Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

C HAPTER 35 • Laparoscopic Placement of Adjustable Gastric Band 389
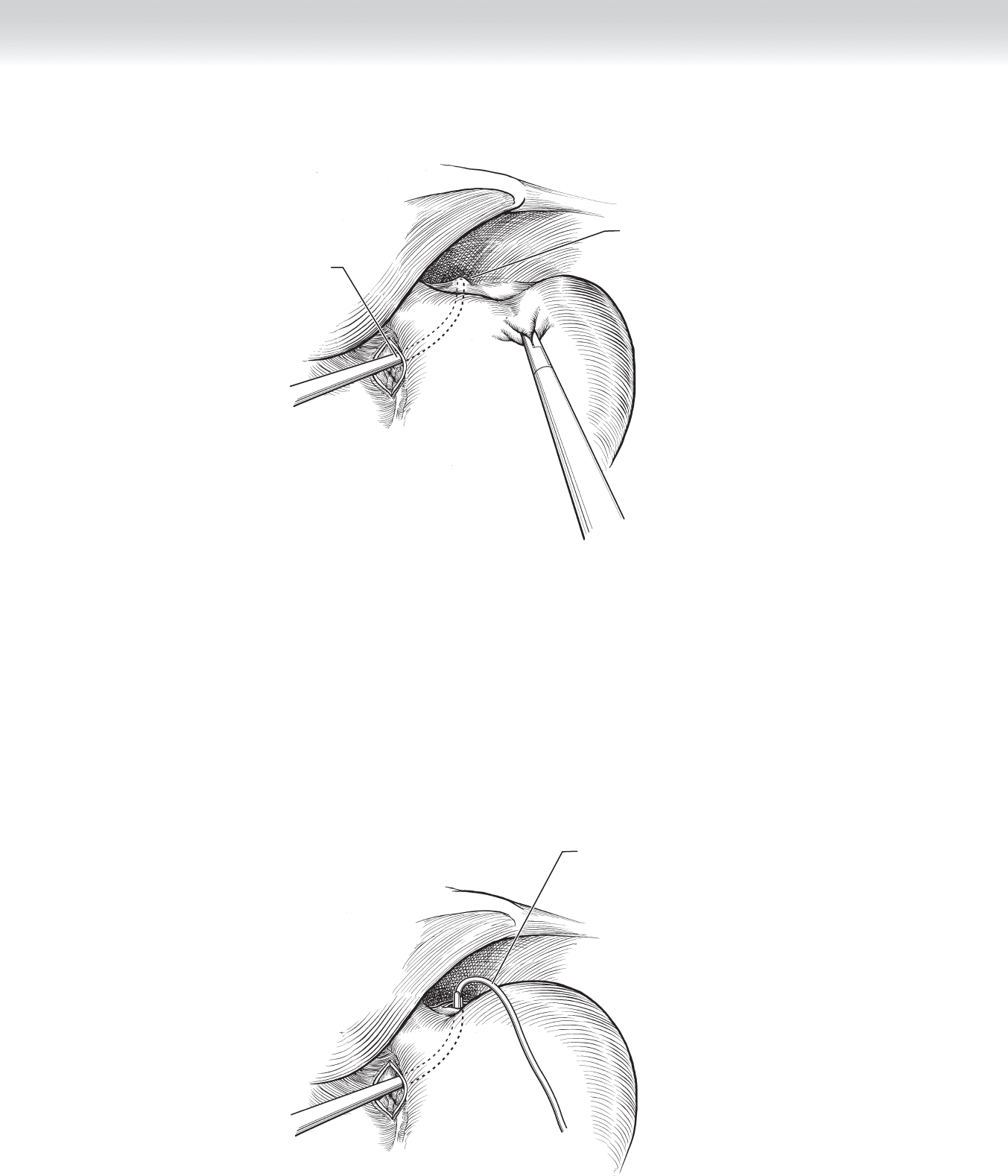
Articulating dissector tenting
phrenogastric ligament at
angle of His for blunt dissection
Articulating dissector
inserted in tunnel
posterior to stomach
FIGURE 35 –3
Band tubing
grasped and pulled
around cardia of stomach
FIGURE 35–4
◆ The retrogastric instrument is withdrawn, pulling the tubing and band into position
behind the stomach. There is often signifi cant resistance met as the band passes behind
the stomach. The tubing is fed through the band buckle, and the device is closed securely.
Each band has an indicator to identify a securely closed band (Figures 35-5 and 35-6).
◆ The fundus of the stomach is then wrapped over the left lateral aspect of the band and
secured to the pouch of stomach above the band with a series of interrupted seromuscular
2-0 polyester sutures. Usually three sutures are suffi cient. No effort should be made to
cover the area around the buckle or the buckle itself (Figure 35-7).
◆ The buckle is lifted to check for underlying tension and then rotated toward the lesser
curvature as far as allowable. The tip of the band tubing is grasped and pulled through the
15-mm trocar after the surgeon ensures that the tubing is not knotted. The instruments in-
cluding the liver retractor are removed, and the pneumoperitoneum is released.
◆ The 15-mm trocar is removed, leaving the band tubing in place. A pocket is created bluntly
through the 15-mm port site. The pocket is medial to the incision and at the level of the
anterior abdominal fascia. Enough space should be made for the injection port to rest fl ush
against the fascia as far medially as allowable.
◆ Two to four nonabsorbable sutures are placed in the fascia in an orientation consistent with
the port being used. The two tails of each suture are clamped together with a hemostat to
avoid tangling. The distal few centimeters of the tubing is trimmed and connected to the
injection port, which has been prepared according to the manufacturer’s specifi cations. The
sutures are threaded through the holes on the injection port and then clamped together
again (Figure 35-8).
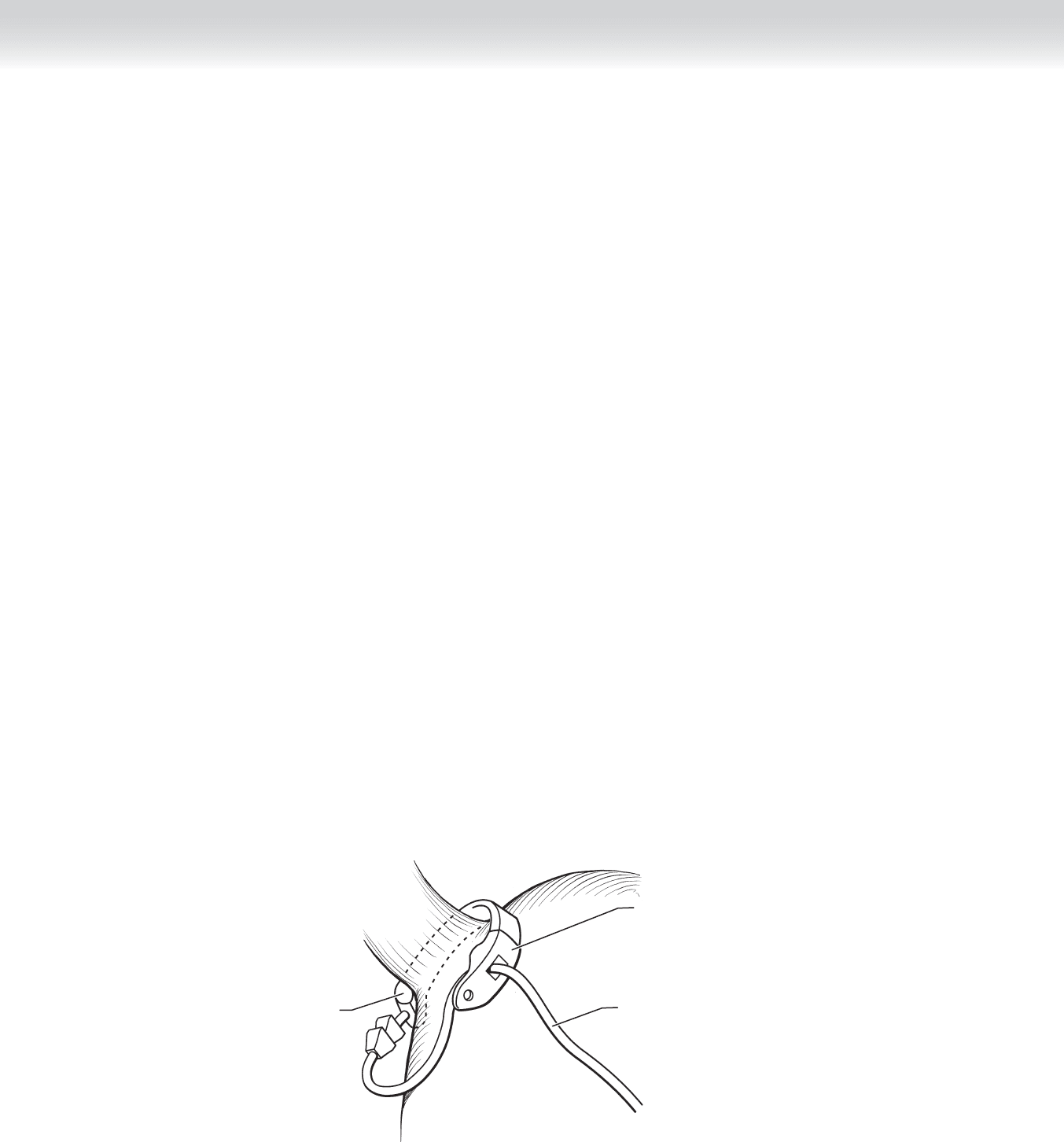
Band
Buckle
Band tubing
FIGURE 35 –5
Section IV • The Abdomen390
Band in place
Esophagus
FIGURE 35 –6
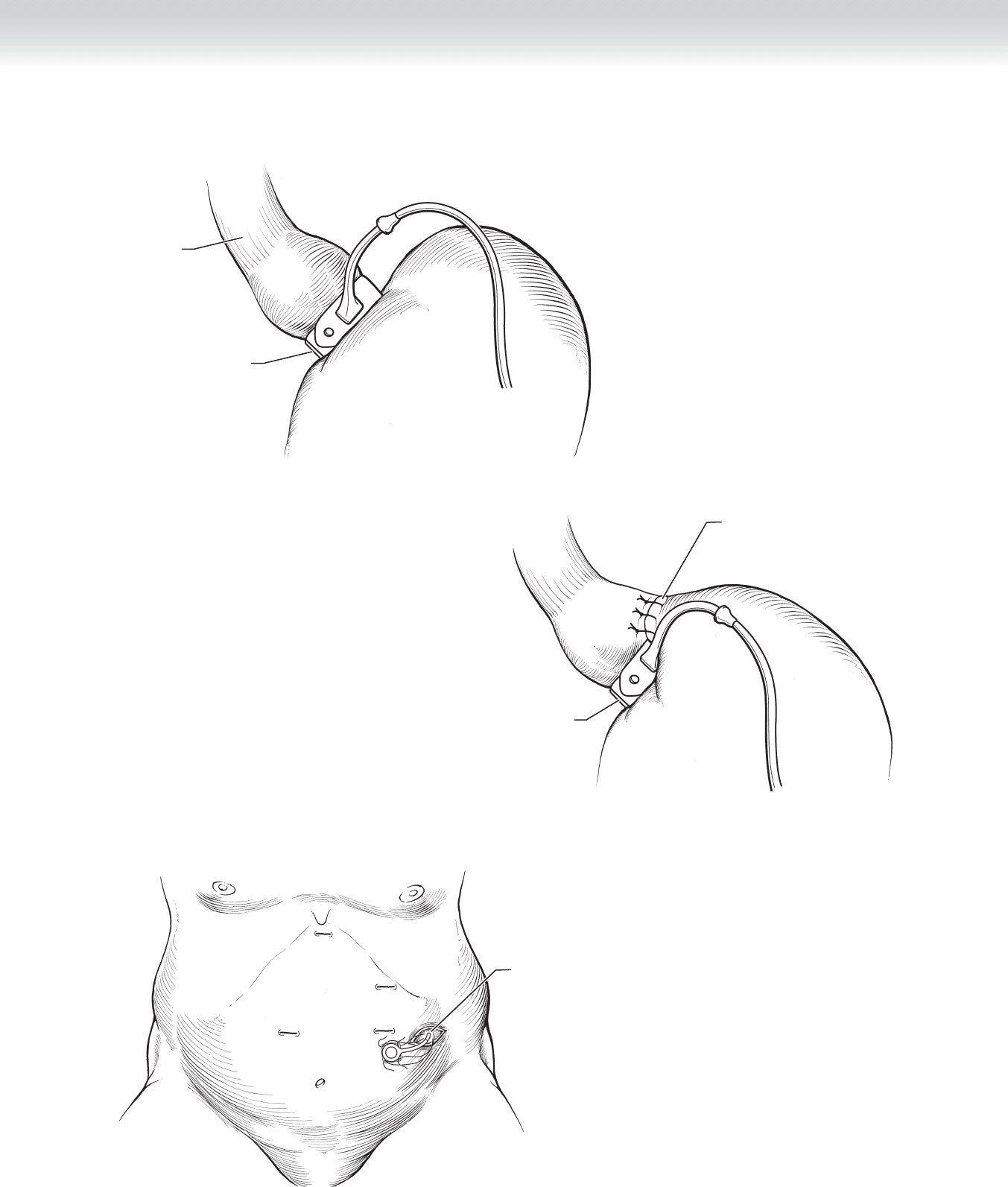
Band in place
Fundus of stomach sewn
over to secure band
FIGURE 35 –7
Tubing brought
out of 15-mm
port site
FIGURE 35 –8
C HAPTER 35 • Laparoscopic Placement of Adjustable Gastric Band 391
392 Section IV • The Abdomen
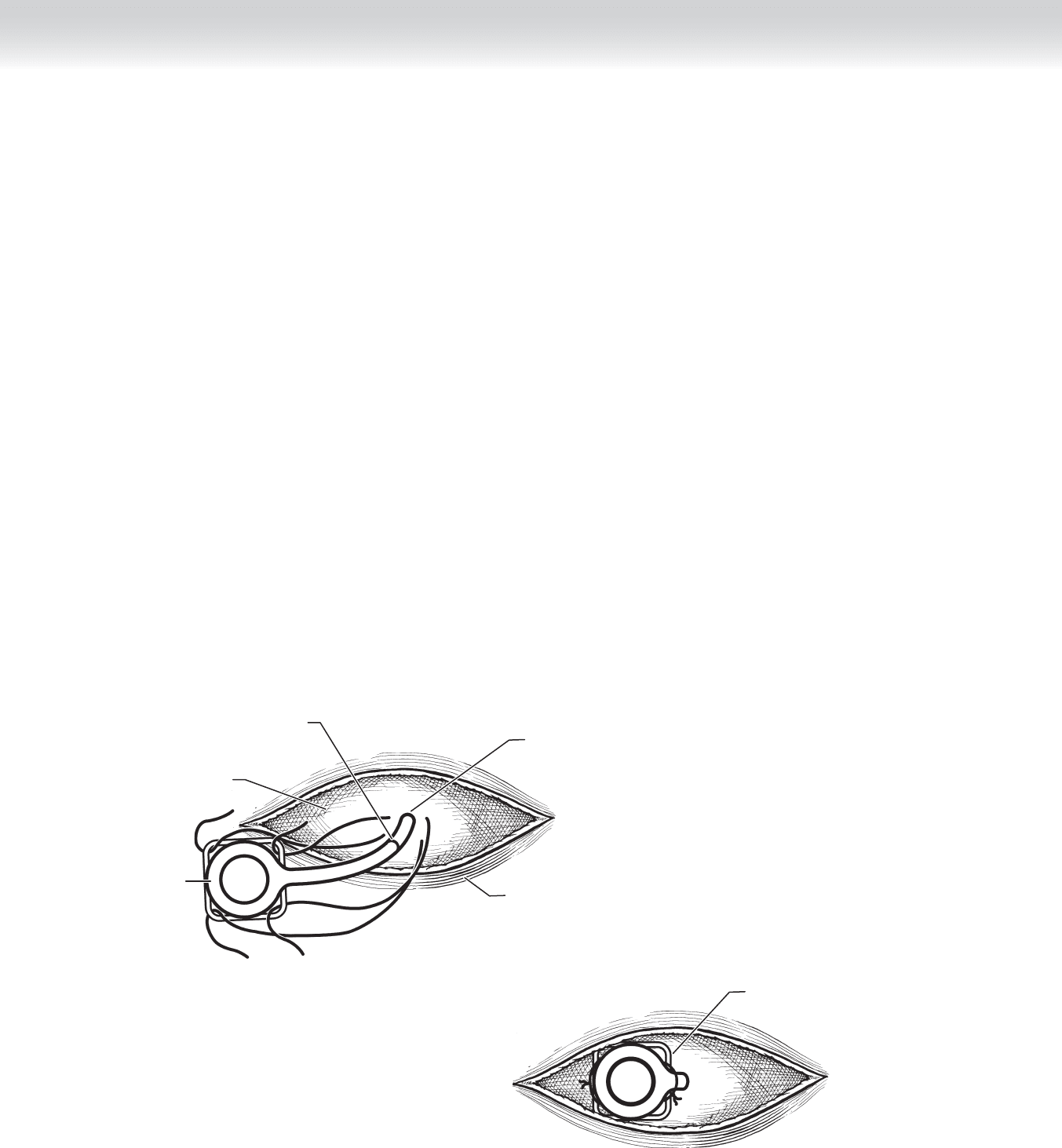
◆ Once all of the sutures are in place, the excess tubing is fed through the fascial opening and
into the peritoneal cavity. The port is rested on the fascial surface, and the sutures are tied
(Figure 35-9).
3. CLOSURE
◆ The wounds are inspected for hemostasis. A subcuticular closure with absorbable suture is
preferred. The wounds are dressed with tissue adhesives or wound approximation tapes
and small bandages.
STEP 4: POSTOPERATIVE CONSIDERATIONS
◆ A low-potency oral narcotic combination elixir, such as acetaminophen with codeine or
hydrocodone/acetaminophen, is usually suffi cient for pain management.
◆ Nausea is a common postoperative complaint that should be effectively managed to avoid
retching and possible displacement of the band.
Tubing brought
out of 15-mm port site
Skin
Connection
Anterior
rectus sheath
Port
A
Port secured to
rectus sheath
B
FIGURE 35 –9

C HAPTER 35 • Laparoscopic Placement of Adjustable Gastric Band 393
◆ Patients are offered sugar-free, carbonation-free clear liquids when awake. Advancing the
diet to pureed foods is determined by patient progress, but no solid foods are offered for
4 postoperative weeks.
◆ A barium swallow is used to check band position and patency before discharge. It is also
helpful to have this early postoperative study for comparison and troubleshooting of
problems in the future.
◆ Most patients are observed in the hospital overnight, but outpatient band surgery is becom-
ing more common recently, and is likely to be the most common postoperative management
strategy soon.
◆ A dedicated postoperative adjustment and follow-up schedule must be provided to achieve
even reasonable results with gastric banding. Weight loss approaches that seen after gastric
bypass when patients have access to band adjustments on short notice. The fi rst adjustment
is not offered until 6 weeks after the operation.
STEP 5: PEARLS AND PITFALLS
◆ Failure to repair even the smallest hiatal hernia can result in worsening of refl ux as the
band is infl ated, leading to frustrating symptoms and unsatisfactory outcomes.
◆ The position of the bra line and belt line should be kept in mind when selecting the loca-
tion of the 15-mm trocar to minimize discomfort over the site of the injection port.
◆ The posterior aspect of the distal esophagus and stomach wall are at risk for injury when
passing the angled dissector through the retrogastric tunnel. One must be sure no resistance is
met when the instrument is inserted and fl exed. In addition, there should be no esophageal or
gastric tissue when passing the tip of the instrument through the peritoneum at the angle of
His. Often the peritoneum overlying the left crus immediately to the left of the angle of His
should be bluntly opened before passing the dissector through the pars fl accida window. If
this is done, the tip of the dissector will be easily identifi ed.
◆ Once buckled, the band can be quite diffi cult or impossible to reopen. One should be sure
the band is in the appropriate position and will not be too tight before closing it. If the
band appears too tight, the underlying fat along the lesser curvature or at the esophagogas-
tric junction may need to be divided with the cautery or ultrasonic shears. Rarely, the band
may have to be replaced with a larger size.
◆ Careful needle management and knot tying must be used to avoid sticking any component
of the band system. Leaks of the band balloon can be fi xed only by replacing the whole
system. The needle should remain in view continuously.

394
STEP 1: SURGICAL ANATOMY
◆ Meckel’s diverticulum is an outpouching in the terminal ileum on the antimesenteric border.
It exists in approximately 2% of the population but is largely asymptomatic. The frequent
presence of ectopic gastric mucosa contributes to its common clinical presentation of brisk
gastrointestinal (GI) hemorrhage.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Asymptomatic Meckel’s diverticulum is identifi ed during abdominal cavity operation for other
unrelated etiology. In general, resection of asymptomatic Meckel’s diverticulum should be
considered carefully based on the patient’s overall condition and initial reasons for laparotomy.
◆ All symptomatic Meckel’s diverticulum should be resected. Massive lower GI tract hemor-
rhage is its typical presentation, and the diagnosis is determined by scintigraphy with
sodium technetium-99m (Tc-99m)-pertechnetate, which localizes ectopic gastric mucosa.
◆ For Meckel’s diverticulitis, its presenting signs and symptoms are generally indistinguishable
from acute appendicitis and determined only at operation.
◆ Preoperative prophylactic antibiotic should be administered intravenously 30 minutes before
skin incision.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ Patient is positioned supine and the right-sided transverse abdominal skin incision is made
slightly inferior to the umbilicus (Figure 36-1).
CHAPTER
36
Meckel’s Diverticulectomy
Dai H. Chung
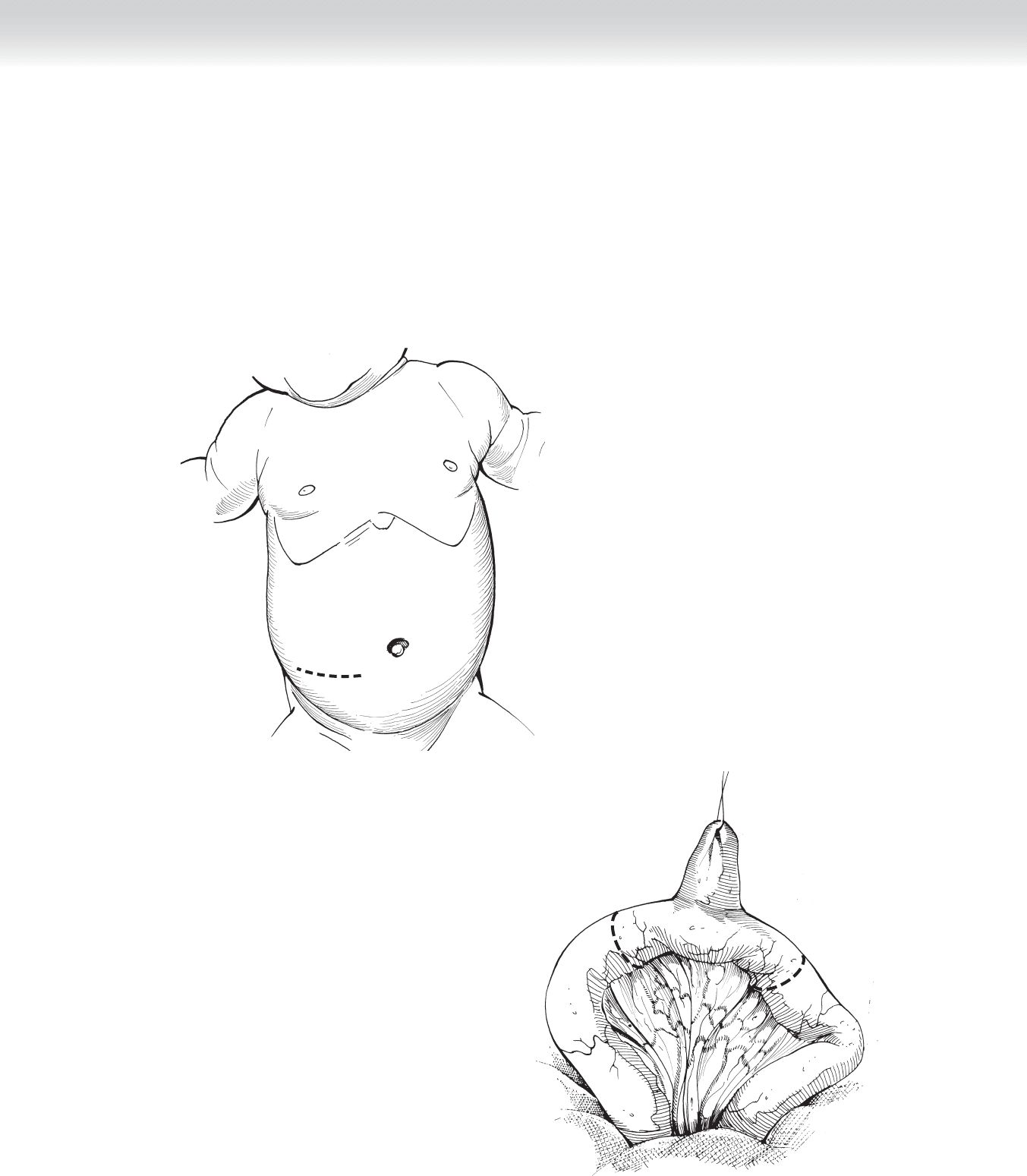
◆ For a laparoscopic approach, umbilical trocar incision is made for the laparoscope and two
additional small trocar incisions on either side of the abdomen for instrumentation.
◆ Meckel’s diverticulum is typically located on the antimesenteric side of the terminal ileum,
within 2 to 3 feet from the ileocecal region (Figure 36-2).
FIGURE 36–1
FIGURE 36–2
C HAPTER 36 • Meckel’s Diverticulectomy 395

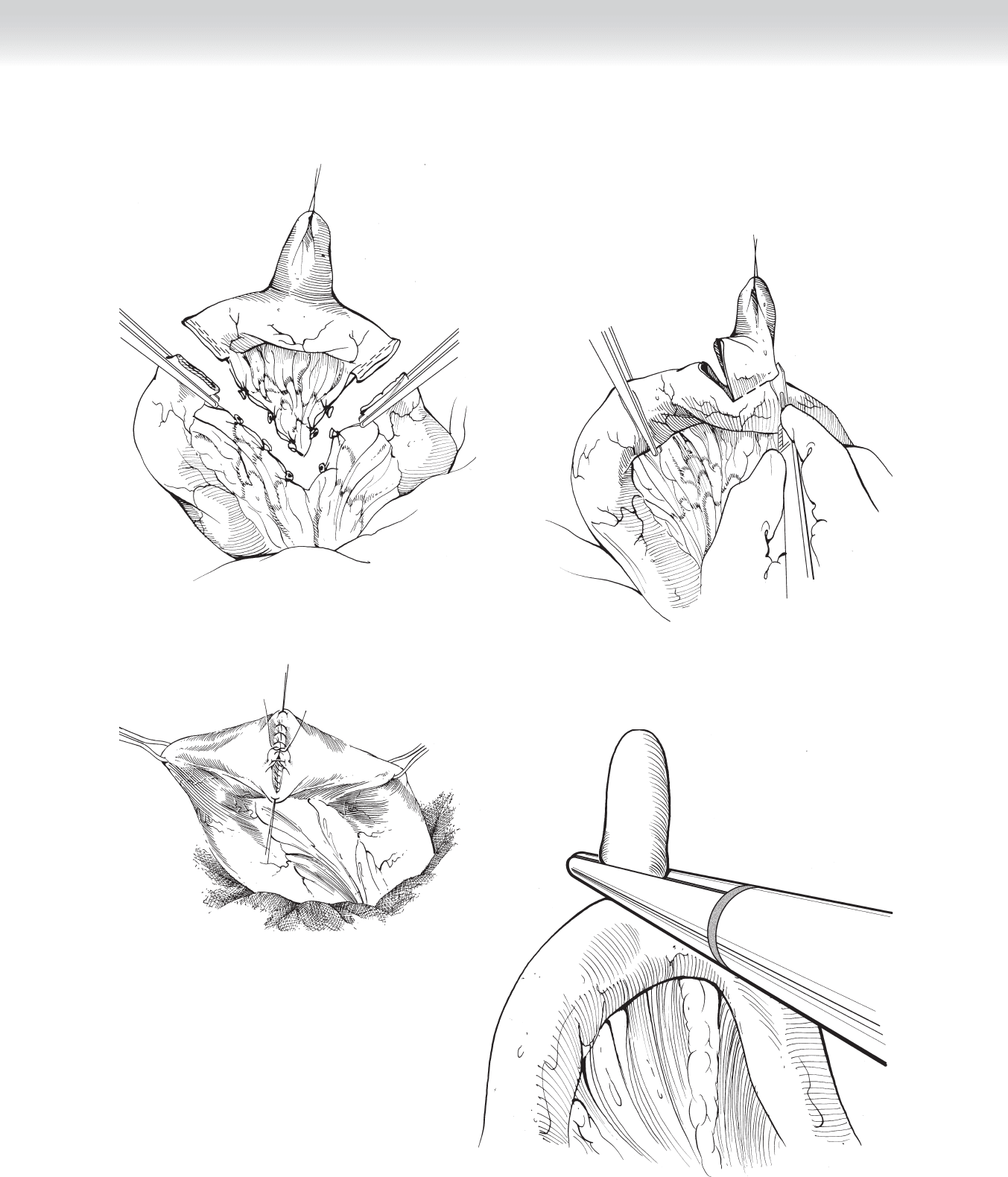
2. DISSECTION
◆ Segmental resection of ileum incorporating the Meckel’s diverticulum is the ideal resection
margin, because ectopic mucosa may be present throughout the entire axis of the diverticulum
(Figure 36-3). For resection, proximal and distal luminal content fl ow should be controlled
using either gentle placement of bowel clamps or circumferential vessel loops. A stapling device
may also be used to perform bowel resection.
◆ Alternatively, wedge resection of the diverticulum is also acceptable, if no abnormal thick-
ening at the base is confi rmed. After controlling intraluminal fl ow, the surgeon resects the
diverticulum using a knife or electrocautery (Figure 36-4).
◆ Two-layer anastomosis is preferred using inner running chromic sutures with outer interrupted
seromuscular silk stitches (Figure 36-5). For small infants (younger than 6 months), single-
layer anastomosis with full-thickness silk sutures is also acceptable. The mesenteric defect
should be closed to prevent potential internal hernia.
◆ For a laparoscopic approach, the tip of the Meckel’s diverticulum is suspended with a
grasper, and an ensdoscopic gastrointestinal anastomosis (GIA) stapler is used to
transect at its base. Stapling at 90 degrees to the longitudinal axis of the ileum is ideal to
avoid narrowing the lumen (Figure 36-6).
3. CLOSING
◆ Once anastomosis is complete and hemostasis is ensured, abdominal fascia closure is
performed in layers using absorbable sutures (3-0 polyglycolic) in a continuous manner.
◆ The skin is reapproximated with a subcuticular stitch of 5-0 absorbable Monocryl suture.
STEP 4: POSTOPERATIVE CARE
◆ Nasogastric tube decompression is seldom necessary.
◆ Patient may be started on an oral clear liquid diet on postoperative day 1 and then gradually
advanced to regular diet appropriate for age.
◆ Two doses of postoperative intravenous antibiotics are administered.
Section IV • The Abdomen396
C HAPTER 36 • Meckel’s Diverticulectomy 397
FIGURE 36–3
FIGURE 36–4
FIGURE 36–5
FIGURE 36–6

398 Section IV • The Abdomen
STEP 5: PEARLS AND PITFALLS
◆ Adequate resection of Meckel’s diverticulum with complete incorporation of any ectopic
mucosa is critical to this procedure.
◆ Laparoscopic approach is gaining popularity; however, it is critical to ensure adequate
resection margin at the base.
SELECTED REFERENCES
1. Yahchouchy EK, Marano AF, Etienne JC, Fingerhut AL: Meckel’s diverticulum. J Am Coll Surg
2001;192:658-662.
2. Cullen JJ, Kelly KA: Current management of Meckel’s diverticulum. Adv Surg 1996;29:207-214.
3. Brown RL, Azizkhan RG: Gastrointestinal bleeding in infants and children: Meckel’s diverticulum and
intestinal duplication. Semin Pediatr Surg 1999;8:202-209.
4. Rothenberg SS: Laparoscopic segmental intestinal resection. Semin Pediatr Surg 2002;11:211-216.