Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

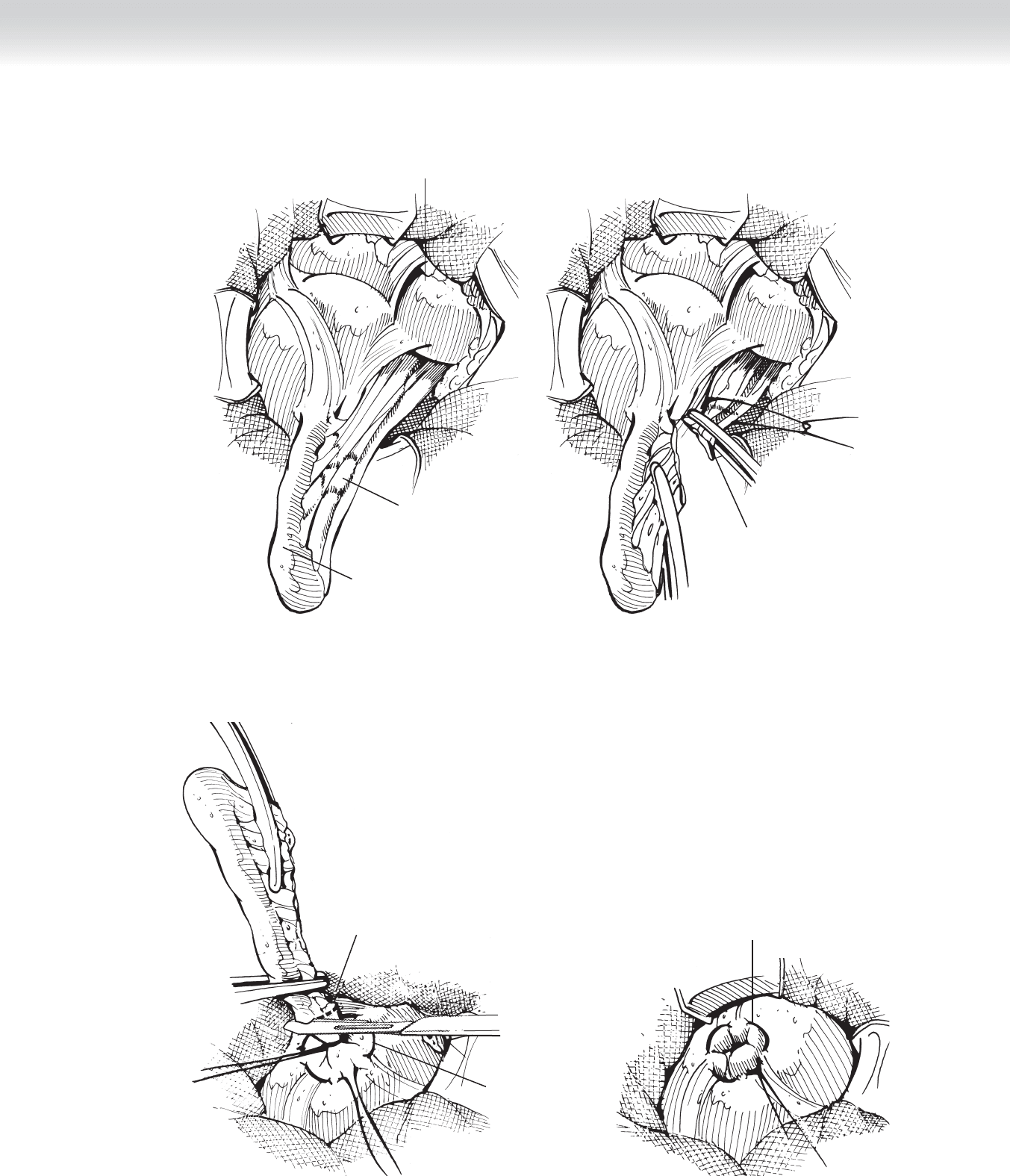
A
Appendix
Mesoappendix
Ileocecal junction
Mesoappendix divided
and appendiceal artery
ligated
B
FIGURE 38 –5
A
Purse-string suture
in cecum
Ligature tied and
appendix divided
at its base
Appendiceal stump invaginated
and purse-string suture tied
B
FIGURE 38 –6
CHAPTER 38 • Open Appendectomy 409

410 Section IV • T
HE ABDo MEN
STEP 4: POSTOPERATIVE CARE
◆ Dietary resumption may begin immediately in the case of acute appendicitis, but if free
purulence was found at operation, postoperative ileus mandates awaiting the return of
bowel function.
◆ Postoperative antibiotics are not necessary in acute appendicitis but should be continued in
the presence of intra-abdominal purulence.
STEP 5: PEARLS AND PITFALLS
◆ Placement of the skin incision slightly cephalad to the anticipated position of the appendix
in its anatomic position will allow easier manipulation of the cecum, once brought out of
the RLQ wound.
◆ Despite preoperative evaluation, a missed diagnosis (normal appendix at exploration) should
include a search for the underlying pathologic condition, including perforated duodenal
ulcer, pancreatitis, urinary tract infections or calculi, gynecologic pathologic fi ndings, or
Meckel’s diverticulum.
SELECTED REFERENCES
1. Silen W, Cope Z: Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. New York, Oxford University
Press, 2005, pp 67-83.
2. Lally KP, Cox CS Jr, Andrassy R: The appendix. In Townsend CM, Beauchamp RD, Evers BM, Mattox KL
(eds): Sabiston Textbook of Surgery, 17th ed. Philadelphia, Saunders, 2004, pp 1381-1399.

411
STEP 1: SURGICAL ANATOMY
◆ Intussusceptions in infants and toddlers occur as a result of invagination of proximal bowel
(intussusceptum) into the lumen of the distal bowel (intussuscipiens). It typically involves
the ileocolic region of the intestine with variable degree of colonic involvement. The leading
point of the intussusception is typically a Peyer’s patch in the terminal ileum. Occasionally,
Meckel’s diverticulum may be the leading point of the intussusception.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Sudden, intermittent, colicky, severe abdominal pain associated with calm, asymptomatic
periods in a toddler is characteristic. It is commonly associated with a history of preceding
upper respiratory tract infections. A jelly stool is another characteristic of this condition.
◆ Abdominal radiographs may demonstrate paucity of bowel gas in the right lower quadrant
along with soft tissue mass in the upper abdomen representing an intussusceptum.
◆ When the diagnosis is suspected, hydration status along with presence of acute abdomen
(peritonitis, perforation, or obstruction) should be assessed. Ultrasound examination can
identify the presence of an intussusception.
◆ Contrast (or air) enema study can confi rm diagnosis and also potentially be therapeutic.
Hydrostatic or pneumatic reduction of intussusception is successful in approximately 60%
to 95% of cases. A history longer than 24 hours or radiologic evidence of bowel obstruction
signifi cantly reduces the likelihood of successful reduction by enema.
◆ Contrast is instilled through a catheter from a reservoir 100 cm above the patient. Air is
delivered at 80 to 150 mm Hg. The criterion for successful reduction is refl ux of contrast
or air into the terminal ileum.
◆ After a successful reduction, the child is observed overnight to ensure complete resolution
of symptoms and absence of recurrence.
CHAPTER
39
Intussusception
Dai H. Chung
412 Section IV • The Abdomen
STEP 3: OPERATIVE STEPS
1. INCISION
◆ Operative reduction is necessary for failed enema reduction and/or multiple recurrent
intussusceptions.
◆ Preoperative prophylactic intravenous antibiotic should be administered 30 minutes before
skin incision.
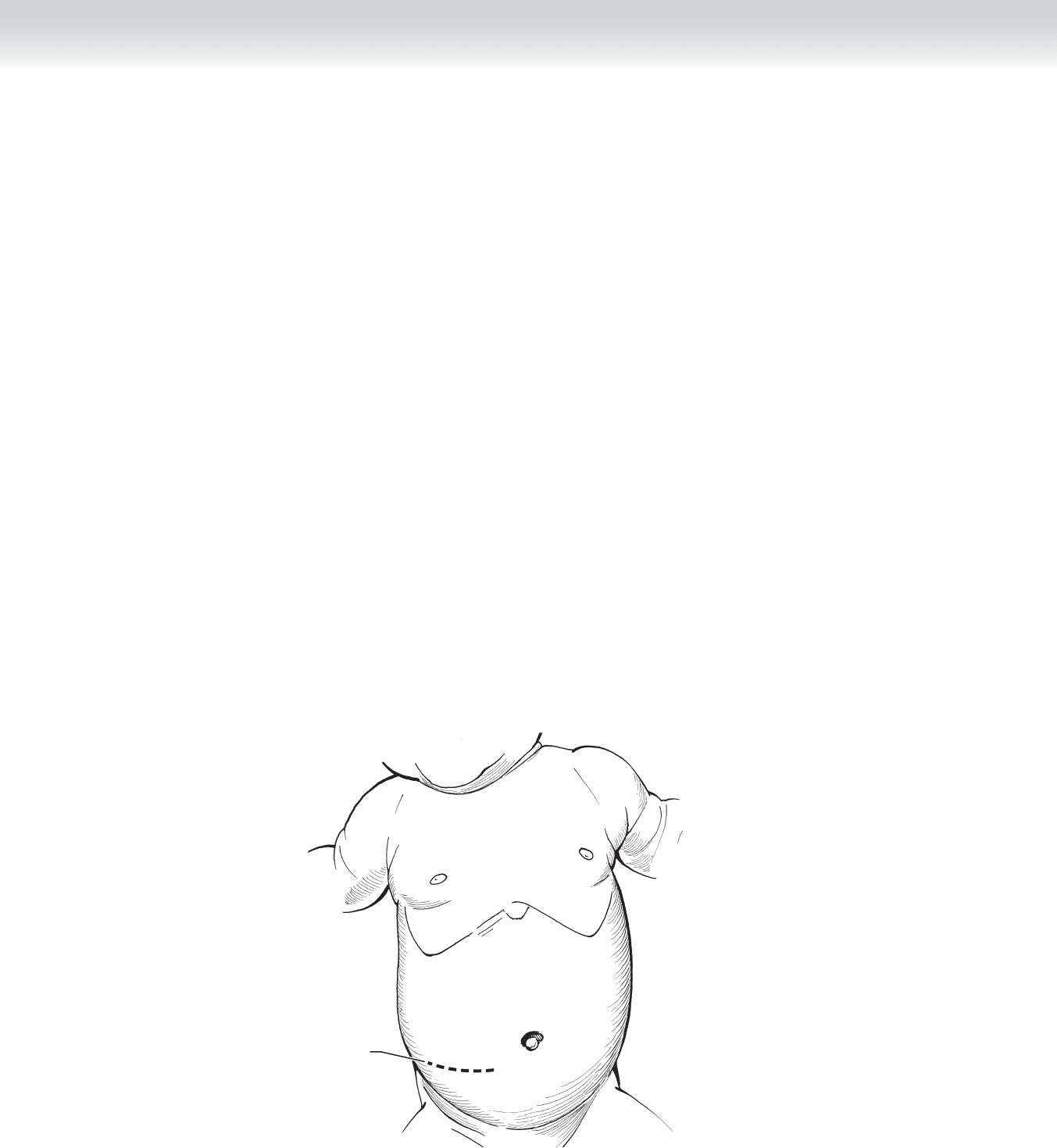
◆ Patient is positioned supine and the right-sided transverse abdominal skin incision is made
slightly inferior to the umbilicus (Figure 39-1). Depending on the degree of intussuscep-
tion, the incision may be made at the level of or above the umbilicus.
2. DISSECTION
◆ Muscle-splitting technique is used to dissect through external, internal oblique, and trans-
versalis fascia.
Incision
J. Smith
FIGURE 39 –1
CHAPTER 39 • Intussusception 413
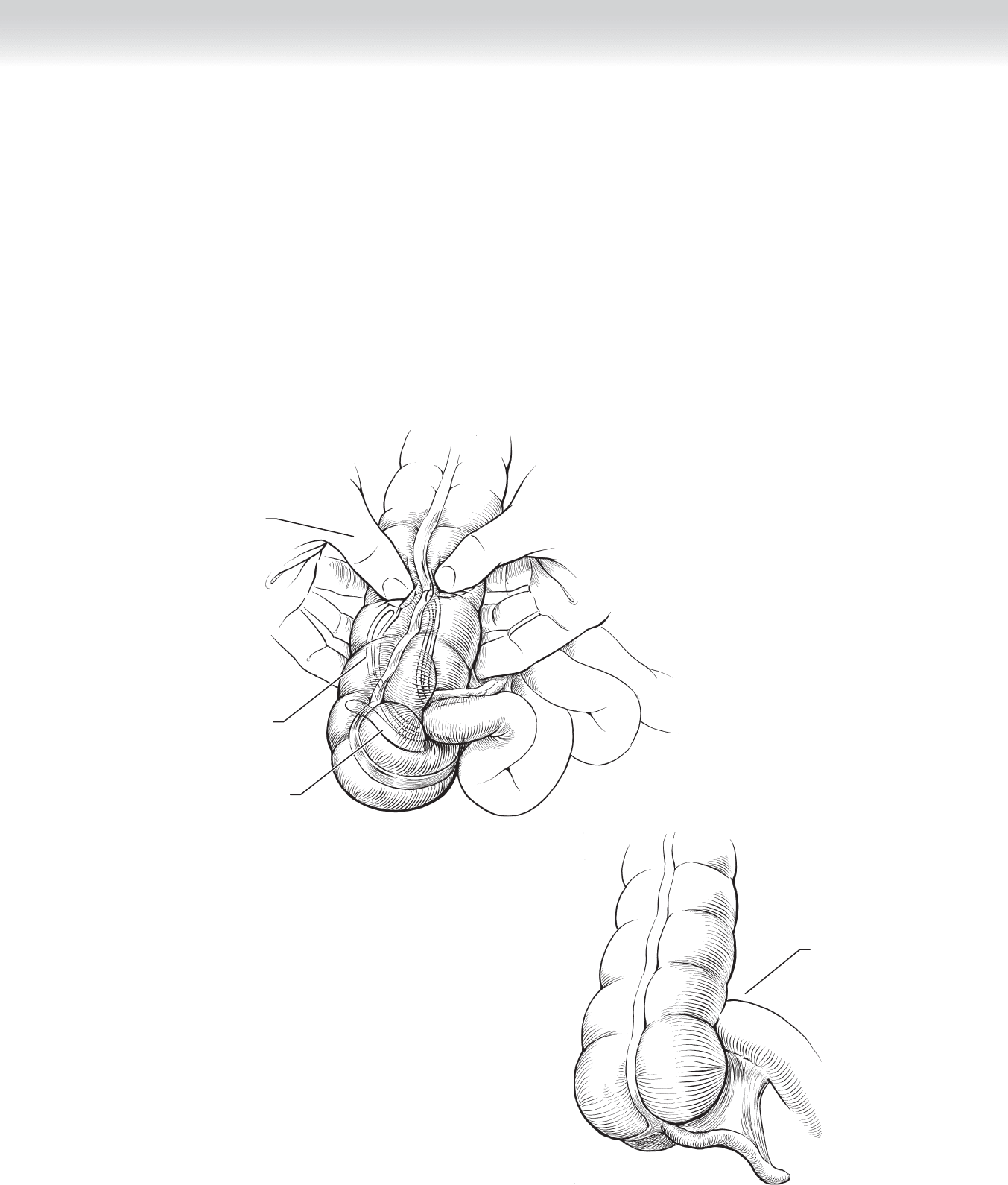
Invaginated ileum
within colon
M. Cooley
after J. Smith
Appendix
within colon
Milking ileum
out of the colon
FIGURE 39 –2
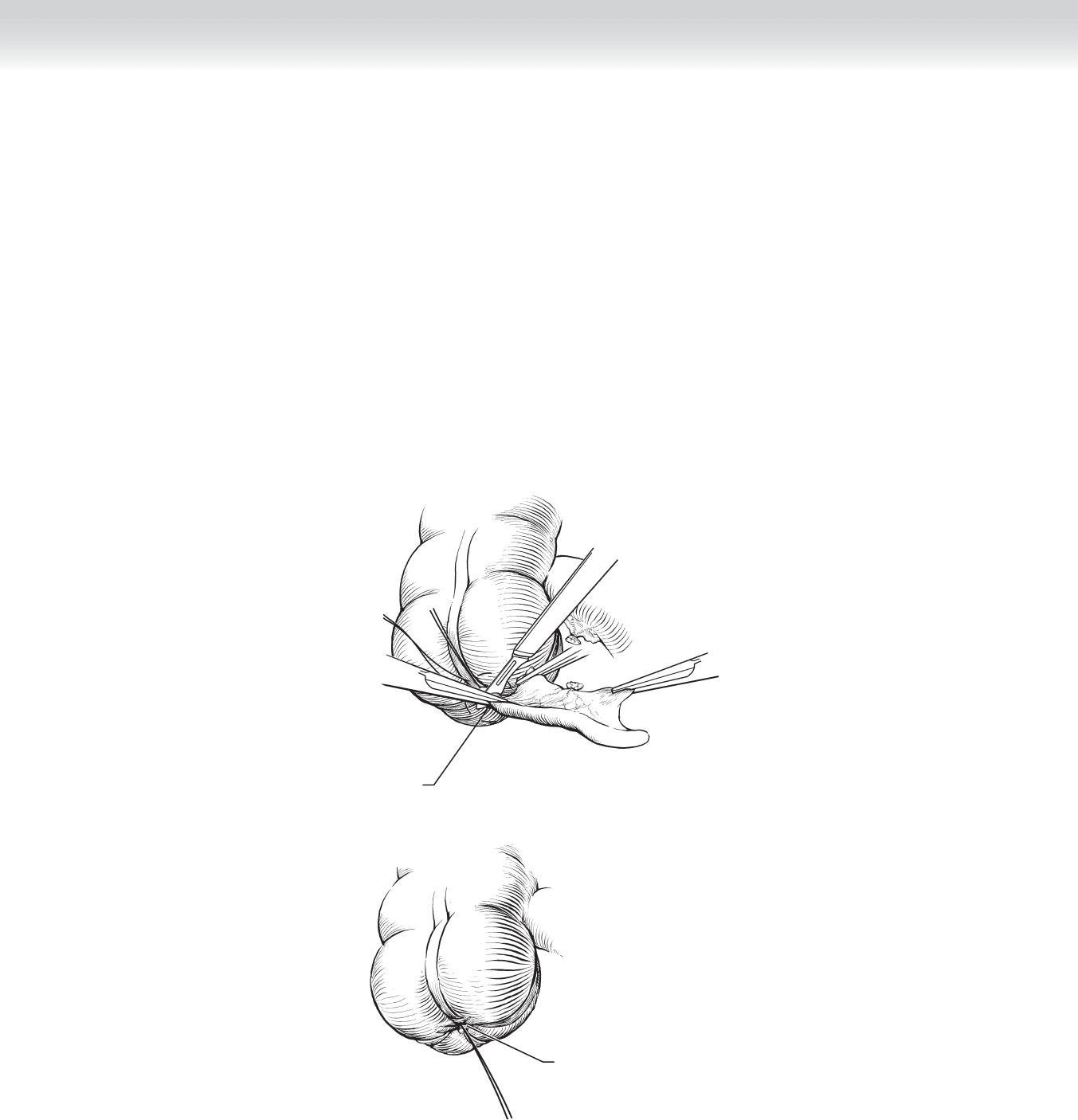
MC
Reduced ileum
FIGURE 39 –3
◆ Bowel loops of intussusception are carefully delivered into the wound and reduction is
achieved by gently squeezing the bowel distal to the apex along with gentle pull of proximal
bowel to aid with the reduction (Figure 39-2). Traction or strong pulling of intussuscepted
bowel should be avoided, because this can easily result in further injury to the bowel.
◆ After reduction, general condition of the intussuscepted terminal ileum should be assessed
carefully (Figure 39-3). Occasionally, segmental bowel resection is necessary if reduction
cannot be achieved or necrotic bowel is identifi ed after reduction. Commonly, reduced
terminal ileum appears dusky and thickened to palpation. Placement of a warm, moist
sponge for a few minutes can improve local tissue perfusion, thus, potentially avoiding
unnecessary surgical resection.
414 Section IV • The Abdomen
◆ Standard appendectomy should be performed if the adjacent cecal wall is normal
(Figure 39-4). In general, inversion appendectomy is not recommended.
3. CLOSING
◆ Once reduction is achieved or resection performed (if required) and hemostasis is ensured,
abdominal fascia closure is performed in layers using 3-0 absorbable sutures in continuous
manner.
◆ The skin is reapproximated with a subcuticular stitch of 5-0 absorbable suture.
A
Appendix cut
anterior to purse string
and posterior to clamp
B
Appendectomy
complete
FIGURE 39 –4

CHAPTER 39 • Intussusception 415
STEP 4: POSTOPERATIVE CARE
◆ Nasogastric tube decompression is necessary if there were symptoms of bowel obstruction
preoperatively.
◆ The patient may be started on an oral clear liquid diet with return of bowel function and
gradually advanced to regular diet.
◆ Two postoperative doses of an intravenous antibiotic are administered.
STEP 5: PEARLS AND PITFALLS
◆ Recognition of acute abdomen is critical to prompt surgical management and to avoid un-
safe delays and risks to patients with attempts of enema reduction.
◆ Intussusception should be reduced by pushing the involved bowel retrogradely, with only
gentle pull if necessary.
SELECTED REFERENCES
1. DiFiore JW: Intussusception. Semin Pediatr Surg 1999;8:214-220.
2. Shehata S, El Kholi N, Sultan A, El Sahwi E: Hydrostatic reduction of intussusception: Barium, air or
saline. Pediatr Surg Int 2000;16:380-382.

416
STEP 1: SURGICAL ANATOMY
◆ In patients without malrotation, a broad mesentery and attachments at the cecum and
ascending and descending colon prevent volvulation of the small bowel around the superior
mesenteric vessels (Figure 40-1). Incomplete rotation of the intestine during fetal develop-
ment results in lack of these attachments, a very narrow mesentery, and peritoneal bands
(Ladd’s bands) that place the cecum close to the duodenum. This incomplete rotation may
cause obstruction in the second or third portions of the duodenum (Figure 40-2). The
absence of peritoneal attachments, in combination with a narrow mesentery and a relatively
fi xed point to the duodenocecal area, creates the conditions in which the midgut can volvu-
late (in clockwise fashion) around the superior mesenteric vessels (Figure 40-3). Although
most patients present in the neonatal period or in the fi rst year of life with bilious vomiting,
this condition may remain asymptomatic until adulthood.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ In children younger than 1 year of age, however, bilious vomiting must be considered due
to malrotation until proven otherwise. The diagnosis is confi rmed by upper gastrointestinal
series, barium enema, or sonography. Once this condition is diagnosed, surgical correction
should always be treated as an emergency.
◆ In the presence of midgut volvulus, time is of the essence. Vigorous intravenous resuscita-
tion and broad-spectrum antibiotics are initiated. The stomach is decompressed with an
orogastric tube, and a urinary catheter is placed to measure urine output. The operation
should not be delayed in an attempt to correct metabolic imbalances, because this is usually
futile until the volvulus is managed.
◆ After thorough gastric suctioning, general endotracheal anesthesia is induced with the patient
supine. The abdomen is prepped with povidone-iodine (Betadine) solution.
CHAPTER
40
Correction of Malrotation
with Midgut Volvulus
Carlos A. Angel
CHAPTER 40 • Correction of Malrotation with Midgut Volvulus 417
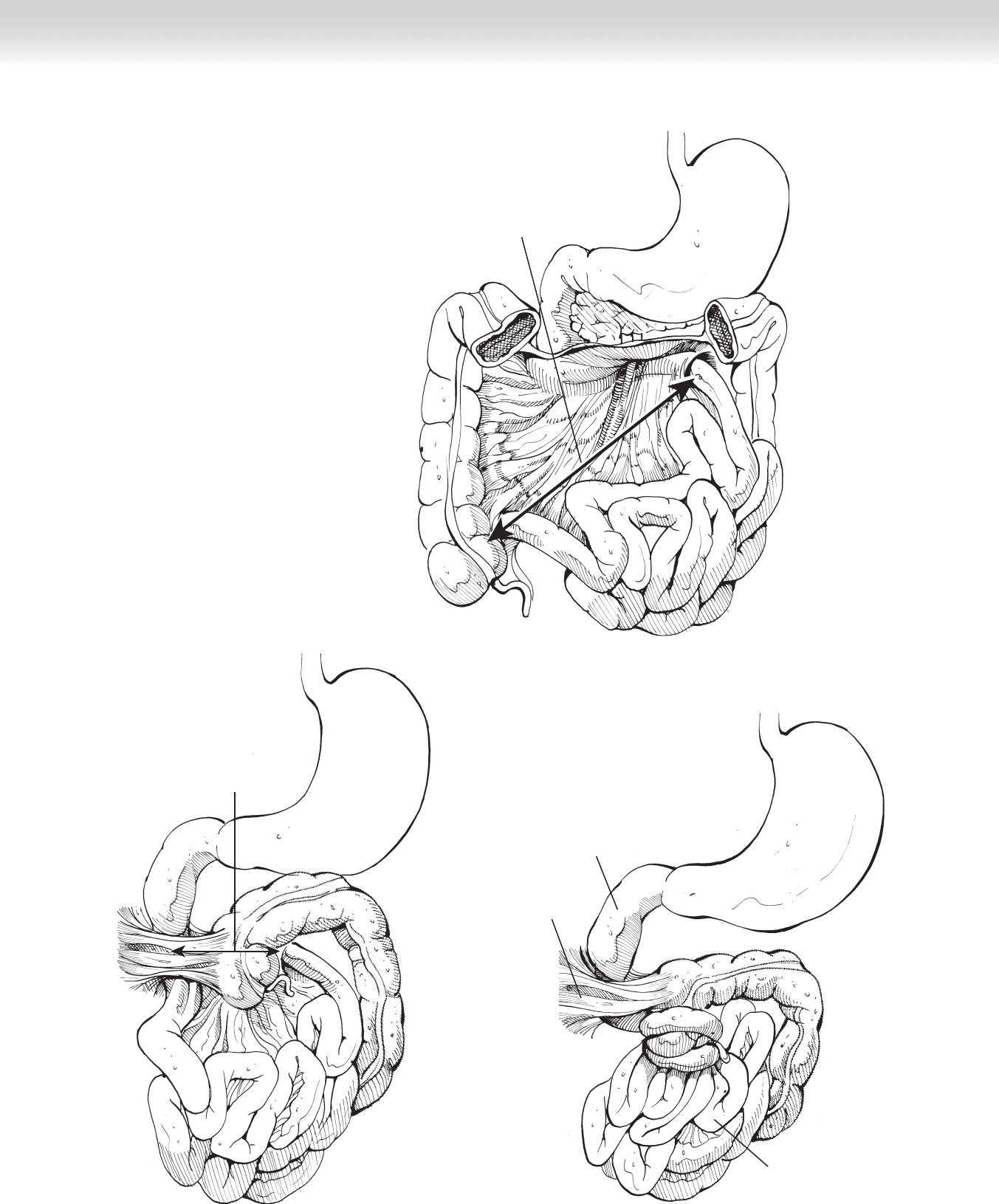
Broad axis
inhibits volvulus
FIGURE 40 –1
Short axis with
potential for volvulus
FIGURE 40 –2
Volvulus
Duodenum
Ladd's
bands
FIGURE 40 –3
418 Section IV • The Abdomen
STEP 3: OPERATIVE STEPS
1. INCISION
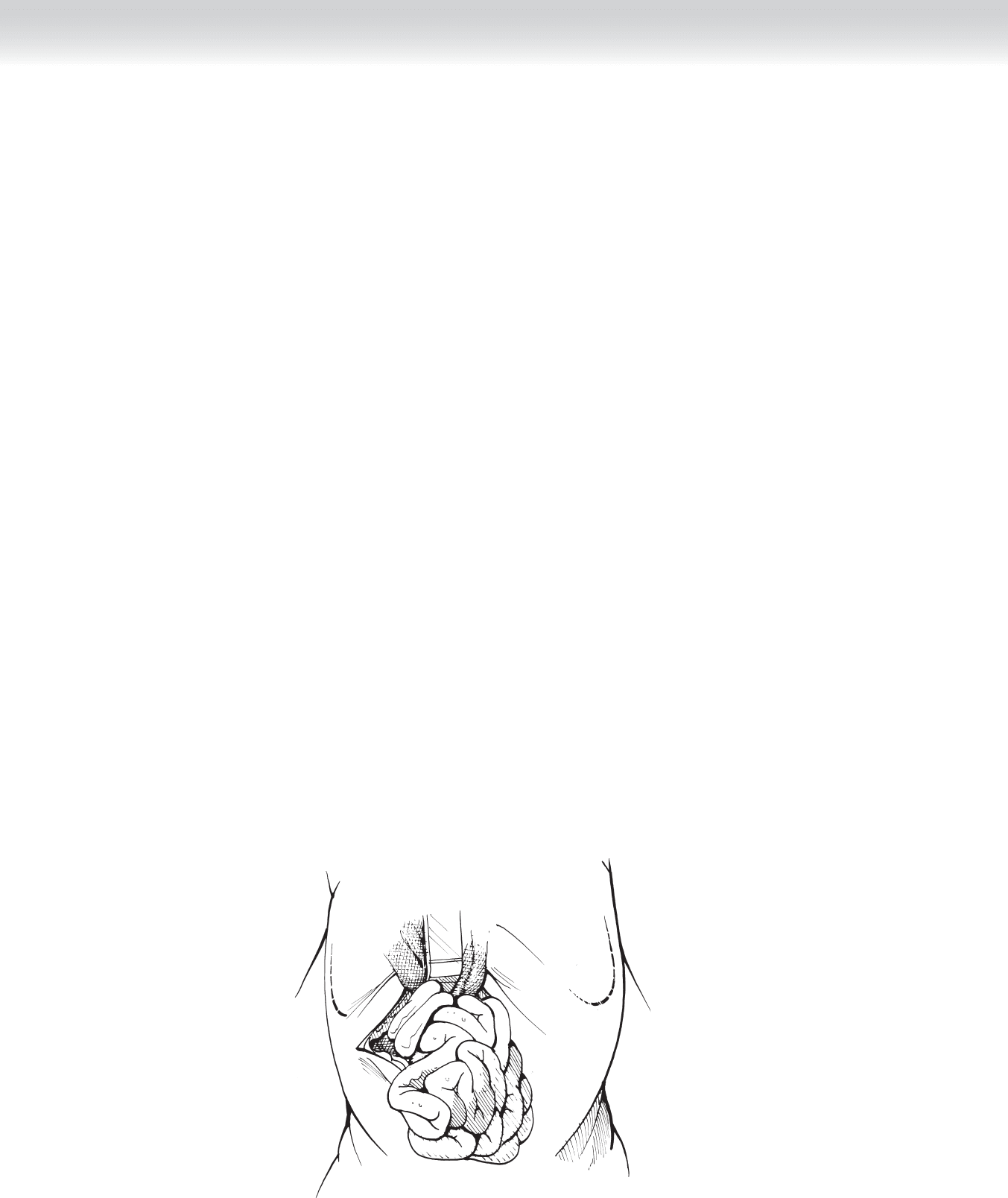
◆ A right upper quadrant transverse laparotomy is performed, the muscles are divided in the
direction of the incision, and the umbilical vein in the free edge of the falciform ligament is
tied with 5-0 silk sutures and divided (Figure 40-4).
2. DISSECTION
◆ The entire bowel is delivered outside the incision to verify the presence or absence of a
midgut volvulus (see Figure 40-4). Because, in most cases, the volvulus has twisted clock-
wise, devolvulation should proceed counterclockwise (Figure 40-5). This maneuver usu-
ally produces signifi cant improvement in the appearance of the intestine. Warm com-
presses can be applied to intestine of questionable viability and left alone for 10 minutes.
All intestines that are frankly gangrenous should be removed; intestines of questionable
viability should be left behind, and a second-look laparotomy planned in 24 to 36 hours
to allow for better demarcation of the segments to be resected. Often during this second-
look operation a primary end-to-end anastomosis can be performed. Ladd’s bands extend
from the cecum and ascending colon, attaching to the anterior surface of the duodenum
and across the duodenum to the posterior aspect of the right upper quadrant. These
bands are sharply divided (Figure 40-6). To relieve any obstruction, the surgeon must
free the duodenum from the Ladd’s bands on both its lateral and medial aspects. The du-
odenum is straightened by division of the ligament of Treitz. Takedown of Ladd’s bands
results in separation of the duodenum, cecum, and ascending colon and broadening of
the mesentery (Figure 40-7). A nasogastric tube is passed to make sure that there is no
further obstruction of the duodenal lumen. Because the cecum will ultimately lie in the
left upper quadrant, an appendectomy is performed (Figure 40-8). The intestines are re-
trieved into the abdominal cavity beginning with the duodenum, leaving the duodenum
and small bowel on the right side and the colon on the left side.
FIGURE 40 –4