Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

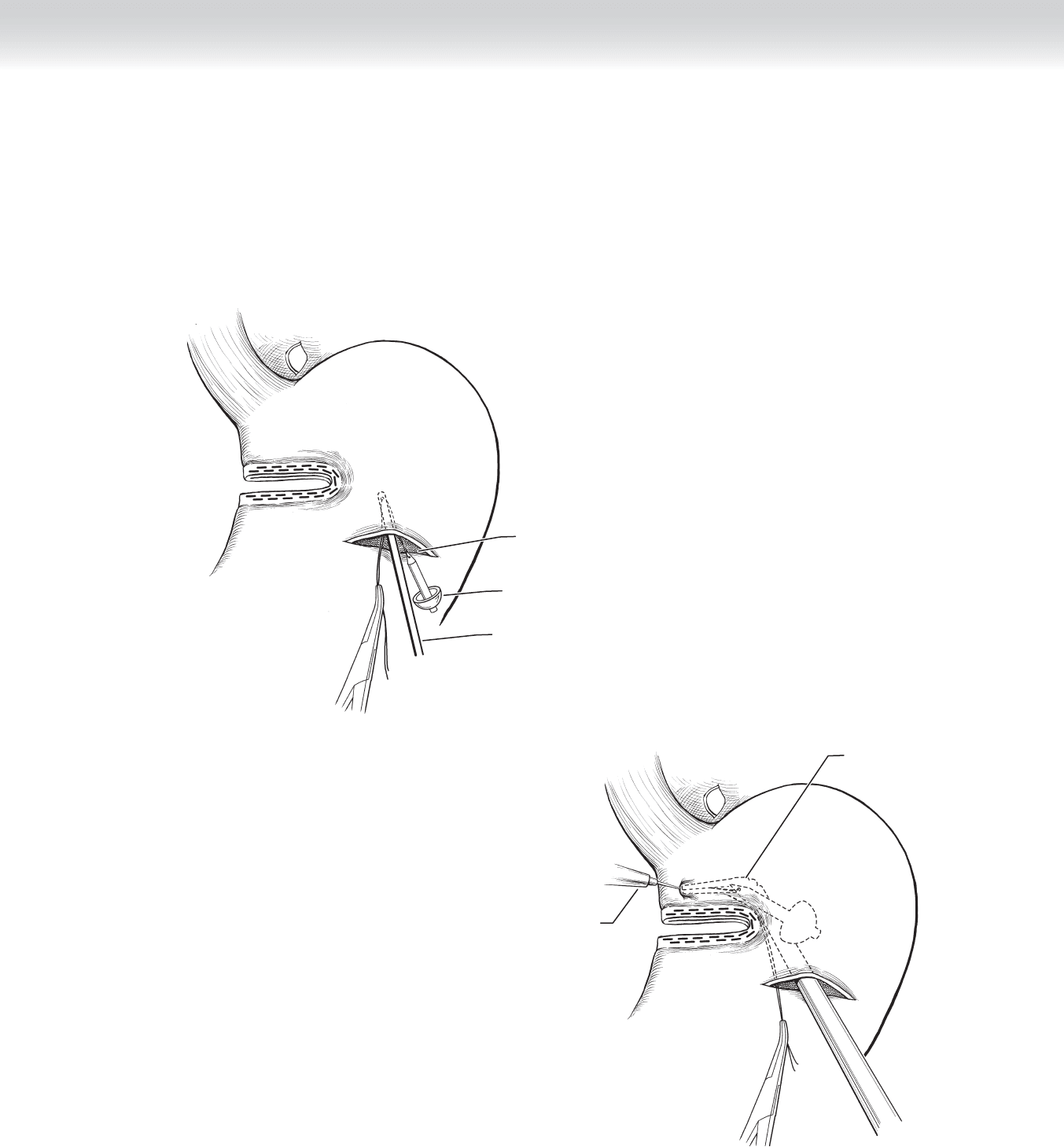
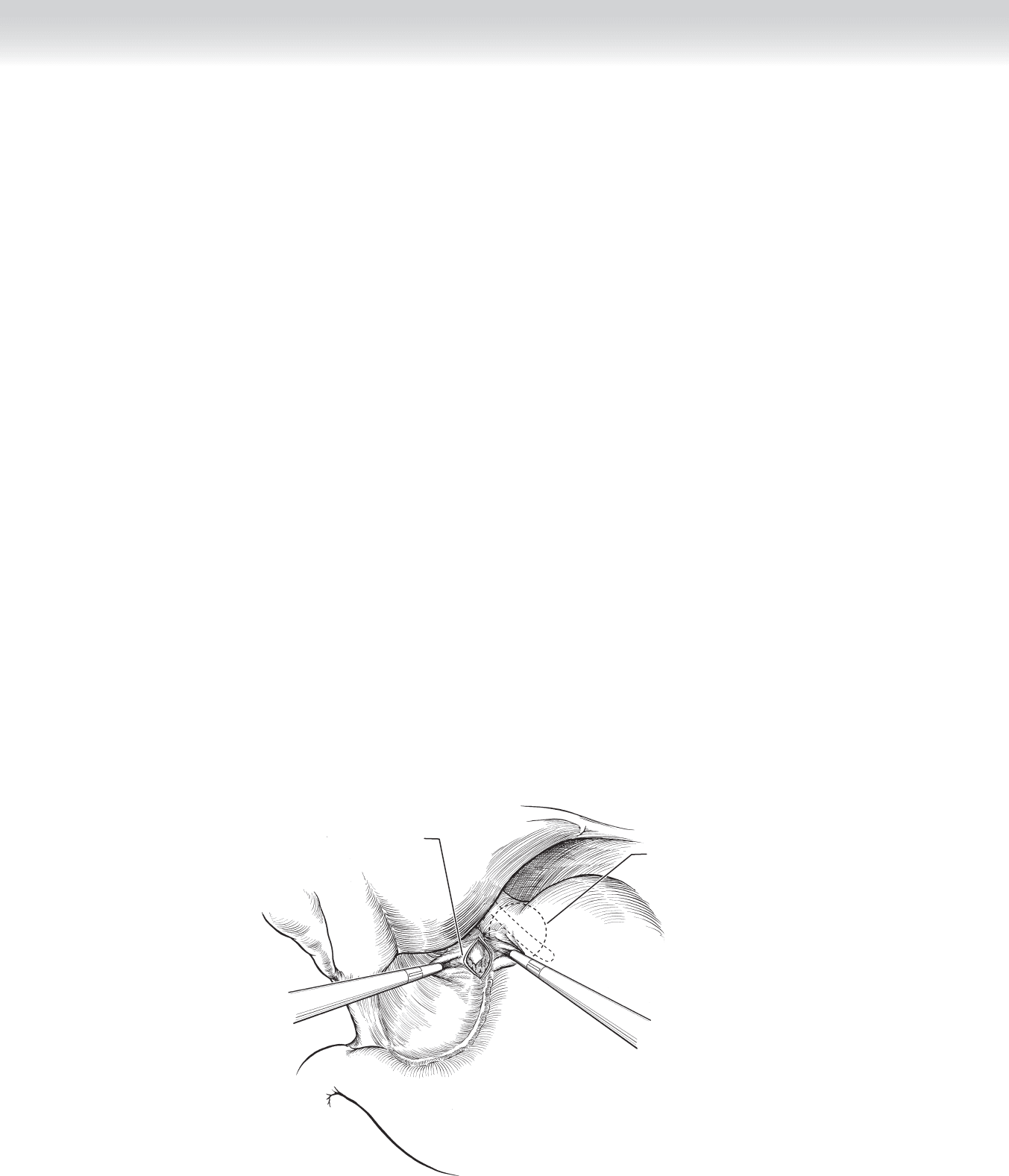
◆ The articulating dissector is placed through the gastrotomy and fl exed so that its tip tents
up the stomach at the staple line near the lesser curve. The cautery or ultrasonic dissector is
activated while touching the tip of the articulating dissector to create a gastrotomy only big
enough to pass the articulating dissector through it. The suture is then grasped, and once it
is pulled through the tiny gastrotomy, the articulating dissector is straightened and removed
(Figures 34-42 and 34-43).
Anvil
Gastrotomy
Band passer
FIGURE 34–42
Angled dissector
Bovie used to
create gastrotomy
FIGURE 34–43
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
379
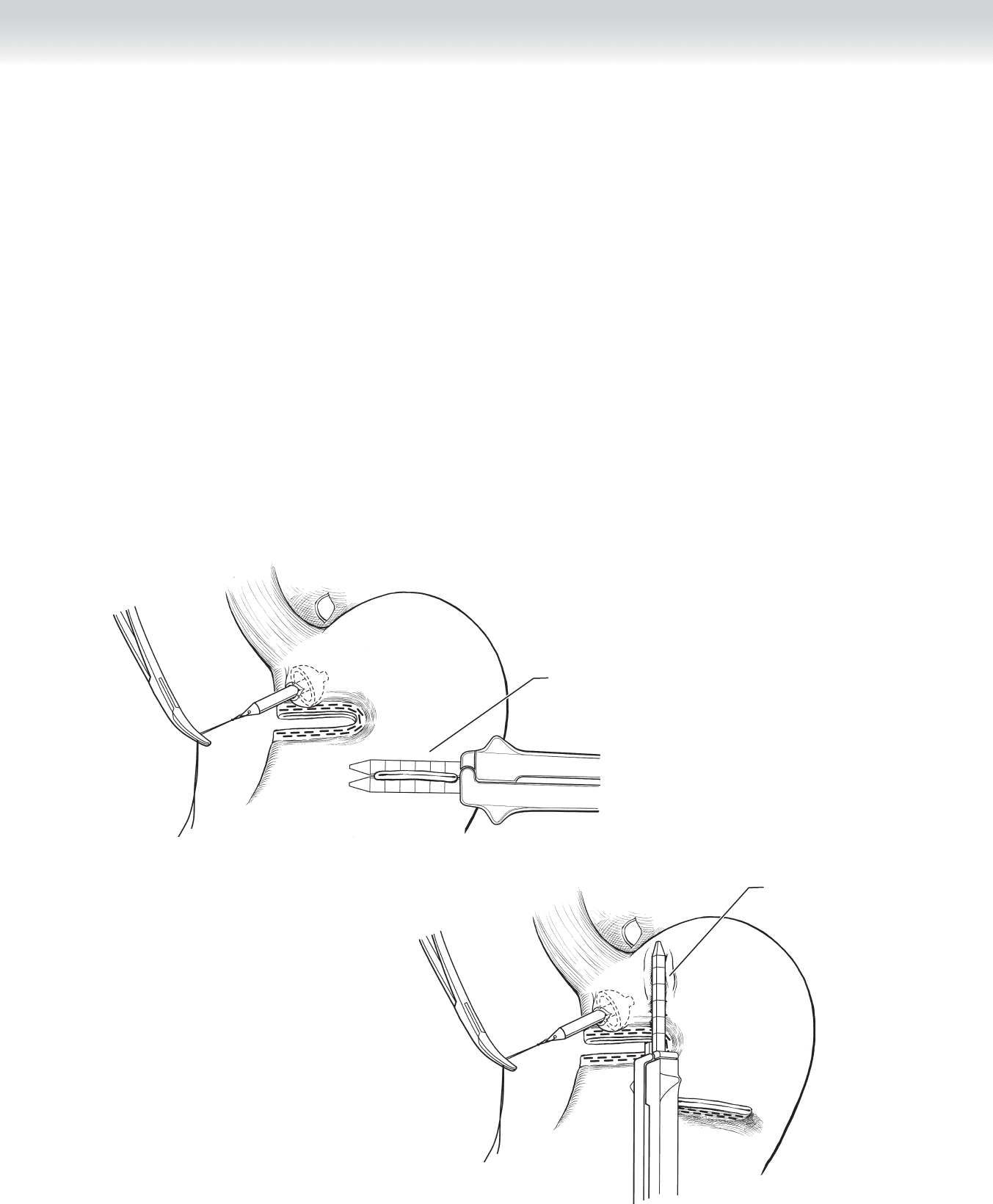
◆ Once the anvil is in position, the original gastrotomy is closed with the linear stapler
containing 3.5-mm staples (Figure 34-44).
◆ The 60-mm linear stapler with 3.5-mm staple height is applied to the stomach paralleling
the lesser curve. Downward traction on the suture on the anvil facilitates proper placement.
Before fi ring the stapler, the orogastric tube is advanced until it can be certain that it is visible
within the pouch and not within the main body of the stomach or caught by the stapler. This
is repeated until the surgeon is certain the pouch has been completely separated from the
main body of the stomach (Figure 34-45).
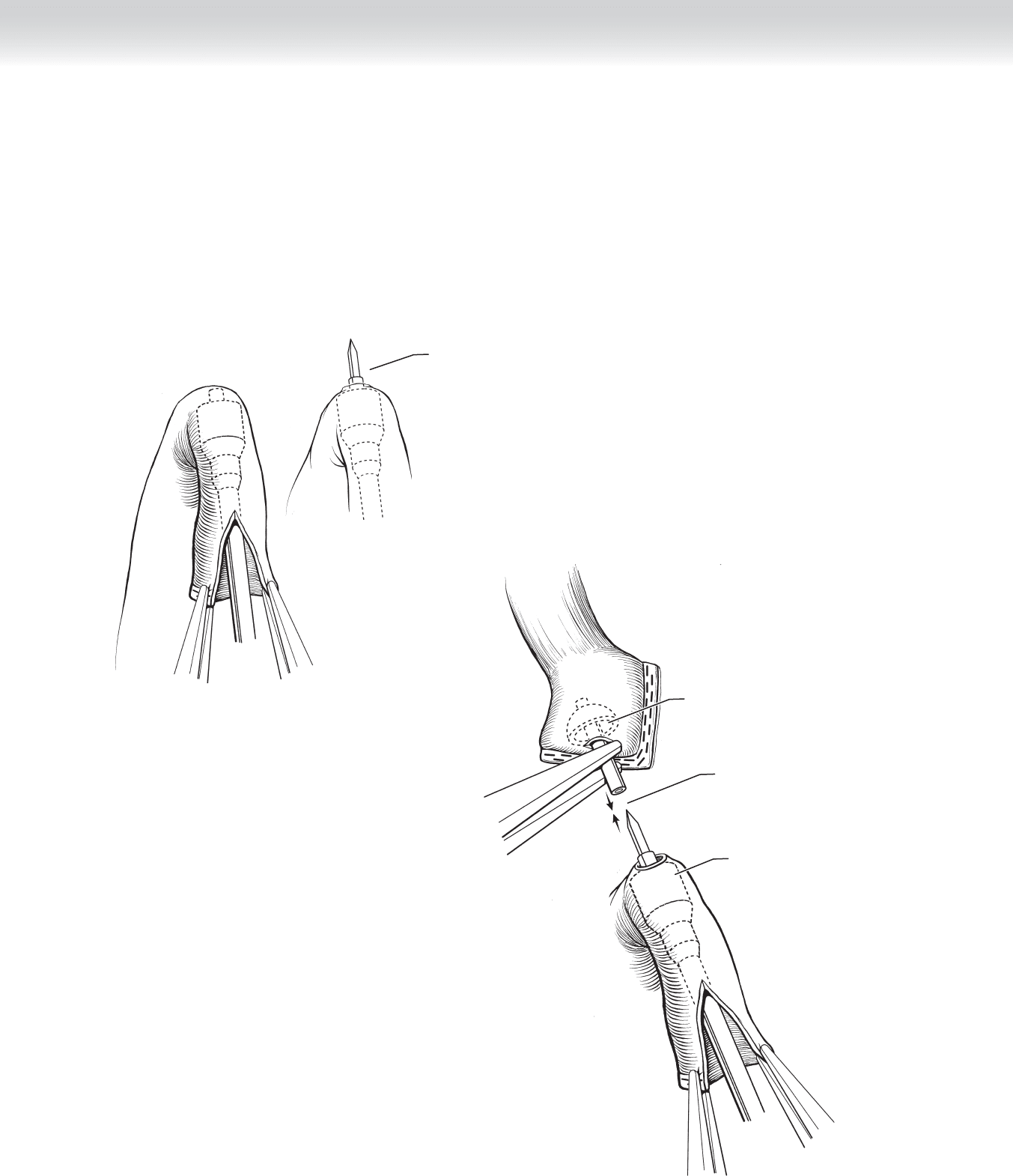
◆ The spike is removed and discarded (Figure 34-46).
◆ The jejunal Roux limb is opened longitudinally on its end (Figure 34-47).
◆ The circular stapler is placed into the lumen of the Roux limb (Figure 34-48).
Closing gastrotomy
with stapler
FIGURE 34–44
Begin completion
of pouch with stapler
FIGURE 34–45
Section IV • The Abdomen380

Applying a one-quarter turn,
trocar is removed from anvil
Stomach pouch
FIGURE 34–46
Inserting circular stapler
into Roux limb lumen
FIGURE 34–48
Open staple line
FIGURE 34–47
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
381
382 Section IV • The Abdomen
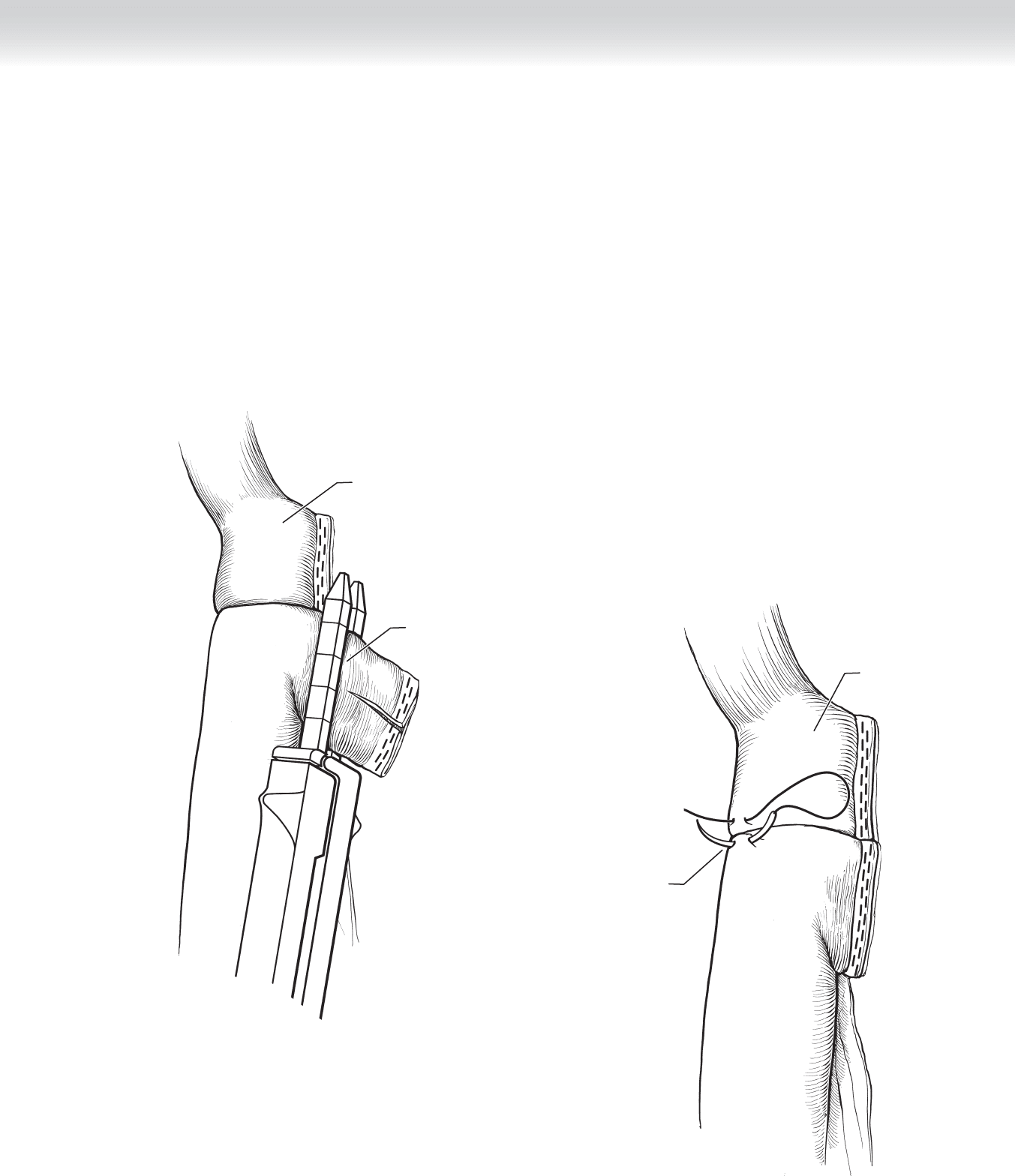
◆ Once past the demarcated segment, the stapler is opened to pierce the antimesenteric
border (Figure 34-49).
◆ The stapler and anvil are mated together, and the instrument is closed and fi red. The stapler
is partially opened and removed (Figure 34-50).
Piercing through
antimesenteric border
of jejunum
FIGURE 34–49
Mating together
circular stapler
and anvil
Circular stapler
Anvil
FIGURE 34–50
CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
383
◆ The redundant open segment of jejunum is trimmed and sealed by fi rst incising the mesen-
tery and then applying the linear stapler with 2.5-mm staples. Before fi ring the stapler, the
orogastric tube should be passed through the gastrojejunostomy for the subsequent leak
check (Figure 34-51).
◆ A seromuscular stitch of 2-0 Vicryl is placed at the right side of the gastrojejunostomy
(Figure 34-52).
◆ The leak check and placement of the closed suction drain complete the operation.
Cutting away
jejunal excess
Stomach pouch
FIGURE 34–51
Pouch
One seromuscular
suture
FIGURE 34–52

384 Section IV • The Abdomen
3. CLOSURE
◆ Interrupted #2 Vicryl sutures are used to close the abdominal fascia, and the skin is closed
with staples after thorough irrigation.
STEP 4: POSTOPERATIVE CONSIDERATIONS
◆ Telemetry and pulse oximetry monitoring should be strongly considered for several hours
postoperatively in these high-risk patients.
◆ Ambulation within the fi rst 2 hours of emergence from anesthesia should help prevent
venous thrombosis. Patients appropriately educated preoperatively will be anxious to get up
out of bed.
STEP 5: PEARLS AND PITFALLS
◆ A thorough preoperative educational program is the best way to achieve the lowest risk of
perioperative complications and highest patient compliance.
◆ Venous thrombosis and gastrointestinal leaks are among the most lethal perioperative com-
plications, and surveillance for them is important.
◆ Despite prophylaxis with ambulation, sequential compression devices, and low-molecular-
weight heparin, the risks of deep venous thrombosis and pulmonary embolism are still
signifi cant.
◆ Intraoperatively, a simple and quick way to test the integrity of the gastrojejunostomy is
to occlude the Roux limb with an atraumatic instrument, fl ood the upper abdomen with
saline, and inject boluses of air through the orogastric tube. Bubbles of air when present
should be traced to their source to reinforce the staple line with Vicryl sutures. This proce-
dure can also be performed with methylene blue injection through the orogastric tube.

CHAPTER 34 • Roux-en-Y Gastric Bypass (Open and Laparoscopic)
385
◆ Another way to detect leaks in the early postoperative period is to place a closed suction
drain at the gastrojejunostomy under the left lateral segment of the liver. This also helps
protect against the progression of gastrojejunal leaks to peritonitis and abscess.
◆ Finally, consideration should be given to a contrast swallow with fl uoroscopy before allow-
ing any oral intake to screen for early postoperative leaks.
SELECTED REFERENCE
1. Brolin RE: The antiobstruction stitch in stapled Roux-en-Y enteroenterostomy. Am J Surg 1995;169:
355-357.

386
STEP 1: SURGICAL ANATOMY
◆ Experience with the anatomy and a surgical procedure of the esophagogastric junction is a
prerequisite to a successful gastric banding operation (see Figure 34-1).
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The standard indications for a bariatric operation include either a body mass index of at
least 40 kg/m
2
or a body mass index of at least 35 kg/m
2
with signifi cant associated medical
illness. Potential patients must also have tried multiple dietary, activity, and lifestyle modifi -
cation programs. They should be free of substance abuse and be psychologically stable so
that they can make an intelligent decision regarding the risks of the operation and the need
to dramatically alter their lifestyles. The indications for banding are the same as the indica-
tions for gastric bypass.
◆ Bariatric operations should not be offered unless a dedicated team is in place for the
thorough preoperative evaluation and close long-term follow-up that are required for every
patient.
◆ Banding is considered the safest of all the bariatric operations.
◆ Twenty percent to 40% of patients getting an adjustable gastric band will need to have a hi-
atal hernia repair. Small but signifi cant hiatal hernias can be missed on preoperative studies.
These are often not diagnosed until the intraoperative test, so the surgeon must be prepared
for this inevitable situation.
◆ Patients should receive prophylaxis against wound infection with an intravenous cephalo-
sporin and against venous thrombosis with sequential compression devices and low-
molecular-weight heparin before induction of anesthesia.
CHAPTER
35
Laparoscopic Placement
of Adjustable Gastric Band
(Pars Flaccida Approach)
Michael D. Trahan

C HAPTER 35 • Laparoscopic Placement of Adjustable Gastric Band 387
◆ Each incision site is preemptively anesthetized with local anesthetic injection.
◆ General anesthesia is required for this operation. An anesthesia team specially trained and
equipped for the morbidly obese patient is necessary.
◆ There are currently two devices with approval from the U.S. Food and Drug Administration
(FDA) for use in the United States. There are several others being used internationally. The
techniques for insertion may differ slightly, but the principles are the same.
◆ Use of the devices requires a formal education and offi cial proctoring process before the
bands are made available to the surgeon. This description is not meant to substitute for that
qualifi cation process.
STEP 3: OPERATIVE STEPS
1. INCISIONS
◆ Five small incisions are made as diagrammed. Initial entry is made using a 5-mm optically
guided bladeless trocar at the left costal margin in the midclavicular line—this will be the
main telescope port. The peritoneal cavity is insuffl ated and the remaining ports are placed
under direct internal visualization. The liver retractor is inserted near the xiphoid process.
A 5-mm trocar is placed on either side of the midline to be used as the surgeon’s working
ports. A 15-mm trocar is placed below the left costal margin near the anterior axillary line.
The assistant will use this port to expose the esophagogastric area (Figure 35-1).
MC
Surgeon
Assistant
FIGURE 35 –1
2. DISSECTION
◆ The orogastric calibration tube is inserted and watched as it enters the stomach. The bal-
loon is infl ated with 15 mL of air or water. The tube is pulled back to identify and test the
integrity of the esophagogastric junction. If the balloon slips up into the mediastinum, a
hiatal repair should be performed, usually by mobilization of the anterior aspect of the dis-
tal esophagus and suturing the anterior aspect of the hiatus. A larger hiatal hernia may re-
quire a posterior repair. Once the balloon confi rms adequate hiatal repair, it is defl ated, and
the tube is removed.
◆ The pars fl accida is the clear membrane covering the caudate lobe and running between the
lesser curvature of the stomach and the liver. This membrane is bluntly opened (Figure 35-2).
◆ The assistant grasps the fat along the lesser curvature and retracts it to the patient’s left.
This maneuver exposes the right crus of the diaphragm, which should be carefully distin-
guished from the inferior vena cava. The peritoneum covering the fat just anterior to the
lower aspect of the right crus is bluntly opened just enough to allow passage of the 5-mm
articulating dissector. The dissector is placed through this opening and should pass without
the slightest resistance behind the stomach aiming toward the angle of His (Figure 35-3).
◆ The band is selected and prepared according to the manufacturer’s specifi cations. The band
and tubing are inserted through the 15-mm trocar by grasping the tip of the band buckle
and pushing the device through the trocar with the band fi rst. The grasper then releases the
band, and the tubing is gently grasped and fed through the trocar, as well. The tip of the
tubing is grasped before inserting the tubing all the way through the trocar. The tip of the
tube is grasped by the retrogastric grasper or, if using a band passer, fed through the eye at
the tip of the instrument (Figure 35-4).
Opening pars flaccida
15 mL fluid
insufflated in
intragastric balloon
FIGURE 35 –2
Section IV • The Abdomen388