracic and upper abdominal trauma should be considered as a
unit; suspect abdominal injury in any penetrating wound below the level of the nipple. With
significant injury, abdominal tenderness and guarding are prevalent, whereas rebound
tenderness and rigidity are relatively uncommon. Most importantly, 20% to 40% of patients
with serious intra-abdominal injury may appear asymptomatic.
3. What are some of the biomechanical differences between blunt and
penetrating trauma?
Blunt trauma results from a combination of crushing, stretching, and shearing forces. The
magnitude of these forces is proportional to the mass of the object, rate of change in velocity
(acceleration and deceleration), direction of the impact, and elasticity of the tissues. Conversely,
penetrating injuries result from the dissipation of energy and consequent tissue disruption along
the path of the offending projectile. The magnitude of injury depends on the kinetic energy
imparted by the penetrating object and the trajectory. Gunshot wounds can produce extensive
tissue damage (KE5MV
2
), making the injury patterns much less predictable than stab wounds.
Gunshot wounds that violate the peritoneum generally require a laparotomy.
Chapter 87 ABDOMINAL TRAUMA 603
4. Lower rib fractures are typically associated with what intra-abdominal
injuries?
Lower rib fractures are associated with injuries to the liver and spleen.
5. What is a Chance fracture?
A Chance fracture, a transverse fracture of a low thoracic or lumbar vertebrae, is caused by
flexion of the back and is associated with two-point seat-beat use. The incidence of associated
intra-abdominal injuries with a Chance fracture approaches 50% and includes small bowel and
abdominal aorta.
6. What injuries are associated with pelvic fractures?
Pelvic fractures are associated with injuries to the spleen, liver, or gastrointestinal tract in
approximately 10% of patients.
7. What is a seatbelt sign?
It is an ecchymotic imprint of the seatbelt on the anterior chest or abdomen of a restrained
passenger, indicating rapid deceleration from a motor vehicle crash. Presence of a seatbelt
sign is associated with a 20% incidence of intra-abdominal injury.
8. What is the characteristic finding of diaphragmatic rupture on chest X-ray?
A displaced nasogastric tube representing the stomach through the left hemithorax reveals a
diaphragm rupture. However, the chest X-ray is normal in up to half of patients with left
diaphragmatic injury and is often normal with right-sided injuries.
9. Does a normal serum amylase exclude pancreatic injury?
No, serum amylase is neither a sensitive nor specific test for pancreatic injury (i.e., a normal
amylase does not exclude pancreatic injury) and an elevated amylase may be due to increase
in salivary amylase.
10. What is the most commonly injured abdominal organ?
In blunt trauma, the spleen, and in penetrating trauma, it is the liver. The small bowel is the
most commonly injured abdominal hollow viscus.
1. Ultrasound FAST examination
2. DPL or DPA
3. CT
KEY POINTS: DIAGNOSTIC TOOLS FOR BLUNT TRAUMA
11. Which is the initial test of choice?
The focused abdominal sonography for trauma (FAST) is currently the initial test of choice in
the evaluation of blunt abdominal trauma. Performed by emergency medicine physicians and
surgeons, FAST is a rapid, painless, and sensitive test for identifying intra-abdominal fluid. If
the test is initially negative, repeating the examination in an unstable patient is imperative
because . 250 mL of blood within the abdominal cavity must accumulate in Morrison’s
pouch before a fluid stripe will appear on FAST.
12. What is the role of computed tomography (CT) scanning?
Abdominal CT is the test of choice for evaluating the abdomen of patients with significant
blunt abdominal trauma who are hemodynamically stable. Abdominal CT serves a major role
in the decision to manage the injured spleen, liver, or kidney nonoperatively. Because CT can
help determine the trajectory of a projectile, it also serves a role in selecting stable patients
with penetrating trauma for nonoperative management.
Chapter 87 ABDOMINAL TRAUMA604
13. What is the role of diagnostic peritoneal lavage (DPL)?
The major advantage of DPL is a sensitivity rate . 95% for the identification of intraperitoneal
hemorrhage. Because the technique is invasive and DPL fails to identify the source of
bleeding, its use has declined (as FAST has become routine). For hemodynamically
unstable patients, FAST is a more rapid, less invasive test, but is operator dependent. For
hemodynamically stable patients, CT provides more accurate information. A negative FAST
does not exclude injury in penetrating trauma. DPL is used predominantly when CT is
unavailable, or if the FAST results are negative but there is no other source to account for a
patient’s hemodynamic instability. The DPL is often done without the infusion of fluid (i.e.,
diagnostic peritoneal aspiration [DPA]). If the patient is hemodynamically unstable due to
intra-abdominal hemorrhage, gross blood should be retrieved on insertion of the catheter.
14. How are DPL results interpreted?
DPL is considered positive if . 10 mL of free blood is aspirated. Otherwise 1 L of warmed
normal saline is infused. A minimal recovery of 75% of lavage effluent is required for the test
to be considered valid. The fluid is analyzed for red blood cell (RBC) counts, white blood cell
(WBC) counts, lavage amylase, alkaline phosphatase, and bilirubin.
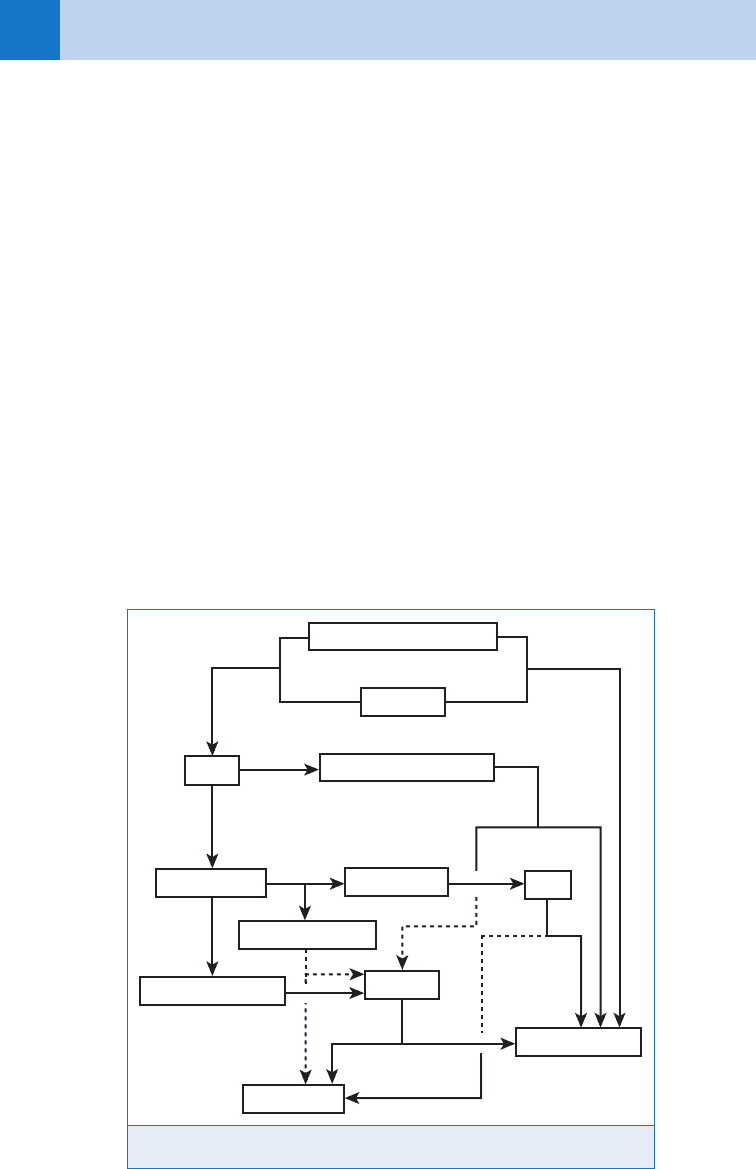
In blunt trauma, unlike in penetrating trauma, there are multiple sources that can cause
hemodynamic instability in which a laparotomy would not be the priority in management.
These include intrathoracic trauma, pelvic retroperitoneal injury, long bone fractures, or spinal
cord injury or intra-thoracic trauma. Therefore, it is important to search beyond the abdomen
for causes of hypotension before deciding to proceed to the operating room (Figs. 87-1
and 87-2).
Figure 87-1. Algorithm for management of blunt abdominal trauma.
Hemodynamic instability
Peritonitis
No
No
Yes
Yes
FAST
+
+
+
Recurrent hypotension
−
−
−
Hypotension
DPA
Operating room
CT scan
Repeat FAST
Distracting injuries
Clinical judgment
Observation
Chapter 87 ABDOMINAL TRAUMA 605
15. What are the unique concerns in a pregnant patient with abdominal
trauma?
The prevailing rule is that optimal care of the mother ensures the best outcome for the
fetus. Noninvasive fetal monitoring is used routinely if the fetus is potentially survivable
(i.e, .26 weeks). Hemodynamic instability, uterine rupture, placental abruption, and fetal
distress are indications for abdominal exploration.
16. What are the general principles of trauma in the elderly population?
The combination of chronic medical conditions and limited organ reserve makes elderly
patients especially vulnerable to trauma. Preinjury b-blocker use inhibits the physiologic
response to hemorrhagic shock and is associated with increased mortality. Anticoagulant
use (i.e., warfarin) prolongs hemostasis and is associated with increased mortality in patients
with head injuries.
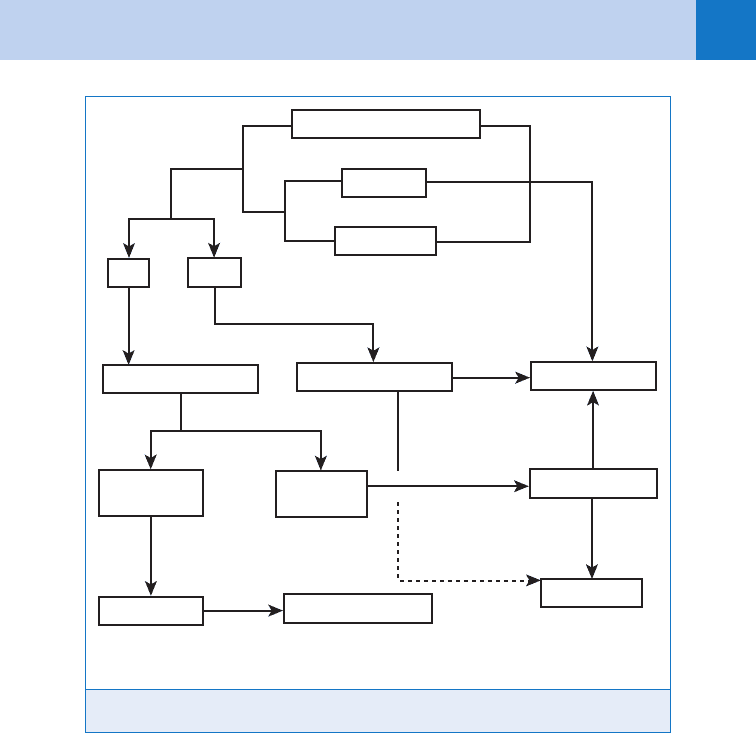
Gunshot wounds (GSW) that violate the peritoneal fascia mandate a laparotomy,
with the possible exception of a low energy GSW to the liver. Stab wounds are managed
selectively. Local wound exploration in the ED provides valuable information because only
two thirds of stab wounds to the anterior abdomen actually violate the peritoneum. Even if
the peritoneum is violated, only 50% of these stab wounds produce injuries that require
surgical intervention.
Figure 87-2. Algorithm for management of penetrating abdominal trauma.
Hemodynamic instability
No
Yes
SW
GSW
Peritonitis
Evisceration
Peritoneum violated
Peritoneal violation*
Operating room
Serial abd.
exams
Peritoneal signs
Local wound
exploration
Fascia intact
Observation
Discharge to home
No
No
No
Yes
* Isolated liver injury: non-op management in select cases
Yes
Chapter 87 ABDOMINAL TRAUMA606
17. In the management of abdominal trauma, are children really just small adults?
No, injury patterns are different in children due to their size (see Chapter 90). The elasticity of
the child’s lower rib cage and the relatively large abdominal cavity increase susceptibility to
injury. Although blunt injuries tend to be self-limited, an aggressive operative policy is
warranted for pediatric trauma because of the child’s limited physiologic reserve.
1. Any patient who has persistent hemodynamic instability or signs of peritonitis following ab-
dominal trauma requires emergent laparotomy.
2. A meticulous physical examination is the most important element in the evaluation of a lucid
trauma patient.
3. A negative FAST examination does not reliably exclude significant intraperitoneal injury.
4. Observing a trauma patient is an active process, including serial physical examinations and
repeat abdominal ultrasonography.
5. CT scan is the most reliable means to evaluate abdominal trauma in the hemodynamically
stable patient.
KEY POINTS: ABDOMINAL TRAUMA
BIBLIOGRAPHY
1. Demetriades D, Velmahos GC: Indications for and techniques of laparotomy. In Moore EE, Feliciano D, and
Mattox K, editors: Trauma, ed 6, New York, 2008, McGraw Hill Professional, Chapter 30.
2. Hunt JP, Weintraub SL: Kinematics of trauma. In Moore EE, Feliciano D, and Mattox K, editors: Trauma, ed 6,
New York, 2008, McGraw Hill Professional, Chapter 7.
3. Kaufman CR: Initial assessment. In Moore EE, Feliciano D, and Mattox K, editors: Trauma, ed 6, New York,
2008, McGraw Hill Professional,, Chapter 11.
4. McKenney MG, Schulman CI: Geriatric trauma. In Moore EE, Feliciano D, and Mattox K, editors: Trauma, ed 6,
New York, 2008, McGraw Hill Professional, Chapter 47.
5. Murr PC, Moore EE, Lipscomb R, et al: Abdominal trauma associated with pelvic fracture. J Trauma 20:
919–923, 1980.
6. Neideen R, Lam M, Brasel K: Preinjury beta blockers are associated with increased mortality in geriatric trauma
patients. J Trauma 65:1016–1020, 2008.
7. Scalea TM, O’Toole R: Pelvic fractures. In Moore EE, Feliciano D, and Mattox K, editors: Trauma, ed 6, New York,
2008, McGraw Hill Professional, Chapter 38.
8. Tuggle DW: Pediatric trauma. In Moore EE, Feliciano D, and Mattox K, editors: Trauma, ed 6, New York, 2008,
McGraw Hill Professional, Chapter 46.
607
CHAPTER 88
PELVIC FRACTURES AND
GENITOURINARY TRAUMA
Walter L. Biffl, MD, FACS
1. Why are pelvic fractures so deadly?
Pelvic fractures can lead to life-threatening hemorrhage. Sources of bleeding include the pelvic
bones themselves, surrounding soft tissue, and the extensive arterial and venous networks
running through the pelvic ring. The considerable force required to fracture the pelvis typically
results in significant associated injuries in up to 90% of patients. Collectively, these factors
account for high rates of morbidity and mortality.
2. What is the approach to the patient with a pelvic fracture?
The evaluation begins with the primary survey (the ABCs) and resuscitation. Unstable patients
with pelvic fractures require a multidisciplinary approach, with the fundamental objectives of:
n
Control of hemorrhage
n
Reversal of shock
n
Identification of associated injuries
n
Prioritization of treatment based on threat to life
Life-threatening associated injuries are evaluated and treated simultaneously with systematic
assessment of the pelvic fractures. Because these patients may require coordinated
interventions by multiple specialties, the immediate presence of the attending trauma surgeon,
attending orthopedic surgeon, and interventional radiologist in the ED is warranted. (Fig. 88-1)
3. How do you examine the patient with a pelvic fracture?
Very carefully! The physical examination directed at the pelvis includes gentle manual
compression of the bony pelvis and inspection of the perineum, rectum, and vagina for
ecchymosis, ongoing bleeding, and open wounds. An unstable pelvic fracture is not a
“teaching case;” every manipulation leads to further hemorrhage because bony edges disrupt
clot and lacerate tissue and blood vessels. Plain anteroposterior radiography of the pelvis is a
priority in patients with suspected fracture. Hemodynamically stable patients may be evaluated
further with additional views (e.g., inlet/outlet) or computed tomography (CT), but this should
not interfere with resuscitation or necessary interventions.
4. How are pelvic fractures classified?
The Tile classification, based on pelvic stability, is useful for reconstructive planning:
n
Tile A: Rotationally and vertically stable
n
Tile B: Rotationally unstable, vertically stable
n
Tile C: Rotationally and vertically unstable
A commonly used scheme is that of Young and Burgess, which is based on injury mechanism
and is more helpful in assessing the risk of hemorrhage:
Anteroposterior compression (APC)
n
APC I: Pubic symphyseal diastasis , 2.5 cm, no significant posterior ring injury
n
APC II: Pubic symphyseal diastasis . 2.5 cm, tearing of anterior sacral ligaments
n
APC III: Complete disruption of pubic symphysis and posterior ligament complexes
Lateral compression (LC)
n
LC I: Posterior compression of sacroiliac (SI) joint without ligament disruption
n
LC II: Posterior SI ligament rupture, sacral crush injury
n
LC III: LC II, with APC injury to contralateral pelvis