Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


399
STEP 1: SURGICAL ANATOMY
◆ Anatomic relationships of the appendix for laparoscopic appendectomy are identical to
those for the open appendectomy.
◆ With the limited access and visibility possible through the laparoscope, the serosal land-
marks of the colon and appendix become more signifi cant.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Early diagnosis and expeditious operative intervention for appendicitis prevents the compli-
cations of perforation and spillage of purulence.
◆ Perform laparoscopic appendectomy after careful consideration with the option of open
appendectomy and after assessing the patient, habitus, placement of trocars and scars, and
likelihood that you can complete the procedure without needing to convert to an open
procedure.
Laparoscopic Appendectomy
Arthur P. Sanford
CHAPTER
37
400 Section IV • The Abdomen
STEP 3: OPERATIVE STEPS
1. INCISION/TROCAR PLACEMENT
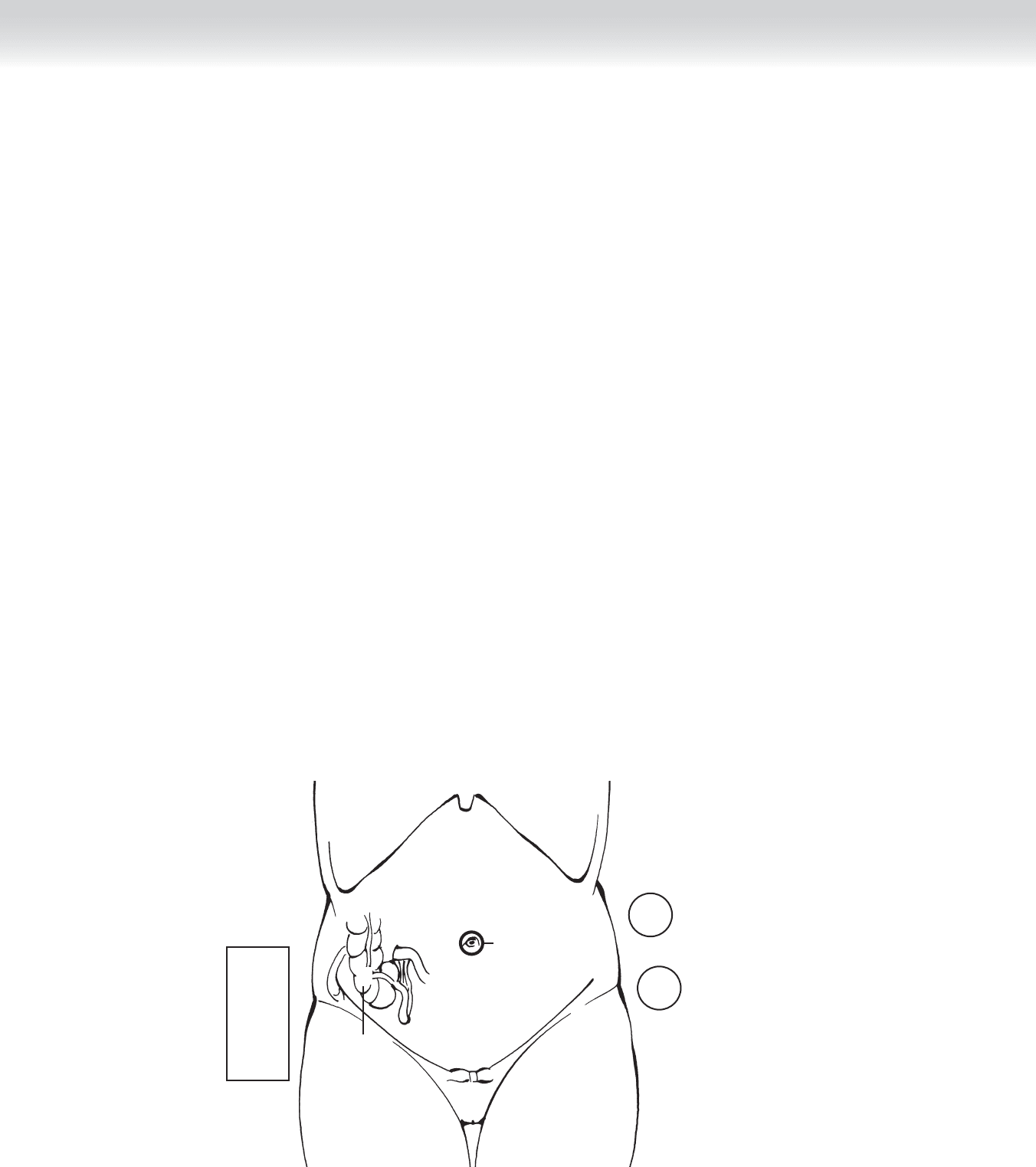
◆ Both the surgeon and assistant/camera operator assume places at the left side of the patient
(Figure 37-1).
◆ Access to the peritoneum begins with a 12-mm umbilical port, placed by either Hasson or
Veress technique and insuffl ated to 15 cm H
2
O pressure for placement of the laparoscope.
◆ Thorough laparoscopic evaluation of the abdomen is undertaken to ensure that it is appro-
priate to proceed without conversion to an open procedure.
◆ The patient is placed in enough of the Trendelenburg position to move the intra-abdominal
contents out of the lower quadrants of the abdomen.
◆ Two additional ports are placed under direct visualization from the laparoscope, with a 5-mm
port in the left lower quadrant (LLQ) and a 10-mm port in the right upper quadrant (RUQ).
◆ Transillumination of the abdominal wall prevents injury to the nearby vascular structures.
Monitor
5-mm trocar
10-mm trocar
5-mm trocar
Surgeon
Assistant
Camera port
10-12 mm
X
X
X
X
FIGURE 37 –1
C HAPTER 37 • Laparoscopic Appendectomy 401
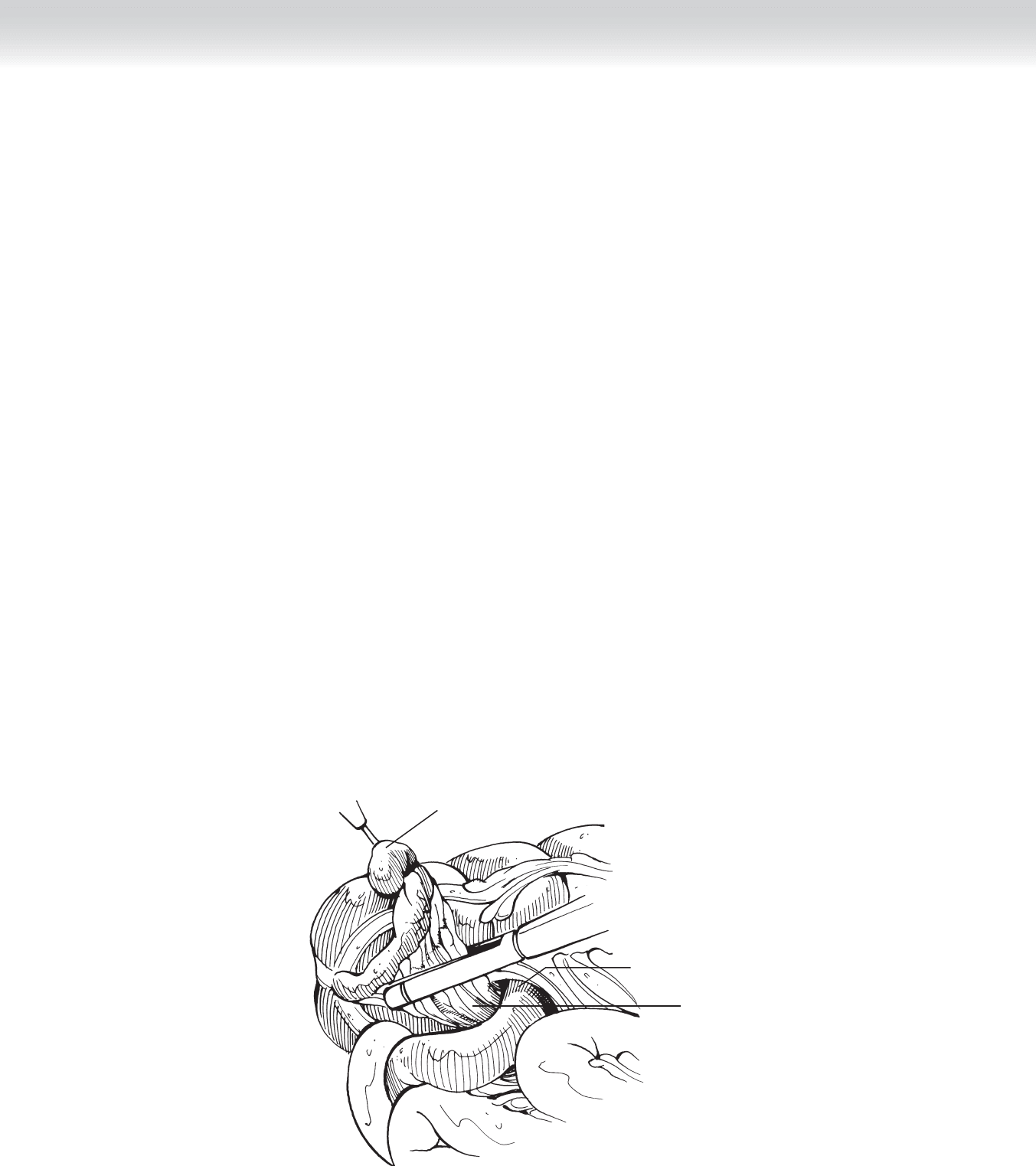
Appendix held up
by Endoloop
Mesoappendix and
appendiceal artery
Ileocecal junction
FIGURE 37 –2
2. DISSECTION
◆ Use the instruments to expose the cecum and appendix.
◆ It is necessary to dissect the cecum to take down the white line of Toldt and adequately
mobilize the base of the appendix and the mesoappendix.
◆ Elevate the cecum and base of the appendix using a laparoscopic Babcock clamp from the
RUQ trocar.
◆ Identify the mesoappendix containing the appendiceal artery and pass a curved Maryland
dissector through the mesoappendix at the base of the appendix; visualize both sides of the
mesoappendix to ensure no other unintended structures are present.
◆ Divide the mesoappendix between the free edge of the mesoappendix and the previously
dissected point using an endoscopic stapler, endoscopic clips, or a harmonic scalpel
(Figure 37-2).
402 Section IV • The Abdomen
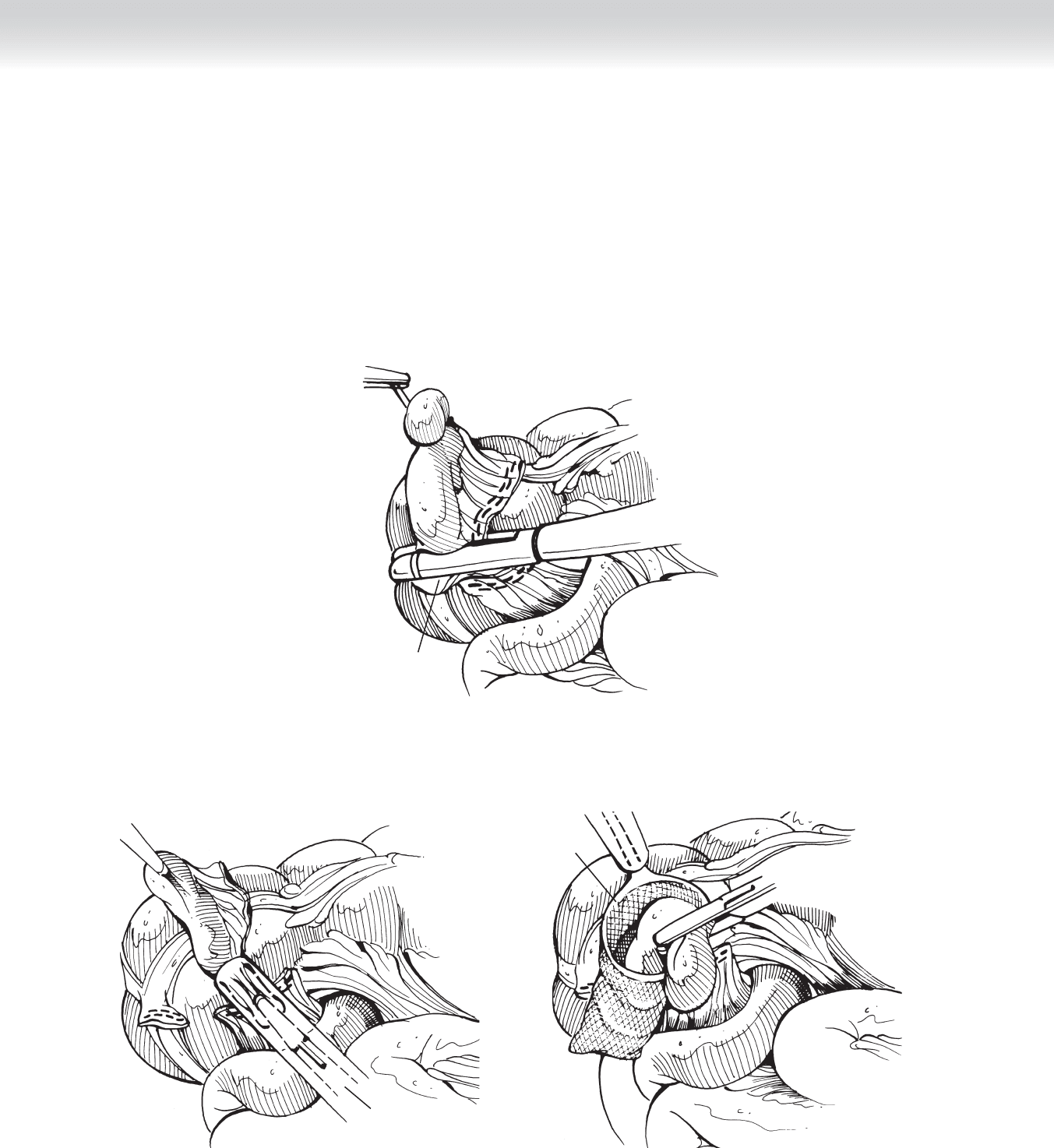
◆ Ligate the appendical base with either an endoscopic stapler using a tissue load or an
Endoloop to prevent spillage of cecal contents (Figure 37-3).
◆ Then either place the appendix in an Endobag or retract into the larger RUQ trocar for
withdrawal from the abdomen (Figure 37-4).
"Second fire" of endostapler
at base of appendix
FIGURE 37 –3
Appendix drawn into
reducing sleeve
A
Appendix
placed
in Endobag
B
FIGURE 37 –4

C HAPTER 37 • Laparoscopic Appendectomy 403
3. CLOSING
◆ Undertake a fi nal inspection for hemostasis before removal of the laparoscope and ports.
◆ Minimize irrigation of the abdomen to a volume that you can completely aspirate to prevent
abscess formation.
◆ Remove ports under direct visualization from within the abdomen.
◆ Undertake suture closure for any port greater than 5 mm and the umbilical port.
◆ Apply sterile dressings.
◆ No peritoneal drains are indicated.
STEP 4: POSTOPERATIVE CARE
◆ If placed at operation, nasogastric tube and Foley catheter can be removed immediately
postoperatively.
◆ Dietary resumption may begin immediately in the case of acute appendicitis, but if free
purulence was found at operation, postoperative ileus mandates awaiting the return of
bowel function.
◆ Postoperative antibiotics are not necessary in acute appendicitis but should be continued in
the presence of intra-abdominal purulence.
STEP 5: PEARLS AND PITFALLS
◆ Placement of trocars facilitates intra-abdominal manipulation and avoids narrow angles of
functional use.
SELECTED REFERENCES
1. Silen W, Cope Z: Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. New York, Oxford University
Press, 2005, pp 67-83.
2. Lally KP, Cox CS Jr, Andrassy R: The appendix. In Townsend CM, Beauchamp RD, Evers BM, Mattox KL
(eds): Sabiston Textbook of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 1381-1399.

404
STEP 1: SURGICAL ANATOMY
◆ The blood supply for the appendix comes from the appendiceal artery, a branch of the
ileocolic artery.
◆ The location of the appendix in the right lower quadrant (RLQ) is variable, depending on
a possible retrocecal position.
◆ Note: The gravid uterus also displaces the cecum cephalad.
◆ To increase exposure of the peritoneal cavity, extend a muscle-splitting incision, lateral to
the arcuate line, medially and laterally.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ History, physical examination, laboratory tests, and computed tomography (CT) scan as in-
dicated will identify patients with acute appendicitis for appendectomy.
◆ Appropriate preoperative antibiotics should be administered upon confi rmation of the
diagnosis of appendicitis until operative intervention, with postoperative administration
based on operative fi ndings. Coverage should include typical intestinal fl ora, including
gram-negative organisms and anaerobes.
CHAPTER
38
Open Appendectomy
Arthur P. Sanford
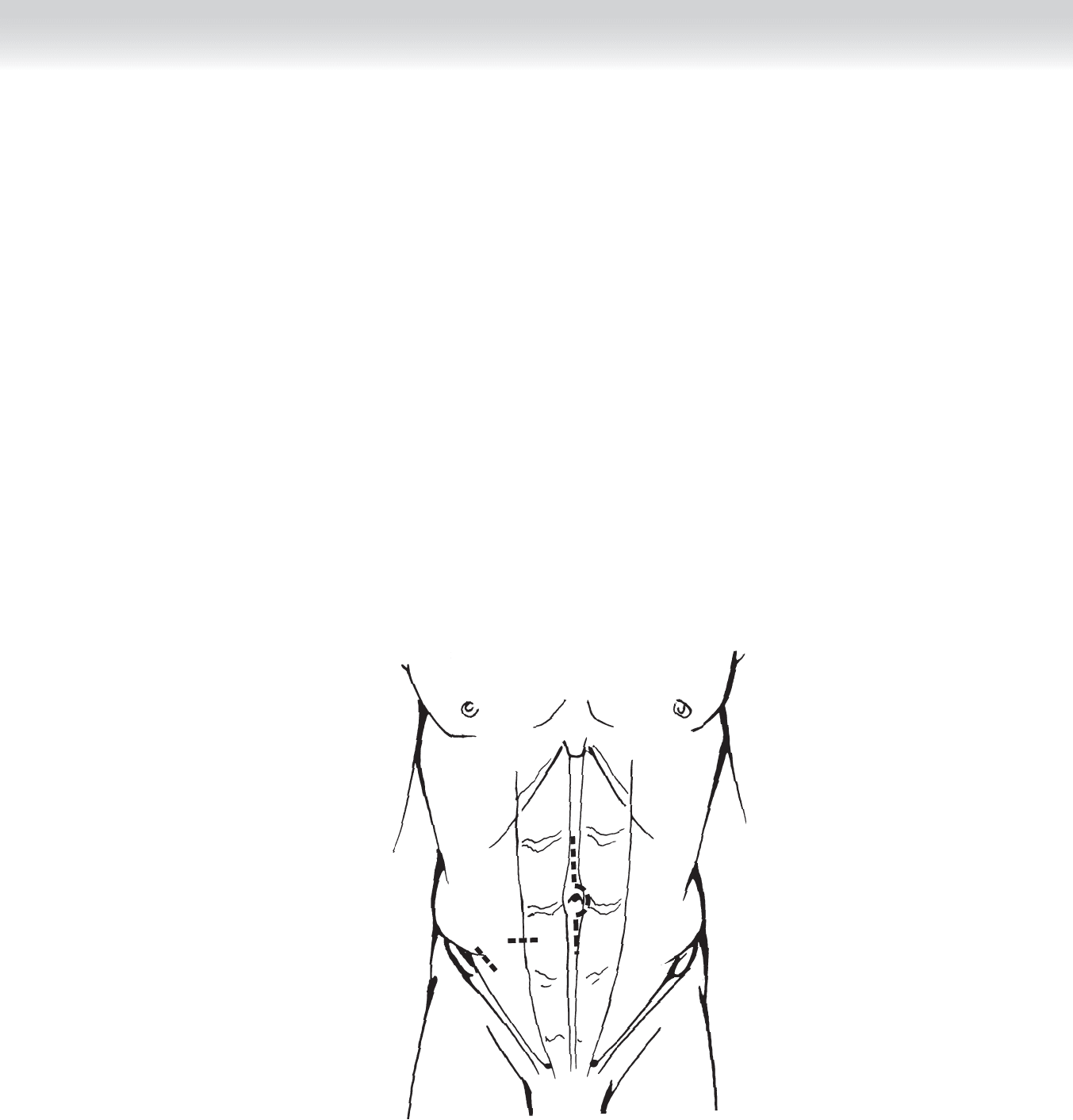
FIGURE 38 –1
CHAPTER 38 • Open Appendectomy 405
STEP 3: OPERATIVE STEPS
1. INCISION
◆ Identify the midpoint of a line between the umbilicus and right anterior-superior iliac
spine. Appropriate skin incision is made at this level (Figure 38-1).
◆ Electrocautery is used to dissect down to the fascia of the external oblique muscle, lateral to
the rectus abdominus muscle.
◆ The external oblique fascia is incised along the length of its fi bers and spread.
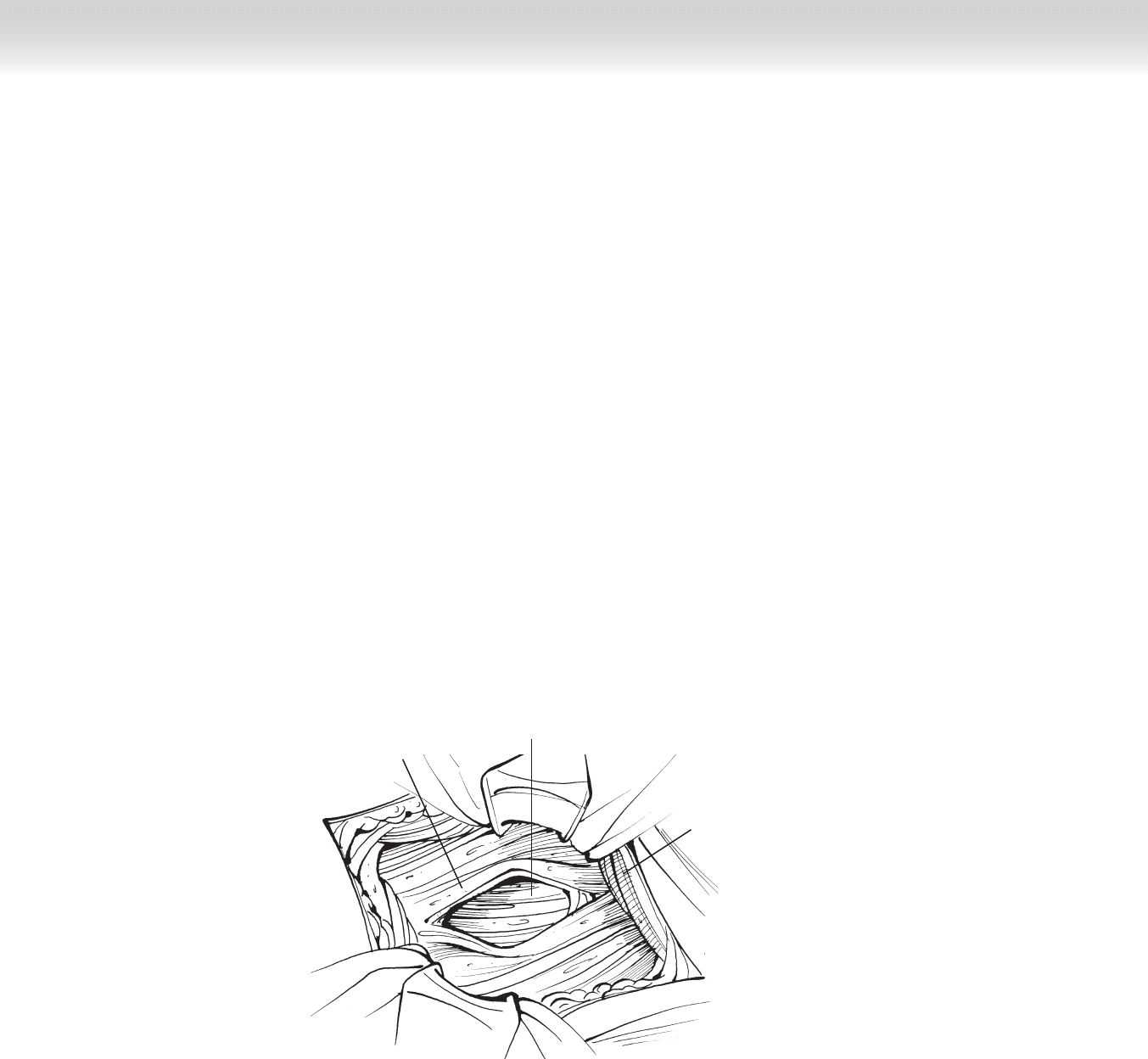
406 Section IV • T
HE ABDo MEN
◆ Blunt dissection can be used to separate the underlying internal oblique and transversus
abdominis muscles along the length of their fi bers in layers, as well (Figure 38-2).
◆ The peritoneum can then be cleaned off and incised.
◆ Peritoneal incision is typically done by elevating the peritoneum between two hemostats
and making sure no intra-abdominal contents have been trapped in the operative fi eld.
2. DISSECTION
◆ Once the peritoneum has been entered, the RLQ can be explored to identify the location of
the appendix and any associated pathologic fi ndings or abscess.
◆ The small intestine can be retracted medially, allowing identifi cation of the cecum.
FIGURE 38 –2
External
oblique muscle
Internal oblique
muscle split
Transversus
abdominis muscle
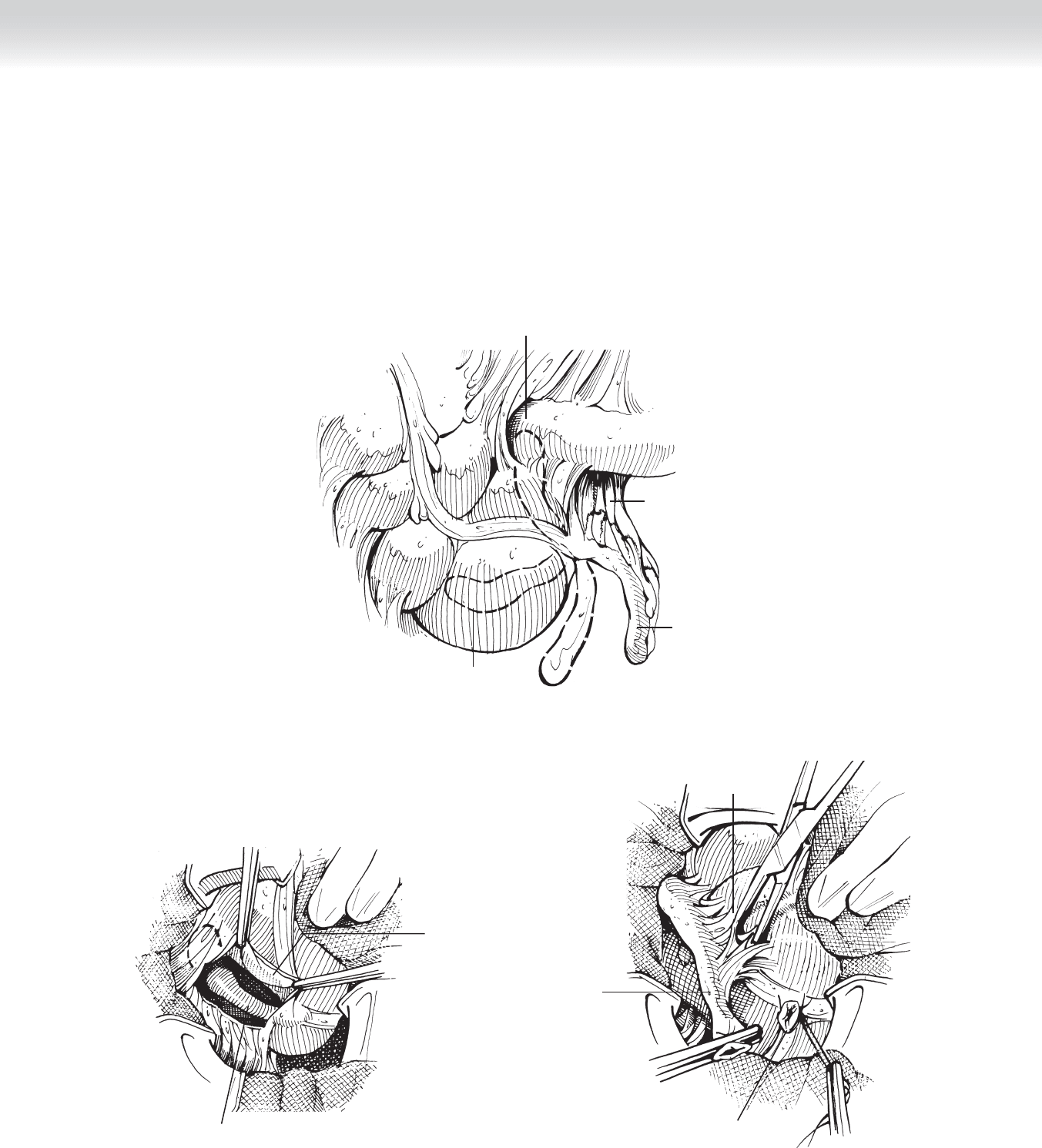
CHAPTER 38 • Open Appendectomy 407
Appendix
Mesoappendix
Ileocecal junction
Retrocecal appendix
FIGURE 38 –3
Retrocecal
appendix exposed
Peritoneal
reflection incised
A
Appendiceal
stump ligated
Paracecal
appendix
Dissection of
adhesions
B
FIGURE 38 –4
◆ The taeniae coli converge at the base of the appendix, allowing identifi cation of anatomic
landmarks that aid in its removal (Figure 38-3).
◆ Mobilization of the cecum by incision of the lateral, avascular attachments of the right
side of the colon may allow better visualization of a retrocecal appendix (Figure 38-4).

◆ The cecum and base of the appendix are brought out of the wound.
◆ The mesoappendix containing the appendiceal artery is divided and ligated down to the
serosa of the appendix where it joins the cecum (Figure 38-5).
◆ The appendiceal base is crushed at the proposed level of division, and the clamp released
and replaced distally. This creates a position to ligate the appendix (Figure 38-6, A).
◆ The appendiceal stump can be doubly ligated with slowly absorbing suture, or the appendix
can be singly ligated with rapidly absorbing suture if it is to be imbricated. The ligature is to
obliterate the lumen but not strangulate the short segment of appendix between the ligatures
(Figure 38-6, B).
◆ The mucosa of the appendiceal stump should be obliterated with electrocautery to prevent
accumulation of a mucocele.
◆ Purse-string suture around the appendiceal base or Z stitch can be used to secure the base
of the appendix, as well.
3. CLOSING
◆ Once hemostasis is ensured, the abdomen is closed in layers, starting with the peritoneum
(optional); if a muscle-splitting incision has been performed, the internal oblique and
transversus abdominis muscles require only loose approximation.
◆ More attention should be given to closure of the fascia of the external oblique muscle,
which will be a strength layer.
◆ In more corpulent patients, Scarpa’s fascia can be loosely approximated.
◆ If purulent appendicitis was found at exploration, the skin should be left open, or closed in
acute appendicitis.
◆ No intraperitoneal drains are indicated.
◆ Sterile dressings are applied.
Section IV • T
HE ABDo MEN
408